PDA 2 Exam 3 Molecules
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
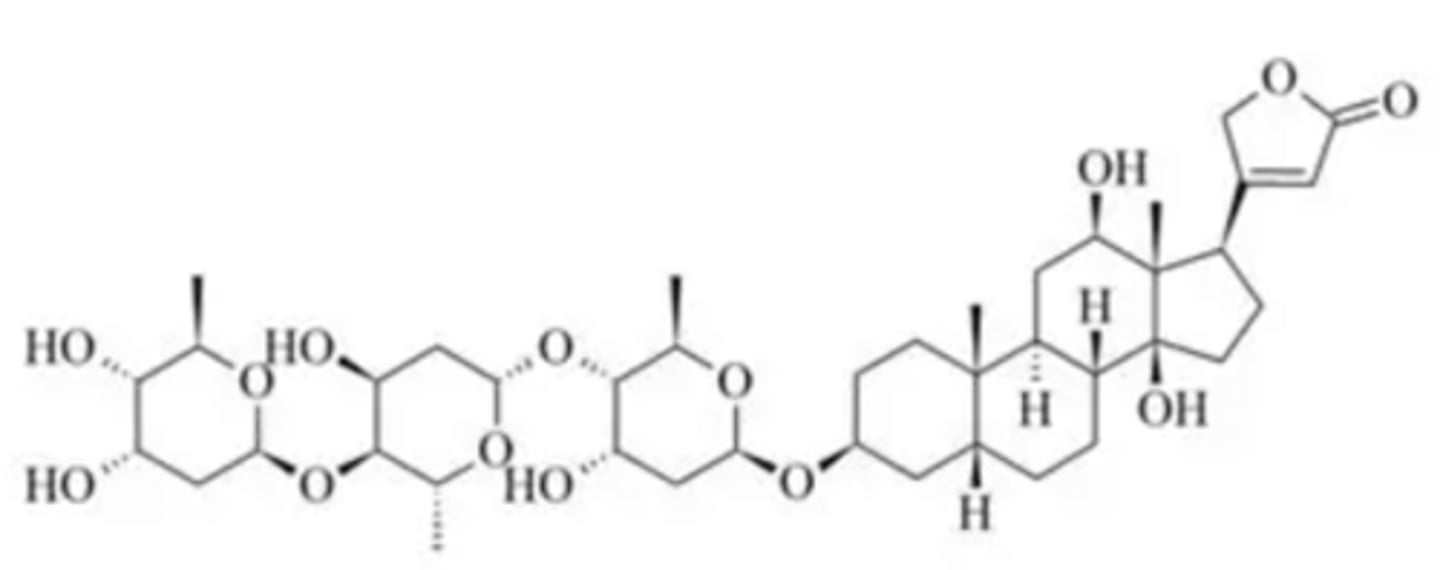
Digoxin
•a cardiac glycoside that consists of three sugar residues attached to a steroid group.
•binds near the extracellular side of the Na+/K+ ATPase and blocks the potassium binding site non-competitively
-> indirect increase in intracellular Ca2+ levels
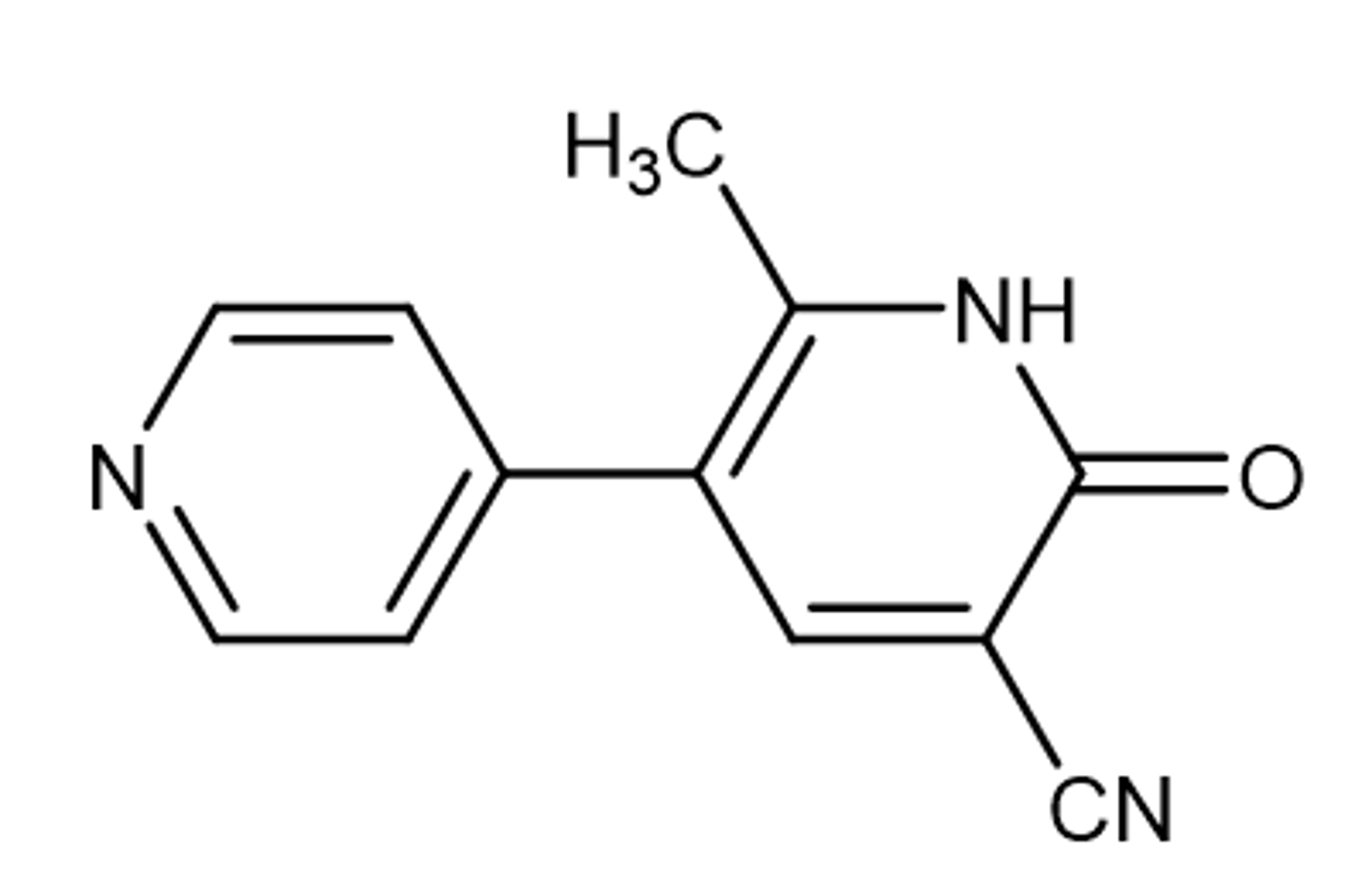
Milrinone
PDE-3 inhibitor in different cell types
inodilator (positive inotrope and vasodilator) used for the treatment of acute and chronic heart failure
•short half-life (2 to 2.5 hours), so, it is generally administered as a continuous IV infusion.
•mostly excreted unchanged in the kidney (~85%) with some liver metabolization (O-glucuronidation)
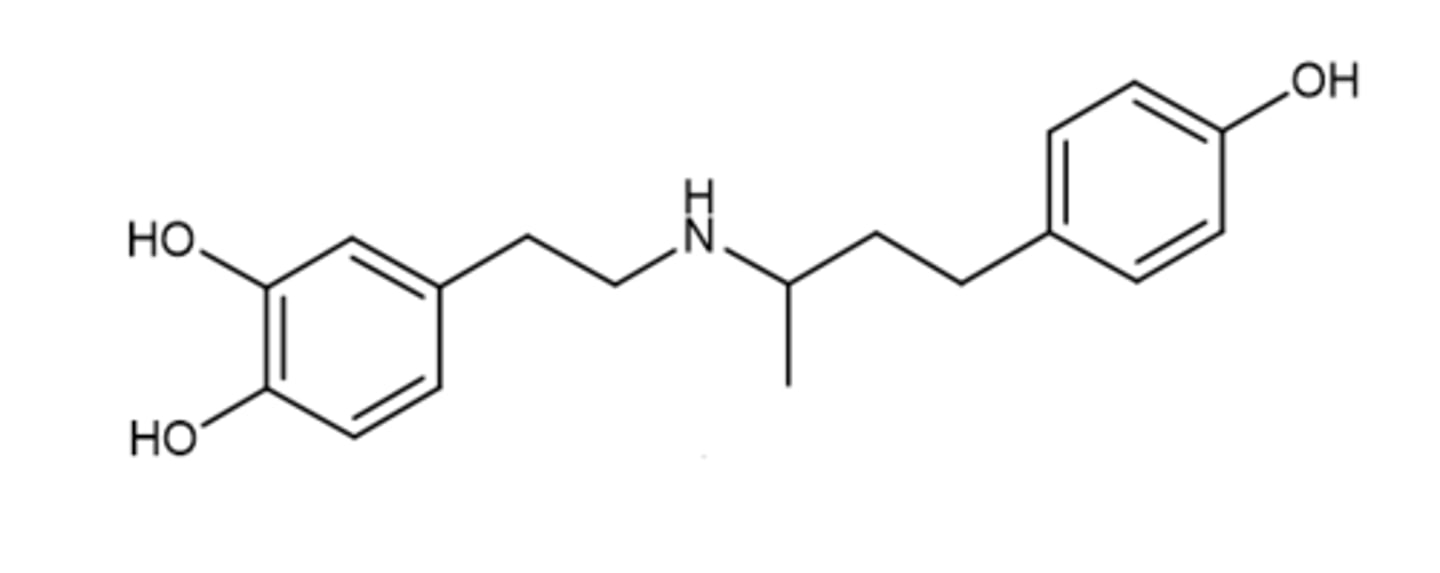
Dobutamine
selectively stimulates β1-adrenergic receptors -> increase in intracellular levels of cAMP.
