Urinary System 3 - Loop of Henle, DCT and Collecting Duct
0.0(0)
Card Sorting
1/30
Earn XP
Description and Tags
Last updated 6:31 PM on 2/6/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
1
New cards
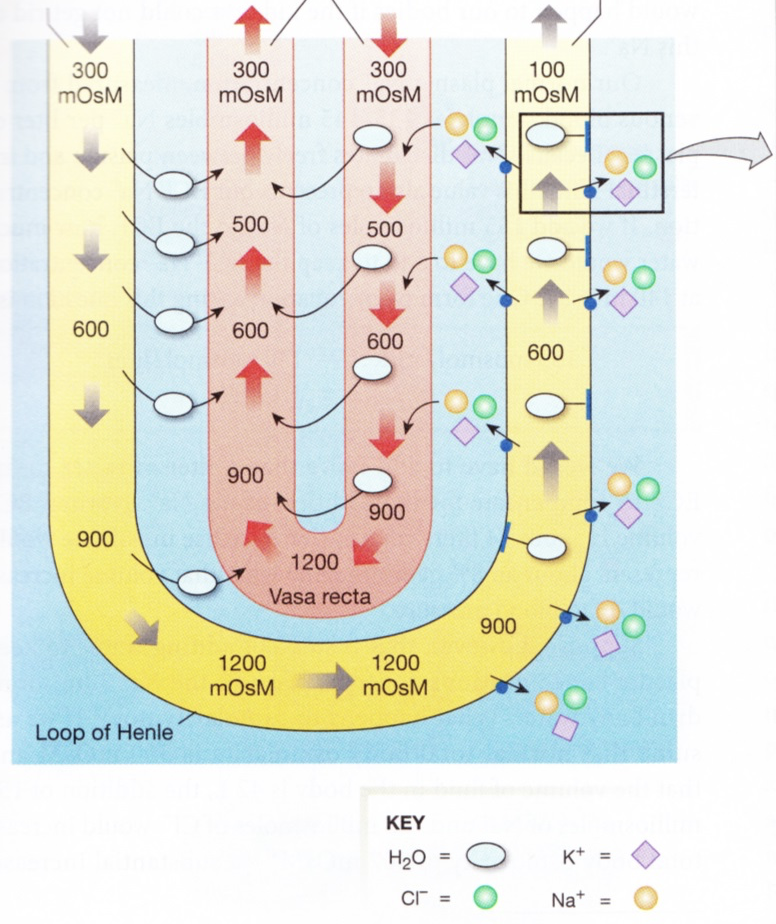
osmotic gradient in renal medulla
* The interstitial fluid in the renal medullar gets increasingly hyperosmotic
* The limits for the osmolarity of urine are species specific and determined by the osmolarity of the renal medulla
* The limits for the osmolarity of urine are species specific and determined by the osmolarity of the renal medulla
2
New cards
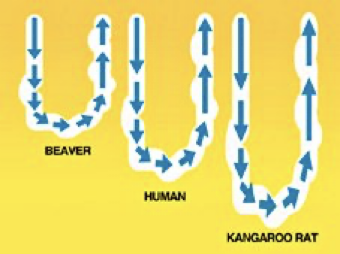
Maximum Concentrating Ability of the Kidneys Varies with Species
The ability to concentrate depends on the relative length of the loop of henle and the number of juxta medullary nephrons.
Some animals e.g. humans also have cortical nephrons which have little value in concentrating urine.
Some animals e.g. humans also have cortical nephrons which have little value in concentrating urine.
3
New cards
Why have a medullary osmotic gradient?
We need something against which we can move water by osmosis.
4
New cards
loop of henle
* Descending limb lacks ion pumps but is very permeable to water
* The ascending limb is not permeable to water
* Active transport of ions out of the ascending limb leads to osmotic transport of water out of the descending limb
* The ascending limb is not permeable to water
* Active transport of ions out of the ascending limb leads to osmotic transport of water out of the descending limb
5
New cards
static effect
1. **Static effect**
* Active transport of solute out of ascending limb to make interstitial space hyper osmotic and draws water out of descending limb making filtrate more concentrated
6
New cards
fluid flow
2. **Fluid flow**
* As filtrate is continually produces new tubular fluid enters the descending limb and pushes the fluid at higher osmolarity down the tube
7
New cards
what happens as static effect and fluid flow are repeated
As these 2 steps are repeated over, the osmotic gradient steadily multiples down the tube.
