Looks like no one added any tags here yet for you.
Bones
Tibia and Fibula
Articulations
Tibiofibular joints
Superior (proximal) and inferior (distal)
Syndesmosis joint (distal only)
Ligaments
Superior & inferior and posterior tibiofibular ligaments
Also interosseus membrane
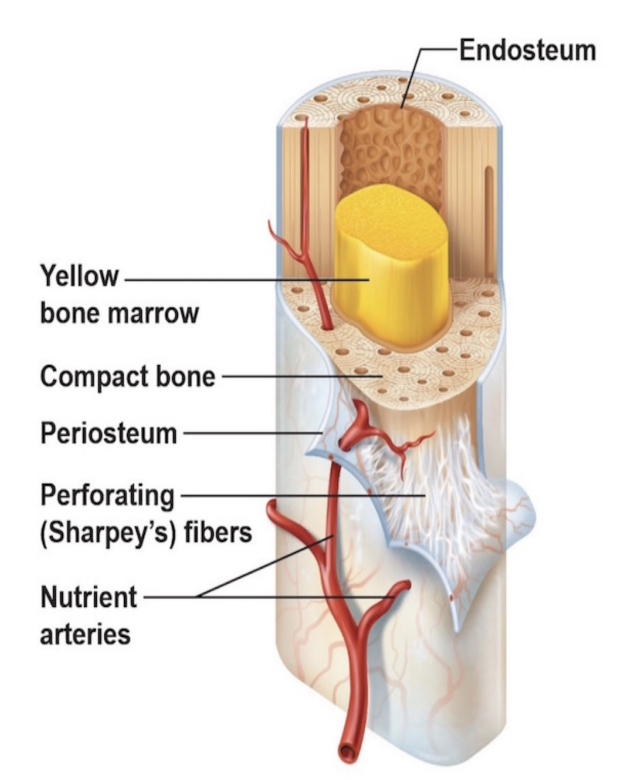
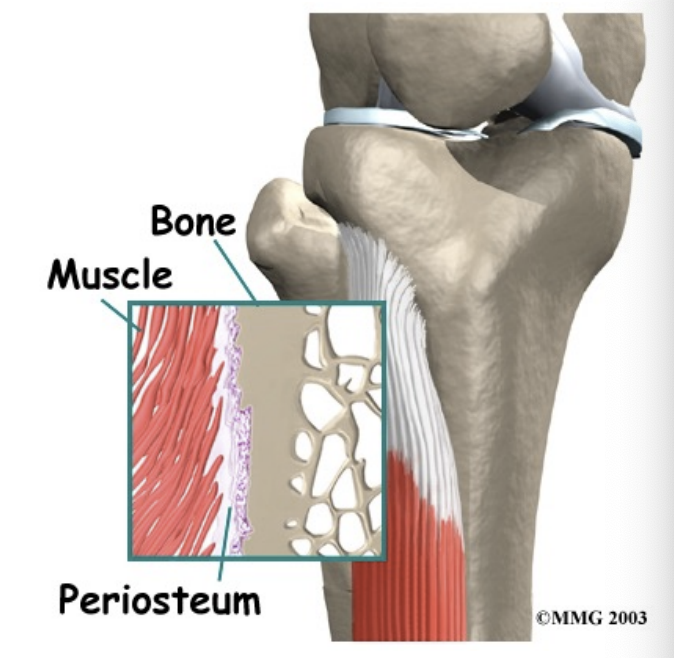
Periosteum
Forms the outer surface of bone and endosteum lines the medullary activity
Periosteum: Outer Fibrous Layer
Contains blood vessels, nerves, lymphatic vessels that nourish bone
Contains sharpey’s fibres that attach periosteum to bone AND ligaments and muscle tendons to bone
Periosteum: Inner Cellular Layer
Responsible for bone repair and growth
Cells it contains are osteoblasts which lay down new bone cells as bones grow or repair when damage
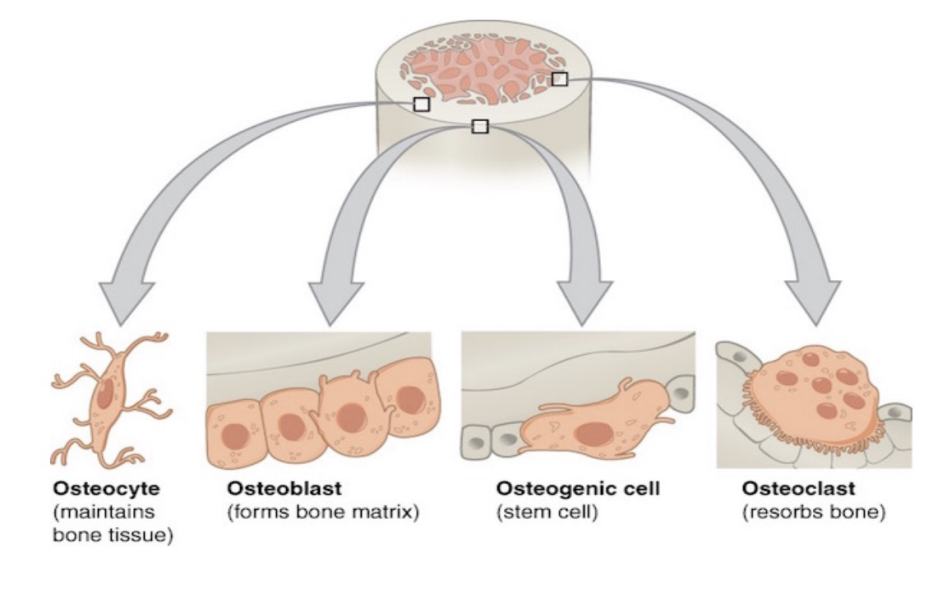
Bone cells
Osteocyte
Osteoblast
Osteogenic order
Osteoclast
Osteocyte
Maintains bone tissue, release calcium (becomes trapped)
Osteoblast
Forms bone matrix
Osteogenic cell
Stem cell
Osteoclast
Reabsorbing old bones (responds to stress)
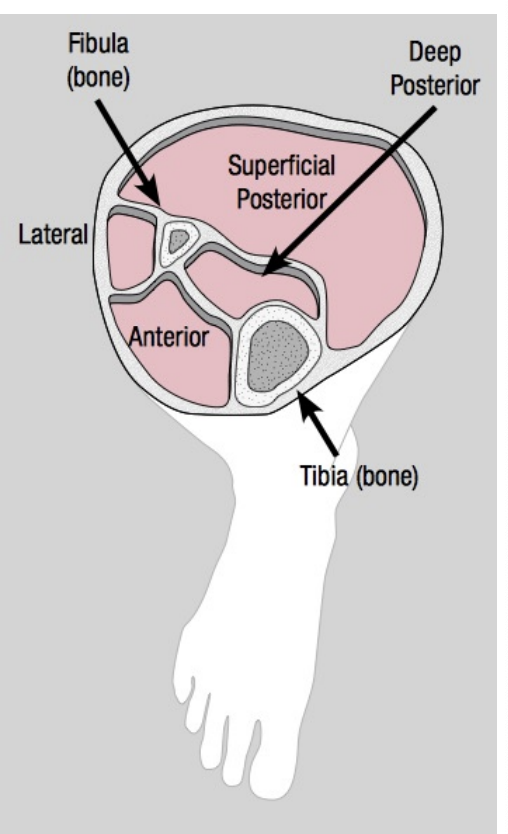
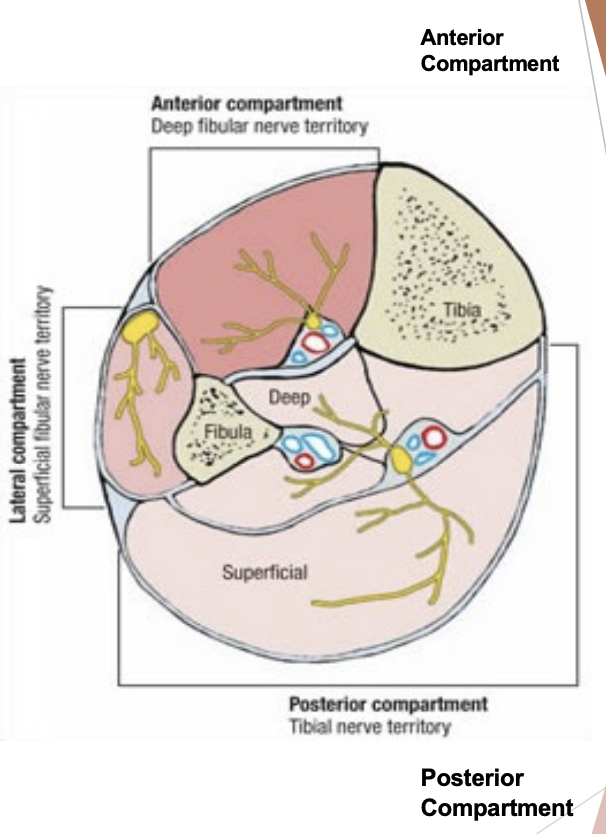
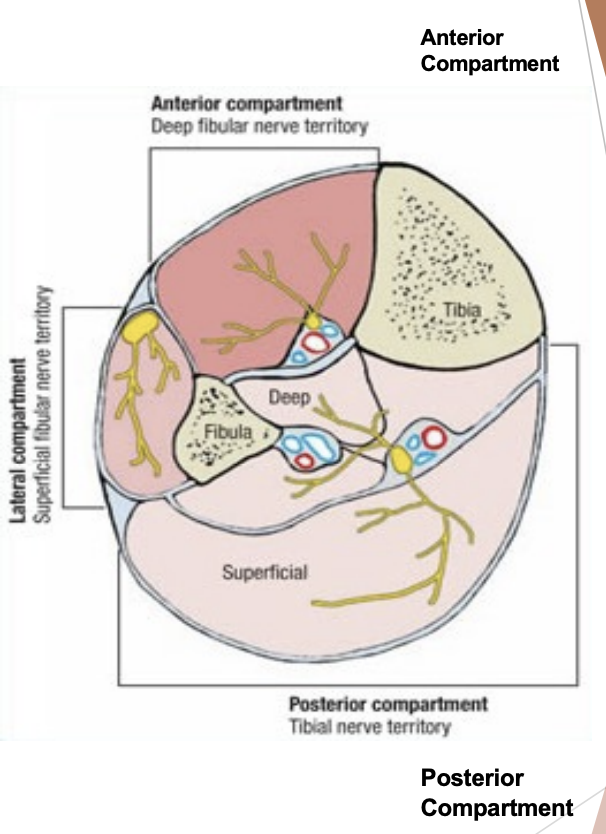
Compartments
Anterior Compartment
Muscles for dorsiflexion, toe extension
Anterior tibial artery, deep peroneal nerve
Tight
Posterior Compartment
Loose
Plantarflexors, inverters, toe flexors