This results in enhanced calcium influx into cardiac myocytes during systole -> increased myocardial contractility
Typically, it causes no significant increase in heart rate
Available as a racemic mixture
main metabolite, 3-O-methyldobutamine, is mostly inactive
Levosimendan
a calcium sensitizer that has a dual mechanism of action:
1. During systole (contraction)= It makes the heart muscle more sensitive to calcium, so it contracts stronger without using extra energy
---sensitizes troponin C to calcium in a manner dependent on the calcium concentration, thereby increasing the effects of calcium on cardiac myofilaments and improving contraction at low energy cost
2. During diastole (relaxation)= when calcium levels drop, the effect goes away, so the heart can relax normally (or even better)
---sensitization is diminished due to a plunge in calcium concentration level which does not cause a deterioration of diastolic relaxation but, on the contrary, does cause an improvement
Nitroglycerin (NTG, Glyceryl trinitrate, GTN)
Organic nitrate (a volatile oil)
Onset is 1-4 minutes, DOA is 30 minutes
Taken sublingually to prevent first-pass metabolism
Isosorbide dinitrate (ISDN, Dilatrate®, Isordil®)
Organic nitrate
Sugar scaffold increases bioavailability ~29%
80% of it is converted o 2 active metabolites= greatly extended activity of the drug
Isosorbide-5- Mononitrate
Metabolite of ISDN with 100% bioavaibility
t1/2= 5h
Isosorbide-2- Mononitrate
Metabolite of ISDN
t1/2= 2h
Hydralazine
Used in combination with ISDN (Combo called BiDil®)
BiDil® decreases mortality and reduces rate of first hospitalization in heart failure patients self-identified as black
MOA: (not fully known) Directly relaxes arteriolar smooth muscle -> reduced afterload and vasodilation
Sodium nitroprusside
Inorganic nitrate
Spontaneously releases NO -> sGC activation causes vasodilation (NO ENZYME= no tolerance)
•Dilates arteries and veins to the same degree
•Parenteral administration
•Used in HTN emergency or heart failure
•DOA: 1-10 min
•Can decrease BP in 30 seconds
•Used just enough to titrate the BP
