Trauma Study
1/173
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
174 Terms
List the two primary types of mobile x-ray units.
True/False: A fully charged battery-powered mobile unit has a driving range of up to 10 miles on level ground.
With battery-powered mobile unit types, how long does recharging take if the batteries are fully discharged?
Which type of mobile unit is lighter in weight?
What is the common term for a mobile fluoroscopy unit?
What are the two primary components of a mobile fluoroscopy unit (located on each end of the structure from which it derives its name)?
Why should the mobile fluoroscopy unit not be placed in the AP projection (“tube-on-top” position)?
With the tube and intensifier in a horizontal position, at which side of the patient should the surgeon stand if he or she must remain near the patient—the x-ray tube side or the intensifier side? Why?
Of the two monitors found on most mobile fluoroscopy units, which is generally considered the "active" monitor—the right or the left? ______________
True/False: The operator must determine image orientation on the mobile fluoroscopy monitors before the patient is brought into the room.
True/False: All mobile digital fluoroscopy units include the ability to magnify the image on the monitor during fluoroscopy.
A 30° C-arm tilt from the vertical perspective increases exposure to the head and neck regions of the operator by a factor of ______________.
True/False: Automatic exposure control systems are not feasible with mobile fluoroscopy.
Name the feature that allows an image to be held on the monitor while also providing continuous fluoroscopy imaging and removing stationary structures from the viewing screen. ______________
Situation: The C-arm is in position for a posteroanterior (PA) projection. What exposure field range would the operator receive at waist level standing 3 feet from the patient?
Approximately how much exposure at waist level would the operator receive with 5 minutes of fluoroscopy exposure standing 3 feet from the patient? (Hint: First convert mR/h to mR/min by dividing by 60; then multiply by minutes of fluoroscopy time.)
If a technologist receives 50 mR/h standing 3 feet from the mobile fluoroscopy unit, what would be the exposure rate if he or she moved back to a distance of 4 feet?
A technologist standing 1 foot from a mobile fluoroscopy unit is receiving approximately 400 mR/h. What is the total exposure to the technologist if the procedure takes 10 minutes of fluoroscopy time to complete?
Situation: An operator receives 25 mR/h to the facial and neck region with the C-arm in position for a PA projection (intensifier on top). Approximately how much would the operator receive at the same distance if the C-arm were reversed to an AP projection position (tube on top)?
True/False: The intermittent mode used during mobile fluoroscopy procedures is helpful during procedures to produce brighter images, but it results in significantly increased patient exposure.
Which single term best describes the primary difference between trauma positions and standard positioning?
What should be done to achieve specific projections if the patient cannot move because of trauma?
What is the minimum number of projections generally required for any trauma study?
How many joints must be included for an initial study of a long bone? ______________________
True/False: A follow-up postreduction radiograph of the middle portion of long bones should be collimated closely to the fracture region.
True/False: Digital radiography is well suited for emergency department (ED) and mobile procedures.
True/False: Nuclear medicine is effective in diagnosing certain emergency conditions such as pulmonary emboli.
True/False: For trauma patients who cannot be moved for conventional diagnostic imaging, other modalities, such as Diagnostic medical sonography (DMS) or nuclear medicine, may be used rather than trying to move the patient into specific positions.
What is defined as the displacement of a bone that is no longer within its normal articulation?
List the four regions of the body most commonly dislocated during trauma.
What is the correct term for a partial dislocation? ______________
A forced wrenching or twisting of a joint that results in a tearing of supporting ligaments is a
An injury in which there is no fracture or breaking of the skin is called a
What is the term that describes the associative relationship between the long axes of fracture fragments?
Which term describes a type of fracture in which the fracture fragment ends are overlapped and not in contact?
Which term describes the angulation of a distal fracture fragment toward the midline? Would this fracture angulation be described as a medial or a lateral apex?
What is the primary difference between a simple and a compound fracture?
List two types of incomplete fractures.
Which type of comminuted fracture produces several separate wedge-shaped fragments?
What is the name of the fracture in which one fragment is driven into the other?
List the secondary name for Hutchinson Fracture
List the secondary name for Baseball fracture
List the secondary name for Compound fracture
List the secondary name for Depressed fracture
List the secondary name for Simple fracture
True/False: An avulsion fracture is the same as a chip fracture.
What type of reduction fracture does not require surgery? ______________
Incomplete fracture with broken cortex on one side of bone only
Greenstick
Fracture resulting in multiple (two or more) fragments
Comminuted
Fracture of proximal half of ulna with dislocation of radial head
Monteggia
Fracture of distal fifth metacarpal
Boxer
Fracture of distal radius with anterior displacement
Smith
Intra-articular fracture of radial styloid process
Hutchinson Tibia
Fracture of the base of the first metacarpal
Bennett
Fracture resulting from a severe stress to a tendon
Avulsion
Indented fracture of the skull
Depressed
Fracture with fracture lines radiating from a center point
Stellate
Fracture of lateral malleolus, medial malleolus, and distal posterior tip of tibia
Trimalleolar
Fracture producing a reduced height of the anterior vertebral body
Compression
Complete fracture of distal fibula, frequently with fracture of medial malleolus
Potts
Fracture of distal radius with posterior displacement
Colles
Fracture of the pedicles of C2
Hangman
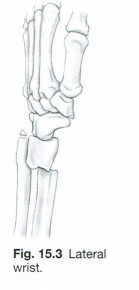
Which specific named fracture does Fig. 15.3 illustrate? Which bone is most commonly fractured, and which displacement commonly occurs with this fracture? Describe the type of injury or fall that commonly results in this type of fracture.
