Attrition
Bruxism, form of this, excessive grinding. Wearing of teeth from tooth to tooth contacts, malocclusion, grinding and mastication.
Abrasion
Teeth wear from use of abrasive substances, EX: Chewing foreign objects. Excessive oral hygiene habits handed brushing.
Abfraction
Angular notch at the gumline caused by bending forces applied to the tooth.
For of non-carious tooth tissue loss that occurs along the gingival margin.
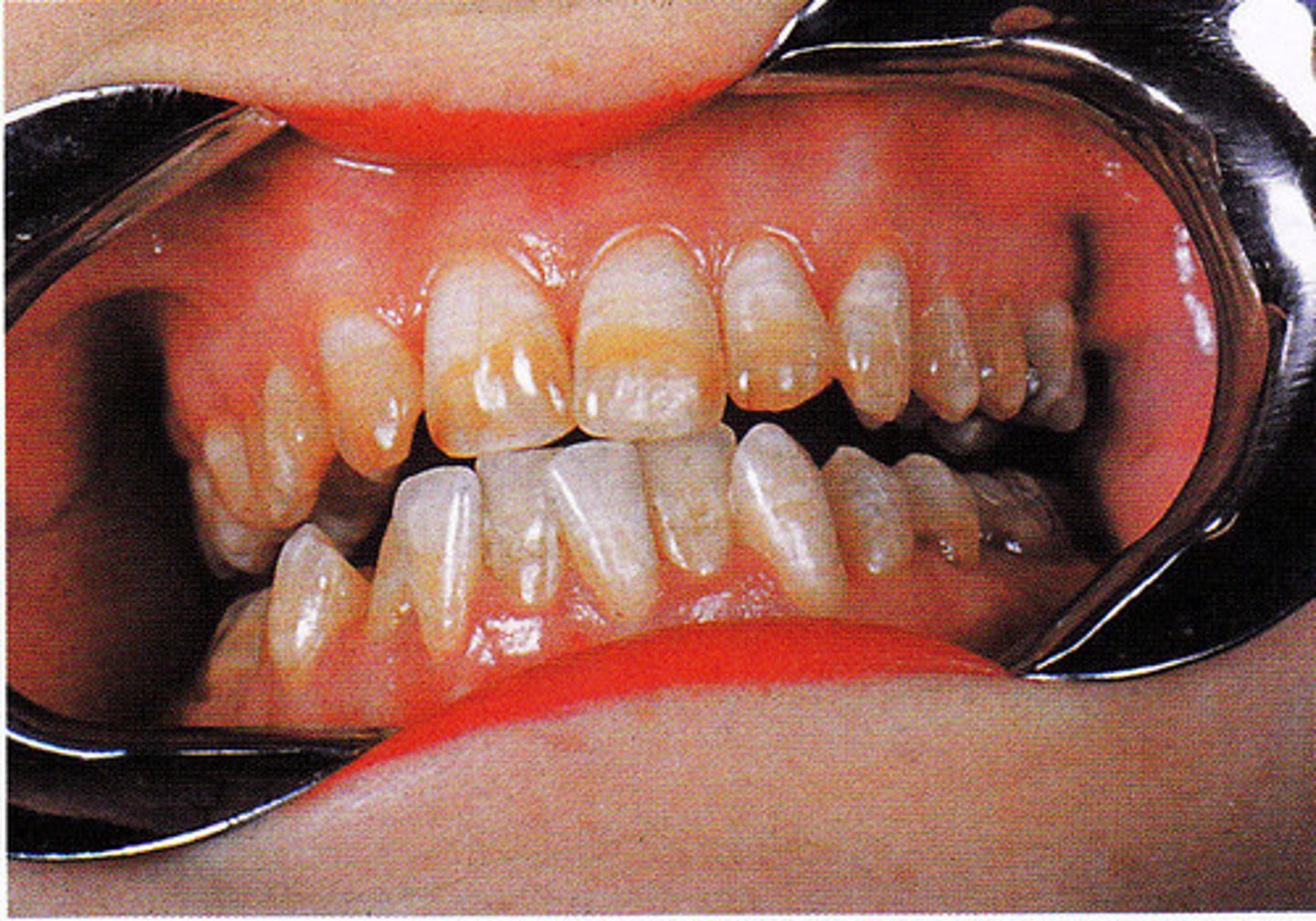
Erosion
Loss of tooth structure from a chemical process
Affects many or all teeth in an arch; shiny, glossy look.
Common causes: Chronic vomiting seen bulimia, acidic foods, GERD (Gastro-esophageal reflux disease)
BOARD ALERT: Bulimia patients often present with this!!
Massester Muscler
What muscle will become more prominent if a patient engages in bruxism?
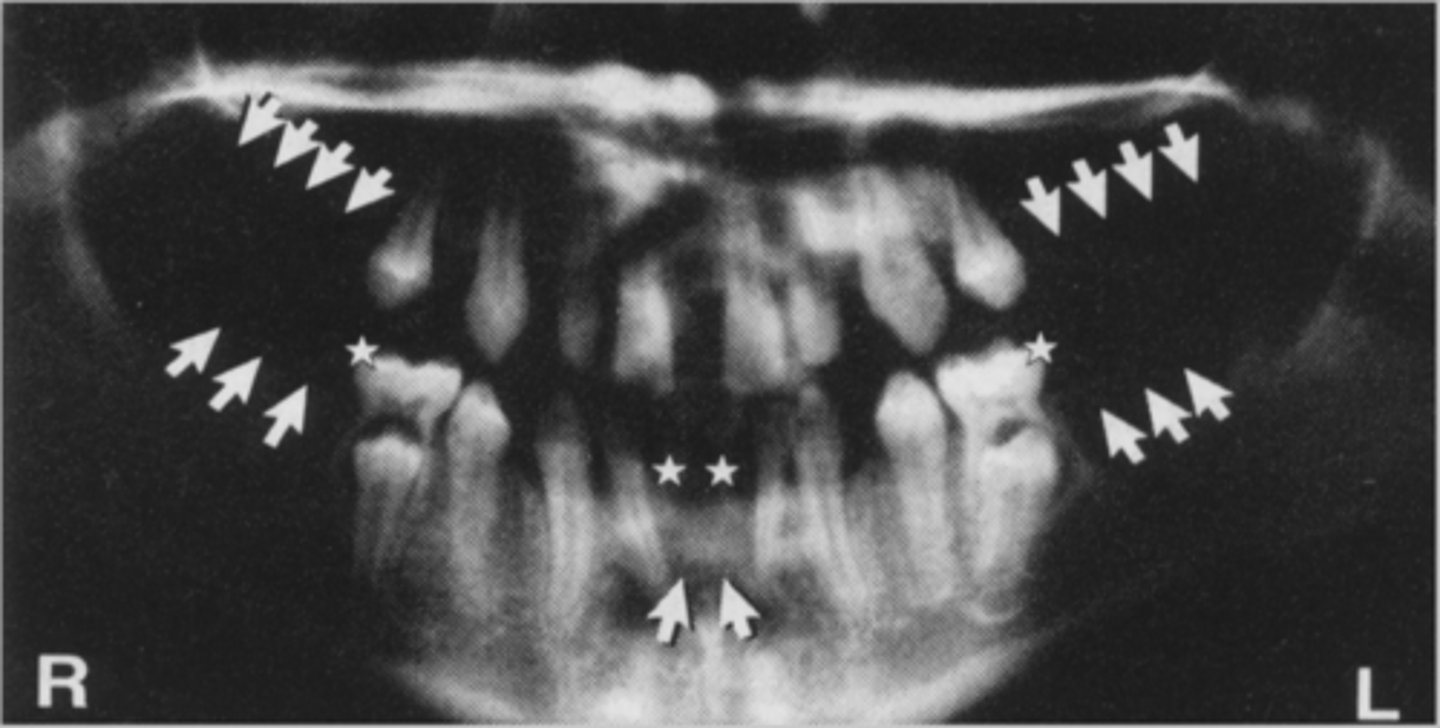
Supernumerary Teeth- Hyperdontia
Excess number of teeth
Mesiodens
Between #8 and #9 (Maxillary midline) this is where it's most common.
Next it can happen in the maxillary molar area (Fourth molars, distomolar) 2nd most common.
Anodontia
Complete absence of teeth
Ectodermal Dysplasia
Abnormal development of teeth
Hypodontia
Partial anodontia- one or several teeth are missing-common with conical shaped teeth.
