IMED2001 - Medically Important Parasites P2 (L15)
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
What will be covered in this lecture
- something that might be useful is that if something is enteric its likely they will be enteric pathogens, and if you know theyre non-invasive you can remember the symptoms (stomach upsets etc.)
- also you can predict how its identified (e.g faecal sample)
.
- likewise, if we know the parasite is deep in the body, we're going to look at the blood and we will look for antibodies
Protozoan parasites NAMING
- Giardia intestinalis - mild intestinal disease, global distribution
- Toxoplasma gondii - infects around 30% of the world's population - most successful parasite
- Malaria - highest morbidity and mortality for a protozoan pathogen
- Leishmania - most diverse disease phenotype

Giardiasis
The species names Giardia duodenalis, Giardia intestinalis, and Giardia lamblia are used interchangeably in current literature referring to the same organism." (Feng & Xiao 2011). However, G. intestinalis is considered the best one to use.
- this is an enteric parasite
.
- a gastrointestinal disease caused by the flagellate protozoan Giardia intestinalis
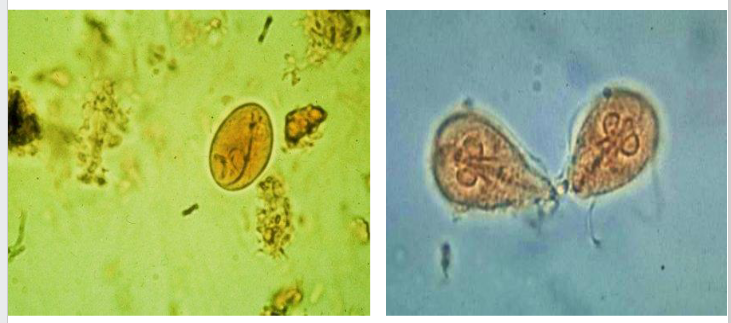
- worldwide distribution (more prevalent in warm climates)- 2 stages: Trophozoite and cyst
.
- any parasite that lives in your gut has to live in a feeding form, and thats what we call a trophozoite so this is the form that actively feeds on your gut (material thats passing by)
- but to go to the next person it has to enter the environment, and the way it does this is it enters a resilient stage called a cyst. The cyst is non-feeding. Its just a state that allows it to survive until the next person picks it up and then it can exist and go into the gut and become feeding again
.
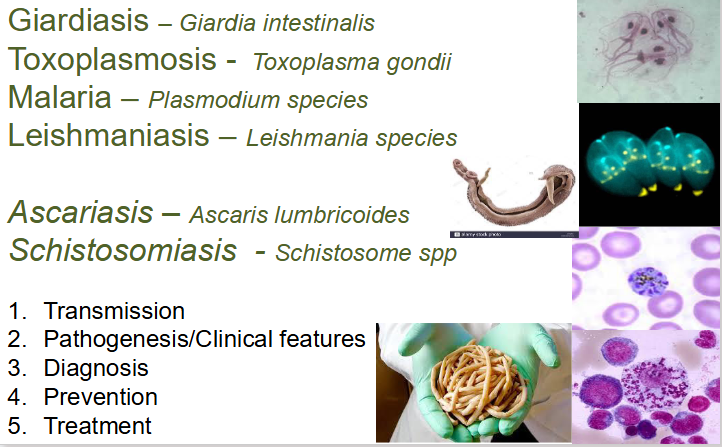
- interesting way to tell this virus is that it has a smiling face and it has 4 pairs of flagella

Symptoms of giardiasis
- Diarrhea
- Gas or flatulence
- foul smelling faeces
- greasy stools that tend to float (malabsorption of fat)
- Stomach or abdominal cramps
- Upset stomach or nausea
- Weight loss and dehydration possible
.
NON-INVASIVE: so no fever or significant immune response
HOWEVER, there are associations with post infectious reactive arthritis
.
- it sits in the gut and replicates quickly, meaning that it leads to lack of absorption as it absorbs things moving past
- leads to diarrhea as youre not absorbing that much water. not absorbing fat
- anything that doesnt invade likely doesnt cause fever
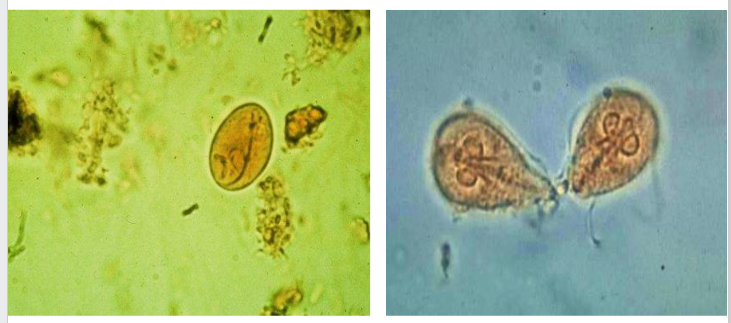
Giardia intestinalis DIAGRAM
- right shows the trophozoite phase, left shows cyst (when it moves into next host)
Epidemiology - Giardiasis
- In developing countries, there is a level of continual infection, common in children.
- Occurs all over the rest of the world
- All ages affected (many symptomatic adults as well as children)
- Transmission by food, person-to-person etc (common in day-care centres - e.g. Thompson 1994, Overturf, 1994, Nunez et al. 1999)
- Most big outbreaks are waterborne - In winter 2004/05 a large (~1500 cases) waterborne outbreak of giardiasis occurred in Bergen, Norway.
