Physiology Lab Exam #2
1/62
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
63 Terms
Skeletal Muscle
voluntary and requires a stimulus to contract
Latent Period
the length of time between stimulation of the fiber and the actual contraction is directly proportional to the weight
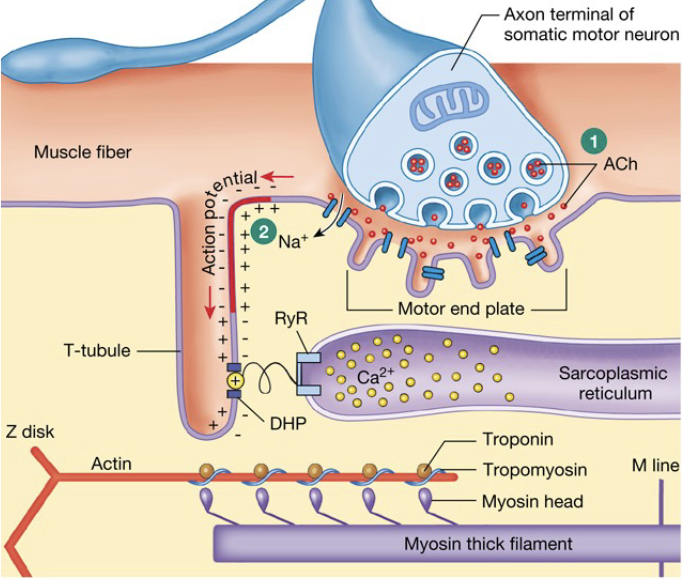
AP travels down the T-tubules
Voltage sensor triggers opening of Ca2+ gate
Ca2+ release from SR
Ca2+ diffuses and binds to troponin
Troponin pulls tropomyosin away
Cross-bridges can be formed and tension generated
Contraction period
once the weight is overcome, the muscle can contract
this is an active state is finite, heavier weight = less time the muscle has to shorten
binding site = troponin and is blocked by tropomyosin
AP depolarizes cell → travels down T-tubules
Ca2+ enters cell (via diffusion through channel, fast); binds to troponin → rolls and exposes binding site
Troponin pulls tropomyosin off of binding site
cross-bridges are formed and start the power-stroke cycle
Ca2+ is pumped back into the SR → pump is slow
Energy for Contraction
Must have ATP: power-stroke cycle, active transport of [Ca2+] into SR, Na+/K+/ATPase pump to replace Na+/K+ from AP
Phosphocreatine
Anaerobic glycolysis: glycolysis (Cori/Lactate Cycle)
Aerobic metabolism: glycolysis, citric acid cycle, ETS
both phosphocreatine and anaerobic glycolysis produce ATP in low [O2] env.
Relaxation period
muscle fiber relaxes
Ca2+ ATPase pump removes Ca2+ from cytosol, continually pumping it back into SR
once free, Ca2+ is removed, Ca2+ releases from troponin
Troponin allows tropomyosin to slip back over actin binding site
cross-bridges can no longer be formed
muscle is relaxed
Muscle Twitch
all events from the action potential, latent period, contraction, and relaxation.
Isotonic contraction
when a weight is lifted, and the muscle shortens, and the tension that develops in the muscle remains constant
tension is the same, muscle length changes
Isometric contraction
Same length, different tension
If the muscle fiber is not allowed to shorten (weight too heavy, equal and opposite force applied or muscle is restrained), tension builds but no movement
Factors that determine muscle strength
Ultimately, the determining factor for muscle strength is the number of cross-bridges formed→ actin and myosin binding
motor unit recruitment
changes in initial length
mechanical summation
Motor Unit Recruitment
accomplished by stimulating the gastrocnemius muscle with stimuli of progressively increasing strength
once all motor units have been recruited increasing the strength of the stimulus will not result in a larger contraction
How does an electric current spread through the muscle during the latent period?
connective tissue
muscle fiber cell membrane
stimulate the release of calcium within the muscle fibers
the time required for the muscle to overcome inertia (internal and external) and begin to contract
Graded contractions of skeletal muscle
changing the strength of the muscle contraction or the extent of shortening in proportion to the load placed on the muscle
skeletal muscles are able to react to different loads → e.g. load of walking on level ground < climbing stairs
What controls the degree of skeletal muscle contraction?