Keep away from light
Hydroxocobalamin
Antidote for cyanide toxicity
Chelate cyano group at central OH= Cyanocobalamin
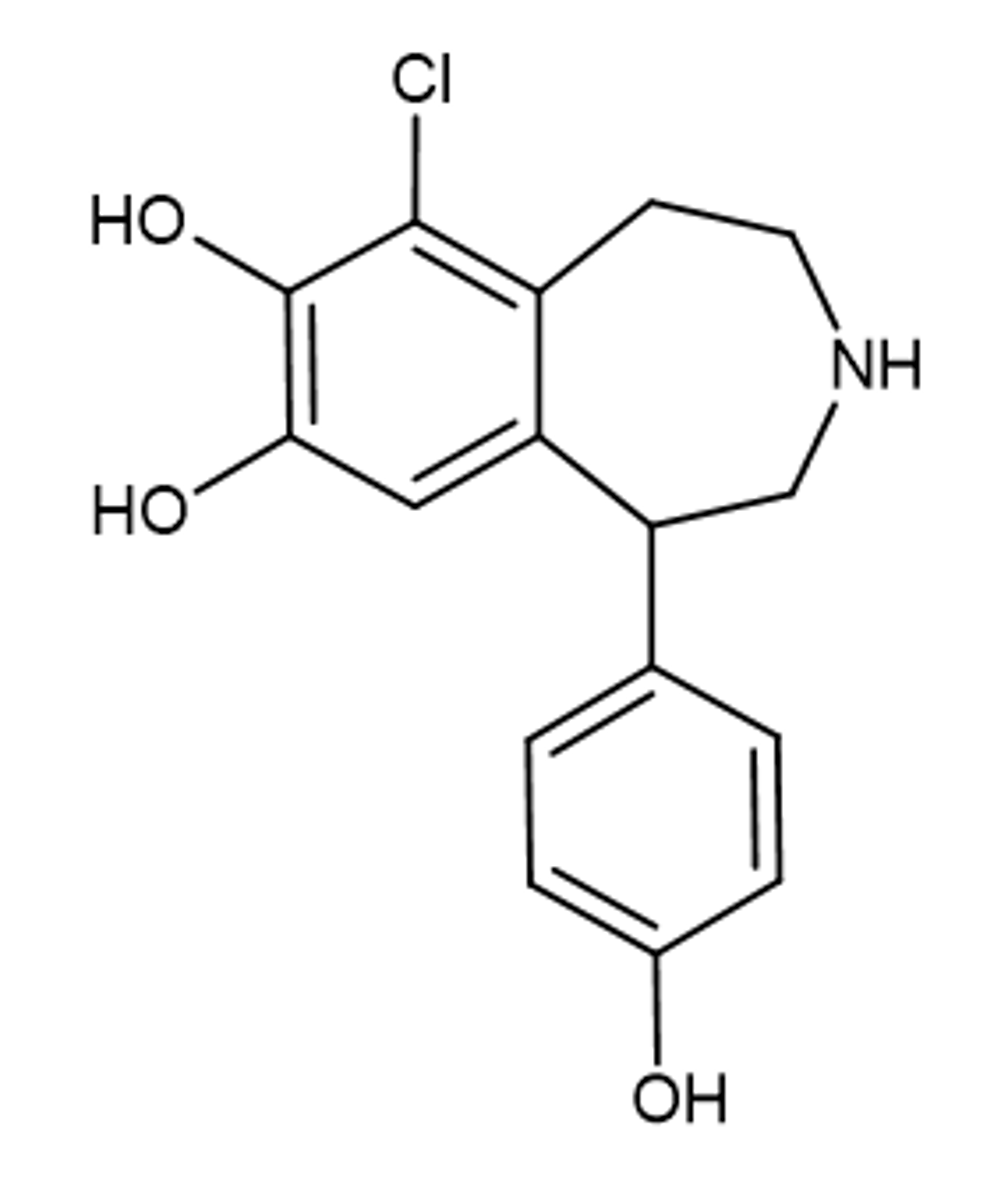
Fenoldopam
Selective Peripheral D1 Receptor Agonist
Indicated for short-term treatment of severe hypertension -> used parenterally
Equivalent to nitroprusside in lowering blood pressure
Poorly soluble in lipids -> does not penetrate BBB and has no CNS effects
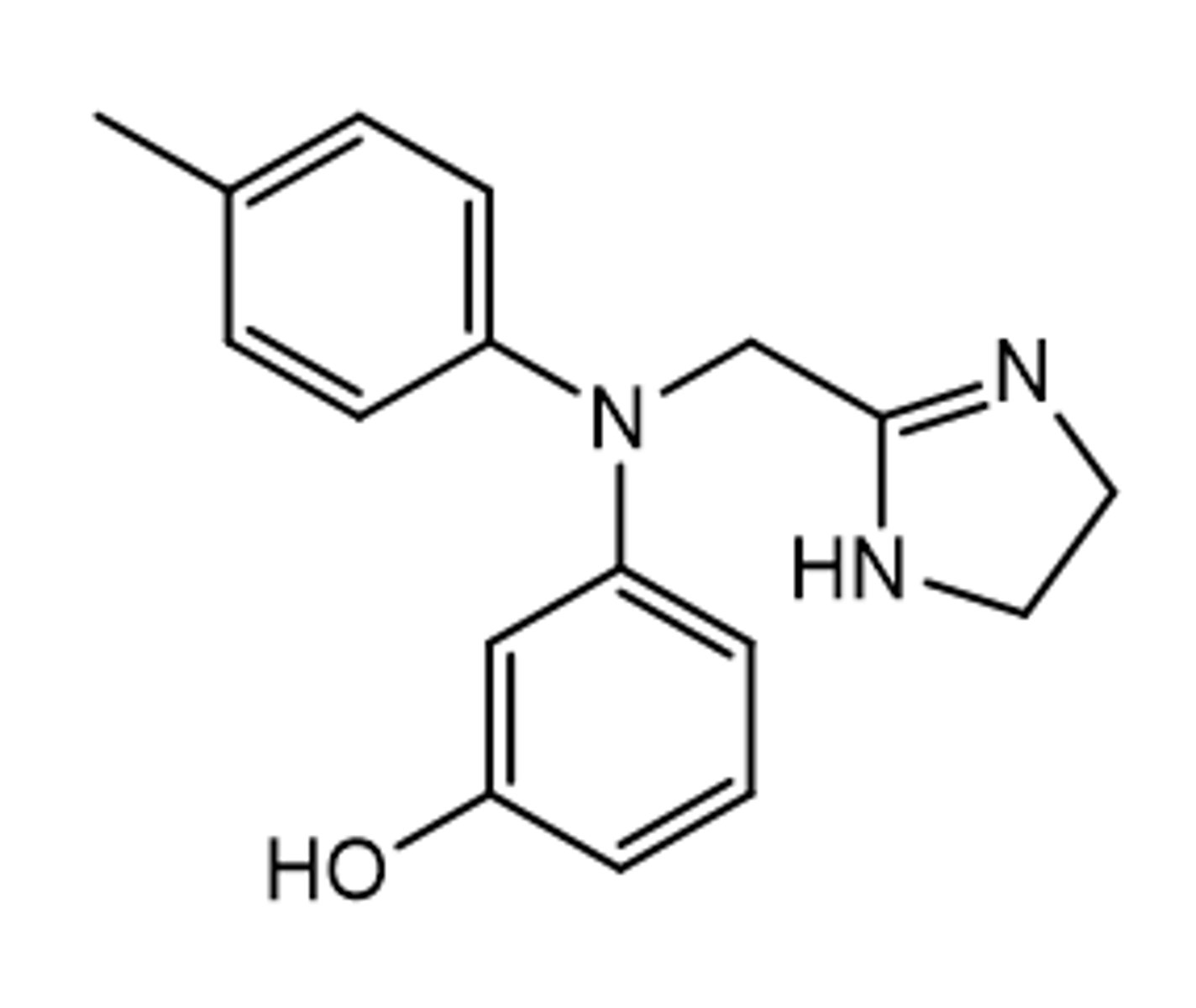
Phentolamine
Alpha 1 adrenergic antagonist for ED
Non-oral (intracavernous)
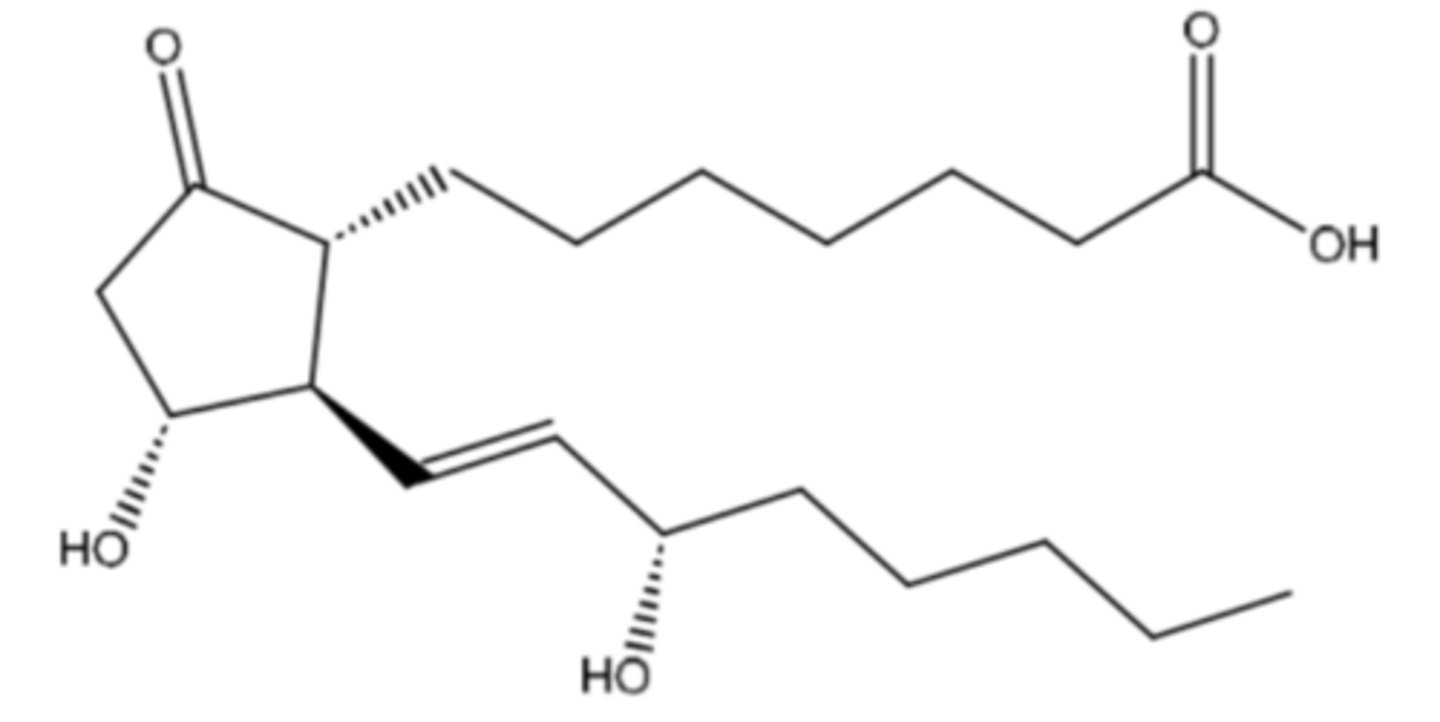
Alprostadil (IDK IF ON EXAM)
PGE1 derivative used for ED
Stimulates adenylyl cyclase to increase cAMP= smooth muscle relaxation
Non-oral (intracavernous)
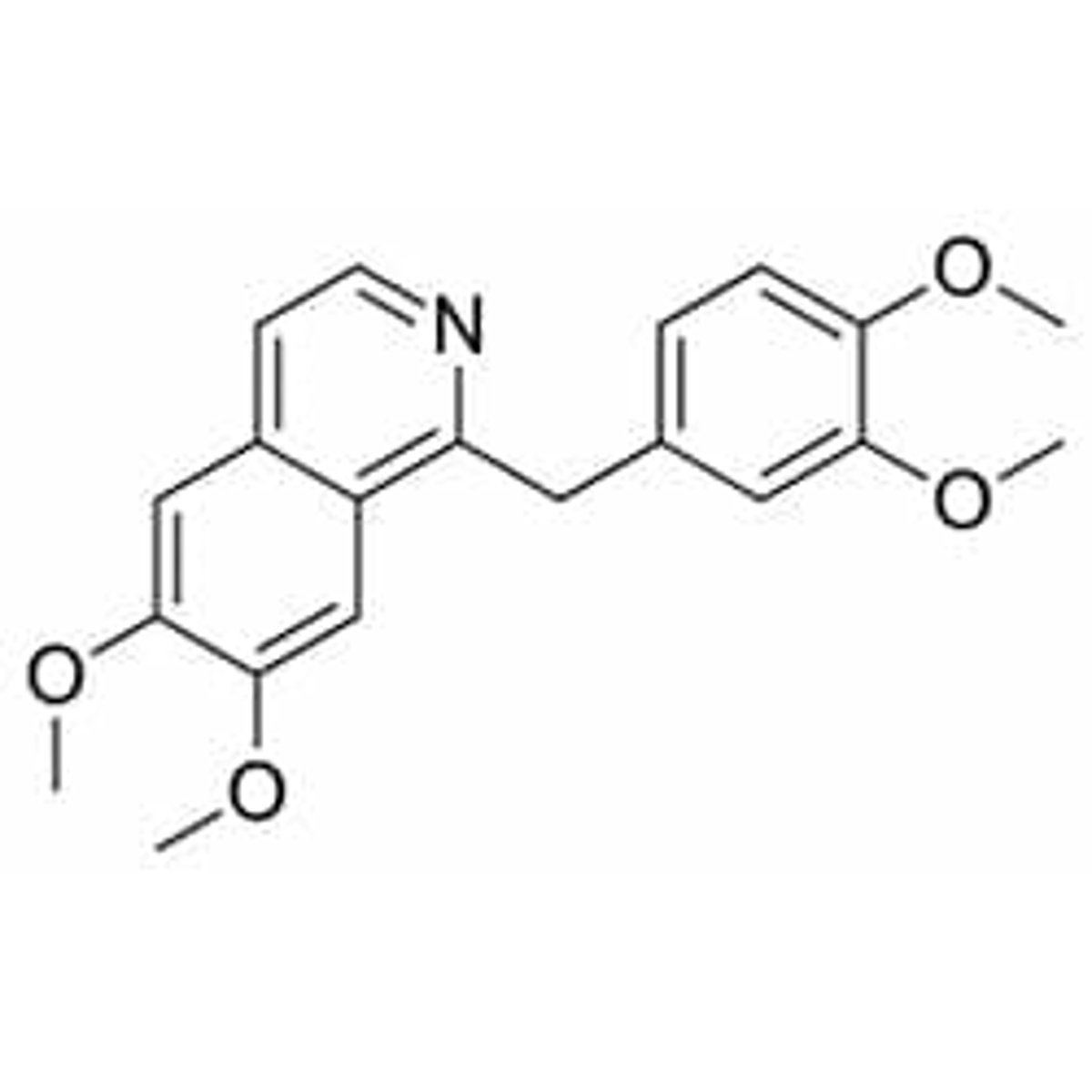
Papaverine (IDK IF ON EXAM)
PDE2, 3, and 4 inhibitor used for ED
Alkaloid found in opium
Non-oral (intracavernous)
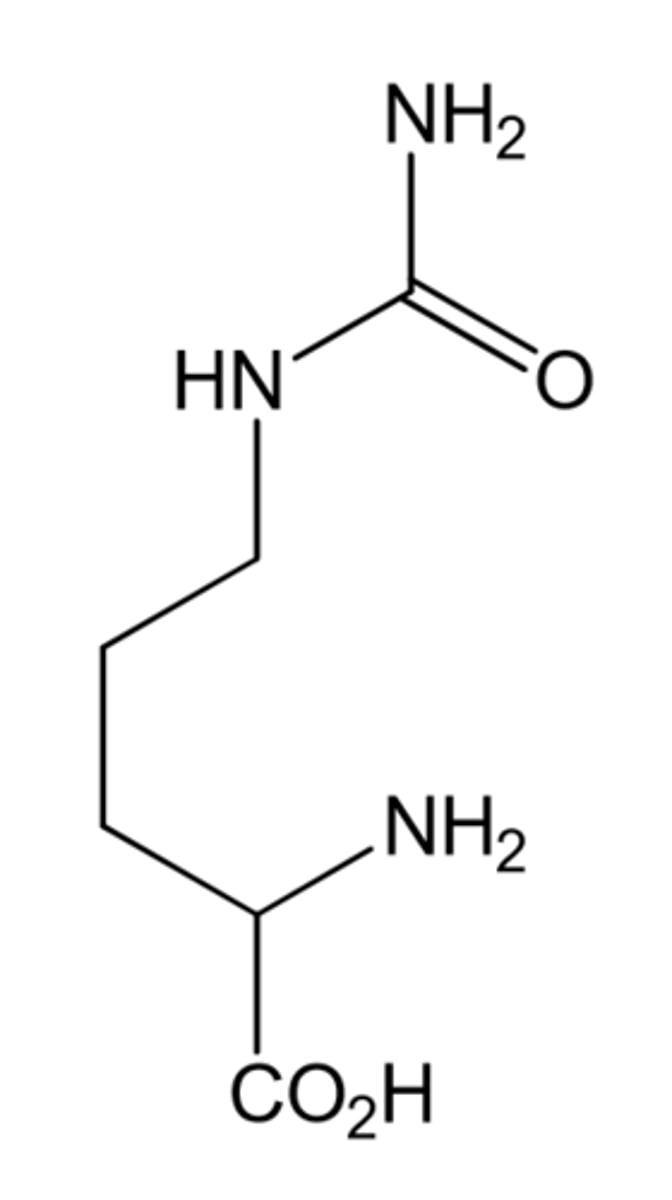
Citrulline
Product (in additon to NO) of arginine and eNOS