Giardiasis - Transmission
FAECAL-ORAL ROUTE VIA INGESTION OF VIABLE CYSTS:
1. Person to person
- hand-to-mouth (children, siblings, day care centres)
- some sexual practices implicated
2. Contaminated food and water:
- Epidemic if water supply is contaminated
- unhygienic food handlers - traveller's disease
3. It is easily transmitted because:
- Infectious dose is very small (~10 cysts)
- The cysts are resistant to chlorine and other disinfectants
- They remain viable for weeks in cold water
Giardiasis - diagnosis, control
DIAGNOSIS:
- symptoms
- Microscopic observation of cysts or trophozoites in faeces
- Immunological tests (antigen immunoassays and Immunofluorescence)
- String (Enterotest) or biopsy (routine use not justified in alow-incidence population - Chew et al. (2008)
- Conventional, Multiplex or real time PCR
.
PREVENTION:
- Communal, group and personal hygiene
- Avoidance of potentially-contaminated food or water
Treatment
- Metronidazole is still widely used and is regarded as very effective (active against DNA) - Evidence of resistance in some regions
- Tinidazole (another 5-nitrimidazole with a longer half-life but presumably the same mode of action) more effective
- Paromomycin is also effective
- Albendazole may be of similar effectiveness to metronidazole, may have fewer side effects have the advantage of a simplified regimen.

Toxoplasmosis - Toxoplasma gondii
- Cosmopolitan, zoonotic, intracellular sporozoan, the most successful parasite ever??
- Causes toxoplasmosis - important opportunistic infection
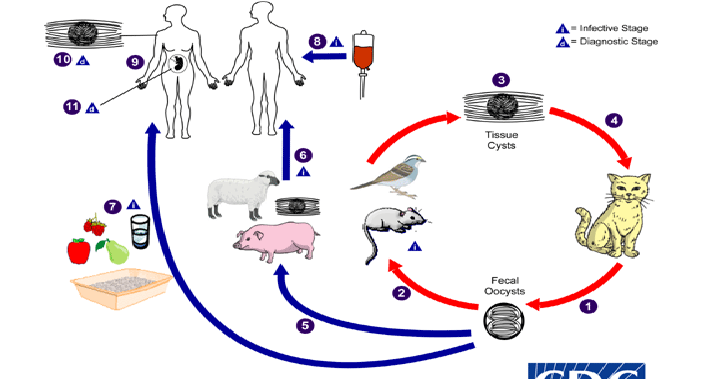
- Life cycle closely associated with cat
- One Pacific Island free of cat - the only known Toxoplasma free place
- Reproduces asexually and sexually in cat, definitive host
- Wide range of vertebrate hosts - asexual reproduction by endodyogeny: 2 daughter cells formed within mother cell
- Estimated one third adult contracts chronic but asymptomatic infection globally
- Major opportunistic infection - re-emergence of silent infection

So why is it the most successful parasite ever?
1. It has at least 5 mechanisms of transmission
2. Despite it having only 1 definitive host it can infect every warm blooded animal and bird
3. It can infect every nucleated cell
4. It is truly global, every habitat
5. It will live inside you for your entire life (and you would never know)
6. It does not kill the host (normally)
7. However, it does effect your brain to improve it's chances of transmission
8. It is very hard to treat
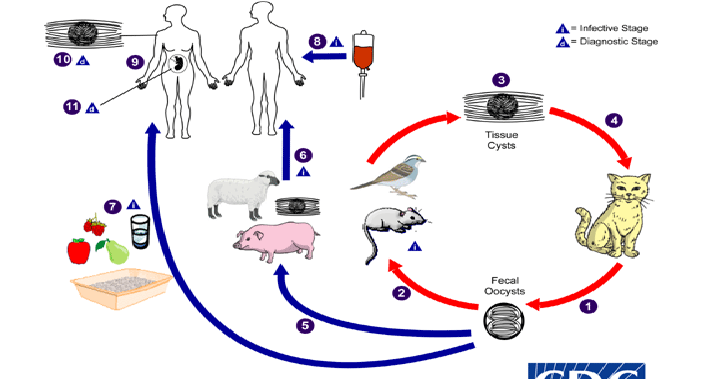
How do you catch the disease - Toxoplasma gondii
DIAGRAM ON SLIDE 14
Toxoplasma gondii - pathology
Pathogenesis/Clinical aspects
- Most remain asymptomatic BUT can cause severe and fatal disease
Acquired toxoplasmosis less severe generally:
- Asymptomatic: around 90%
- Lymphadenopathy with/without fever
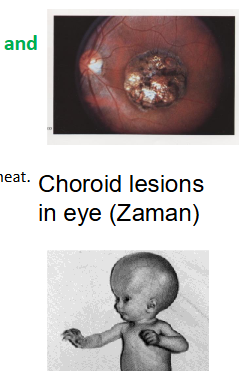
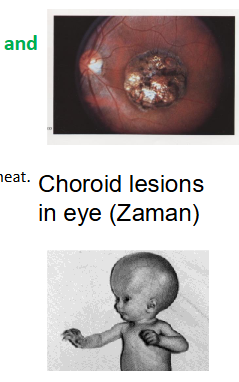
- Eye lesions: uveitis, retinochoroiditis, choroiditis
- Myocarditis.
- Acquired from cysts in soil food or pseudocysts in undercooked meat.
.