Less than normal teeth
Oligodontia
Congenitally missing 6 teeth or more (3rd molars are common)
-Occurs during development
Microdontia
Small teeth. "Peg Lateral"- Maxillary lateral incisor-most common
Macrodontia
Large teeth-rare
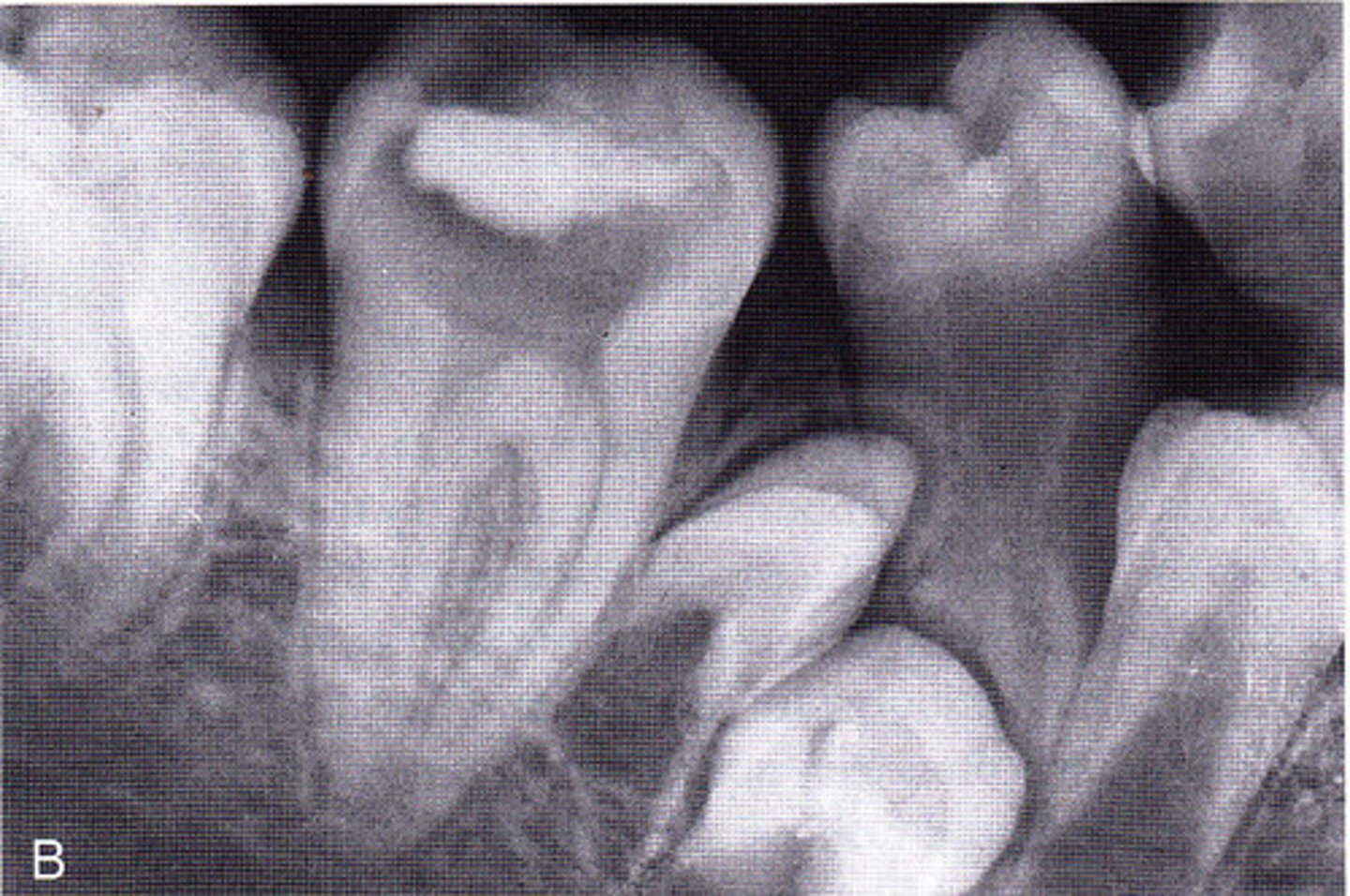
Taurodontism
"Bull Tooth". Rare development disturbances of a tooth-isolated normally. Body is enlarged at the expense of the roots.
-Enlarged pulp chamber, apical displacement of the pulpal floor, lack of constriction at the CEJ.
More common in Down Syndrome clients.
Amelogenesis Imperfecta
Hereditary disorder of enamel formation.
-Clinically see enamel hypoplasia, pits, grooves, soft enamel, teeth can darken or be discolored. Dentin and Pulp appear normal.
Dentinogenesis Imperfecta
-Inherited dentin disorder
-Teeth are discolored-opalescent dentin
-Poor dentin formation compromised normal enamel
-Radiographically-abnormal pulp and crown
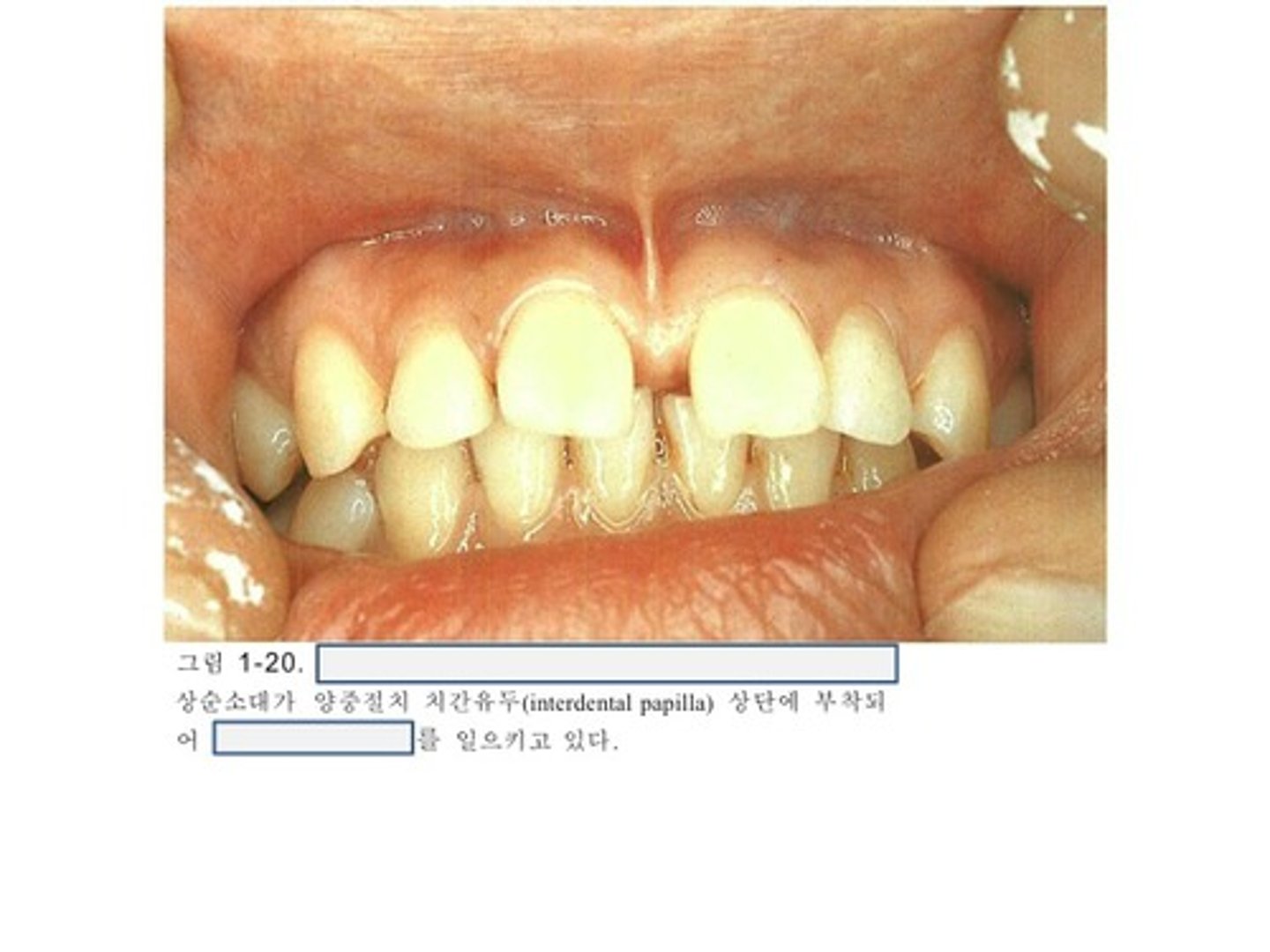
Diastema
-Space between two adjacent teeth
-Hereditary Trait
-Some factors that may contribute-frenum attachment and muscle pull.