the activation of the desired number of motor units within the muscle
motor unit
motor neuron and all the muscle fibers it innervates
each muscle fiber is only innervated by a single motor neuron, but each motor neuron may innervate more than one muscle fiber
the size of a motor unit is designed by a ratio relating one nerve fiber to the number of muscle fibers it innervates → e.g. 1:50
Finer movement of fingers calls for 1:1, movement of thigh muscles for large movements are 1:1000
What law does a muscle fiber follow
the all-or-nothing
this means that if the stimulus is strong enough to produce any response in the fiber the response will be maximal
Stimulation and muscle contractions
not all muscle fibers have the same threshold for stimulation
as the strength of the stimulus is increased there will be a minimum stimulus required to get an observable response → threshold stimulus
Beyond this point any increase in stimulus strength will result in an increase in the force of contraction of the whole muscle. A stimulus that is just strong enough to elicit the most forceful contraction
that the muscle is capable of generating is known as the maximal stimulusStimuli of greater intensity that do not cause any further increase in muscle contraction are known as supramaximal stimuli
Work
the application of a force which results in the movement of an object.
skeletal muscles perform mechanical work
Work (g x cm) = weight lifted (g) x actual distance (cm)
How much work a given muscle can perform is dependent upon the length of the muscle prior to contraction
How is optimal muscle length determined
for each muscle there is an optimal length at which the most work can be done.
This optimal length is determined by the degree of overlap of actin and myosin filaments within the sarcomere of muscle fibers
Mechanical summation
If the muscle is stimulated with a second adequate stimulus before the
response to the first is completed (i.e. muscle contraction fully relaxes), the second twitch will add its mechanical effect to the first.This produces a stronger contraction than that produced by a single stimulus.
Physiologically, smooth graded contractions of skeletal
muscle are produced by mechanical summation of fiber twitches that occur when fibers twitch synchronously so that some are in the process of contraction before others have had time to completely relax.
Incomplete tetanus
If stimuli are repeated at a rapid enough intervals or frequency, the
individual twitches will fuse into a state known as incomplete tetanus.Incomplete tetanus is characterized by only a slight relaxation between muscle contractions
Complete tetanus
If the frequency is high enough to not allow any relaxation, complete tetanus will be achieved (a state of constant contraction).
Skeletal Muscle fatigue
If the state of tetanus, be incomplete or complete, is allowed to continue the muscle will eventually fatigue.
fatigue occurs as the muscle uses energy at a rate faster than energy, in the form of ATP, can be generated by cellular metabolism.
Fatigue is also caused by a build-up of metabolic waste products (carbon dioxide, lactic acid) some of which directly interfere with the contractile process.
Normally, the circulatory system removes these metabolic wastes. But, in this preparation, the muscle has been separated from its blood supply and will, therefore, fatigue quickly
Sarcomere
repeating unit of a muscle fiber
the same banded appearance from which the name striated muscle was derived
Slow Twitch, Aerobic
these muscles are weak and fatigue resistant
Fast Twitch, Glycolytic
strong muscles, but fatigue quickly
Muscle Fiber Types: Fast-Twitch and Slow-Twitch
This designation is determined by the type (or isoform) of myosin, the rate of ATPase activity and cross-bridge binding each muscle fiber possesses.
Within the group of fast twitch muscle fibers there are those that use glycolysis and oxidative phosphorylation, and others that only use glycolysis.
This latter group is less reliant on oxygen and much stronger than the former type. However, the stronger glycolytic fibers break down glucose very inefficiently, so the burst of contractile activity in these muscle fibers soon fatigue, glucose levels diminish and lactic acid accumulates.
Muscles that are composed of mostly fast glycolytic fibers (sometimes referred as white muscle fibers) are good for sprinting and jumping high, but not for sustaining activity.
muscle twitch
a single contraction followed by relaxation
Wave Summation = Mechanical Summation
Human skeletal muscle lab
If a muscle repeated stimulated quickly, the amount of cytoplasmic calcium will increase faster than the calcium pumps can remove it.