Congenital toxoplasmosis by far more severe:
- Abortion
- Still birth
- Hydrocephaly, mental retardation and eye lesions
- Acquired by vertical transmission across placenta
.
Toxoplasmosis in immunodeficient subjects:
- Reactivation of latent infection
Fatal, acute fulminating disease:
- Necrotising encephalitis
- Pneumonitis
- Myocarditis Choroid lesions in eye (Zaman)
Diagnosis of toxoplasma gondii
- Detection of antibody by serology: ELISA; Fluorescent antibody; Haemagglutination; Complement fixation - Most common means of diagnosis - differentiate between current/acute infection and chronic infection
.
- Detection of parasite from suspect autopsy or biopsy materials, including bone marrow, spleen, CSF, lymph, and brain
.
- Detection of parasite DNA in blood by PCR: especially relevant in detecting congenital infections in utero. - Only useful during acute infections
.
- PCR is useful in the acute phase, since you can take a blood sample
- but in the chronic phase, PCR is useless (because it hides)
Prevention of Toxoplasma gondii
- adequate cooking of meat is essential
- Proper disposal of domestic cat's faeces
- Protecting children's play-areas from cat contamination
Treatment of Toxoplasma gondii
- Only curative in acute phase, No curative treatment available for chronic phase
- Cllinical improvement via synergistic pyrimethamine (Daraprim) and sulphadiazine plus folinic acid (prevent bone marrow suppression)
.
- for this next part, titre refers to antibody titres (IgG, IgM)
Asymptomatic subjects:
- Seropositive but stable titre: No treatment
- Seropositive, rising titre: Treatment indicated
- Stable/rising titre and starting immunosuppressive therapy: Treatment
.
Symptomatic subjects:
- Stable or rising titre: Treatment indicated
- Infant with falling titre; IgM absent: No treatment - maternal antibody
- Infant with stable/rising titre; IgM present: Treatment -Transplacental infection
.
- daraprim eradicates it in the acute phase
- once chronic happsens no point of treatment unless they are immunocompromised where in that case you treat with daraprim for life
.
seropositive means that its positive in blood serum
Long-term sequelae of toxoplasma gondii (T. gondii in italics)
- A small but growing body of evidence suggests that T. gondii infection may sometimes have severe consequences - often decades after infection
- Suggestion that infection is linked to affective disorders such as schizophrenia (Xiao et al. 2009 -
- Significant link (IgG seropositive) to bipolar disorder but not to any unipolar mood disorders in US (OR: 2.4, Pearce et al. 2012) and France (OR 2.2, Hamdani et al. 2012)
- In France "In adult age classes 55 years and older, regional mortality rates due to brain cancer correlated positively with the local seroprevalence of T. gondii." (Abdollahi et al 2022), maybe due to modifying miRNAs in the brain
.
- The "manipulation hypotheses" proposes that parasites may alter their host's behaviour in order to increase their chance of being transmitted
- Chronic T. gondii infection affect mouse behaviour, reduces their fear of cats and cat urine
- Toxo infected chimpanzees morbidly attracted to leopard urine (Poirette et al 2016)
- Alters epigenetic programming in humans (Asuger 2011)
- Infected men attracted to cat urine although this has no obvious epidemiological impact (Flegr, 2013).
- Reduces response time - associated with car accidents (Flegr 2002)
Malaria - general characteristics
- Obligate intracellular blood sporozoan
- Primarily tropical and sub-tropical (limited by vector)
- Infection transmitted by female Anopheles mosquitos
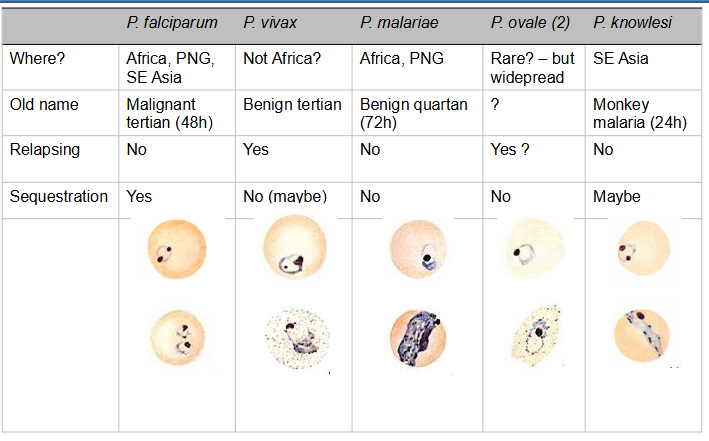
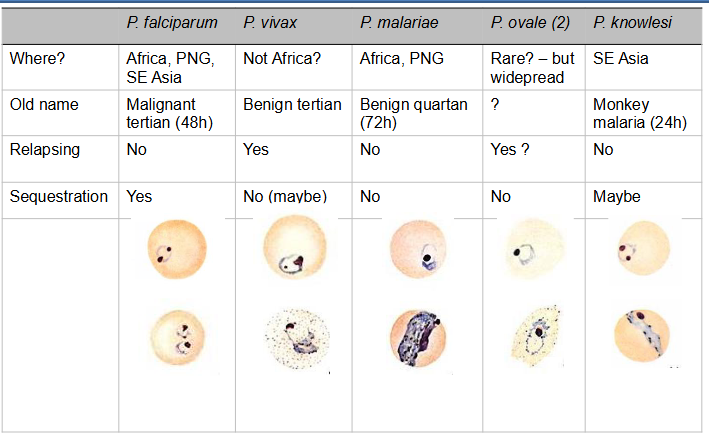
- Four (five) human pathogenic spp: P. falciparum, P. vivax, P. malariae and P. ovale (P. Knowlesi) - also malaria in birds, lizards, rodents, primates.