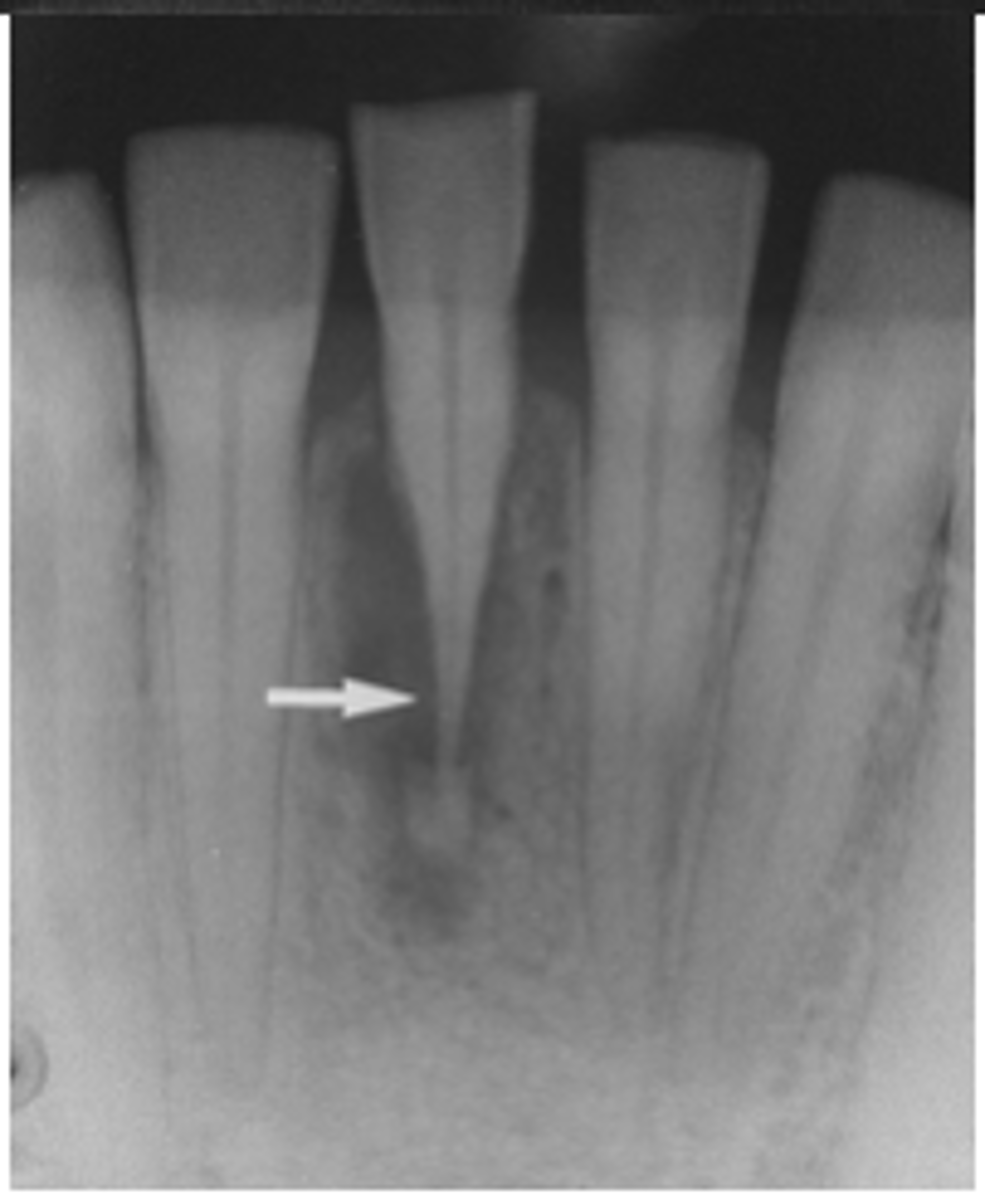
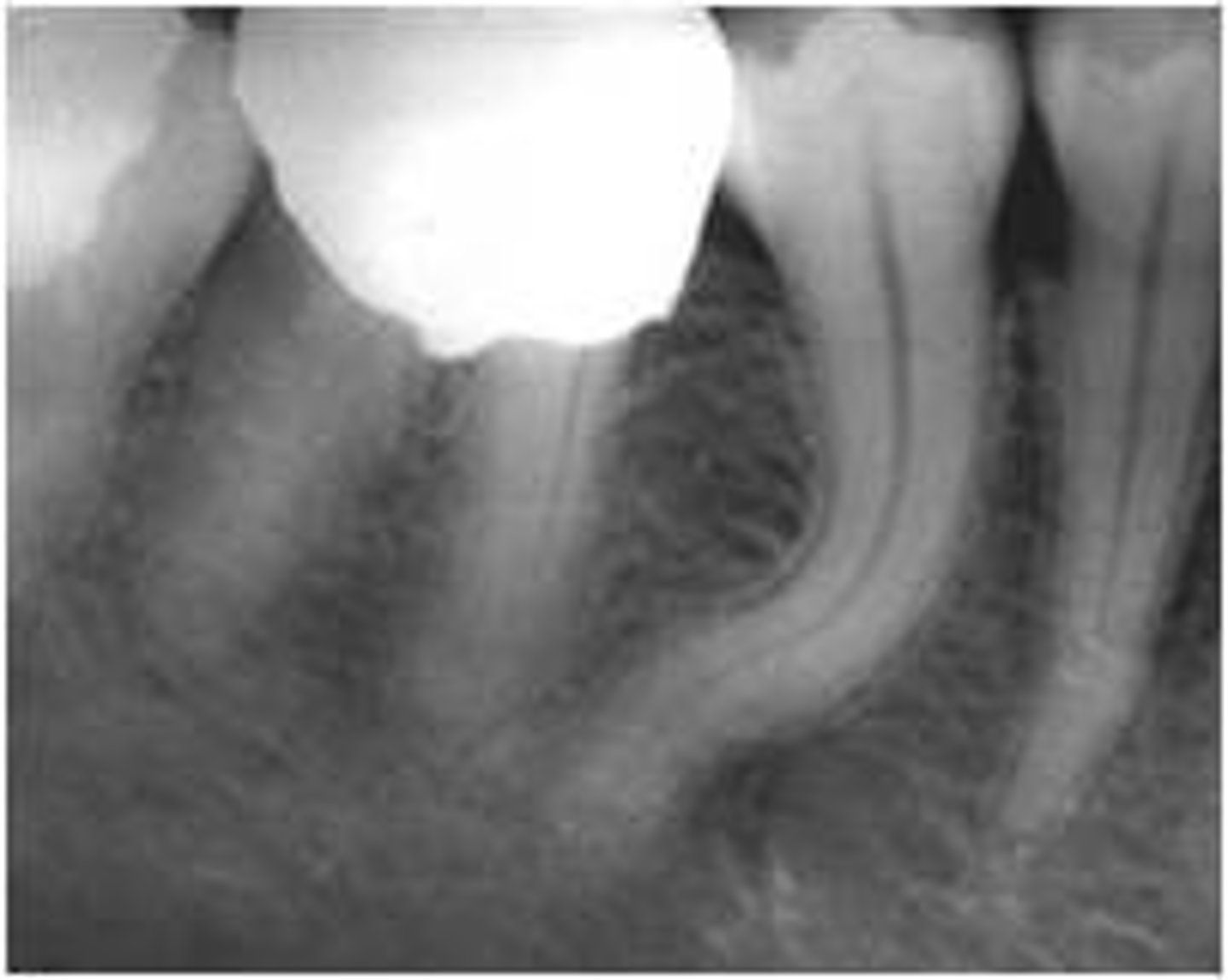
Internal resorption
-Etiology-Possible pulp injury, sometimes unknown.
-Pulp may show through enamel-tooth may appear PINK
-Enlarged pulpal chamber
-Possible endodontic therapy
External Resorption
Abnormal dentin condition-unknown etiology
-Resorption of the teeth externally
Concrescence
-Teeth are joined at cementum
-Second and third molars most affected
Gemination
-Two teeth have developed from a single root.
-Teeth in the arch are normal count
Dens in Dente (Dens invaginatus)
"Tooth within a tooth"
-Invagination of the crown or root that is lined with enamel
-Most common-maxillary lateral incisor; accentuation of the lingual pit.
Dilaceration
-Exaggerated curve or bend in a tooth root or crown
-Difficult to extract or root canal
Enamel pearls ectopic enamel
Disturbance of enamel formation during development
Usually presents in bifurcations or trifurcations
Systemic causes of hypoplasia
-Early childhood diseases
-Birth trauma, syphilis acquired at birth, trauma, fluoride
-Hutchinson's incisors and mulberry molars-syphilis
-Fluorosis
Local causes of hypoplasia
"Turner's tooth"-hypocalcified permanent tooth
Enamel is inhibited possibly due to trauma affecting crown development
Extrinisic Stain (exogenous)
Staining that occurs of environmental factors such as tobacco, use, wine, grape juice
Green
This color stain may become intrinsic with time
Intrinsic stain (Endogenous)
Staining that may occur from enlarged pulp chamber or trauma
Dentin is darkened
Tetracycline staining
-Endogenous gray, yellow, brown staining.
-From mother's ingestion of tetracycline prenatally
-Will respond to whitening methods.
Aspirin induced
This induced lesion is white and necrotic-review history with the patient
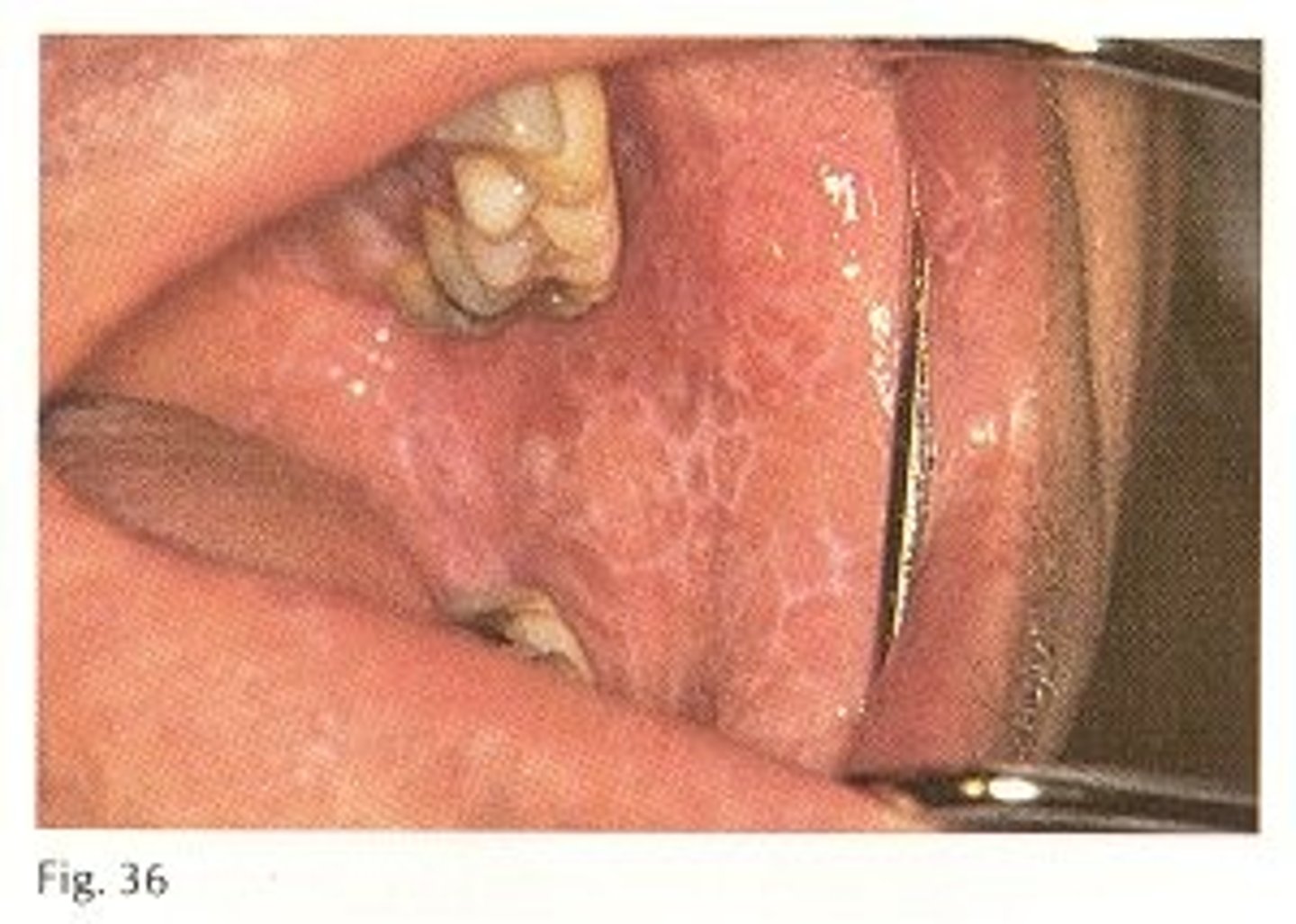
Nicotinic stomatitis (Smoker's palate)
-White, hyperkeratotic, coarse, nodular, wrinkled appearance to hard palate in smokers.