8
New cards
how would a standard capillary network around the loop of henle impact the concentration gradient
Capillaries that freely exchange solutes and water with the medulla pose a risk to the osmotic gradient.
If there was a standard dense capillary network surrounded the loop of henle, there wouldn't be a concentration gradient.
If there was a standard dense capillary network surrounded the loop of henle, there wouldn't be a concentration gradient.
9
New cards
The Capillary Network Surrounding the Loop of Henle is Highly Specialised
* Called vasa recta
* Supply oxygen and nutrients to the medulla
* Run parallel to the limbs of the loop of henle
* blood flows in the opposite direction to the filtrate and the hairpin loop slows blood flow down
* Supply oxygen and nutrients to the medulla
* Run parallel to the limbs of the loop of henle
* blood flows in the opposite direction to the filtrate and the hairpin loop slows blood flow down
10
New cards
vasa recta
11
New cards
2 components of the countercurrent multiplier
The countercurrent multiplier has 2 components:
1. Specialised peritubular capillaries (vasa recta)
2. Loop of Henle
1. Specialised peritubular capillaries (vasa recta)
2. Loop of Henle
12
New cards
**Another reason for the hyper osmotic medulla?** *(don’t need to learn - just need to be aware of)*
* Urea - the nitrogenous waste product becomes increasingly concentrated in the filtrate.
* Very highly concentrated in the collecting ducts
* There are urea channels in the medulla which allow urea to escape from the collecting duct and be recaptured by the loop of henle
* ADH unregulated these urea channels in the inner medullary collecting ducts allowing more urea to flow passively into the interstitial fluid and back into thin descending loop of henle
* this process allow urea to contribute to the medullary concentration gradient
* urea recycling is responsible for about 50% of the osmotic gradient
* Very highly concentrated in the collecting ducts
* There are urea channels in the medulla which allow urea to escape from the collecting duct and be recaptured by the loop of henle
* ADH unregulated these urea channels in the inner medullary collecting ducts allowing more urea to flow passively into the interstitial fluid and back into thin descending loop of henle
* this process allow urea to contribute to the medullary concentration gradient
* urea recycling is responsible for about 50% of the osmotic gradient
13
New cards
regulated reabsorption of water
Water cannot be actively pumped - it moves by osmosis.
Most of water absorbed in PCT - not here.
Most of water absorbed in PCT - not here.
14
New cards
fluid that leaves the loop of henle is…
Fluid that leaves the loop of henle is hyposmotic.
15
New cards
endocrine control of water balance
Antidiuretic hormone = ADH
16
New cards
ADH
→ nonapeptide hormone released from the posterior pituitary
→ also known as (arginine) vasopressin
→ also known as (arginine) vasopressin
17
New cards
ADH - Sensitive Principal Cells in the Collecting Duct
* ADH secreted
* ADH binds to specific membrane receptor
* Receptor activates cAMP 2nd messenger system
* Cell inserts aquaporins into apical membrane
* Water is absorbed by osmosis into the blood
* ADH binds to specific membrane receptor
* Receptor activates cAMP 2nd messenger system
* Cell inserts aquaporins into apical membrane
* Water is absorbed by osmosis into the blood
18
New cards
excessive drinking
**Excessive drinking:**
* No ADH
* No aquaporins
* Large volume of dilute urine/diuresis
* No ADH
* No aquaporins
* Large volume of dilute urine/diuresis
19
New cards
dehydration
**Dehydration:**
* Increased ADH
* Increased aquaporins
* Small volume concentrated urine
* Increased ADH
* Increased aquaporins
* Small volume concentrated urine
20
New cards
key points
* The loop of henle continues to reabsorb further water and solute
* Due to the unique permeability’s of different segments of the loop these reabsorption activities act to generate an osmotic gradient through the renal medulla
* This osmotic gradient will allow the tubular fluid to be concentrated in the presence of ADH
* Due to the unique permeability’s of different segments of the loop these reabsorption activities act to generate an osmotic gradient through the renal medulla
* This osmotic gradient will allow the tubular fluid to be concentrated in the presence of ADH
21
New cards
sodium
* 100% filtered
* Approximately 90% reabsorbed
* Approximately 70% has been reabsorbed in the PCT
* Approximately 20% in loop of henle
* Approximately 90% reabsorbed
* Approximately 70% has been reabsorbed in the PCT
* Approximately 20% in loop of henle
22
New cards
potassium
* 100% filtered
* 100% reabsorbed
* Approximately 70% has been reabsorbed in PCT
* Approximately 30% in loop of henle
* 100% reabsorbed
* Approximately 70% has been reabsorbed in PCT
* Approximately 30% in loop of henle
23
New cards
what is the sodium and potassium concentration of the filtrate further modified by
The sodium and potassium concentration of the filtrate is further modified by principal cells in the DCT and collecting duct.