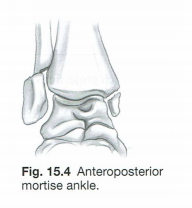
A. Which specific named fracture does Fig. 15.4 illustrate? Which bone(s) is (are) commonly fractured with this type of fracture?
How is the CR centered and aligned in relation to the sternum for an AP portable projection of the chest?
A. A recommended collimation field size of 14 x 17 inches (35 x 43 cm) should be placed ________________________ (landscape or portrait) for an AP portable chest on a sthenic or hypersthenic patient. Why? ________________________
True/False: Focused grids are recommended for mobile chest projections.
Which position can be used to replace the right anterior oblique of the sternum for the patient who cannot lie prone on the table but can be rotated into a semisupine position?
How must the grid be aligned to prevent grid cutoff when angling the CR mediolaterally for an oblique projection of the sternum when the patient cannot be rotated or moved at all from the supine position?
Other than the straight AP, what other projection of the ribs can be taken for the supine immobile patient who cannot be rotated into an oblique position?
Which of the following positions or projections best demonstrates free intra-abdominal air for the patient who cannot stand or sit erect?
Which of the following projections of the abdomen most effectively demonstrates a possible abdominal aortic aneurysm?
What is the disadvantage of performing a PA rather than an AP projection of the thumb?
Which projections are taken for a postreduction study (casted) of the wrist?
True/False: A PA horizontal beam projection of the elbow can be taken for a patient with multiple injuries.
True/False: For a trauma lateral projection of the elbow, the CR must be kept parallel to the interepicondylar plane.
Situation: A patient with a possible fracture of the proximal humerus enters the emergency room. Because of multi-ple injuries, the patient is unable to stand or sit erect. What positioning routine should be performed to diagnose the extent of the injury?
Situation: A patient with a possible dislocation of the proximal humerus enters the emergency room. Because of multiple injuries, the patient is unable to stand or sit erect. In addition to a routine AP projection, what second pro-jection demonstrates whether the condition is an anterior or posterior dislocation?
An AP oblique (scapular Y) projection taken AP supine for a trauma patient usually requires a ________.-° rotation of the body away from the image receptor.
How much CR cephalic angulation should be used for an AP axial projection of the clavicle on a hypersthenic patient?
To ensure that the joints are opened up for an AP projection of the foot, how is the CR aligned?
Situation: An orthopedic surgeon orders a mortise projection of the ankle, but the patient has a severely fractured ankle and cannot rotate the ankle medially for the mortise projection. What can the technologist do to provide this projection without rotating the ankle?
Situation: A patient with a possible dislocation of the patella enters the emergency room. What type of positioning routine should be performed on this patient that would safely demonstrate the patella?
Situation: A patient with a possible fracture of the proximal tibia and fibula enters the emergency room. The routine AP and lateral projections are inconclusive. Because of severe pain, the patient is unable to rotate the leg from the AP position. What position or projection could be performed that would provide an unobstructed view of the fibular head and neck?
To provide a lateral view of the proximal femur, which of the following projections would be performed on a trauma patient?
How must the IR and grid be positioned for the inferosuperior (axiolateral) projection for the hip?
Which of the following projections demonstrates the odontoid process for the trauma patient who is unable to open the mouth yet can extend the skull and neck? (Subluxation and fracture have been ruled out.)
Situation: A patient with injuries suffered in a motor vehicle accident enters the ED. The emergency room physician orders a lateral C-spine projection to rule out a fracture or dislocation. Because of the thickness of the shoulders, C6–C7 is not visualized. What additional projection can be taken safely to demonstrate this region of the spine?
Situation: A patient with a possible C2 fracture enters the emergency room on a backboard. The AP projection does not demonstrate C2. In addition, the patient cannot open his mouth because of a mandible fracture. Which projection can be performed safely to demonstrate this region of the spine?
Which projection will best demonstrate (with only minimal distortion) the pedicles of the cervical spine on a severely injured patient?
Identify the two CR angles for the AP axial trauma oblique projections of the cervical spine.
True/False: A grid must be used with the AP axial trauma oblique projection for the cervical spine to reduce scatter radiation reaching the IR.
Situation: A patient with a possible basilar skull fracture enters the ED. The emergency room physician wants a projection that best demonstrates a sphenoid effusion. The patient cannot stand or sit erect. Which of the following projections would achieve this goal?
Which of the following projections of the skull would project the petrous ridges in the lower one-third of the orbits on a supine trauma patient?
True/False: The CR should not exceed a 30° caudad angle for the AP axial projection of the cranium to avoid excessive distortion of the cranial bones.
True/False: AP projections of the skull and facial bones will increase exposure to the thyroid gland as compared to PA projections.
How is the CR angled and where is it centered for the AP acanthioparietal (reverse Waters) projection of the facial bones?
What type of CR angulation is required for the trauma version of an axiolateral projection of the mandible?
Situation: A patient with a Monteggia fracture enters the emergency room. Which of the following positioning routines should be performed on this patient?
Situation: A patient with a possible greenstick fracture enters the emergency room. What age group does this type of fracture usually affect?