-Scattered red dots are the orifices of inflamed minor salivary glands. Benign but predisposes to malignancy.
-Heat leads to reddened hard palate.
Leukoplakia
White plaque/patches on oral mucosa-CANNOT wipe off.
-May be related to tobacco use: Cigarettes and smokeless
-Hyperkeratotic or squamous cell carcinoma.
-Hairy leukoplakia-associated with HIV clients, caused by EBV, white patch on lateral border of tongue.
-Usually benign
Leukoedema
-Milk white/grayish lesions of buccal mucosa that disappear when stretched.
-More prominent in dark skin individuals.
Linea Alba
Hyperkeratotic line of buccal mucosa along plane of occlusion.
Also referred to as frictional keratosis cheek or frictional keratoses.
Candida Albicans
-Most common fungal infection
-Most common oral lesion in HIV positive pt.
-Local factors: Xerostomia, complete/partial dentures, steroid inhalers, etc.
-Systemic factors: Antibiotic therapy, HIV+, uncontrolled diabetes, etc.
-Several different presentations
-All can present with burning
Pseudomembranous Candidiasis (thrush)
White plaque that wipe off but leave red painful patches-classic presentation.
-Erythematous candidiasis-form of this that appears reddened-associated with HIV/AIDS clients.
Physiological pigmentation
This varies with dark skinned individuals.
Normal pigmentation is this.
Melanotic Macule
Flat, brown-freckle.
-Found intraorally or on lip
-Also known as oral focal melanosis
-Asymptomatic, no treatment required.
-Addison's disease-buccal mucosa, gingiva, tongue and lips (petechiae, also on palate)
Amalgam tattoo
Gray, blue-black, flat lesion
Amalgam particles embedded in soft tissue
Fordyces Granules
Intraoral sebaceous (oil) glands
Small, bilateral, yellow nodules of buccal mucosa and vermillion after puberty.
Angular cheilitis
Fissured areas at the corner of the mouth.
Often associated with riboflavin (vitamin B2) deficiency
Nystatin, clotrimazole
Topical treatment for angular cheilitis
Ketoconazole, fluconazole (diflucan)
Systemic treatment for angular cheilitis
Cow's milk
Board alert: How do you get vitamin B2?
Staphylococcus aureus and C. albicans
Board alert: What bacteria is associated with angular cheilitis
Varicosities (Varix, varices)
Dilated superficial veins
Prominent on ventral tongue (lingual varices)
Lateral borders
BOARD alert: What is the most common location of intraoral cancer?
Geographic Tongue (Erythema migrans, benign migratory glossitis)
Areas of erythema (atrophy of filiform papillae) surrounded by raised, white border
Asymptomatic, sometimes possible burning.
Ankyloglossia (tongue tied)
- short, thick lingual frenum- limitation of tongue movement affecting speech
- 4 males: 1 female
- associated feeding problems in infancy
- periodontal issues
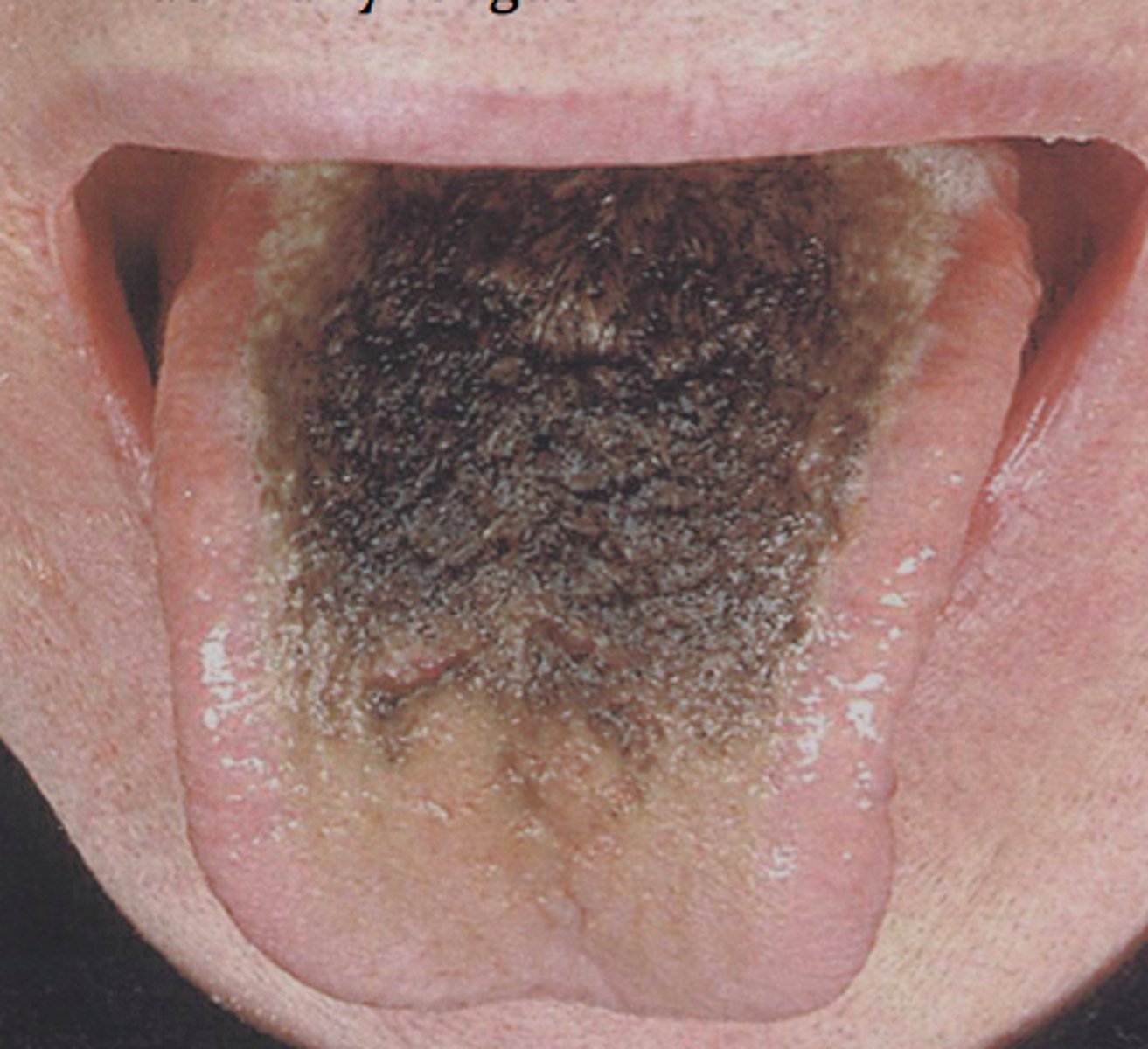
Hairy tongue
Elongation of the filiform papillae
Heavy smoking, antibiotic therapy, poor oral hygiene etc.
Fissured tongue
Fissures and grooves on dorsal tongue surface
Common in Down Syndrome clients
Furrowed tongue
Scrotal Tongue
Macroglossia (Enlarged tongue)
Enlarged tongue
Excess growth hormone
Mouth breathing
Hypodontia
Common in Down Syndrome (Trisomy 21)- may also have fissured tongue
Median Rhomboid Glossitis (central papillary atrophy)
Red, atrophic area
Often associated with candida albicans
Anterior to circumvallate papilla, reddened area at midline of tongue-dorsal surface
Seen in immunocompromised
Xerostomia
May be caused by normal aging process, medications, radiation therapy, and systemic conditions.