24
New cards
Principal Cells in the DCT and Collecting Duct
* Sodium potassium ATPase maintains sodium potassium gradient
* Leak channels on apical side of the principal cells allow passive diffusion of ions between principal cells and filtrate
* Leak channels on apical side of the principal cells allow passive diffusion of ions between principal cells and filtrate
25
New cards
Principal Cells vs Tubular Cells of the PCT
* Both have asymmetrical arrangement of Na+K+ ATPase
* Principal cells deal with lower volume (no microvilli)
* Principal cells are responsive to hormone
* Water does not necessarily follow Na+
* Principal cells deal with lower volume (no microvilli)
* Principal cells are responsive to hormone
* Water does not necessarily follow Na+
26
New cards
Why doesn't water follow Na+?
Cells are impermeable to water without ADH.
27
New cards
principal cells
Secretion of K+ and reabsorption of Na+ is regulated by the hormone aldosterone.
Cells of DCT and collecting duct are impermeable to water in the absence of ADH - reabsorption of water is therefore not linked to reabsorption of sodium.
Cells of DCT and collecting duct are impermeable to water in the absence of ADH - reabsorption of water is therefore not linked to reabsorption of sodium.
28
New cards
phosphorous
**Phosphorous:**
* Inorganic phosphate 100% filtered
* Reabsorption in PCT by Na+ co-transport under hormone control
* Not reabsorbed in DCT and CD
* Dietary excess is excreted via the kidneys
* Inorganic phosphate 100% filtered
* Reabsorption in PCT by Na+ co-transport under hormone control
* Not reabsorbed in DCT and CD
* Dietary excess is excreted via the kidneys
29
New cards
calcium
**Calcium:**
* 50% bound to albumin so only free 50% is filtered
* Approximately 70% reabsorbed in PCT
* Selective reabsorption of Ca2+ in DCT and collecting duct under hormone control
* Normally only 1-2% filtered Ca2+ is excreted
* 50% bound to albumin so only free 50% is filtered
* Approximately 70% reabsorbed in PCT
* Selective reabsorption of Ca2+ in DCT and collecting duct under hormone control
* Normally only 1-2% filtered Ca2+ is excreted
30
New cards
regulation of calcium and phosphorous
Parathyroid hormone (PTH) is released in response to decreased \[Ca2+\] in the blood.
In the kidney, parathyroid hormone (PTH):
* Decreases reabsorption of phosphate in the proximal tubule
* Increases reabsorption of Ca2+ in the ascending loop of Henle, distal tubule, and collecting tubule
In the kidney, parathyroid hormone (PTH):
* Decreases reabsorption of phosphate in the proximal tubule
* Increases reabsorption of Ca2+ in the ascending loop of Henle, distal tubule, and collecting tubule
31
New cards
key points - ions
* Small volume, regulated reabsorption or secretion of Na+ H+ Ca2+ and water occurs in the DCT and collecting duct
* 100% of potassium and bicarbonate have already been reabsorbed by the start of the DCT
* Homeostatic mechanisms can lead to secretion of potassium, and bicarbonate back into the filtrate
* 100% of potassium and bicarbonate have already been reabsorbed by the start of the DCT
* Homeostatic mechanisms can lead to secretion of potassium, and bicarbonate back into the filtrate