- Most serious disease caused by Plasmodium falciparum (cerebral or malignant malaria)
.
Species differentiation includes:
- Morphology and staining characteristic of various stages (Trophozoite, schizont, gametocyte)
- Number of merozoites in blood schizont (a sexual stage)
- Appearance of infected blood cell
- Pathology: severe, benign, cerebral, anaemia
.
out of all the species, the one thats important is P. falciparum, this is the most common and deadly

Malaria - Plasmodium falciparum
- Vast majority of deaths occur from infections with Plasmodium falciparum (the commonest form of malaria)
- P. ovale and P. malariae are generally considered benign, some deaths caused by P. vivax
.
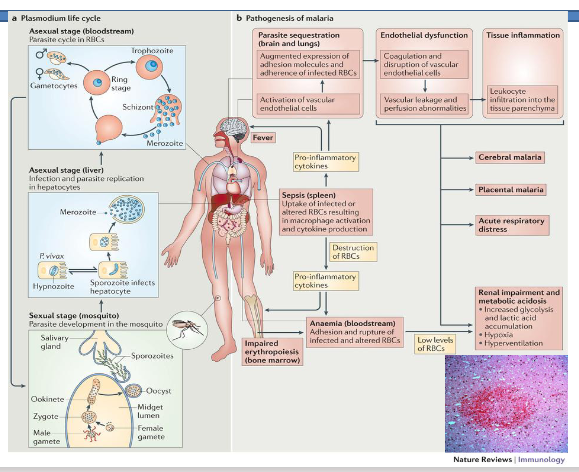
Why does Plasmodium falciparum kill you?
- It is the only species that infects all ages of red blood cell. This leads to very high parasitemia. This in turn leads to high red cell death and anaemia
- It is the only species that secretes proteins to the surface of the infected red blood cell making it 'sticky'. This causes the red blood cells to sequester in the deep organs, adhere to capillary epithelial cells and block the blood vessels causing micro haemorrhaging.
- It causes loss of oxygen, acidosis and haemorrhaging in the organs. This is particularly evident in the brain leading to thousands of micro haemorrhages.
.
- because of the anaemia caused by destruction of red cells, your body cant get oxygen to the whole body, which causes build up of lactic acid (leading to acidosis)

Malaria - Parasite Diversity
- not super important right now

Epidemology of Malaria
Each year 350-500 million cases, > onemillion deaths, most young children and pregnant women.
- In Africa an estimated 990,000 people died of malaria in 1995 -over 2700 deaths per day, or a death every 30 seconds. In 2024 - 610,000 deaths
- Estimated 5-fold reduction in GDP inmalarious countries
- Estimated $12 billion loss to Africa annually due to malaria
- Highest rate of malaria deaths in sub-Saharan Africa near equator, approximately 11% of all deaths in children in developing countries
- Interventions have saved 14 million deaths since 2000

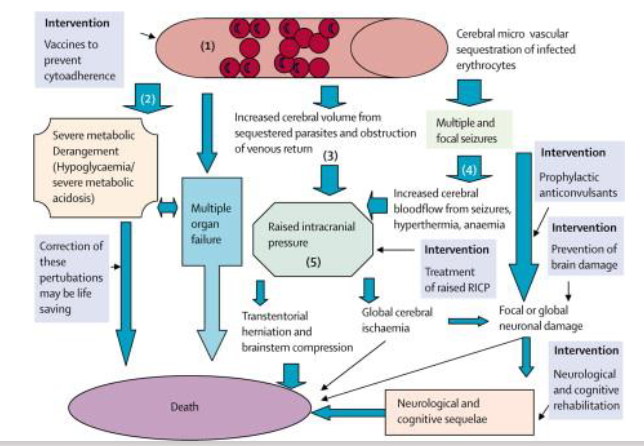
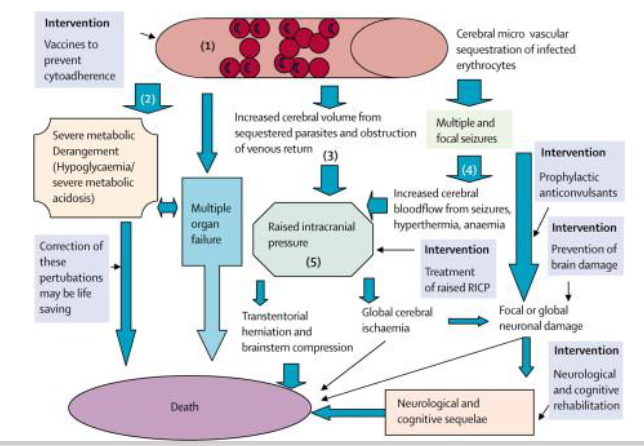
Pathology - Why do kids die of malaria
The 3 ways it kills you:
- it destroys red blood cells
- causes blockages to body
- causes intracranial pressure rising, causing haemorrhaging
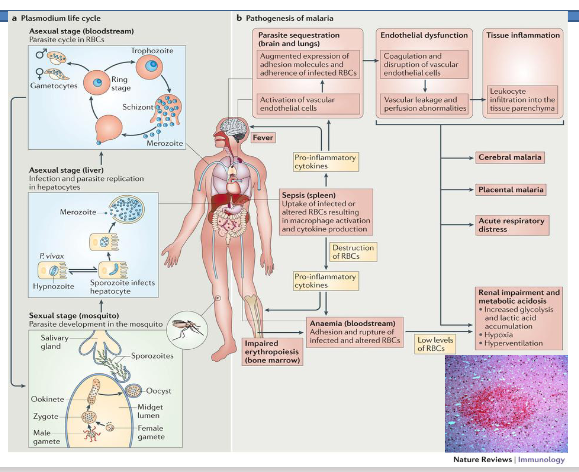
Pathology of Malaria
DIAGRAM ON SLIDE 25

Malaria treatment
Quinine and related agents
- Chloroquine
- Amodiaquine
- Pyrimethamine
- Proguanil
- Sulfonamides
- Mefloquine
- Atovaquone
- Primaquine - kills liver stage (bolded)
- Artemisinin - combination therapy (bolded)
- Halofantrine
- Doxycyline -
- Clindamycin
- Spiroindolones
.