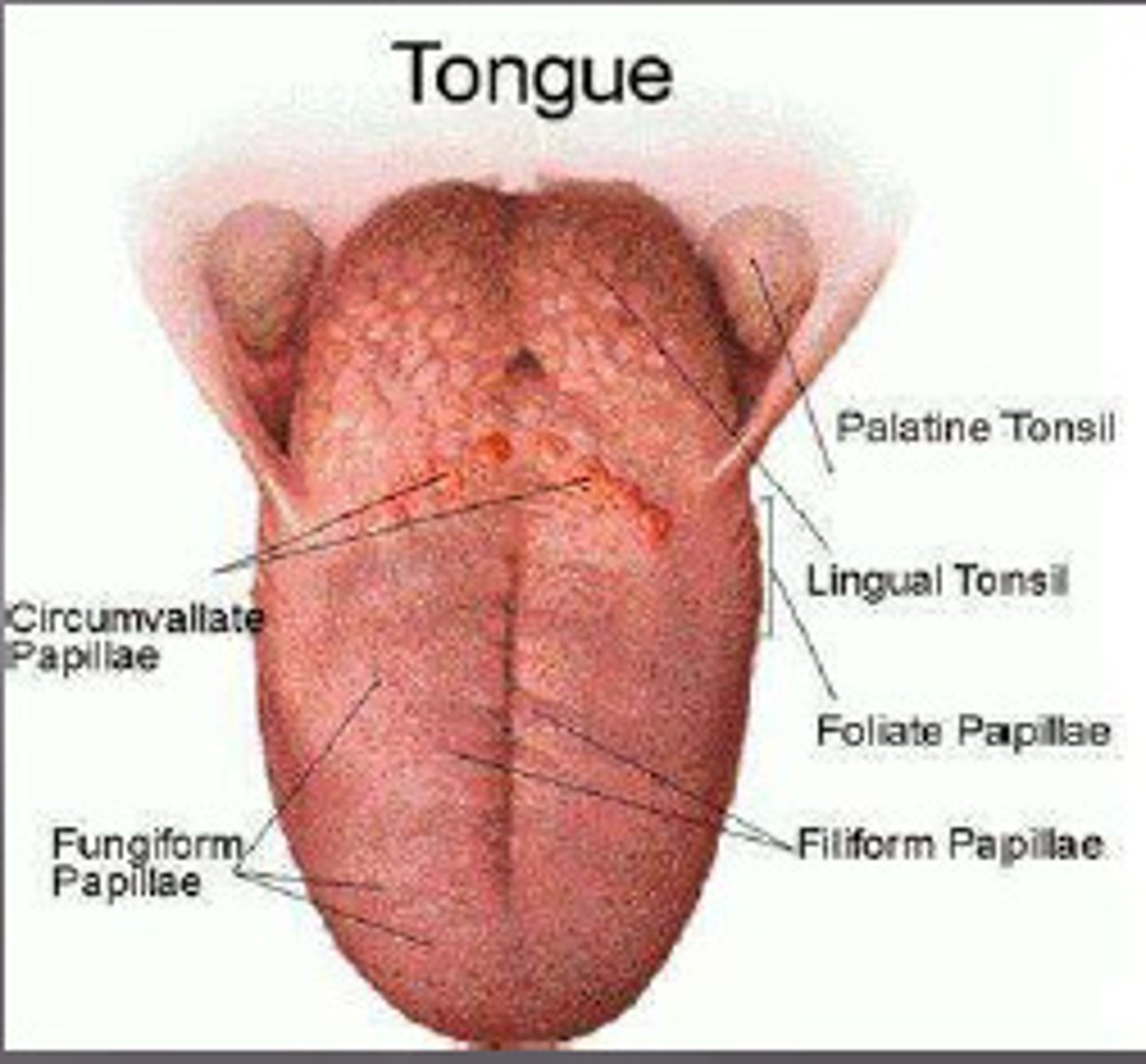
Papilla of the tongue
circumvallate- large v shaped in the back
foliate- on the side
fungiform- mushroom like
filiform- small hair like filament interspaced with fungiform
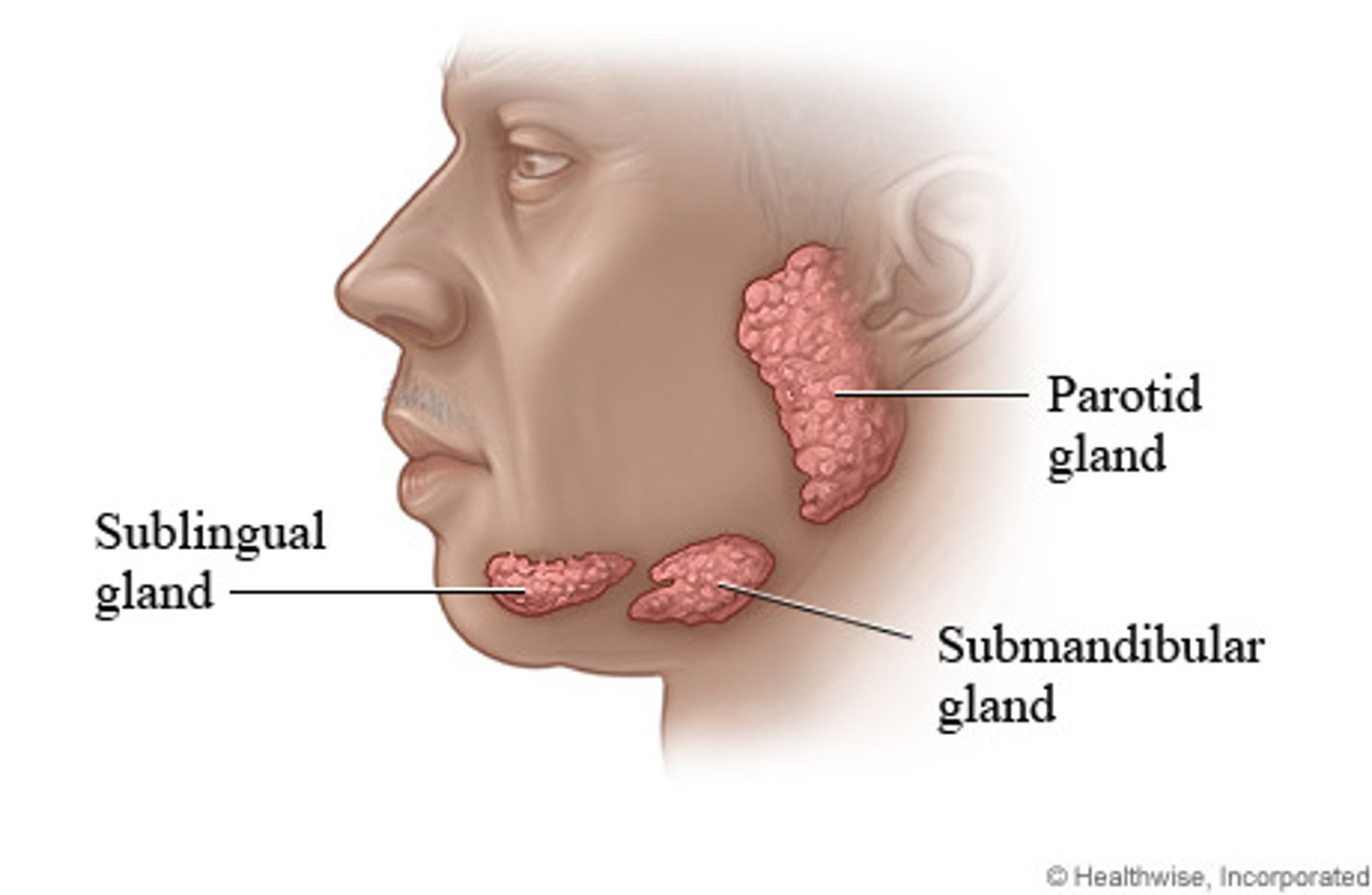
Salivary Glands
Glands of the mouth that produce saliva, a digestive secretion
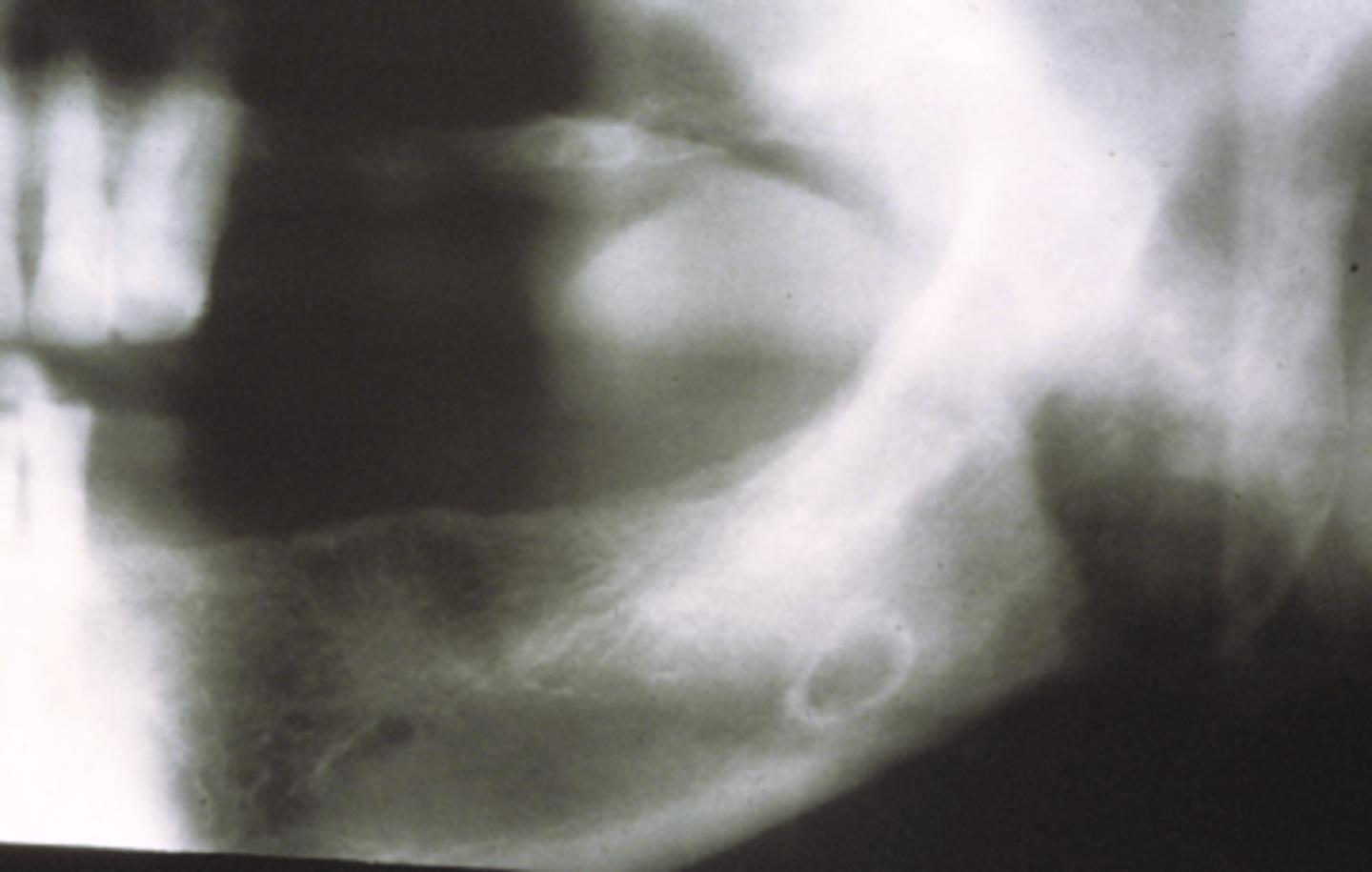
Sialolithiasis (Salivary stones)
- calcification within a gland or duct
- Wharton's (Submandibular) duct is the most common site
- may cause obstruction; swelling seen during eating with partial obstruction
Stafne's bone cyst (Static)