Used for Ed because it gets metabolized by kidneys back into arginine= increased Arg blood levels= increased bioavailability of arginine/smooth muscle relaxation
Arginine F= 10-20%
Citrulline F= 60-70%
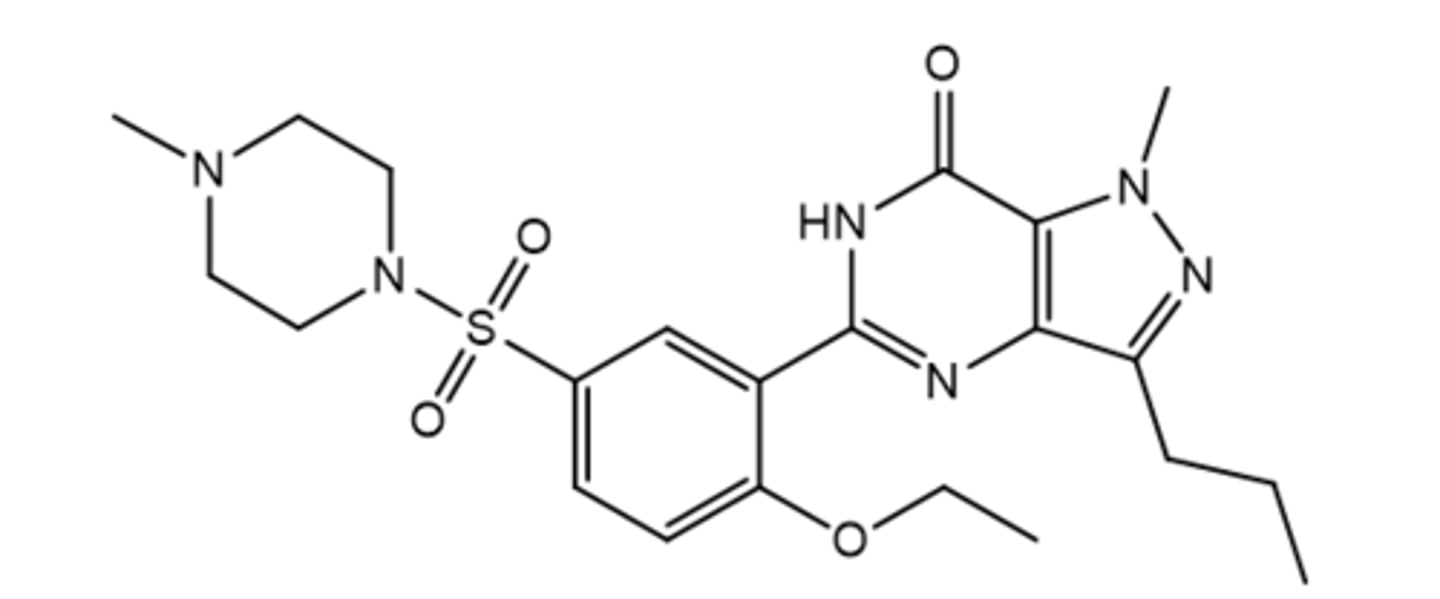
Sildenafil (Viagra)
Oral Nucleotide-like PDE5 Inhibitor for ED
Resembles cGMP (methyl)
Also used for Pulmonary arterial hypertension(PAH)
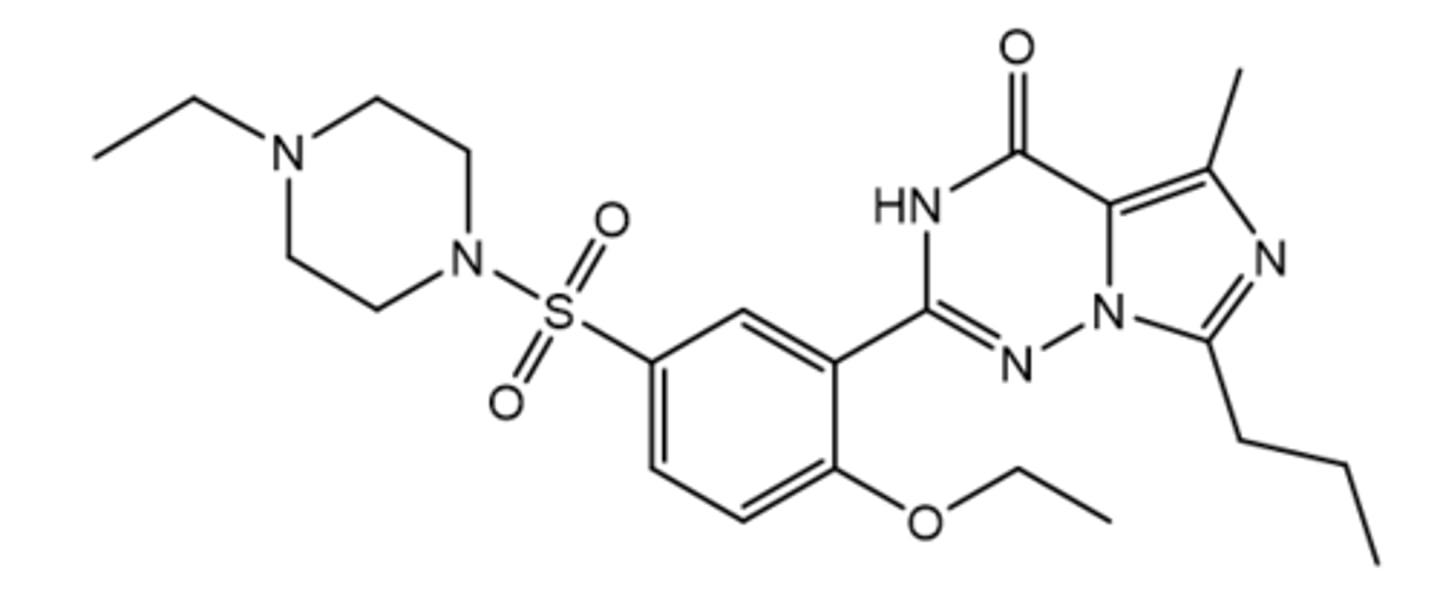
Vardenafil
Oral Nucleotide-like PDE5 Inhibitor for ED
Resembles cGMP (ethyl + extra N)
Highest potency
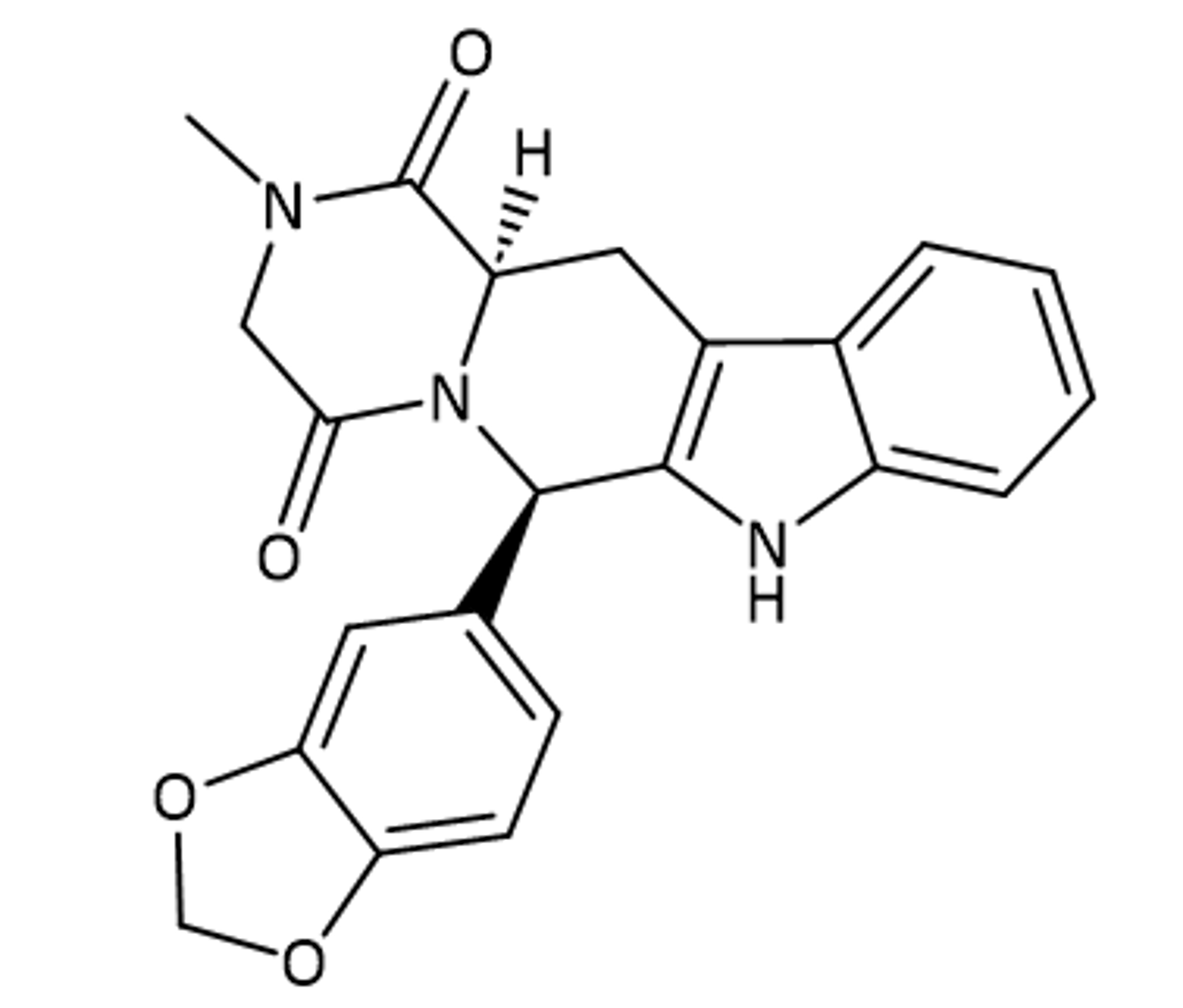
Tadalafil
Oral non-nucleotide-like PDE5 inhibitor for ED
Also used for BPH and PAH
Called "the weekend" due to 36h DOA (if you take on Friday)
Longest onset time and DOA
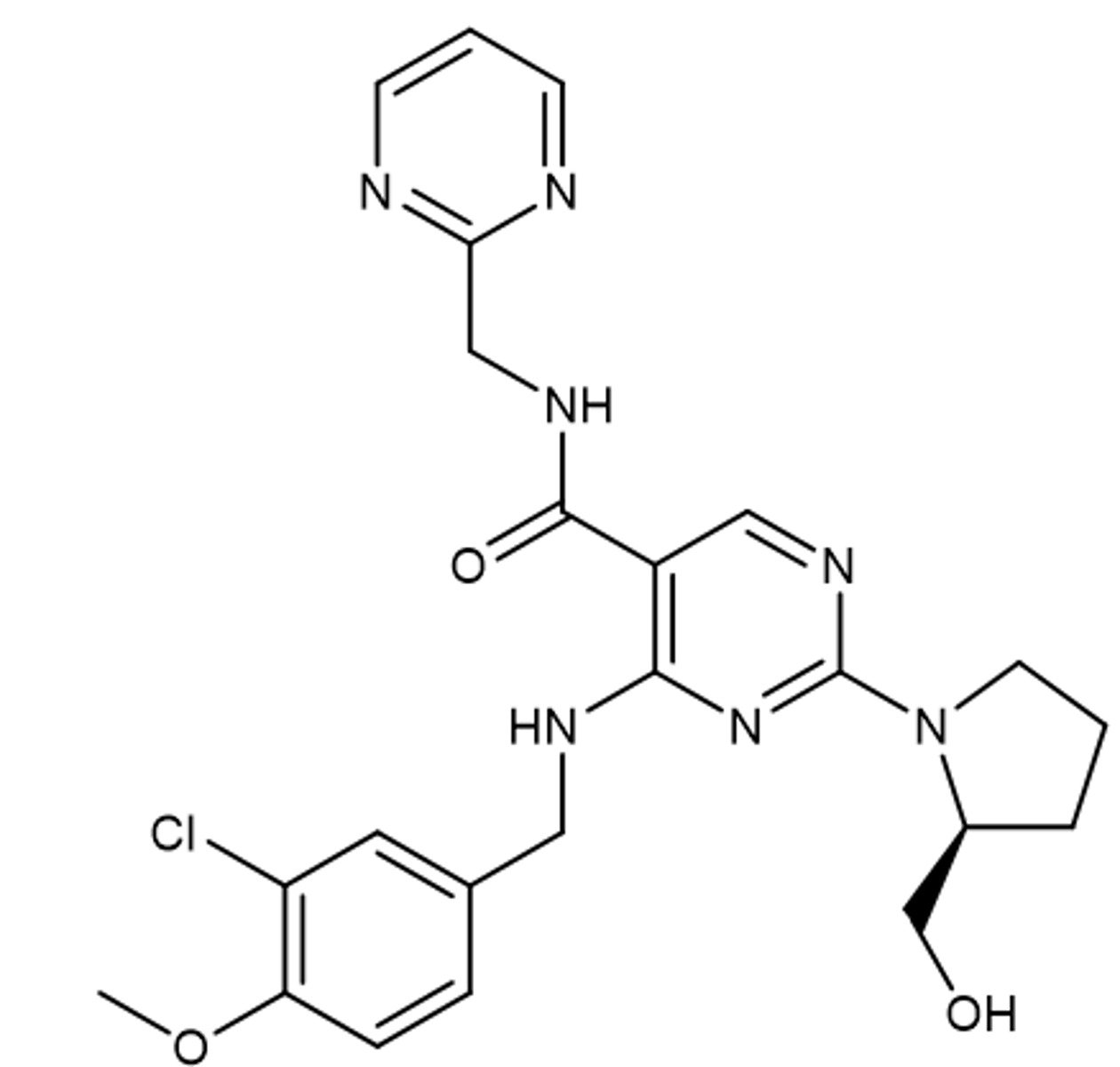
Avanafil
Oral non-nucleotide-like PDE5 inhibitor for ED
Shortest onset + DOA
Riociguat
Soluble Guanylate Cyclase (sGC) Stimulator
Indications: PAH, Chronic thromboembolic pulmonary HTN (CTEPH)
Oraly active
Short DOA (methyl causes shorter T1/2)
TID dosing
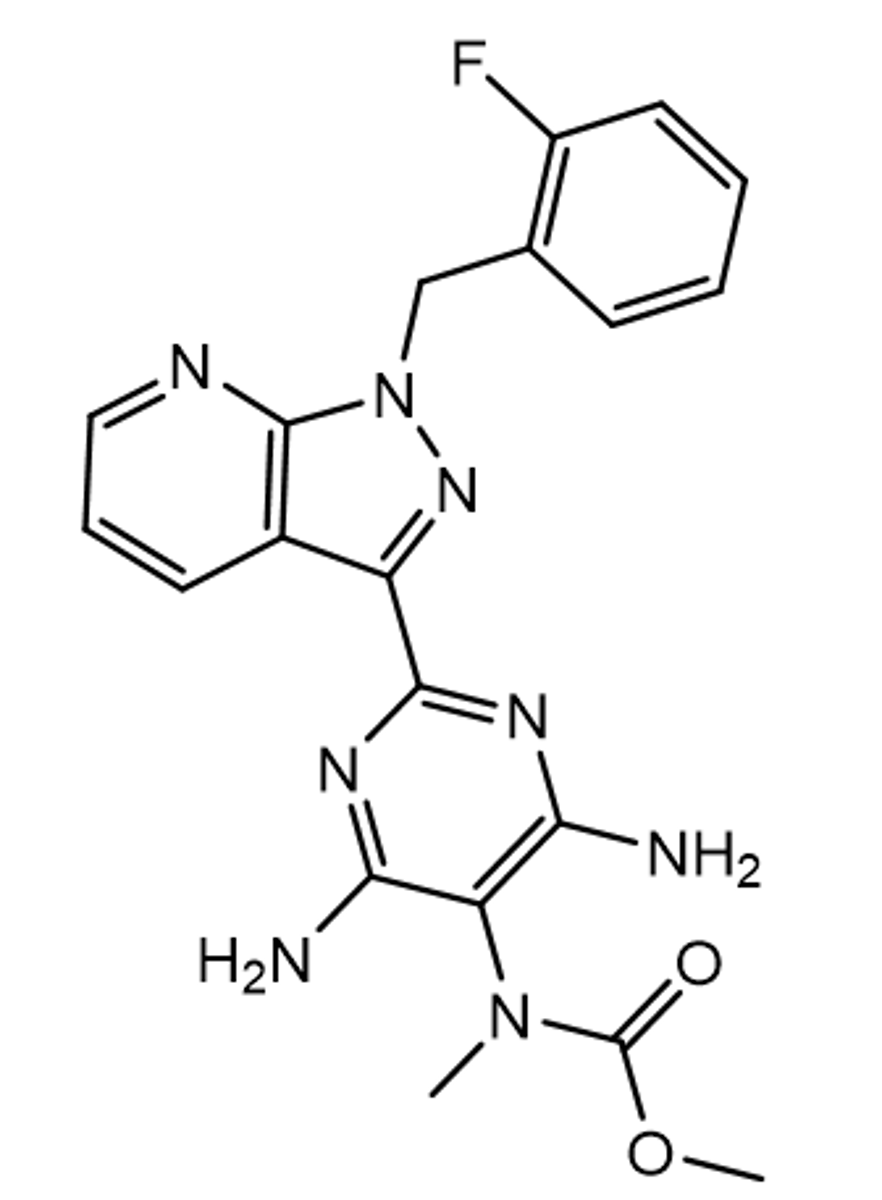
Vericiguat