Chloroquine, Proguanil, Mefloquine and Doxycyline is often given also as prophylaxis
.
- one of the most important ones to remember as its the one you will probs get if you get malaria is artemisinin - combination therapy

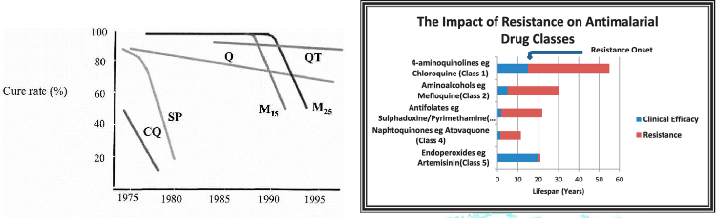
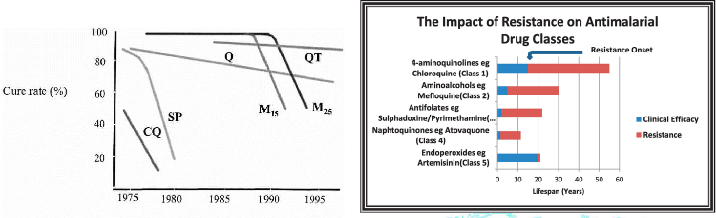
Drug resistance
DIAGRAM ON SLIDE 27
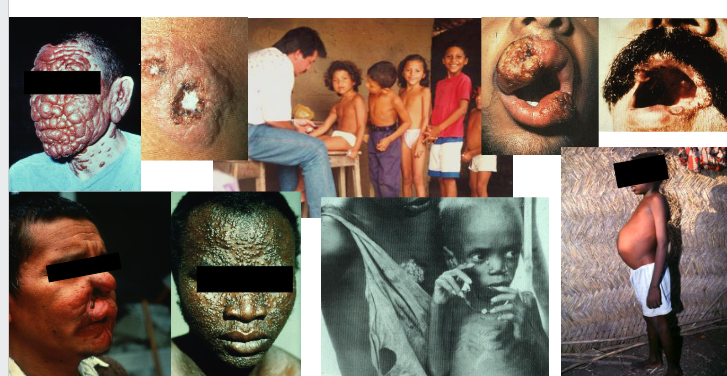
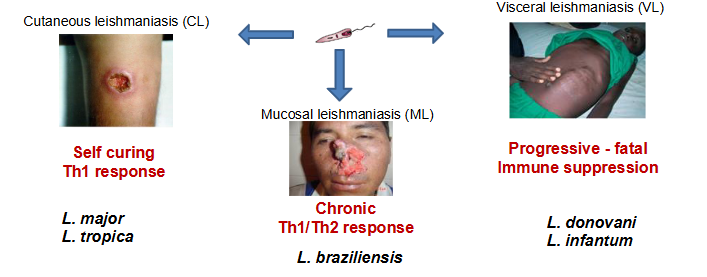
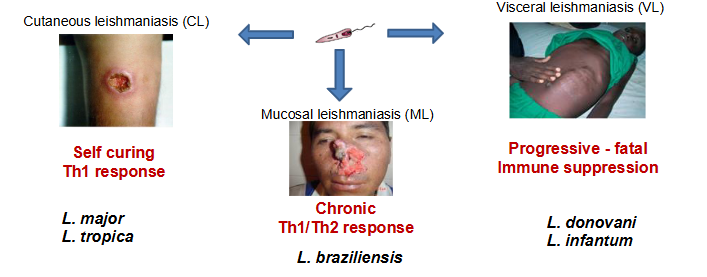
Leishmaniasis - One disease, many phenotypes
DIAGRAM ON SLIDE 28
What is leishmaniasis?
- Leishmaniasis is a diverse disease caused by obligate parasitic protozoan Leishmania spp.
- Digenetic life cycle, zoonosis*
- > 12 million infected worldwide (WHO, 2010)
- 3 main diverse clinical presentations
.
Cutaneous Leishmaniasis (CL)
SELF CURING
TH1 RESPONSE
- L. major
- L. tropica
.
Mucosal Leishmaniasis (ML)
CHRONIC
TH1/TH2 RESPONSE
- L. braziliensis
.
Visceral leishmaniasis (VL)
PROGRESSIVE - FATAL IMMUNE SUPPRESSION
- L. donovani
- L. infantum
.