Depression on the mandible at the inferior alveolar canal-submandibular gland
No treatment indicated
Made up of Salivary gland tissue
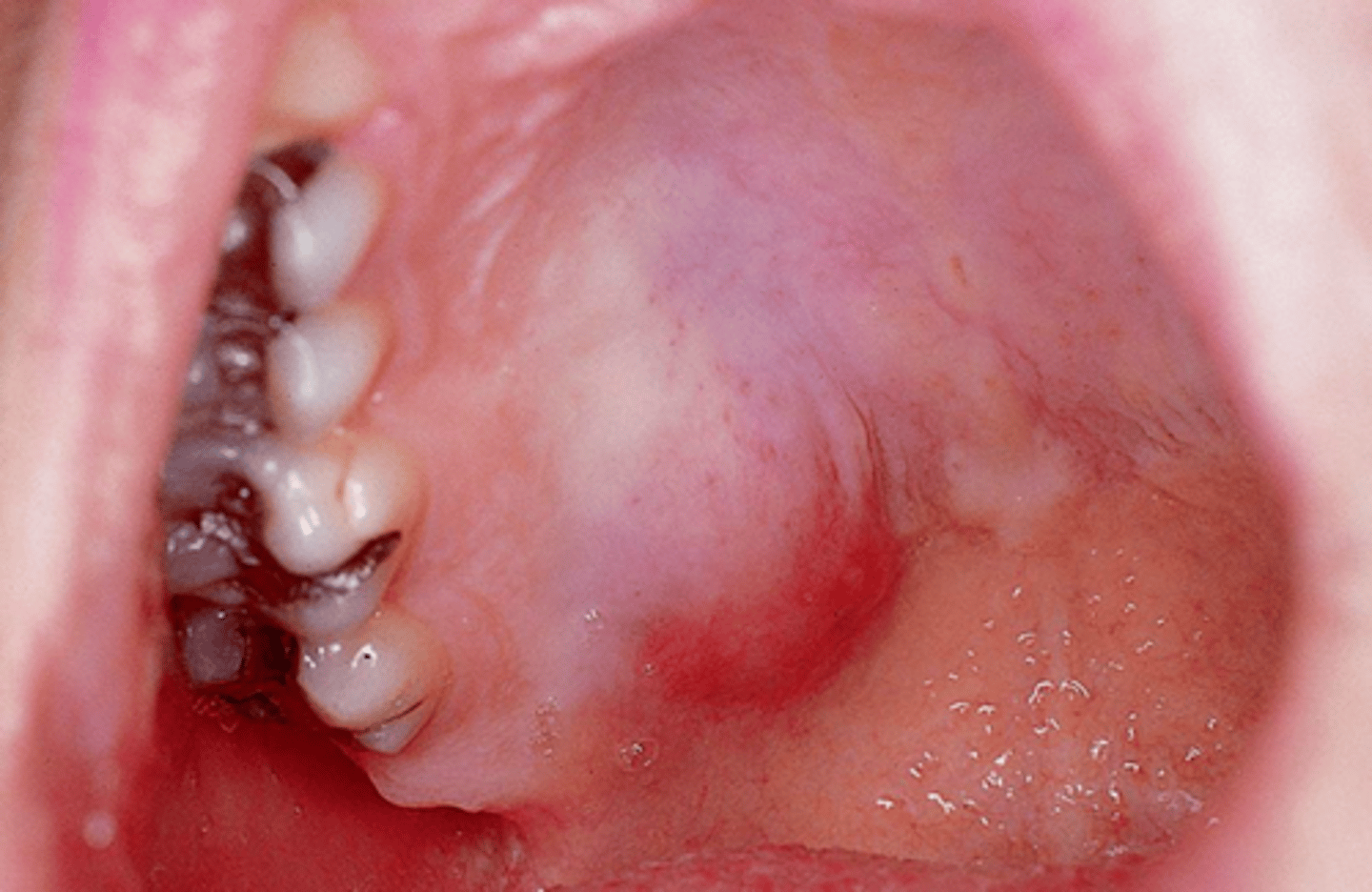
Mucocele
Lower lip most common site
Bluish/pink fluid filled nodule
Caused by traumatic severance of salivary gland ductRanula
Excision
Treatment of a mucocele?
Recurrence: If contributory salivary gland is not removed is not removed.
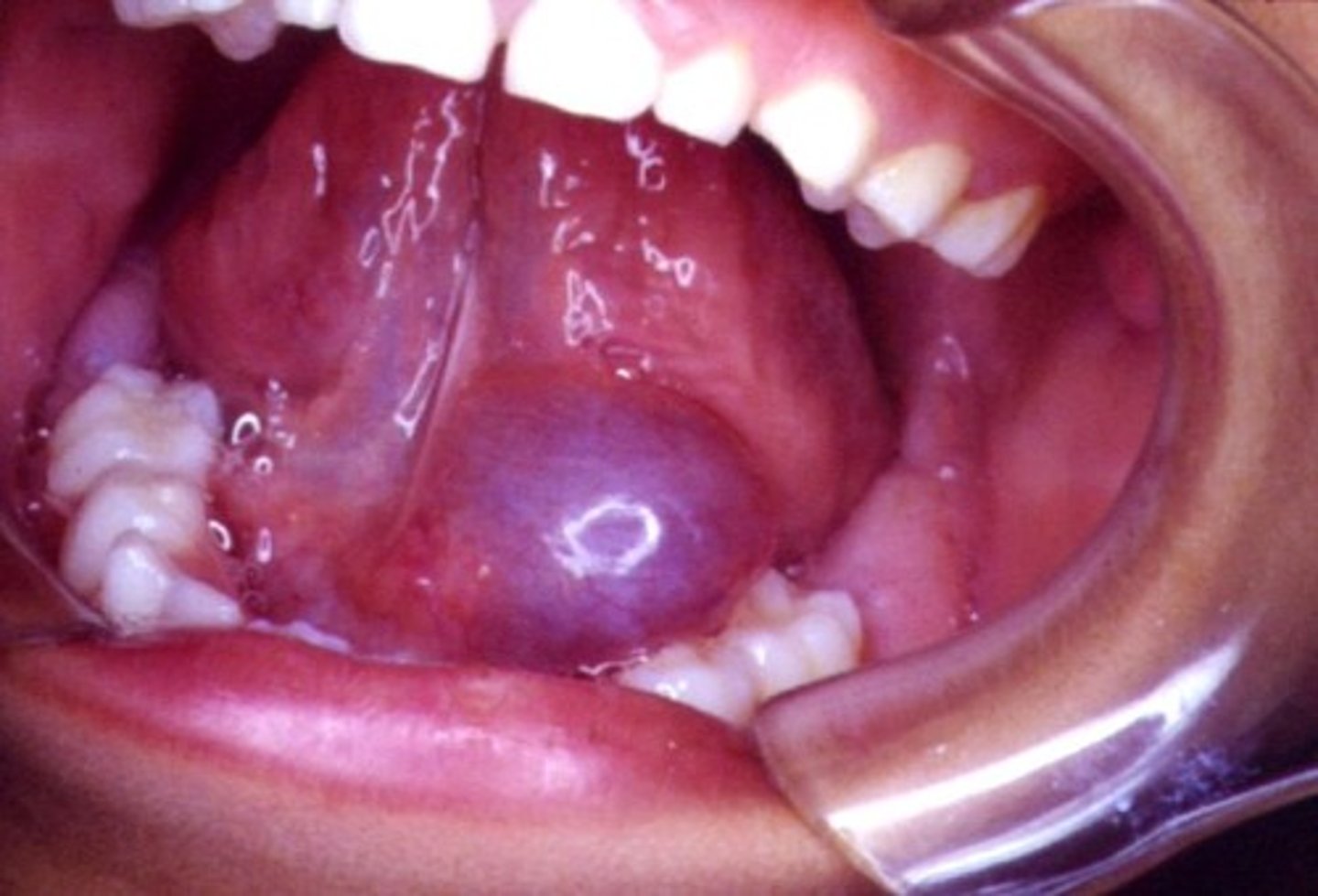
Ranula
"Mucocele of the floor of the mouth"
Usually associated with sublingual gland
Floor of mouth swelling
Pleomorphic adenoma-mixed tumor
Most common tumor of the salivary glands - benign.
