Week 11: PFTs & Monitoring and Life Support - MLML
1/207
Earn XP
Description and Tags
Gemini help w generation
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
208 Terms
Primary purpose of monitoring/life support
To interpret settings, displays, and data to make informed clinical decisions.
Clinical Shift
Equipment is migrating from ICU to long-term care, inpatient rehab, and home health as acute stays decrease.
ECG Lead Configuration
Uses 10 electrodes to provide 12 lead signals (4 limb leads for 6 limb signals; 6 V leads for 6 chest signals).

Standard Clinical Monitor Display
Typically shows heart rate, SpO2 waveform, and respiration waves.
Asystole (flatline) on monitor
Often caused by a detached lead during movement rather than actual cardiac arrest.
PT Wave Monitoring
Look for ST-segment changes, multiple PVCs/change in foci, onset of V-Tach/V-Fib, or worsening heart block during activity.
Continuously Measured Vitals
O2 saturation, Respiratory Rate, Heart Rate, and EKG.
Non-Continuous Vital
Blood Pressure (automated machines are set to specific 5–15 minute intervals).
Pulse Oximetry (SpO2)
Measures arterial oxygen saturation as a percentage of oxygen bound to hemoglobin.
SpO2 Threshold
Maintain levels above 90%; PTs may have orders to titrate O2 during activity to meet this.
Pulse Ox Limitation (Low Perfusion)
Anemia or low circulation prevents an accurate pulsatile signal.
Pulse Ox Limitation (Interference)
Nail polish, fluorescent lights, and jaundice (bilirubin) interfere with light absorption.
Pulse Ox Limitation (Skin Pigmentation)
Darker skin contains more melanin, which absorbs light and can affect accuracy.
Pulse Ox Limitation (Arrhythmias)
Irregular pulsatile signals make consistent calculation difficult.
Critical Safety Rule (Pulse Ox)
Always take pulse manually during the first assessment to ensure the device is reading HR correctly.
Which of the following does not affect the pulse ox readings?
arrhythmia
jaundice or darker skin
nail polish
time of day
anemia
time of day
Manual BP Cuff/Stethoscope
Essential for PTs to bring when mobilizing because automated machines do not move with the patient.
Normal Adult HR (Rest)
50 to 100 beats per minute.
Normal Adult Systolic BP (Rest)
85 to 140 mm Hg.
Normal Adult Diastolic BP (Rest)
40 to 90 mm Hg.
Normal Adult RR (Rest)
12 to 20 breaths per minute.
Normal Adult SpO2 (Rest)
95% on FiO2.
Arterial Lines (A-Lines)
Used for unstable patients needing continuous BP management or frequent arterial blood gas (ABG) sampling.
Mean Arterial Pressure (MAP) Normal Range
70–110 mm Hg.
MAP < 60
Indicates poor organ perfusion.
A-Line Transduction Positioning
Sensor must be at the level of the right atrium; too high reads low, too low reads high.
Radial A-Line Precaution
Limit or avoid weight-bearing on that wrist.
Femoral A-Line Precaution
Monitor closely and avoid dislodging.
A-Line Dislodgement Action
Apply firm direct pressure immediately to stop massive "spurting" blood loss.