This increase in frequency will cause a continuous formation of cross-bridges.
This accumulation of calcium and cross-bridge number is referred to as mechanical summation (or Wave Summation).
Electromyogram (EMG)
The electrical activity in the motor units during a muscle contraction can be recorded as bursts of muscle action potentials that are
collectively known as an electromyogram (EMG).The strength of a striated muscle contraction is directly proportional to the amount of electrical activity in the muscle
EMG Graph
One of the most common transformations used is the integration of the absolute values of the amplitudes of the EMG spikes.
Through this transformation, it has been found that the area under the graph of the absolute integral of the EMG is linearly proportional to the strength of the muscle contraction
Muscles and Movement of body parts
In the skeletal system, muscles work together with bones to create a system of levers that move a body part.
In a lever, the muscle in anchored on a stationary bone at a point known as the origin.
The muscle provides the effort or force that moves
bone that is the lever.The point of attachment of muscle on the lever is known as the insertion.
As the muscle contracts and relaxes, the bone, functioning as the actual lever, rotates around a joint in the skeletal system. The joint is the fixed point that functions as the fulcrum for the lever. The body part being moved is the load on the lever.
flexors
muscles that move body parts toward the body
extensors
muscles that move body parts away from the body
antagonistic muscles
Flexors and extensors that work on the same lever or body part are known as antagonistic muscles.
When performing a function, like throwing a baseball, muscles in various parts of the body relax and contract in a coordinated manner to accelerate and release the ball at the right moment.
What can influence cardiac contractions?
neural, chemical, and thermal influences
refractory period
interrupting impulse conduction
the rate of contraction can be modified by impulses which reach the heart via autonomic nerves, or by chemical substances, like certain hormones and metabolites.
change in temperature affects the rate at which ions move in and out of heart muscle cells and thereby affect the rate of depolarization and repolarization of the cells. Thus, a change in temperature of the heart will cause a change in heart rate and force of contraction
Frog Heart
two atria, one ventricle
pacemaker cells are in sinus venosus (a contractile heart chamber which delivers blood to the right atrium) rather than the SA node
no distinct AV node, differs from humans
still a group of conducting cardiac cells that communicate with the ventricle
Autorhythmicity
an inherent capacity to contract
This contraction is initiated by the autorhythmic depolarization of specialized muscle tissue, called pacemaker cells.
This allows the heart to beat, at least for some time, even though cut free from its blood and nerve supply.
Therefore, we can observe the function of a frog heart for some time after its central nervous system is destroyed
Absolute refractory period
occurs after depolarization
muscle can’t be re-stimulated during this time-period
long compared to skeletal muscle → allows time to move the blood through the heart efficiently and prevent the heart from ever reaching a state of fatigue
Relative Refractory Period and Compensatory Pause
follows absolute refractory period
a strong electrical stimulus can elicit an early extra systole (new contraction)
Since the next naturally occurring depolarization will fall into the absolute refractory period generated by the new contraction, we will
observe a long pause that is called a compensatory pause following the extra systole
Heart block
a condition in which impulses fail to pass normally through the conducting system of the heart to the ventricular muscle → electrical event
partial block: If some, but not all impulses from the pacemaker
reach the ventriclesIf, however, no impulses from the pacemaker reach the ventricular muscle, the atria and ventricles beat independently of one another (in
mammals) and no consistent ratio between their rates of beating is seen. This is a complete heart block.in amphibians and reptiles, complete heart block usually results in no ventricular activity
The heart block is an electrical event, but it may eventually prevent blood from flowing within and around the heart due to its effects on the pumping of the heart
ECG: Electrocardiogram
records electrical activity of the heart
Will the heart ever fatigue? Why?
no
it does have a maximum rate. Stimulation beyond this
maximum will not result in any increase in rate.The reason for the heart muscle’s inability to fatigue is its long duration action potential. The absolute refractory period of the cardiac action potential is so long that the heart muscle (cardiac cells) has begun to relax and is totally relaxed before another stimulus can cause a contraction → gives heart time to fill before its next contraction.