•Parotid gland most common location.
•Hard palate (posterior) most common intraoral location.
•Painless, well-circumscribed soft tissue swelling
Mumps (Epidemic parotitis)
-virus transmitted through saliva or respiratory secretions
-bilateral parotid enlargement
-flu like symptoms
Fibroma
The most common tumor of the oral cavity
Caused by chronic trauma
Pink, smooth firm
Usually painless
Hyperplastic tissue in response to irritation
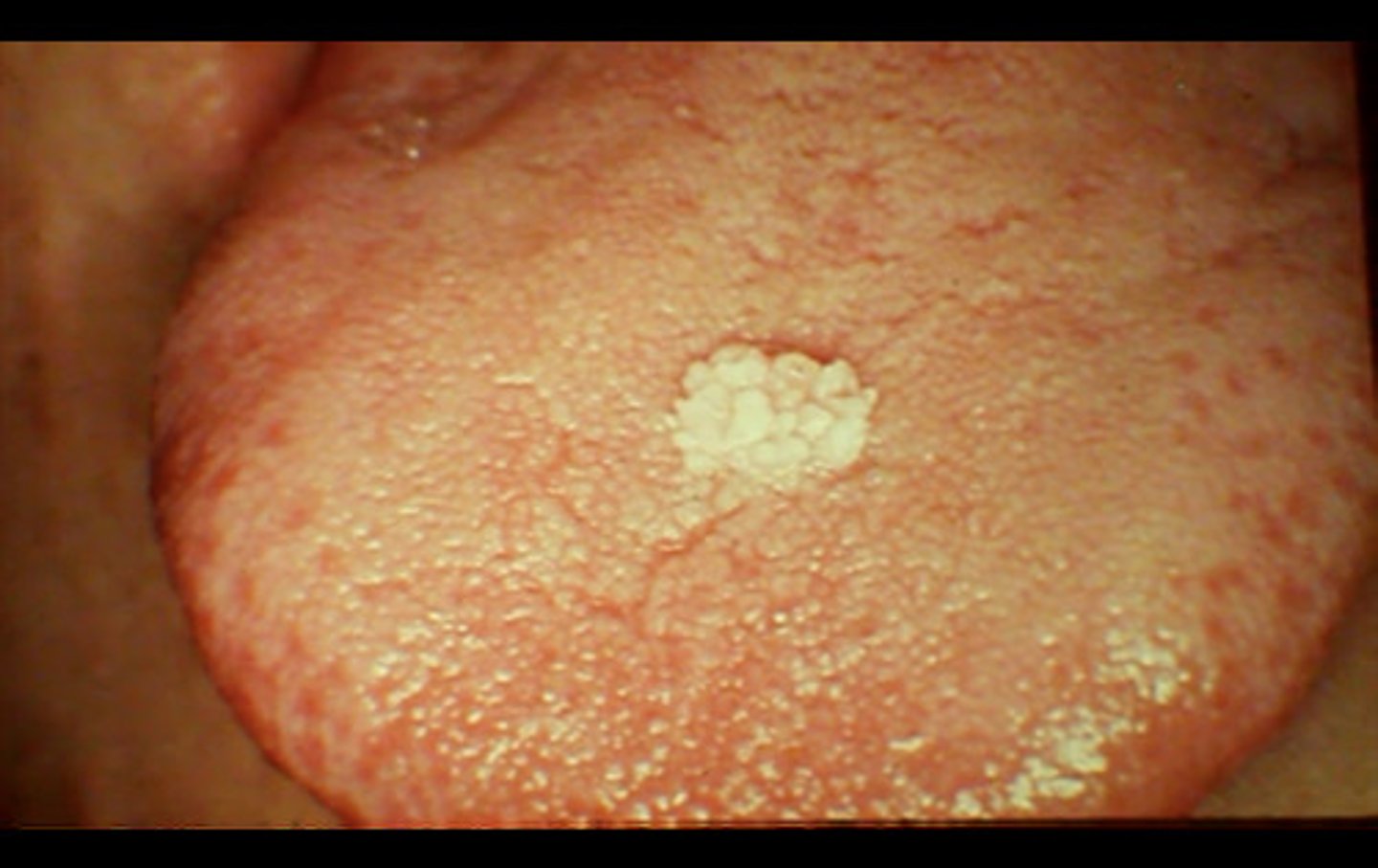
Papilloma
Caused by HPV
Often found in soft palate and uvula
May need to be excised
Cauliflower-like
Peduculated-stalked
Usually does not recur
Hemangioma
Development vascular lesion
Tongue is most common site
Macroglossia can result if found on tongue
Greater incidence in females
Gingival Hyperplasia-Generalized or localized
increase in number of cells present causing inflammation
tx: gingivectomy, OHI
mostly due to medication side effect
medications include: anti seizure medication (phenytoin) hypertensive (procardia)
antirejection (cyclosporine)
Orthodontic appliance may contribute as irritant
Other causes: Hormonal changes, xerostomia, and heredity
Epulis fissuratum (Inflammatory fibrous hyperplasia)
"Fibroma" Around denture flange, caused by ill fitting denture.
Treatment: Remove excess tissue and reline or replace denture
Chronic hyperplastic pulpitis-pulp polyp
Inflamed pulp tissue within a tooth that is severely decayed or has a large open carious lesion.
Painless
Papillary hyperplasia of the palate (Pseudopapillomatosis)
Papillary lesion under maxillary denture, especially if denture never removed.
Excise tissue and remove denture.
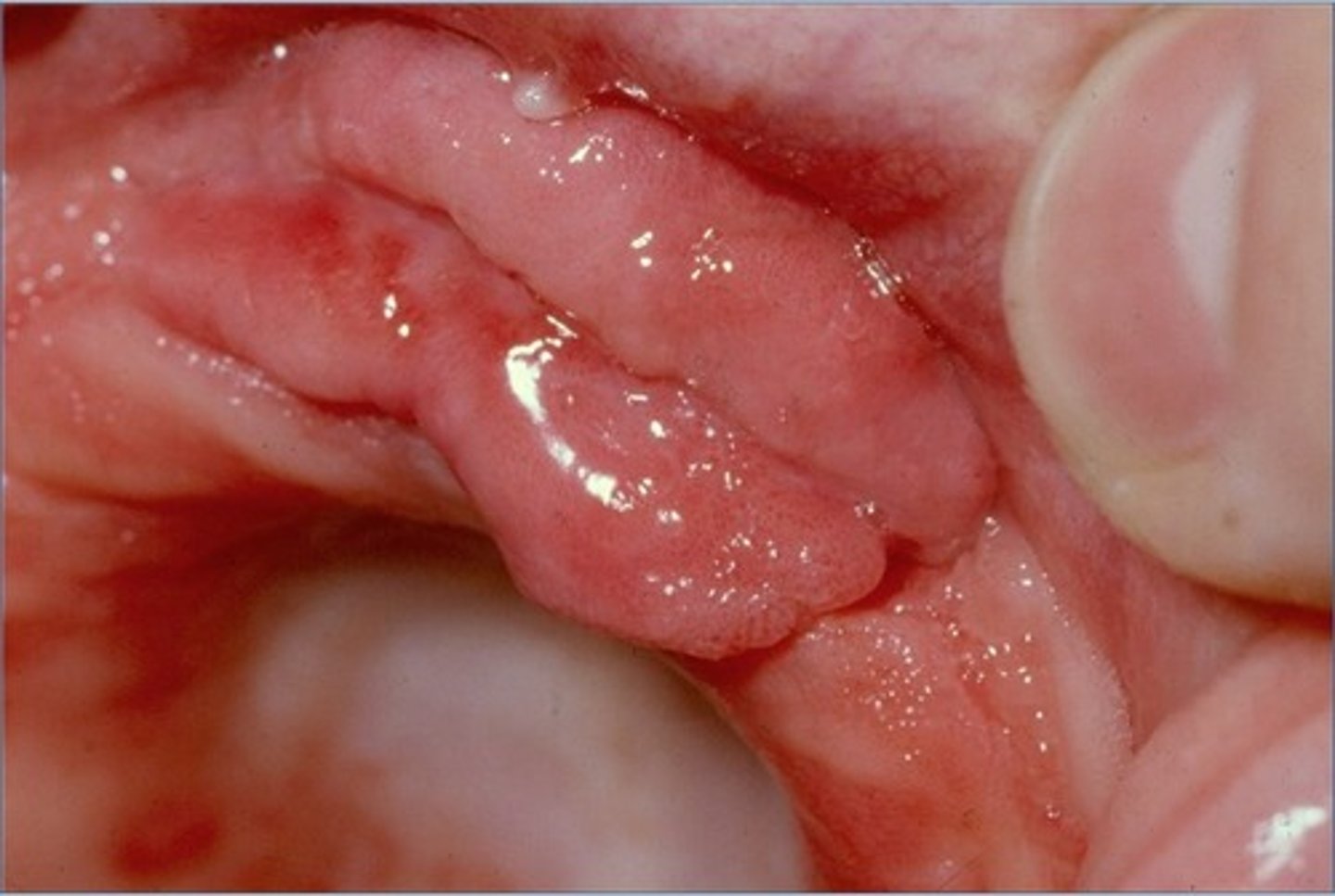
Pyogenic granuloma (BOARD ALERT)
"Pregnancy tumor"- hormonal influenced, especially during pregnancy.
Granulation tissue in response to local irritant
Most common in children and young adults during puberty.
Peripheral Giant Cell Granuloma
Giant cells present-Multinucleated
Clinically similar in appearance to pyogenic granuloma
Multinucleated giant cells present and very vascular causing deep reddish collor
More common in women than men
Central giant cell granuloma: Similar microscopically radiolucent as unilocular or multilocular
Traumatic Ulcer
Caused by trauma-biting, vigorous brushing, eating hard pointed chips.