Soluble Guanylate Cyclase (sGC) Stimulator
Indications: Heart failure
Orally active
Longer DOA (F increases potency)
once a day dosing

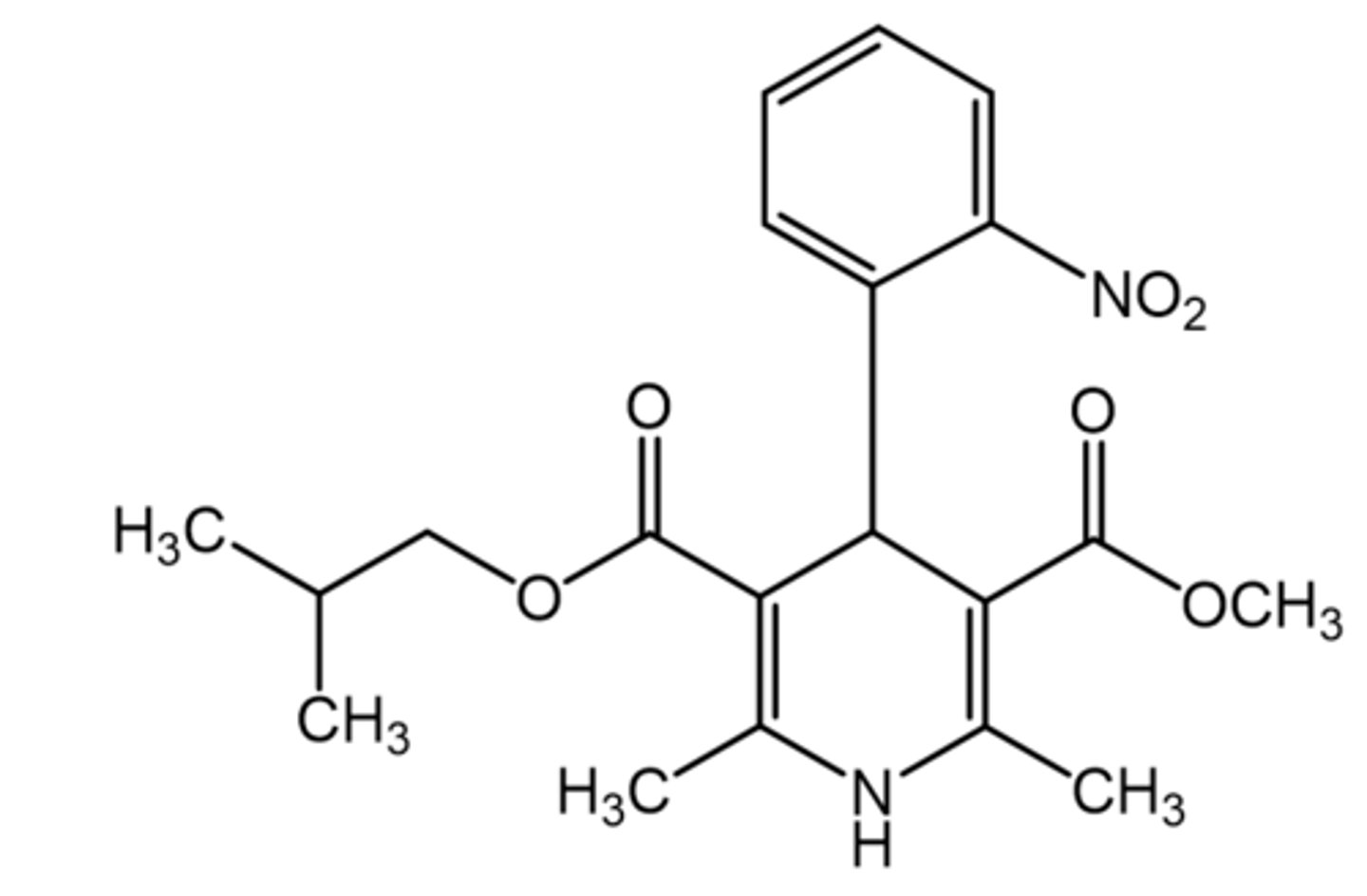
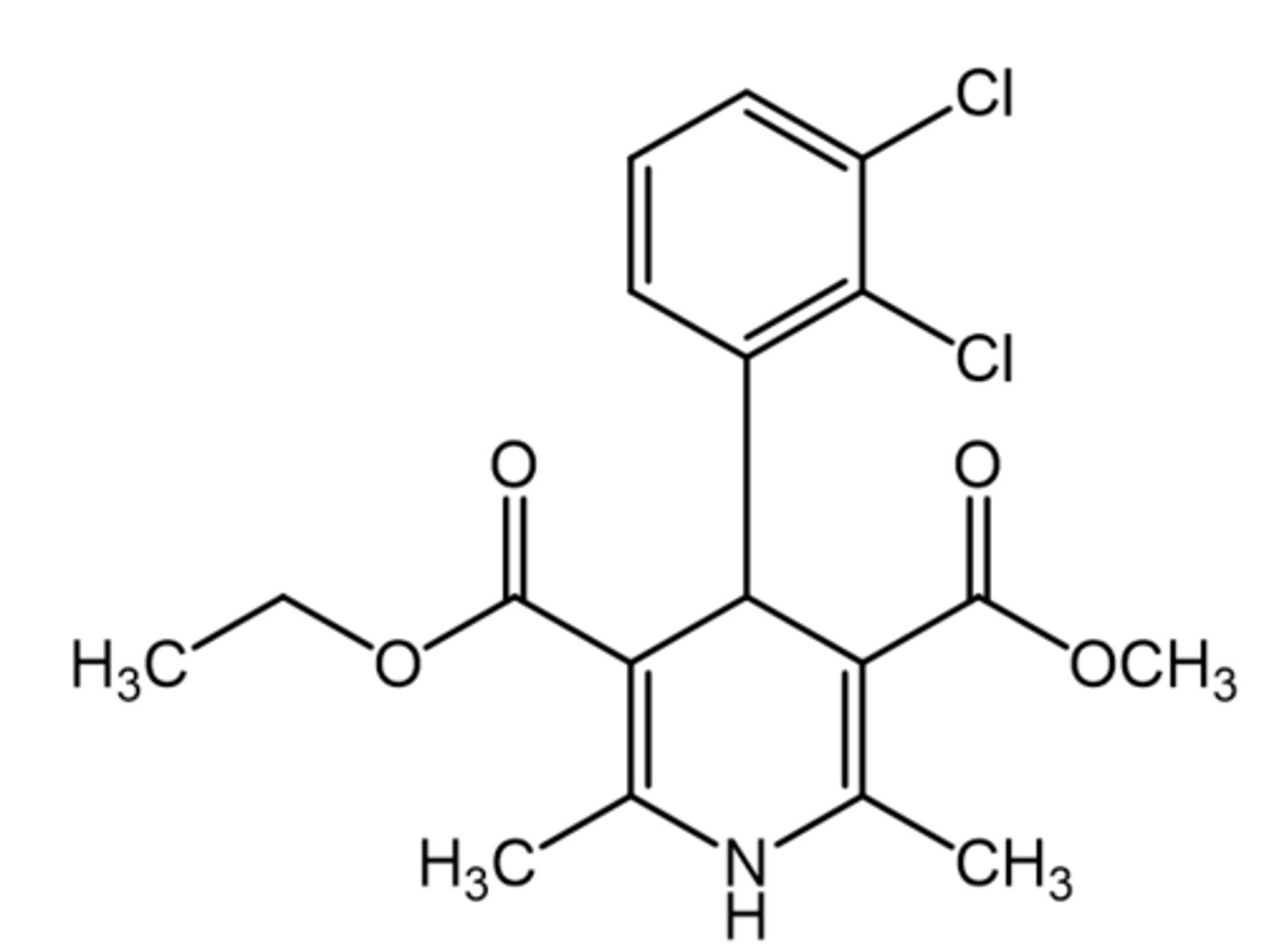
Nisolidipine
Asymmetric 1,4-DHP
Ortho group on C4 phenyl= optimal
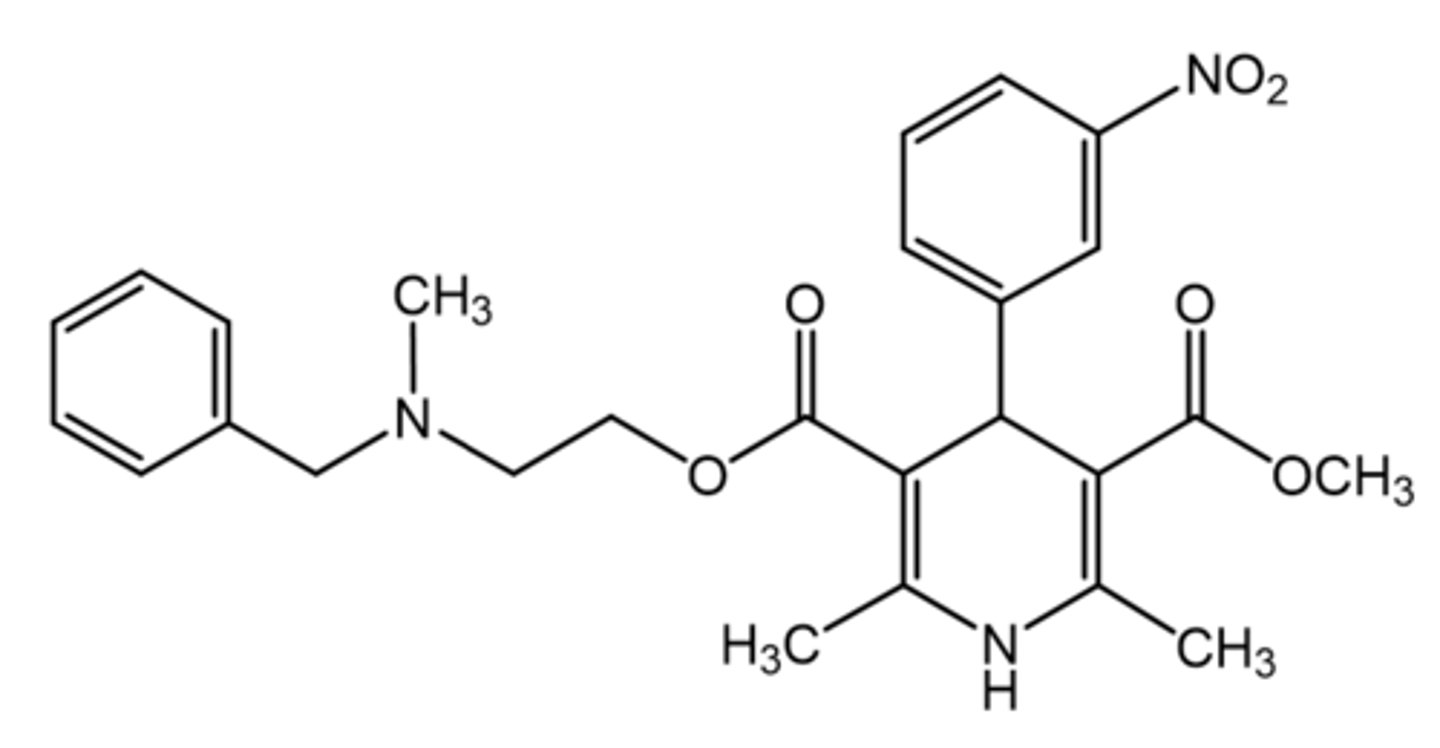
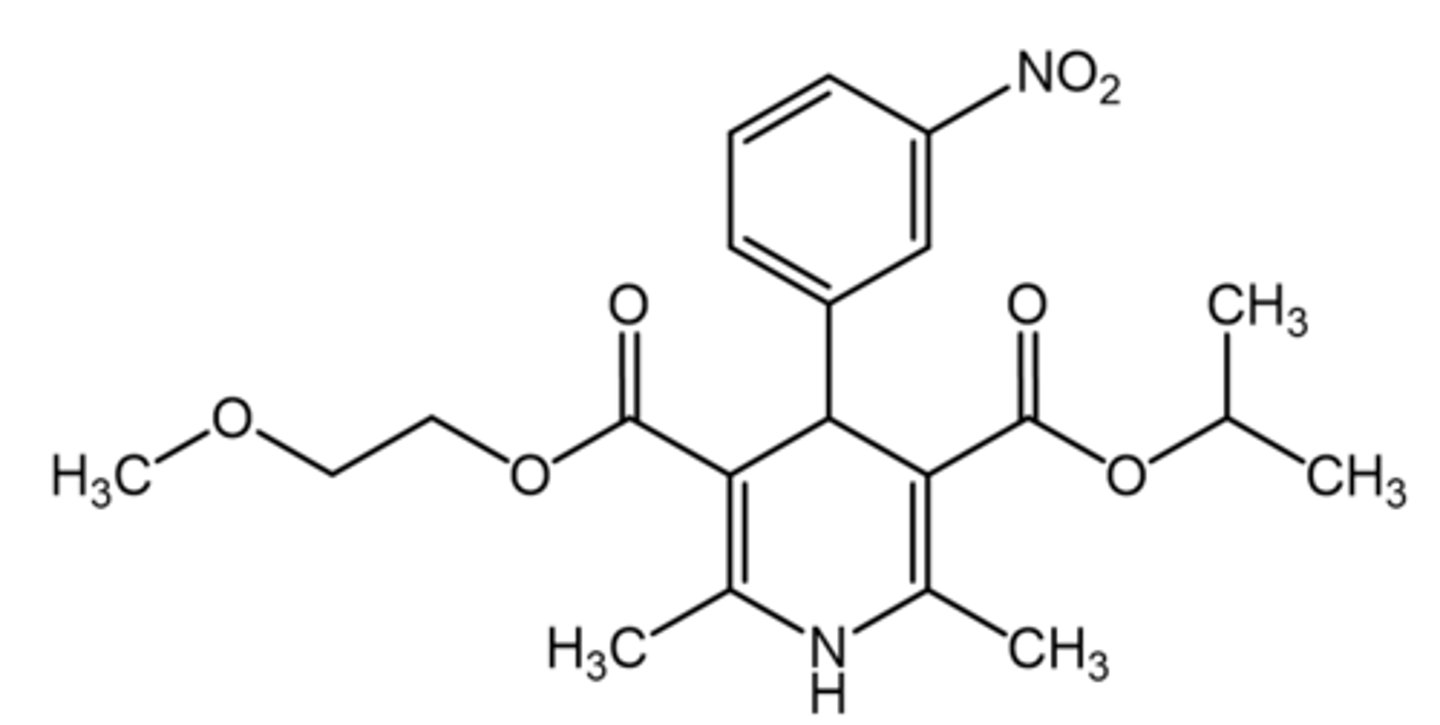
Nicardipine
Asymmetric 1,4-DHPs
Meta group on C4 phenyl= optimal
pKa ~7.2= allows it to be formulated into IV
Faster onset= used in hypertensive crises
Felodipine
Asymmetric 1,4-DHPs
Meta and Ortho groups on C4 phenyl= optimal
t1/2: 25 hours
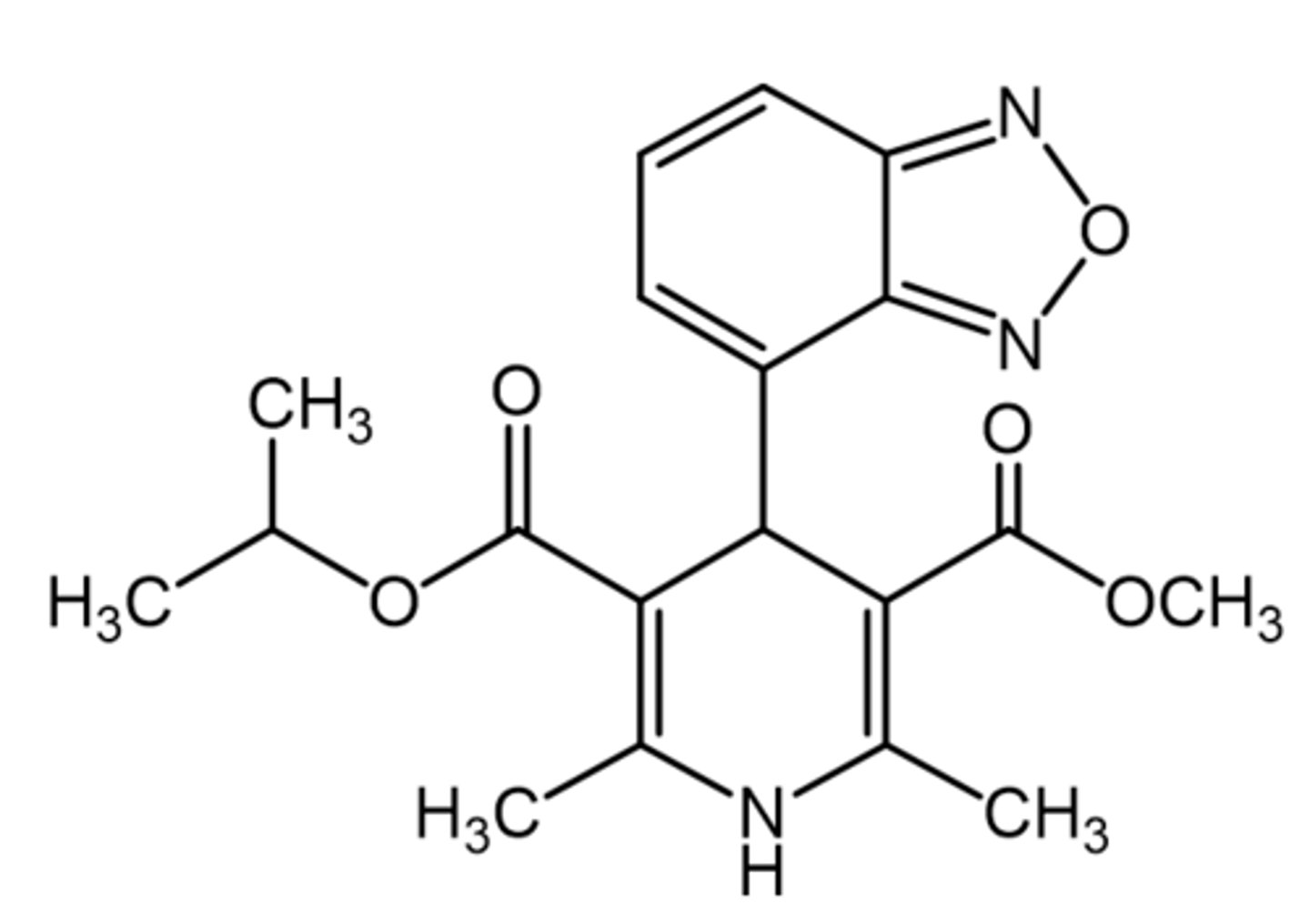
Nimodipine
Asymmetric 1,4-DHPs
Meta group on C4 phenyl= optimal
Increased lipophilicity = Better BBB penetration
Used for Cerebral vasospasms
Isradipine
Asymmetric 1,4-DHP
Meta and Ortho groups on C4 phenyl= optimal
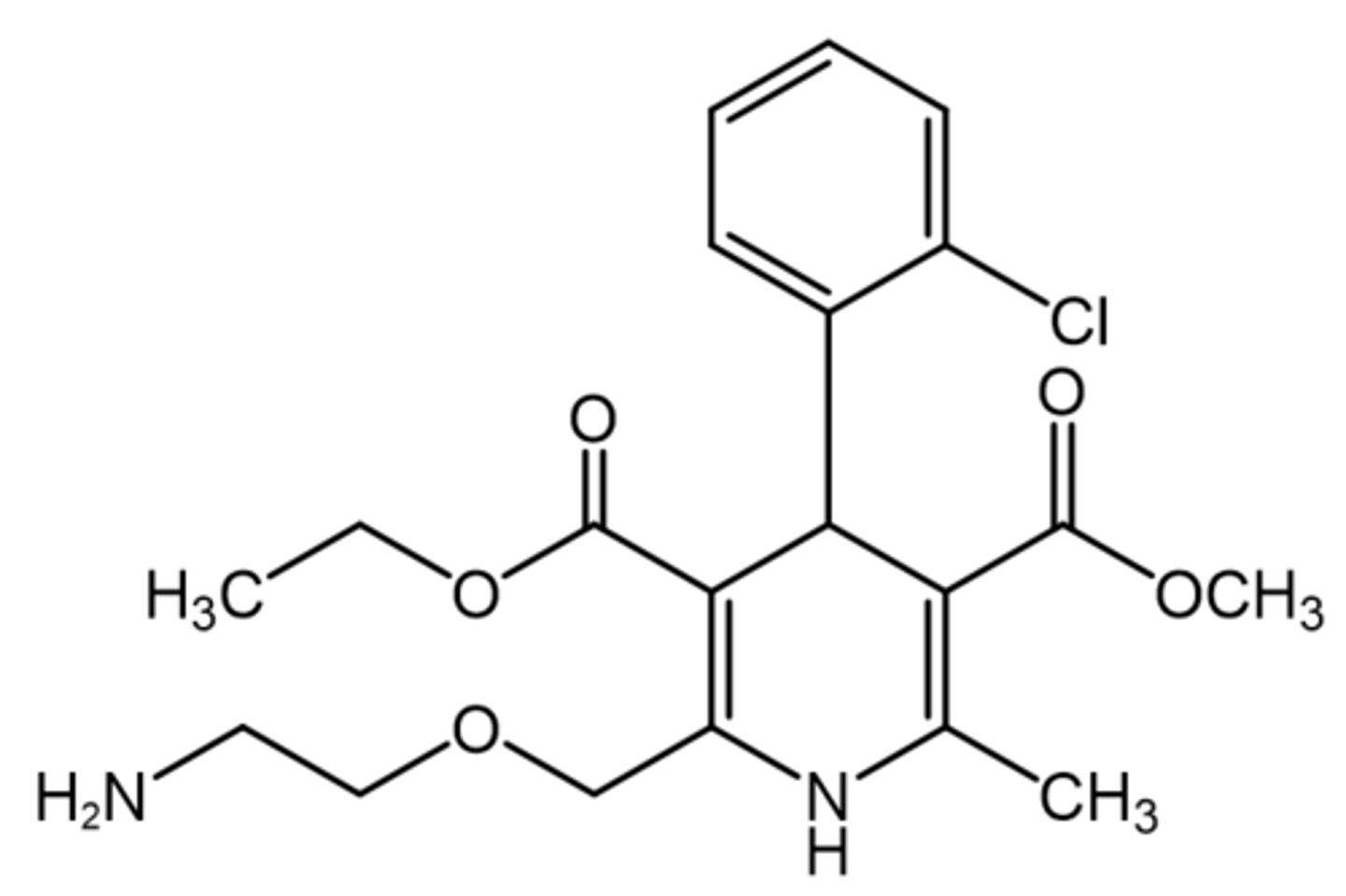
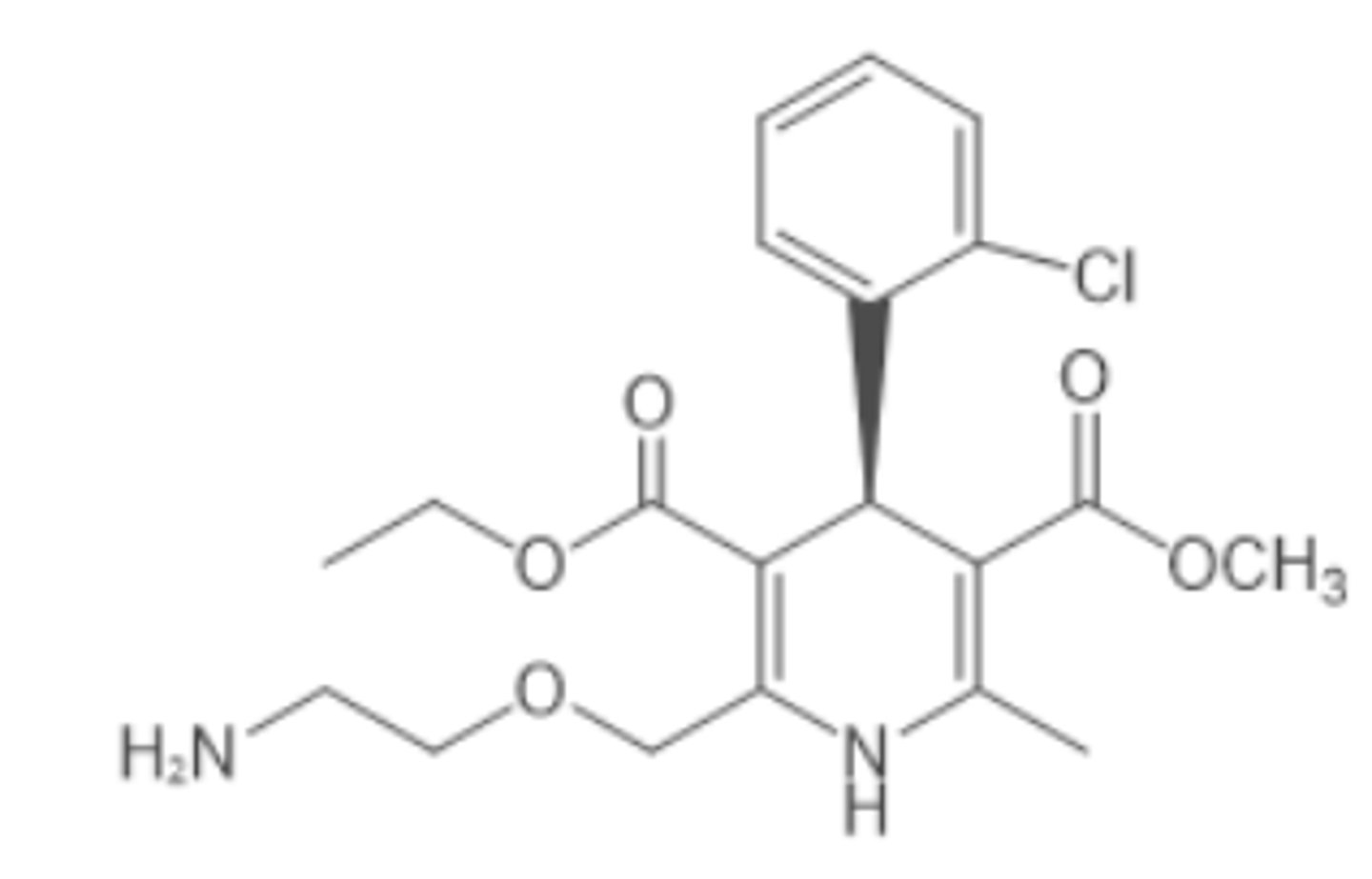
Amlodipine
Asymmetric 1,4-DHP
Ortho group on C4 phenyl= optimal