- An obligate parasite is an organism that cannot complete its life cycle without relying on a living host for survival, nutrition, and reproduction
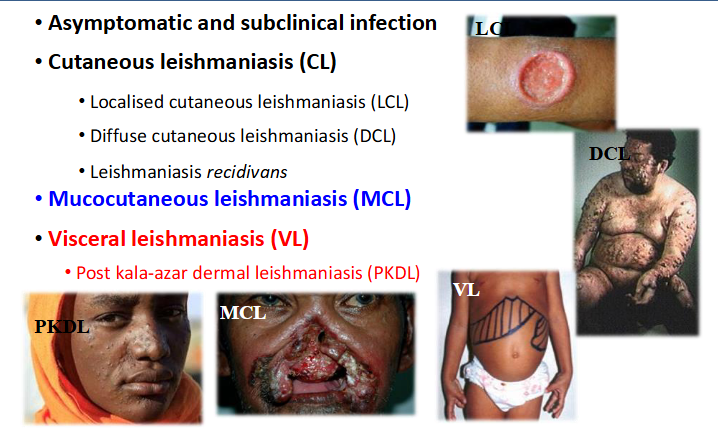
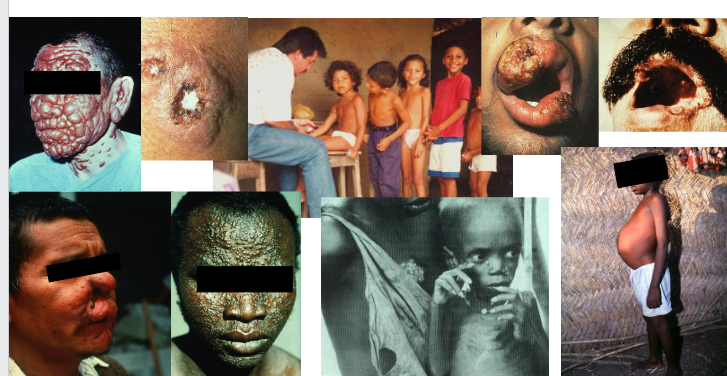
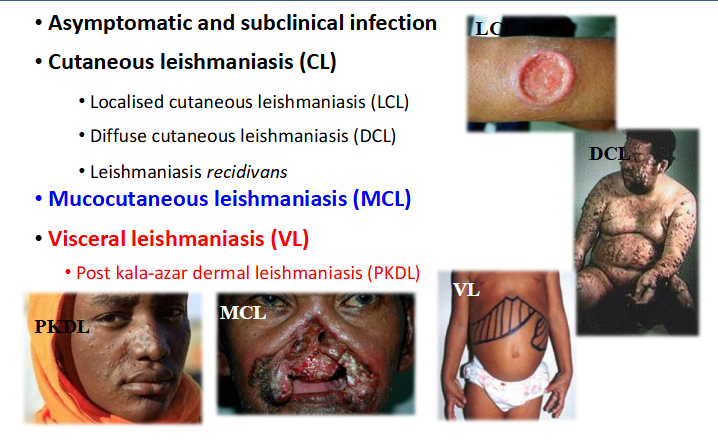
Disease Phenotypes
- asymptomatic and subclinical infection
CUTANEOUS LEISHMANIASIS (CL)
- localised cutaneous leishmaniasis (LCL)
- diffuse cutaneous leishmaniasis (DCL)
- Leishmaniasis recidivans
.
Mucocutaneous leishmaniasis (MCL)
.
Visceral leishmaniasis (VL)
- Post kala-azar dermal leishmaniasis (PKDL)
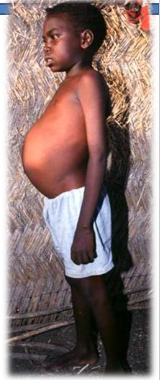
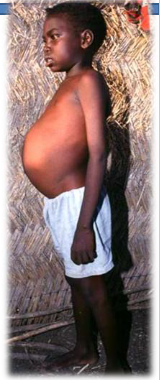
Visceral leishmaniasis - symptoms
- Incubation: 2-6 months (10 d to ~30 y)
- >95% fatal no treatment, >90% cure with treatment
.
Acute, subacute or chronic
- Fever, loss of weight, muscle atrophy, fatigue.
- Pronounced hepatosplenomegaly
- Lymphadenopathy, pancytopenia, abdominal pain, diarrhoea, ascites and epistaxis
- Depressed cell mediated immunity
- Death due to haemorrhaging or 2nd infection
.
- Post kala-azar dermal leishmaniasis
.
Differential diagnosis
- Toxoplasmosis, schistosomiasis, Chagas diseases, typhoid fever, subacute endocarditis, brucellosis, disseminated histoplasmosis, lymphomas, etc.
.
- the only symptom that is really specific is hard, palpable spleen (response to parasites)
Visceral leishmaniasis/HIV Co-infection
- Reported in 35 countries worldwide (2-12% of all VL cases)
.
Diseases are mutually reinforcing as they both depress CMI
- Increases the risk of developing active VL by between 100 and 1,000 fold, reduces therapeutic response, and increases HIV activation
.
Clinical polymorphism
- Papulonodular, ulcerative, infiltrative, lepromatous and diffuse, psoriasis-like, cheloid, histioid or Kaposi-like
.
- Parasite dissemination with visceralization of "dermotropic" species and cutaneous involvement of "viscerotropic" species

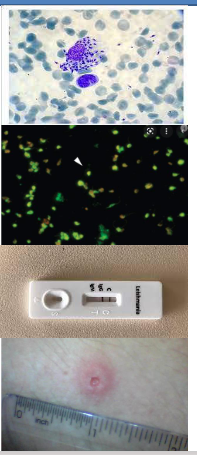
Diagnosis of Visceral Leishmaniasis
- Clinical diagnosis - Hard palpable spleen, fever and wasting
.