Since the cardiac muscle will always be in the relaxed state prior to contraction it will not be able to accumulate inorganic phosphate, produce large amounts of lactic acid (which it can use as a fuel), or run out of ATP
Conditions of high heart beat
Tachycardia and fibrillation are two conditions in which there is a very rapid heart beat.
The heart can beat at these high frequencies without fatigue but becomes a very inefficient pump, thus not circulating enough blood and oxygen
How does KCl work to euthanize?
Remember that the KCl concentration inside the cell is high and
low on the outside.The addition of the KCl to the outside prevents diffusion of K+ out of the cell.
If K+ cannot flow out of the cell, the cell does not repolarize and if it cannot repolarize, it cannot fire again → the heart stops beating
Heart Sounds
When listening to the heart with a stethoscope, two heart sounds are typically heard although there are 4 (4 cardiac valves)
first sound is produced when the AV valves close during the beginning of ventricular systole. The valves themselves are not heard, but their closing causes blood in the ventricles to vibrate and produce sound. Since there are 2 valves you can hear them
separately.The second sound is produced when the semi-lunar valves close, and blood in the aorta and pulmonary trunk hitting these values vibrates.
The first sound is louder overall than the second sound and lasts longer, but the second sound has a more abrupt ending. The sounds are usually described as "Lub-Dup".
Where are heart sounds best heard?
The first sound is most easily heard where the apex of the left ventricle comes closest to the front of the chest wall, behind the fifth intercostal space on a line downward from the middle of the left clavicle.
The second sound is heard best close to either side of the sternum, at the level of the second intercostal space.
Sometimes it is possible to listen specifically for the result of action of a particular valve.
Blood Pressure
When blood is forced by ventricular systole (contraction of the heart) out the aorta and pulmonary trunk, it must overcome the pressure already present in the arterial system during the previous diastole (relaxation of the heart).
As the pressure in the left ventricle rises from near zero in diastole to a typical value of 120 mm Hg during systole, the pressure in the aorta rises to a similar value. As ventricular diastole begins, the closure of the semi-lunar valves keeps the pressure in the arterial system up.
In addition, the elastic energy stored in the arterial walls during
systole, squeezes inward on the blood during diastole. Also, since the arterial system is always full, there is no way for the pressure to drop as a result of fluid loss.All of these factors keep the diastolic pressure in the aorta from dropping, and is typically maintained at about 80 mm Hg. The
pressure in the pulmonary circuit is only about one-fourth of that in the systemic circuit.
Pulse Pressure
The difference between systolic pressure and diastolic pressure is pulse pressure and represents the extra force needed to overcome the resistance to flow created by the diastolic pressure.
The systolic pressure of 120 mm Hg and diastolic pressure of 80 mm would be expressed as 120/80
The difference between these values is 40 mm Hg, which would be the pulse pressure
MAP = Mean Arterial Pressure
An estimate of mean arterial pressure is one-third of the pulse pressure added to the diastolic pressure
(MAP = 1/3 pulse pressure + diastolic pressure) or [(SBP + DBP + DBP)/3] )
Factors that Influence Blood Pressure
age, gender, activity, posture, cardiac output, blood volume, peripheral resistance (degree of vasoconstriction), and elasticity of the arterial walls resulting from disease.
How does the body respond to blood pressure changes?
First, the control centers in the brain must realize that there are changes occurring. Stimuli that are used to signal these changes in
demand happen locally (like Oxygen use, CO2 production and pH) and some systemically (changes in blood pressure, Baroreceptor Reflex).Baroreceptors in the carotids bodies located in the bifurcation of the carotid arteries of the neck sense these changes and increase or decrease their activity.
These changes are monitored by the integrating center in the medulla. Since maintaining blood pressure is under homeostatic control (negative feedback loop), the integrating center sends out signals that will adjust blood pressure.
The circulatory system makes adjustments by a combination of increased cardiac output (usually faster heart rate or greater stroke volume, usually faster heart rate), and increased vasoconstriction.