Posterior tibial artery, tibial nerve
Lateral
Everters (peroneal muscles), superficial peroneal nerve
Interosseous membrane
Forms posterior border for anterior compartments. Holds bone together “tough tissue”
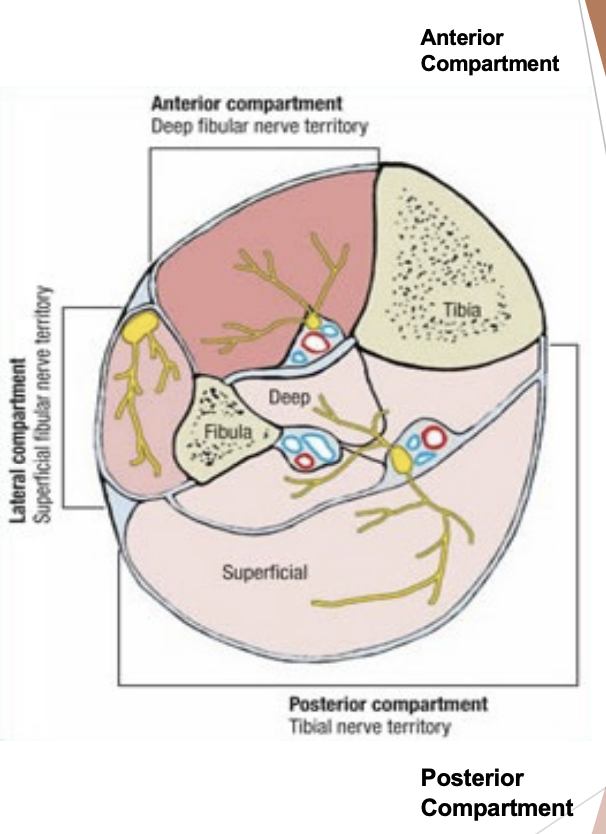
Anterior compartment of lower leg
Tibial anterior, EHL, EDL, deep peroneal nerve, anterior tibial artery
Superficial posterior compartment of lower leg
Gastrocnemius and soleus
Deep posterior compartment of lower leg
Tibialis posterior, FHL, FDL, tibial nerve, posterior tibial artery
Lateral compartment of lower leg
Peroneus longus and brevis, superficial branch of peroneal nerve
Contusion
History: Direct blow
Symptoms: Pain, tenderness, swelling, bruising, disability
Diagnosis: fracture
Treatment: POLICE, Padding, ROM, strengthening, ROM, Physio?
Complication: Anterior compartments syndrome
Strain
History: Sudden stop or start
Most common = Gastrocnemius and soleus muscolotendinous junction or medial soleus/ tibialis posterior/ posterior/ FDL muscle belly
Symptoms: Pain(increased with movement), Tenderness, step deformity, Bruising, Limp, snap wth 2nd or 3rd degree injury and resisted ROM
Treatment: POLICE, taping, phyio, ROM exercises, rehab, ice compression and crutches
Achilles Tendinopathy
The term referred to achilles tendon: tendon is overloaded in some way