Parasitological diagnosis
- Definitive diagnosis
- Parasites found in aspirates of bone marrow, lymph nodes or spleen
- Giemsa stain, culture in blood agar or hamster.
.
Laboratory tests
- ELISA (enzyme linked immunosorbent assay)
- IFAT (indirect immunofluorescence test)
- Immunochromatographic dipstick test, specific antigen Kd39
- Montenegro skin test - cannot differentiate between past and current infections
- PCR tests - RFLP, real time PCR
Treatment and control of Leishmaniasis
Treatment - All drugs are toxic!
- Drugs are expensive, old, toxic, difficult to administer and prone to inducing resistance - drug development
- Pentavalent antimonials (meglumine antimoniate and sodium stibogluconate (around $200), amphotericin B (and lipid formulatios (>1000$), paromomycin, pentamidine isethionate, miltefosine and azoles Cytokine therapy for DCL - very expensive!
.
INDIVIDUAL PREVENTION - CASE DETECTION AND TREATMENT
Avoiding exposure, protective clothing, bed-nets, repellents
.
Vaccines
- No human vaccine available
- Canine vaccine (Leishmune®)
.
Vector control
.
Reservoirs control
- Treatment or elimination of infected dogs
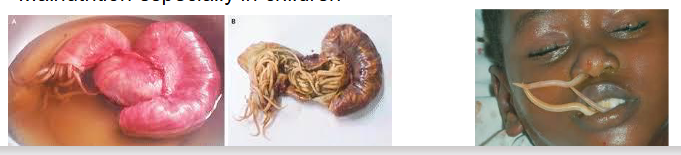
Ascaris lumbricoides - Ascariasis
Very common in developing countries: 1 billion cases
.
Pathology
- 85% asymptomatic
- worms cause intestinal obstruction (basially eggs hatch in body), particularly in children - Migrating larvae travel to lungs - inflammation - Loefflers syndrome, can travel to other organs
- Ascaris metabolites can cause sensitizing phenomena, such as urticaria, and asthma. (because it can get stuck while on its way to the lungs)
- Can move around the body inadvertently blocking narrow organs like the bile duct. Can even appear down the nose
- Malnutrition especially in children
Diagnosis of ascaris lumbricoides
- Recovery of eggs from feces, or adult worms
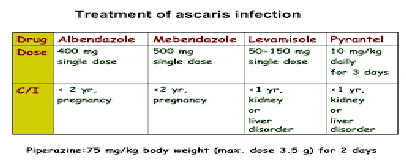
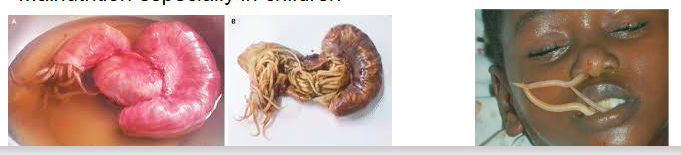
Treatment of ascaris lumbricoides
- Mebendazole, albendazole (except in pregnancy), Levamisole, thiabendazole, Pyrantel, piperazine - worms can migrate away from the gut to avoid drugs
.
- mebendazole and albendazole are bolded
Prevention of ascaris lumbricoides
Clean sanitary toilet and food preparation facilities. Personalhygiene

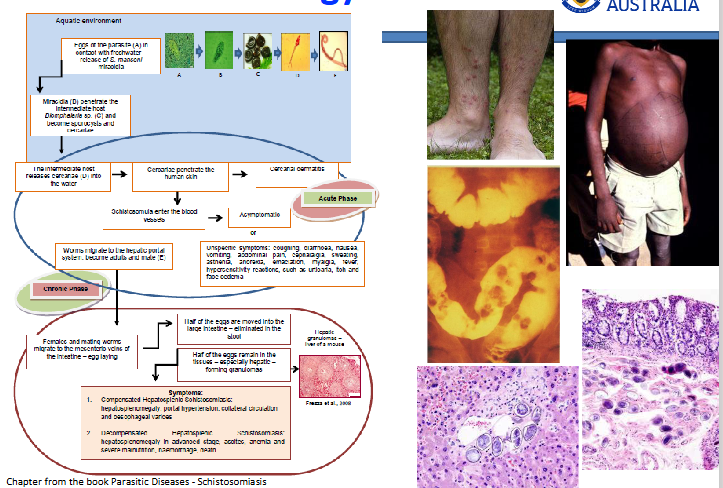
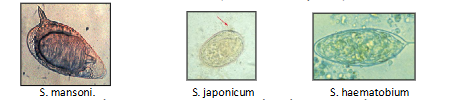
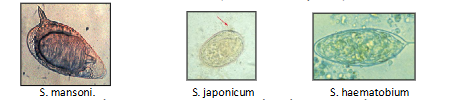
Schistosomiasis (Bilharzia)
Caused by primarily 3 separate species of the trematode Schistosoma (S. mansoni, S. japonicum (Intestinal) and S. haemotobium (bladder)
.
Overview
- Adult worms live in the mesenteric (intestinal) or vesicular (bladder)
- Pathology is caused by the presence of eggs in the gut and bladder tissue and in organs around the body.
- around 250 million infected and 200,000 die each year, endemic in ~70 countries.