CO = HR x SV; Flow ~ CO ; CO ~ MAP / R; MAP ~ CO x R
manometer
measurement of blood pressure that requires an inflatable cuff with associated tubing, pressure gauge, and pumping bulb
The knob on the inflating bulb should be turned clockwise to close off
the bulb from the air, and when the bulb is repeatedly squeezed, air will be forced into the cuff.When the manometer indicates a cuff pressure that you feel will be higher than the subject's systolic pressure, turn the knob very slightly counter-clockwise, so as to let the pressure gradually drop. (usually down 2-3 mm for each heart beat).
After each reading, turn the valve completely counter- clockwise so that the pressure drops to zero.
Do not leave the cuff inflated for more than one or two minutes at a time, as this may cause an elevation of the subject's blood pressure to compensate for lack of flow.
Sphygmomanometer - Palpatory method
measurement of blood pressure that requires an inflatable cuff with associated tubing, pressure gauge, and pumping bulb
Locate the radial pulse in the wrist by feeling with the tips of 2 or 3
fingers (not the thumb) for the radial artery, which lies close to the radius bone.Once the pulse is located, inflate the cuff to a value above systolic pressure. The pressure in the cuff, now being higher than systolic pressure, will block the brachial artery in the upper arm, so that the radial pulse will disappear.
As the pressure is allowed to decrease, at some point the pulse will once again appear – this is the systolic pressure. Note that as the pressure is allowed to go down to zero, the pulse continues to be felt.
Thus, no estimation of diastolic pressure can be made. Make
two determinations of systolic pressure by this method.
Auscultatory method
Use of a stethoscope in conjunction with a sphygmomanometer is the usual method of determining both systolic and diastolic pressure.
The cuff is placed around the upper arm as in the palpatory method, and inflated to a pressure above that of systolic pressure.
As before, allow the cuff pressure to drop gradually, while listening in the inside bend of the elbow for a series of sounds (Korotkof sounds) caused by vibration of the blood in the brachial artery.
With the cuff above systolic pressure, no blood can pass the obstruction, and no sounds are heard.
When cuff and systolic pressures are equal, a small amount of blood is forced through the artery, and a "tapping" noise is heard. Record this as the systolic pressure.
As the cuff pressure continues to decrease, the sounds become louder, and begin to have a kind of "blurred" component added. At lower pressures yet, the sounds become clear "taps" again, which either suddenly drop in loudness or more often, fade away to a point no longer audible. Record this latter value as the diastolic pressure.
Note that sounds are heard between systolic pressure and diastolic pressure, but neither above nor below these values.
After each determination, the pressure in the cuff must be allowed to return to zero, so as not to interrupt the blood supply to the lower arm for lengthy periods of time.
Tension: hyper and hypo
high blood pressure or hypertension is considered to be
systolic pressure above 160 or diastolic pressure above 90 mm Hg. It may produce few noticeable symptoms if borderline.Continued high pressure may lead to a variety of renal and cardiovascular problems.
Low blood pressure or hypotension may result in insufficient blood flow to the head when suddenly assuming more erect positions, and consequent dizziness or fainting
Cardiovascular Responses to Changes in Posture and Exercise
anatomical features
Body is designed with several anatomical features that allow for blood to be pushed back to the heart
One is the muscles in our legs that surround veins. Veins are able to be compressed and when muscles contract they squeeze vessels and the blood that is inside them.
These veins are designed with one-way valves that open to let
blood move toward the heart but close prevent blood from going backward.The thoracic cavity and abdominal cavity are separated by the diaphragm thus the thoracic cavity is closed.
When one takes a deep breath this cavity is expanded lowering the pressure in comparison to the abdominal cavity. This acts as a suction to pull blood back up toward the heart.
Cardiovascular Responses to Changes in Posture and Exercise
Physiological mechanisms
The amount of blood per beat can be altered (stroke volume), the number of beats in a given period can be changed (heart rate) and the size of the arterial vessels can be changed (resistance to flow varies).