Symptoms: Pain and stiffness, tendon feels warm. Weakness with resisted plantar flexion(toe raises), morning stiffness or after sitting for prolonged period of time. Chronic = thickening of tendon
Treatment: Must reduce stress on tendon. Address any biomechanical issues, footwear, orthotics, Ice to decrease inflammation, ultrasound increase blood flow, cross friction massage, eccentric program
Achilles Tendinitis
Acute inflammation of achilles tendon
Achilles Tendinosis
Most people with achilles tendon pain have achilles tendinosis. No inflammatory cells present, collagen fibres in achilles tendon are disorganized, scarred, degenerated
Achilles tenosynovitis
Inflammation of achilles tendon sheath, causes fibrosis and scarring that restricts tendon’s motion within the sheath = stiffness
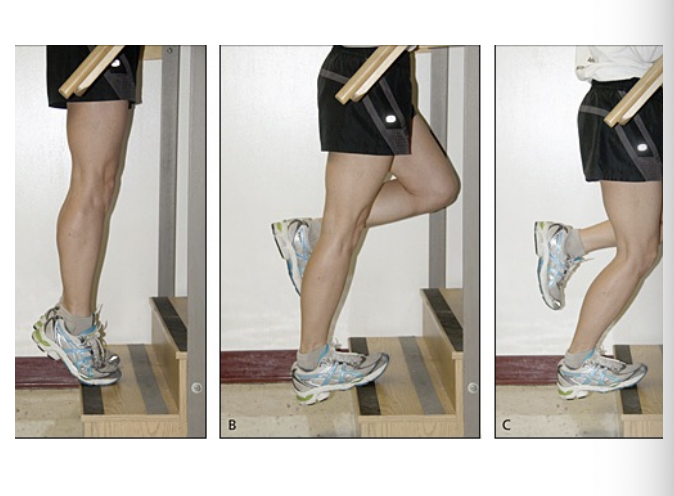
Eccentric Loading Program for Achilles Tendinopathy
Assisted raising onto both feet
Weight transferred to injured leg
Non-assisted lowering
Starting with 1 set of 10 reps, increasing to 3 to 5 sets of 10 reps
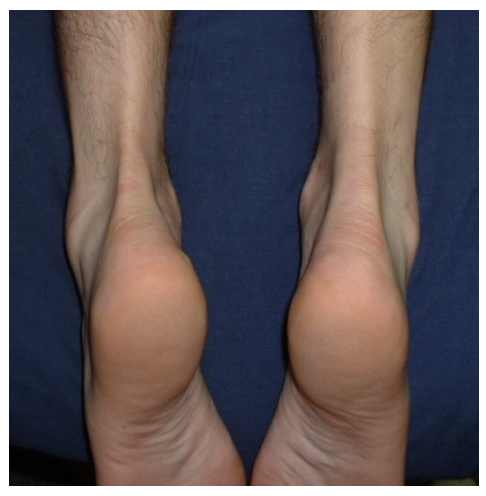
Achilles Rupture
History: Associated in stop and go sports, Usually 30 or older athletes. Associated history of chronic inflammation, achilles tendinopathy
Symptoms: Snap, pop, feeling like kicked, point tenderness, discolouration, swelling. Toe raising impossible on injured side and indent, positive Thompson test