Better bioavailability than other DHPs; circumvents metabolism the most
Levamlodipine
Asymmetric 1,4-DHP
Enhanced potency by altering groups at R5 (bottom right ether)
t1/2 = 30 – 50 hours
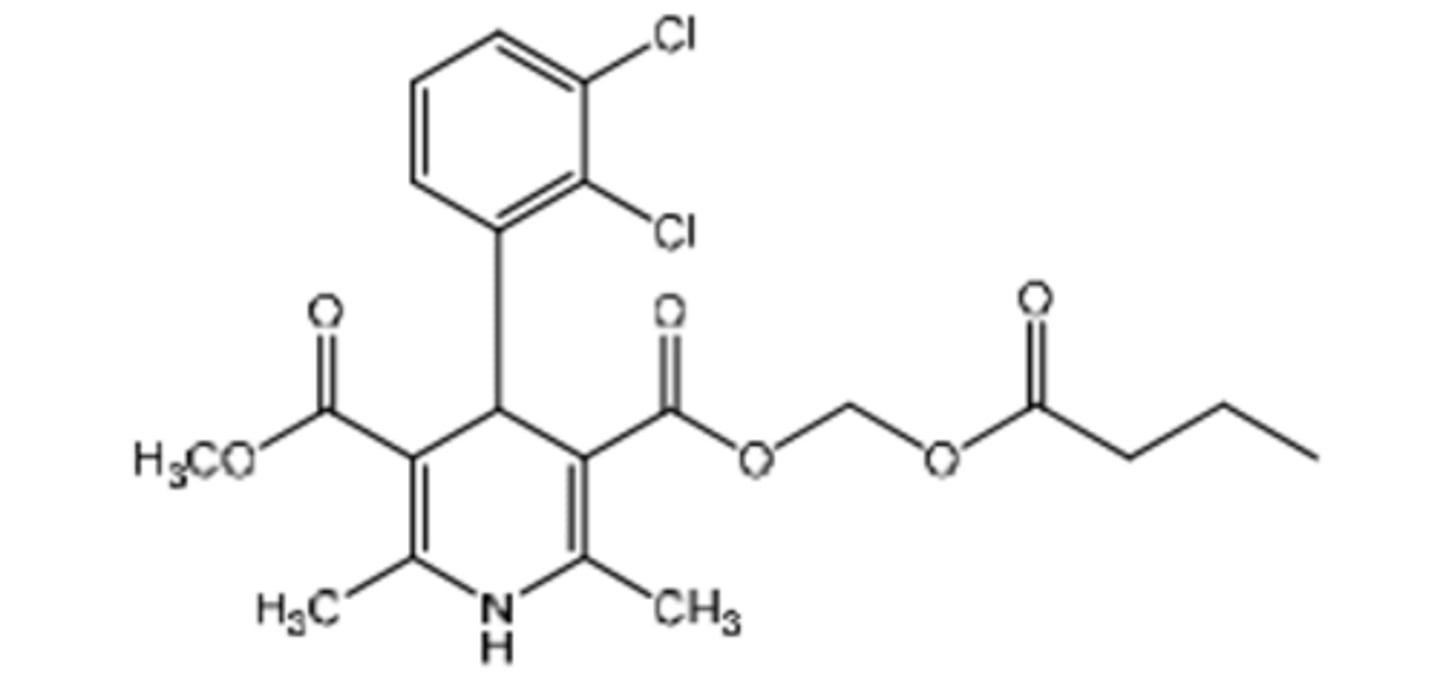
Clevidipine Butyrate
Asymmetric 1,4-DHP
Soft drug!! (Similar to frlopdipine)
IV only
Ultra–short acting (rapid onset & offset); t1/2: 1-15 minutes
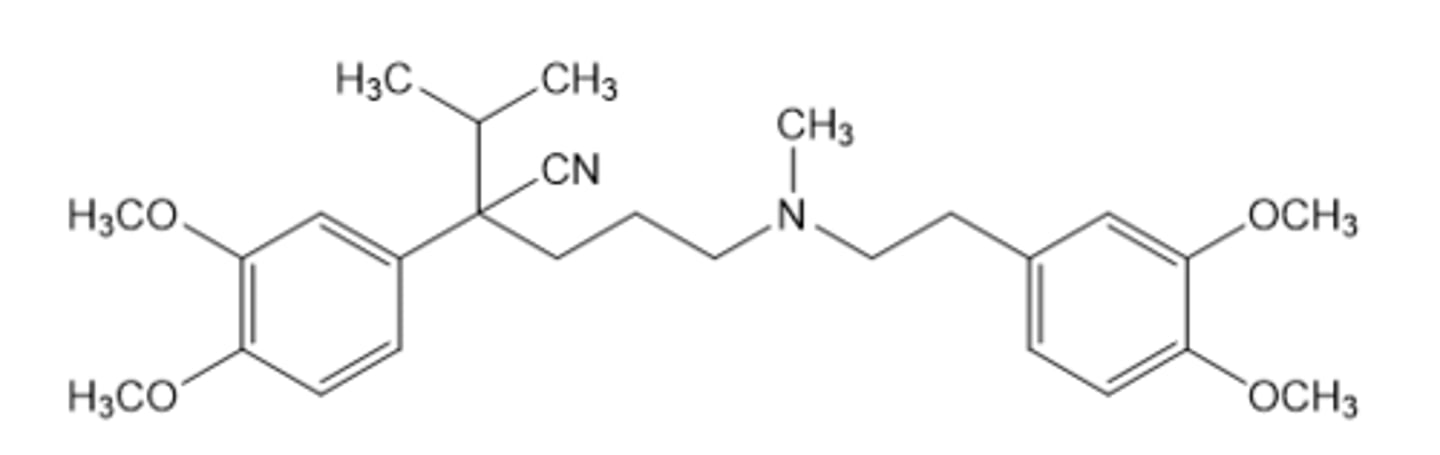
Verapamil
phenylalkylamine (non-DHP CCB)
in addition to hypertension, angina, and arrhythmias Verapamil is also used for the treatment of...
1. supraventricular tachycardia (rapid and regular)
2. atrial fibrillation (irregular).
•It is also used off-label for migraine and cluster headache prevention.
t1/2 = 3 to 7 hours
Metabolized by CYP3A4 9demethylated at N in the middle) to norverampamil
--t1/2 = 5 to 13 hours (20% potency)
S isomer is 10-20x more potent but more subject to 1st pass metabolism
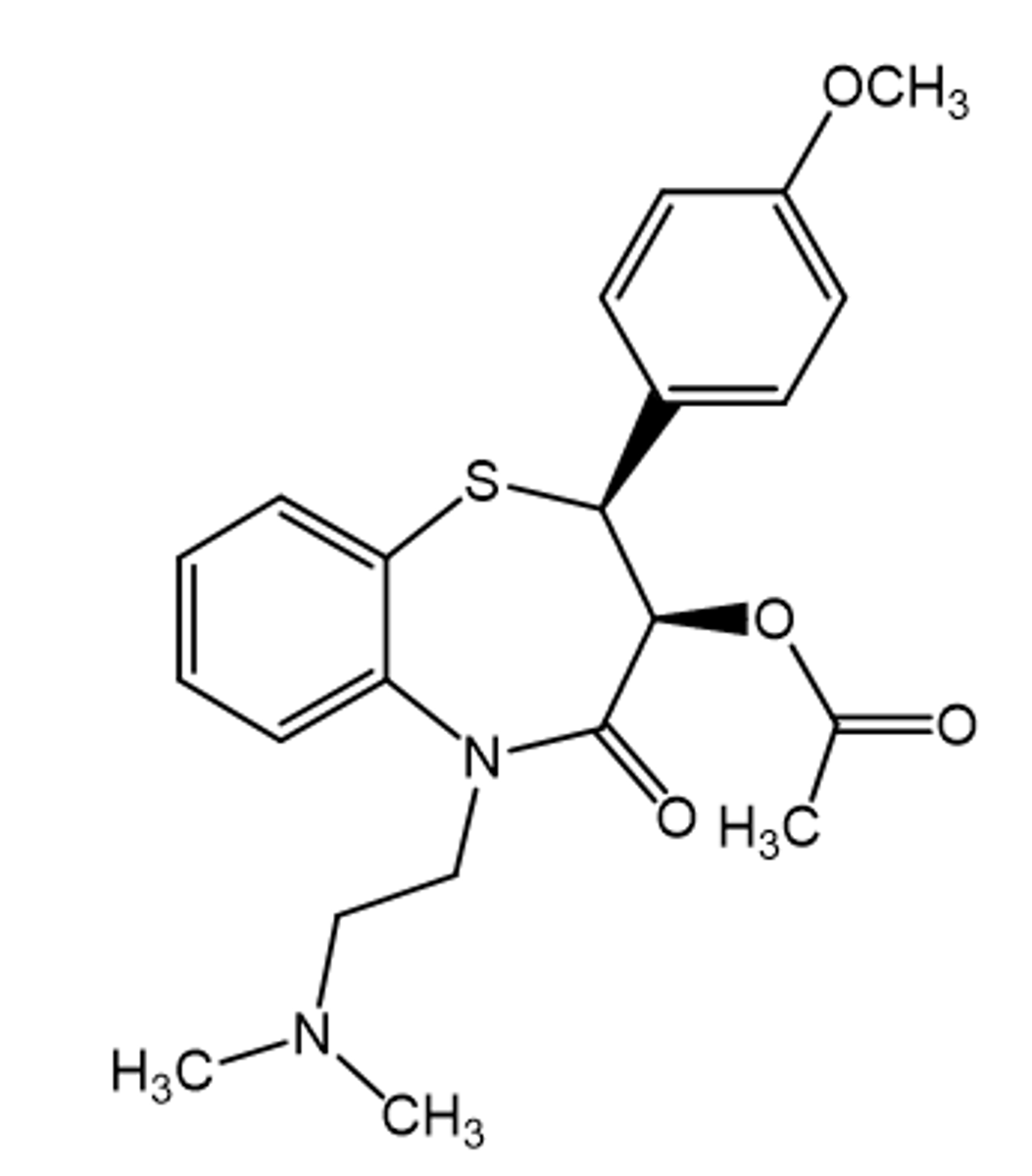
Diltiazem
benzothiazepine (non-DHP CCB)
•preferred for patients who need treatment for hypertension and cardiac issues -> more balanced yet less robust effect