Central Line
Measures Central Venous Pressure (CVP) or right atrial pressure via subclavian or internal jugular veins.
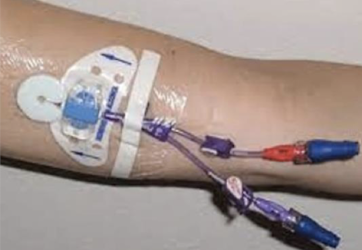
PICC Line
Peripherally Inserted Central Catheter inserted in cephalic/basilic/brachial veins ending at the Superior Vena Cava.
PICC Line Precautions
Must remain sterile. Usually well covered near skin insertion
Secure ends before mobilizing
Avoid compression and dislodging
Use precautions when femoral PICC is used
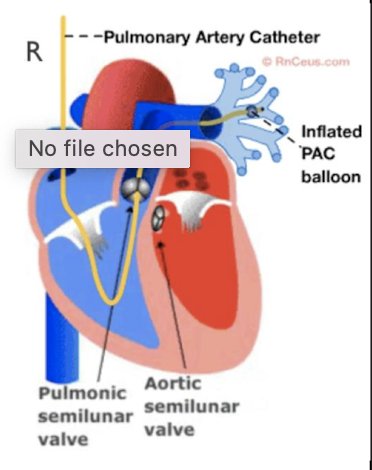
Swan-Ganz (Pulmonary Artery Catheter)
Threaded through the right heart into the pulmonary artery to locate/monitor heart failure/pressures.
Pulmonary Capillary Wedge Pressure (PCWP)
Indirectly estimates left side heart filling pressure and left ventricular function.
Uses of Pulmonary Capillary Wedge Pressure (PCWP)
Monitoring heart function (post-sx)
Diagnosing chronic heart failure
Differentiating causes of pulmonary edema
Guiding diuretic dosing to manage fluid overload
Elevated PCWP
Indicates Pulmonary HTN or resistance to flow into the left ventricle.
Swan-Ganz Complications of dislodgement
Serious arrhythmia, pulmonary artery rupture, valve damage, or heart infection if dislodged.
Temperature can be measured via
Swan Ganz, urinary catheters, NG tube, Rectal probe
Only when is a rectal probe used to measure temperature
When the patient is comotose, intubated, or confused
Intracranial Pressure (ICP) Usage
Brain surgery, head injury, hemorrhage, tumors, or meningitis.
High ICP Effect
Decreases brain perfusion.
What can help control increased/high ICP
Low CO2
A drain or shunt may be placed
PT Role (ICP)
Assessing tolerance/response to position changes and early mobilization.

Nasal Cannula
Most common system; flow rates of 1–6 L/min.
Rule of Fours (Nasal Cannula)
Every 1 L/min of O2 increases FiO2 by ~4% (e.g., 2 L/min = 28%).
Nasal Cannula Humidification
Required if flow is >4 L/min to prevent drying membranes.

Face Mask
5–10 L/min delivering 35–56% FiO2; involves air loss through sides.
Humidification is common

Trach Mask/Collar
Must be humidified because it bypasses the upper airways' natural functions.

Venturi Mask
Provides precise FiO2 delivery using color-coded adapters and specific orifice sizes.
Based on doctor’s orders of FiO2
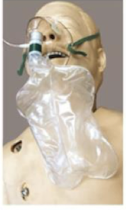
Non-Rebreather Mask
Provides up to 100% O2 via one-way valve and reservoir bag; must be fully inflated.
Due to high flow rate, need to start with full tank and bring a spare

High Flow Nasal Cannula (HFNC)
25–60 L/min; creates Positive Expiratory Pressure (PEP) to splint airways open.
Rank from lower to higher O2 support
Nasal canula, venturi mask, rebreather mask, high flow nasal cannula

CPAP
Constant positive pressure during both inhalation and exhalation.
Common in sleep apnea
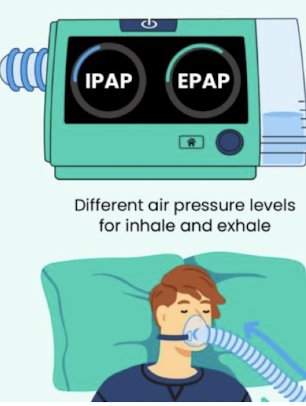
BiPAP
Two pressure levels (IPAP/EPAP); often used to wean patients off ventilators.
Invasive Mechanical Ventilator Indications
Failure to oxygenate, failure to ventilate, or airway protection.
2 types of mechanical ventilations
Endotracheal tube
Tracheostomy tube
Endotracheal tube indications
Nasal or orla
short-term