So, the ability of a person to provide adequate blood flow to the head while standing over an extended period of time may differ from one person to the next. Contraction of leg muscles can assist in venous return during standing thus pushing blood up to the heart against gravity.
Some subjects can maintain adequate pressure to the head by vasoconstriction alone, without much assistance from an increase in heart rate or muscle activity.
Others must increase heart rate a great deal or stroke volume. Some may shift from early vasoconstriction to later an increase in heart
rate.
Measurement of Venous Pressure
Venous pressure (the pressure of the blood entering the right atrium)
can be estimated indirectly (although not very accurately). Have a subject stand beside the blackboard, and make a chalk mark at the approximate level of their right atrium. (This is approximately a hand's width below the clavicle.)Locate a vein on the back of the hand that can be easily seen when the hand is about at waist level. Then lift the hand vertically from a position below the chalk mark, upward until the vein is seen to collapse. Mark this level with a second chalk
mark. Measure the vertical distance between the marks and record.From the vein in the hand through larger veins down to the right atrium serves as a "manometer", but with blood instead of mercury. Since mercury is 13.5 times heavier than blood, your measurement must be divided by 13.5 to get the venous pressure in mm Hg
Electrocardiogram (ECG)
Because body fluids are good conductors, sensitive electrodes
placed on the body surface can record the fluctuations in electrical potentials that represent the sum of the action potentials of myocardial fibers if the rest of the muscles are kept still. The recording of these potential fluctuations is called ECGThe heart's basic rhythm is set by impulses that are generated by depolarization of cells in the sinoatrial (SA) node, or pacemaker
This depolarization spreads over a conductive