Treatment: Referral to hospital ASAP, if surgery, needs to be done very soon, POLICE, walking boot 12 weeks
Exercise Induced Lower Leg Pain
Medial Tibial Stress Syndrome
Stress Fracture
Chronic Extertional Anterior Compartment Syndrome
Contributing Factors:
Poor running mechanics
Inappropriate footwear
Foot shape and biomechanics
Lower limb structural abnormalities
Muscle tightness and imbalance
Poor conditioning/ overweight
Inadequate warm-up and training errors
Terrain and training surfaces
Stress Overload Cycle
Muscle Fatigue → Loss of Shock Absorption → Structural Stress to Bone → Remodelling Process → Pain → Voluntary or Involuntary Disuse → Muscle Inhibition/ Atrophy
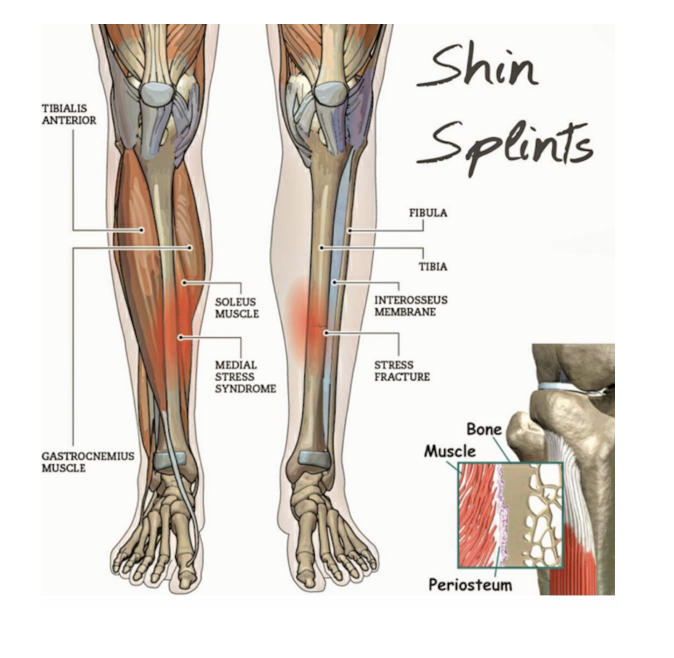
Shin Splints
Medial Tibial Stress Syndrome
General Characteristics
Syndrome (several causes such as periostitis, strains, cortical bone microfractures due to overuse)
Predispositions = hard surfaces, hard surfaces, poor footwear, obesity, heredity
Medial Tibial Stress Syndrome
Symptoms: Aching pain, worse with activity, Tenderness
Grade of Shin Splints:
Grade 1 - dull pain 2-3 hours after activity
Grade 2 - pain before and after exercise, doesn’t affect performance
Grade 3 - pain before, during and after exercise, affects performance
Grade 4 - Severe pain, can’t participate
Medial Tibial Stress Sydrome Treatment
DDx: Stress fracture, Chronic anterior compartment syndrome