Tracheostomy tube indications
Longer term issues
Tidal Volume (TV)
Amount of air delivered per breath.
PEEP
Positive expiratory end pressure
Pressure that keeps alveoli from collapsing to increase gas exchange time.
Ventilator FiO2 Safety Limit
Aim to keep under 50% long-term to avoid oxygen toxicity and atelectasis.
Control Mode Ventilation
Machine has complete control; no patient-initiated breaths.
Assist Control (AC-VC)
Set RR
Every breath has a set volume
Patient can initiate extra breaths, which the machine assists to the full preset volume.
Synchronized Intermittent Mandatory Ventilhation (SIMV-VC)
Set RR and volume provided
Extra patient breaths are NOT volume controlled.
Spontaneous/Pressure Support
Set pressure, PEEP and FiO2
Patient initiates/dictates volume; machine provides pressure to overcome resistance.

Median Sternotomy
Skin incision midline of sternum; used almost exclusively for cardiac procedures.
Posterolateral Thoracotomy
Incision from T4 to anterior axilla; divides trapezius, serratus anterior, and latissimus dorsi.
Anterolateral Thoracotomy
Sternal edge to mid-axillary line; used for lung surgeries or mitral valve repair.
Axillary (Lateral) Thoracotomy
Shorter, muscle-sparing incision for minimally invasive cardiac procedures/pacemakers.
Subxiphoid Incision
Single incision below xiphoid for pericardium or epicardium access.
Thoracoabdominal Incision
Combination used for diaphragmatic procedures; makes mobilization very difficult.
PT Thoracotomy Assist
Give as much assist as needed from supine to sit; focus is upright tolerance.
VATS/RATS Advantages
Shorter LOS, less pain (ribs not spread), and reduced inflammatory response.
Splinted Cough Technique
Essential early PT intervention for pain management and airway clearance.
Chest Tube Purpose
Remove air/fluid from pleural space and re-establish intrapleural pressures.
Chest Tube Placement
Top (apex) for air; lower for fluid/blood.
Chest Tube Rule
Collection system must stay below chest level; device must not be tipped over.
Leadless Pacemakers
Mini-battery devices implanted directly into the heart using a coiled spring.
Intra-aortic Balloon Pump (IABP)
Balloon inflates in diastole (preloading) and deflates in systole (increasing output).
ECMO
Management for total failure; blood leaves femoral vein, is oxygenated, and returns to femoral artery.
Hemodialysis
Similar to ECMO but filters blood and corrects electrolytes without a pump.
Cerebral Edema
Impaired cognition and delirium.
Myocardial Edema
Conduction disturbance and diastolic dysfunction.
Pulmonary Edema
Impaired gas exchange and increased work of breathing.
Hepatic Congestion
Impaired synthetic function and cholestasis.
Renal Interstitial Edema
Reduced GFR and salt/water retention.
Gut Edema
Malabsorption and ileus.
Tissue Edema
Poor wound healing and pressure ulceration
Key Pulmonary Diagnostic Tests
Arterial Blood Gases (ABGs), Spirometry, DLCO, and Imaging (CXR, CT, MRI, V/Q scans).
Arterial Blood Gas (ABG) Analysis
Snapshot of a patient's current metabolic and respiratory status.
pH Normal Range
7.35–7.45 (Human average = 7.4).
PaCO2 Definition
Partial pressure of dissolved CO2 in plasma.
PaCO2 Normal Range
35–45 mmHg.
HCO3- Normal Range
22–28 mEq/L.
PaO2 Normal Range
80–100 mmHg.
SaO2 Normal Range
≥95%.
Base Excess (BE) Normal Range
+/- 2 mEq x L-1.
Indicator of Ventilation Adequacy
PaCO2 levels.
Hyperventilation Definition
PaCO2 < 40 mmHg.
Hypoventilation Definition
PaCO2 > 40 mmHg.