system of specialized muscle cells and over the atria. The atria respond with contraction of the myocardial cells.The propagation of depolarization via the conductive system then reaches the atrioventricular (AV) node, where it is delayed for 200 ms in order to give time for the atrial blood to flow into the ventricles.
It then continues quickly over the bundle of His and then spreads
over the ventricles via the Purkinje fiber. Next, the ventricles respond with contraction to eject the blood
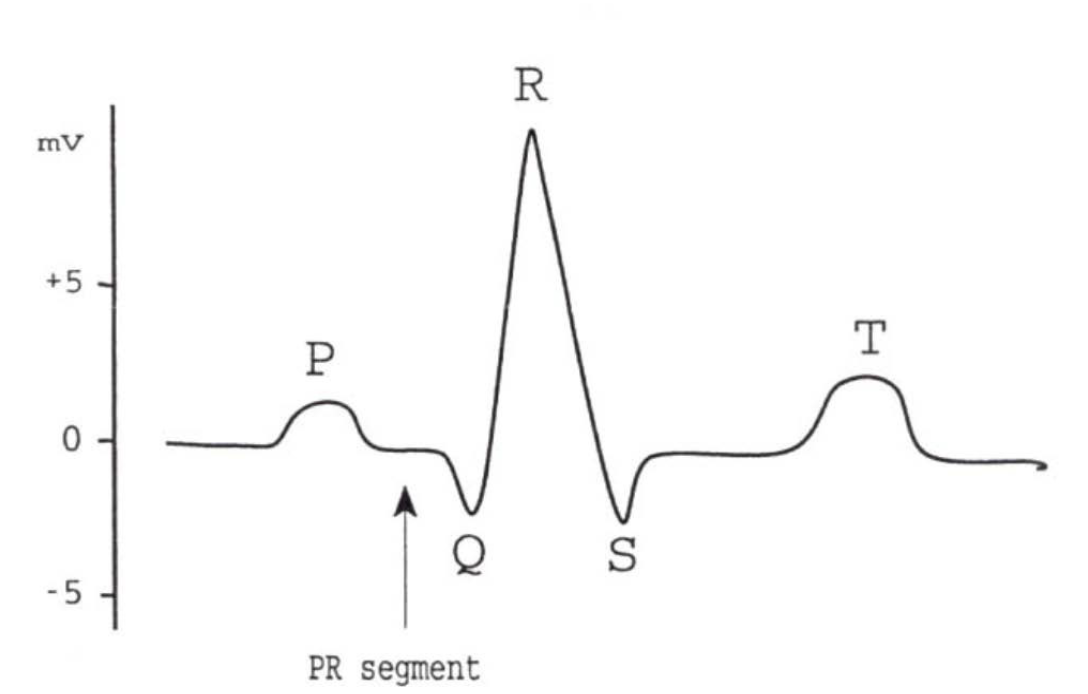
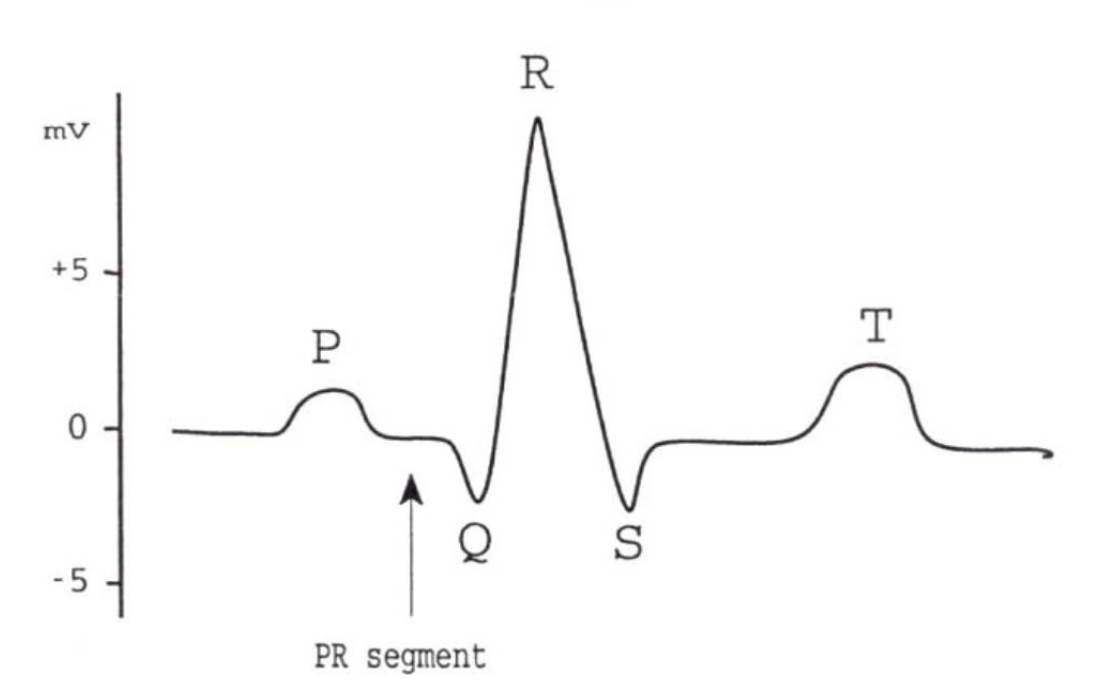
ECG Graph and its elements
P wave: time of depolarization of the atria. An abnormal shape of the P
wave might indicate abnormal atrial function.P-R segment: AV delay, impulse travels over bundle of His and Purkinje fibers. A longer segment might indicate malfunction of the AV node or bundle of His. If the P-R segment is abnormally long, the impulse will probably not pass properly onto the ventricles. This is called a first-degree heart block.
QRS: This interval coincides with the depolarization and contraction of the ventricles. If a P wave is not followed by a QRS wave, and only some impulses from the SA node activate the AV node, this is a second degree heart block. If there is no relation between the P and QRS wave, this is called a third degree heart block.
ST segment and T- wave: These coincide with the repolarization of the ventricle
sinus arrhythmia
can be detected in an ECG.
It can be detected as periods of fast heart rate followed by periods of slow heart rate.
This condition is common in young people, but generally of no clinical significance.
The rate is also slower when a person exhales and faster during inhalation
tachycardia
A heart rate of 100 beats per minute is called tachycardia. This is normal during exercise but abnormal during rest.
bradycardia
The opposite, a slow heart rate below 60 beats per
minute, is known as bradycardia.Often times trained endurance athletes have a low heart rate - they have a large stroke volume to compensate for this.