Usually painful
7-14 day healing time unless trauma reoccurs.
Aphthous Ulcer
-Recurring and painful, well-circumscribed with erythematous halo
-Located on unattached mucosa
-Stress, acidic, or trauma induced
-Incidence in smokers
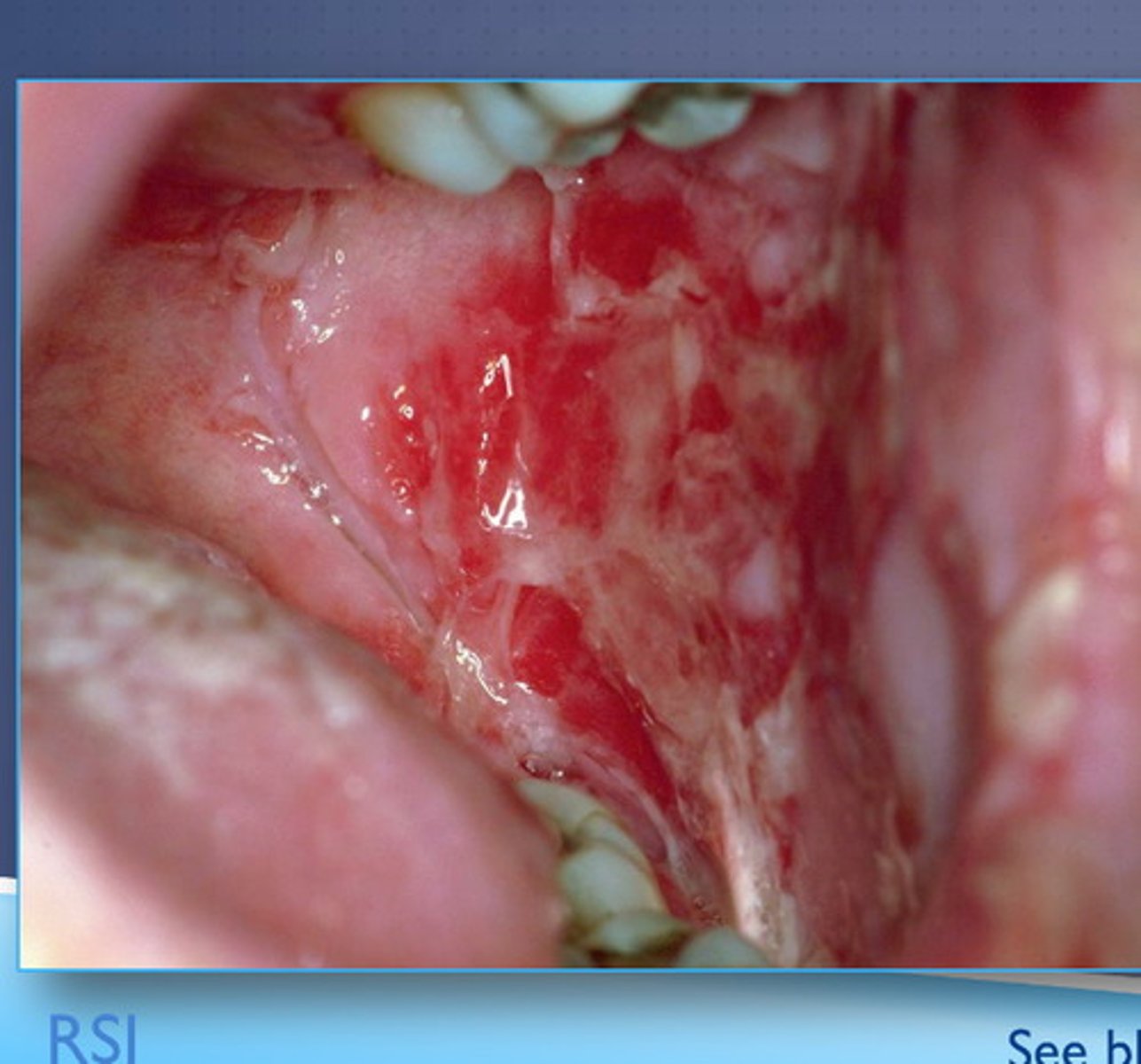
Necrotizing ulcerative gingivitis (NUG/NUP)
Formerly called acute
punched-out, blunted papillae
generally caused by fusiform bacillus and spirochete
associated with decreased resistance to infection
painful, foul odor, metallic taste
Systemic manifestations of NUG/NUP
Fever, cervical lymphaednopathy may be present
May also have oral candidiasis
Abrupt onset may be accompanied by malaise or fever
Excessive salivation
Overwhelmingly foul breath (Fetor oris)
Ulcerations, which are pathognomonic, are present on the dental papillae and marginal gingiva.
Papilla has punched-out appearance and are covered by a gray pseudomembrane.
Similar lesions on the buccal mucosa and tonsils are rare.
Regional lymphadenopathy often is present
Pemphigus vulgaris
Rare autoimmune disorder of the skin.
Oral erosions and lesions may appear before a diagnosis
May be fatal without treatment-high fatality rate
Fragile bullae on skin-thin and ruptures easily
Extensive mucosal involvement-similar to Steven Johnsons syndrome
Difficulty swallowing
Azathioprine, mycophenolate mofetil, Rituximab
Systemic corticosteroids of pemphigus vulgaris
Verruca Vulgaris
Wart caused by Human Papilloma Virus Oral erosions and lesions may appear before diagnosis
Herpes Simplex Virus-1 (HSV-1) Oral herpes
Initial infection: primary herpetic gingivostomatitis- painful, red, multiple vesicles progressing to ulcers
Systemic problems include malaise, fever, lymphadenopathy
Common in young children
May cause trigeminal ganglion
Herpes labialis: found on lip border recurrent cold sores, fever blisters-vesicles will ulcerte
May cause tingling, itching, burning and redness prior to lesion approaching
Triggers: stress, sun exposure, fever, menstruation; especially Problematic for immunocompromised clients
Recurrent intraoral HSV: "bound-down" keratinized mucosa (hard palate and attached gingiva)
Healing in 7-10 days
Treatment: Acyclovir or antiviral creams
Herpes Simplex Virus-2 (HSV-2)
Genital Herpes
STD-More than one out of every 6 people aged 14-49 years
Herpes-1 can infect genital area and cause lesions
Varicella Zoster Virus (VZV)
Chickenpox- Erythema, vesicles, pustules, crusted lesions
Shingles-Painful unilateral erythema, vesicles and ulcers
Epstein-Barr Virus (EBV)
Member of the herpes virus family
Mononucleosus infection-Fatigue, malaise, palatal petechiae
Burkitt's lymphoma and malignancies such as nasopharyngeal carcinoma
Oral Hairy leukoplakia-Primary manifestations of HIV, white, furrowed lines on lateral surface of tongue.
Transmitted via droplets
Herpes Virus
What is the causative organism for Epstein Barr infections?
Cytomegalovirus (CMV)
Mostly in immunocompromised
Oral Mucosa ulcerations
Herpetic Whitlow
Recurrent and painful HSV infection of the fingers
Kaposi's sarcoma (HHV-8 Human Herpesvirus 8)
Associated with AIDS
Neoplastic lesion
Multiple bluish-purple and white macules and plaques
Common HIV-infected clients
Herpangina (Coxsackie virus)
Vesicles or ulcers of posterior oral cavity or soft palate
Flu-like symptoms
Hand-foot and mouth disease (Coxsackie virus)
Ulcerations or vesicles of feet, mouth, and hands-painful
Flu-like symptoms
Prevalent in young children
Diabetes Mellitus Type I and II
gingivitis and periodontitis leading to premature tooth loss
poor oral wounding healing
salivary dysfunction such as xerostomia and sialosis
dental caries
bacterial and fungal infections
halitosis
tongue abnormalities such as fissured tongue, bald tongue, geographic tongue, and median rhomboid glossitis
taste disturbance
oral lichen planus and lichenoid drug reaction
dry socket
neurosensory oral disorder like burning mouth syndrome
Sjogren Syndrome
Autoimmune disease causing xerostomia and dry eyes
May lose papillae
Often painful or uncomfortable, may cause burning and discomfort
Evoxac (cevimeline hydrochloride)
What is the treatment for sjogren's syndrome?
Is a cholinergic agonist use to treat
Erythema multiforme
Stevens-johnson Syndrome
Erythema multiforme major
Multiple mucosal surfaces are ulcerated
Usually triggered multiple medication use
Acute ulcerative condition of skin and mucous membranes
Immunologic response to foods, chemicals, drugs, or microbial infection
Hemorrhagic crusting of lips
"Bull's eye"
Lupus Erythematosis-Chronic discoid (cutaneous)
Autoimmune disorder with periods of remission
Mucosa and skin ulcerations
"Butterfly" rash found on face
Lichen Planus
Skin disease that may appear as fine ace like white lines (reticular)- Wickham's striae or red ulcerations (erosive)
More common in middle-aged women
Myasthenia gravis (MG)
Long-term neuromuscular disease
Varying degrees of skeletal muscle weakness
Scurvy
Vitamin C Deficiency
Can lead to anemia, fatigue, exhaustion
Easily bruised, poor wound healing, hair loss, dry pale skin, small bleeding around the hair follicles (Corkscrew hair) and under nails (periungual) hermorrhage
Spontaneous bleeding, pain in the limbs, and especially legs, swelling in parts of the body.
Gingival ulcerations and tooth loss
Odontogenic cysts
Cyst lining is epithelial tissue produced during tooth development
Epithelial rests of Serres
Remnants of the dental lamina