- Disease is contracted by bathing or washing in water contaminated with the motile form of the parasite that burrow into the skin.
- Malnutrition especially in children
- Adults live for around 20 years in human host
.
- this is what we call a vector-borne parasite, but the vector is a snail (snail is the host before you in the lifecycle)
- way you contract is if ur in South America you go for a swim in the water, and when in the water, bare legged, parasites are swimming around and burrow through skin
- parasites lose little tail once they burrow the skin and make thier way around body via lungs and eventuially end up in the blood system and then they head to your gut
- when they get to your gut, they meet the opposite sex, and males and females get together and migate to vessels around gut or vessels around your bladder
- once they do that they pair up for life, and coat themselves with your antigen
- female lays eggs, and as the eggs try to go into gut so they get washed up in the liver and cause severe immune reaction
- can also cause severe immune reaction in the gut

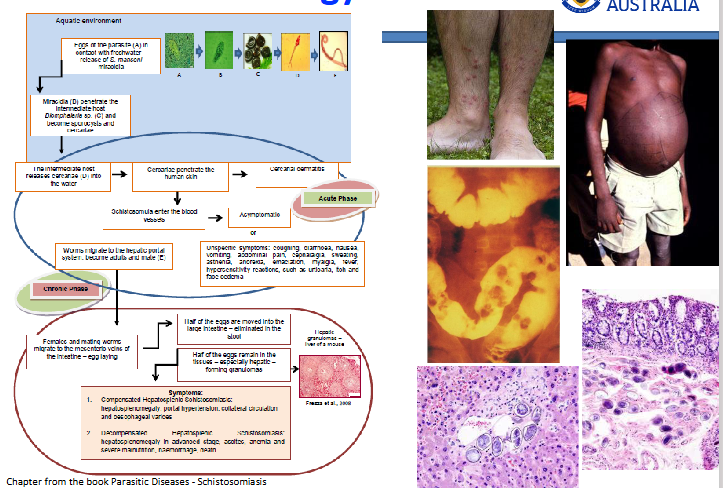
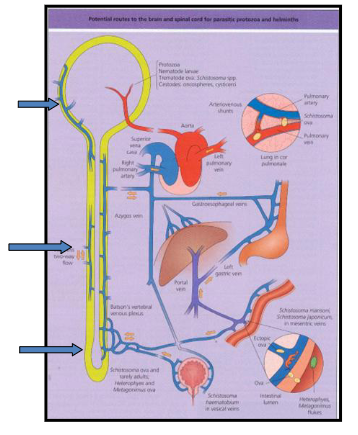
Pathology of Schistosomiasis
DIAGRAM ON SLIDE 38
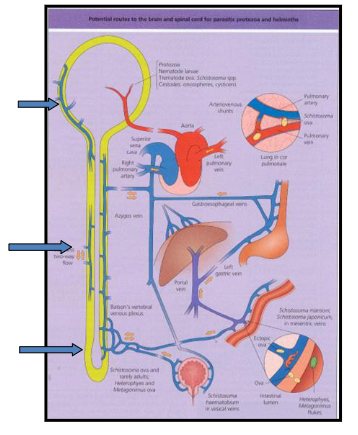
Pathology of Schistosomiasis words
ECTOPIC EGG GRANULOMAS
.
*Brain granulomas (epilepsy)
.
*Lungs - pulmonary (hypertension)
.
*spinal cord - paraplegia
*liver - fibrosis
*spleen - splenomegaly
.
*genitourinary tract (bladder cancer)
.
- occasionally eggs randomly go around body (not just liver)
- the above shows all the problems associated with this
Diagnosis of schistosomiasis
INTESTINAL SCHISTOSOMIASIS
Stool/urine: Identify S. mansoni, (lateral-spined), S. Japonicum (small lateral knob) ova in faeces. S. haemotobium ova (terminal spine) in urine
.
Repeated examinations and concentration method required.
.
Rectal snip. roctoscopy: take 6 snips of mucosa. Crush between glass slides, microscopy. Eggs of SM, SJ and also SH found.
.
Serology: indicates past or present infection. CFT/ELISA. Useful for screening (i.e.tourist visited endemic area and have been exposed but no symptoms).
.
Antigen detection in research laboratories identifies LIVING worms. Intestinal schistosomiasis S. mansoni. S. japonicum S. haematobium
Treatment of schistosomiasis
- Praziquantel single oral dose
- Metrifonate can be used instead for S. haematobium 3 doses are given over several weeks
Prevention of Schistosomiasis
1. Educate public - Target schools.
2. Prevent urine & faeces from contaminating fresh water. Build latrines.
3. Improve irrigation and agriculture systems to prevent snail build up. Include cost of molluscides in new irrigation schemes.
4. Avoid skin contact with fresh water in endemic areas.
5. Provide cercariae-free water for drinking, washing.
6. Identify infected persons and treat. Mass population treatments with praziquantel.
SUMMARY OF LEARNING
DIAGRAM ON SLIDE 42
Example MCQ Questions
2ND Q:
- the way you diagnose them is looking at a faecal or urine sample
- in a faecal sample, if youve seen a large egg about 80 microns in size with a big lateral spine you know its schistosome manima
- if you see an egg and urine sample which has a terminal spine, you know its schistosome haematobium
- if you see an egg in a faecal sample that has just a small, tiny little spine and its round, you know its schistome japonicum
Example SAQ Questions
DIAGRAM ON SLIDE 44