Treatment: Rest, NSAIDs, physiotherapy, Orthotics if needed, Correct other factors as needed and gradual return to activity
Tibial Stress Fractures
History: Overuse (running, jumping)
Symptoms: Aching pain, worse with exercise, possible history of high mileage, speed, hard surface training, Tenderness (focal), X-Ray positive (but many have fracture and negative X-Ray at first). Bone scan positive (SENSITIVE; not specific to fractures however)
DDx: Shin Splints
Treatment: Adequate rest (Walking boot? Cast? Walk only?), Correcting of etiologic factors, Alternating of etiologic factors, Alternate program for fitness and slow return to activity as tolerated
Bone Fracture
The concept of a stress fracture is a healing failure continuum. Normal bone -Stress reaction → Stress Fracture → Full (Acute) Fracture. Osteoclastic activity → Osteoblastic activity. Decreased bone mass perpetuates the problem
Anterior Compartment Syndrome Causes + Symptoms
=ischaemia of muscles
Causes: Internal volume: Hemorrhage from fracture, swelling from burns, contusion, tumour. External: Decreased volume: tight casts, bandage dressing. Overuse(excessive running)
Symptoms: Pain(deep,”boring”) worse with exercise, slow to resolve(around 5-10 min), Tenderness, Weakness (Dorsiflexion, Toe Extension), Numbness(area of between 1st of 2nd toe). Diminished circulation (Dorsalis artery)
5 P’s Of Compartment Syndrome Symptoms
Pain: Out of proportion for their injury, pain with rest or with passive stretch in suspect compartment
Paresthesias: May be earliest subjective complaint due to increase pressure on nerve in tight compartment
Paralysis: Also sign of muscle and nerve dysfunction, difficult to differentiate from muscle guarding as a result of pain
Pallor and Pulselessness: Implies arterial insufficiency. Once pulses are diminished, the damage has been done
Compartment Syndrome: Pain
Pain with passive muscle stretching
Pain out of proportion relative to injury
Progressive
Not relieved by immobilization
Anterior Compartment Syndrome Treatment
Chronic Exertional Compartment Syndrome
Adequate rest
Correct predisposing factors
Physician to access and monitor
Physiotherapy
Slow return to activity as tolerate
Acute (Acute & Acute Exertional Compartment Syndrome)
Potential surgical emergency
NPO & transport to MD ASAP
May need fasciotomy
Then treat otherwise as for chronic
Compartment Pressure Testing
Most widely used diagnostic criteria for determining chronic exertional compartment syndrome were pressure measurements of >15 mmHg before exercise, >30 mmHg at 1 minute after exercise & >20 mmHg after 5 minutes after exercise
Acute Fractures
Hx: Kick, Fall, Ankle Sprain
Symptoms: Pain, tenderness (focal), Bruising, swelling, Crepitus?, Deformity?
Treatment: Recognize, Stabilize, Transport to hospital