can be allosterically coupled with 1,4-DHPs
Metabolized by esterases, CYP3A4 (N-Demethylation), and CYP2D6 (O-Demethylation)
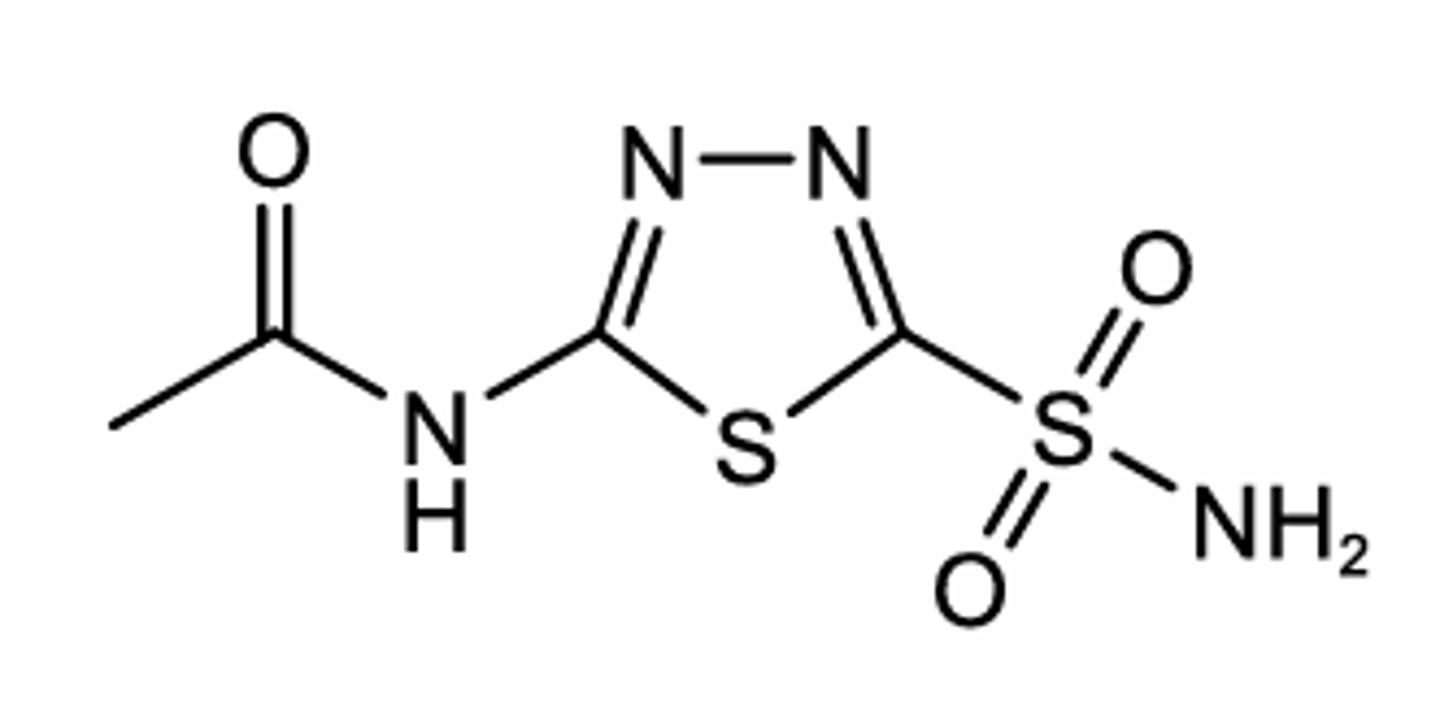
Acetazolamide
Carbonic Anhydrase Inhibitor diuretic (PCT)
Oral (ER capsule/Tablet/powder for injection)
Tx Nephrogenic Diabetes insipidus Tx
Oral form used off label for Primary hypokalemic and hyperkalemic periodic paralysis attacks
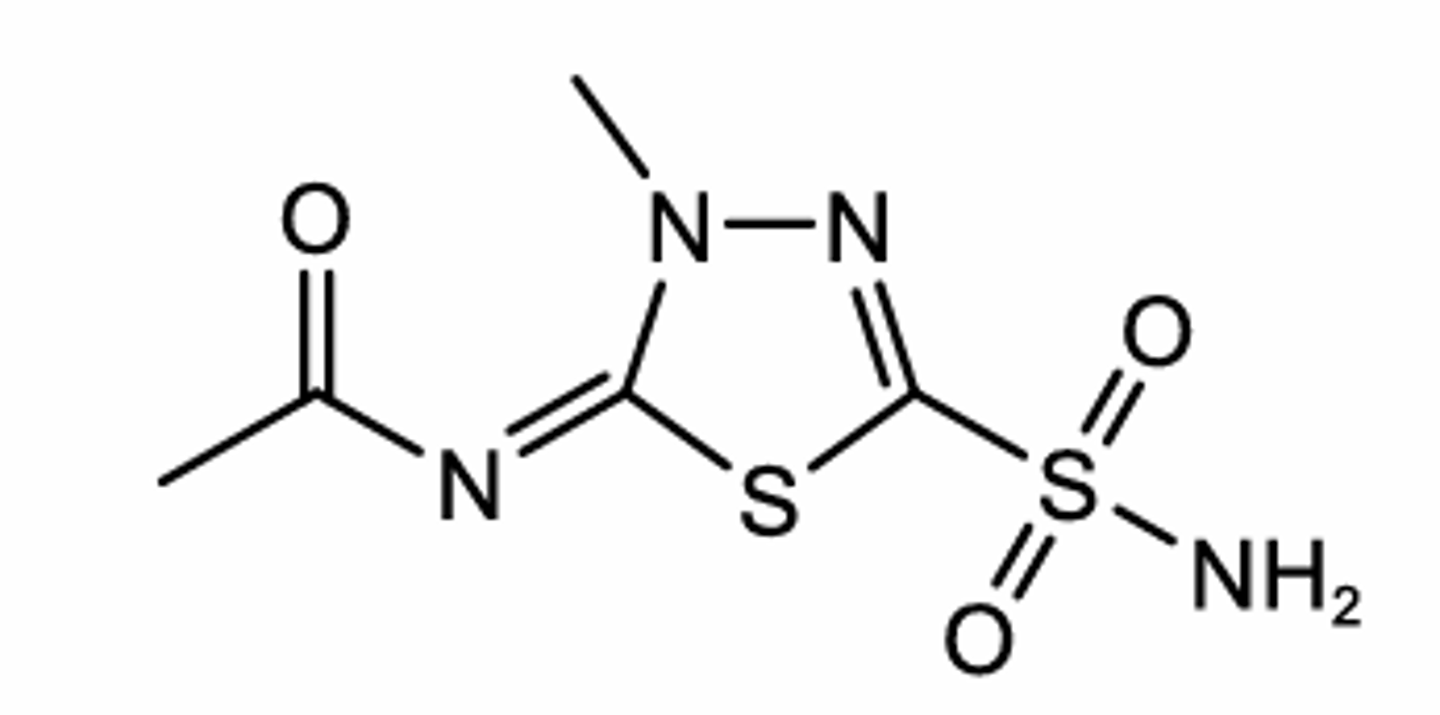
Methazolamide
Carbonic Anhydrase Inhibitor diuretic (PCT)
Oral tablet
Weaker than acetazolamide
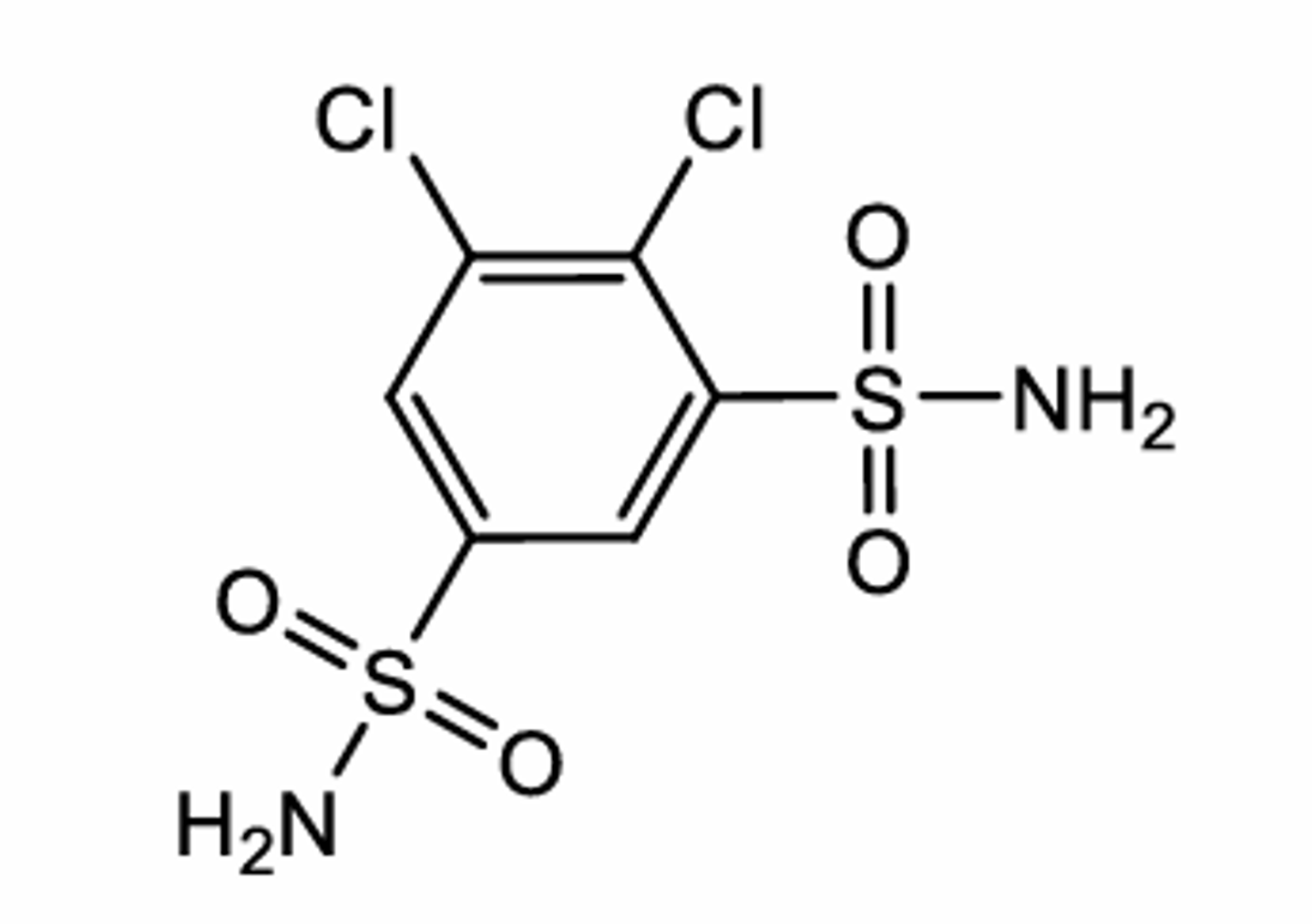
Dichlorphenamide
Carbonic Anhydrase Inhibitor diuretic (PCT)
Oral tablet
Used in Tx of Primary hypokalemic and hyperkalemic periodic paralysis attacks (opening Ca2+-activated K+ channels in myocytes allowing influx of potassium)
Dorzolamide
Carbonic Anhydrase Inhibitor diuretic
Ophthalmic solution
Tx of open-angle glaucoma
Brinzolamide
Carbonic Anhydrase Inhibitor diuretic
Ophthalmic solution
Tx of open-angle glaucoma
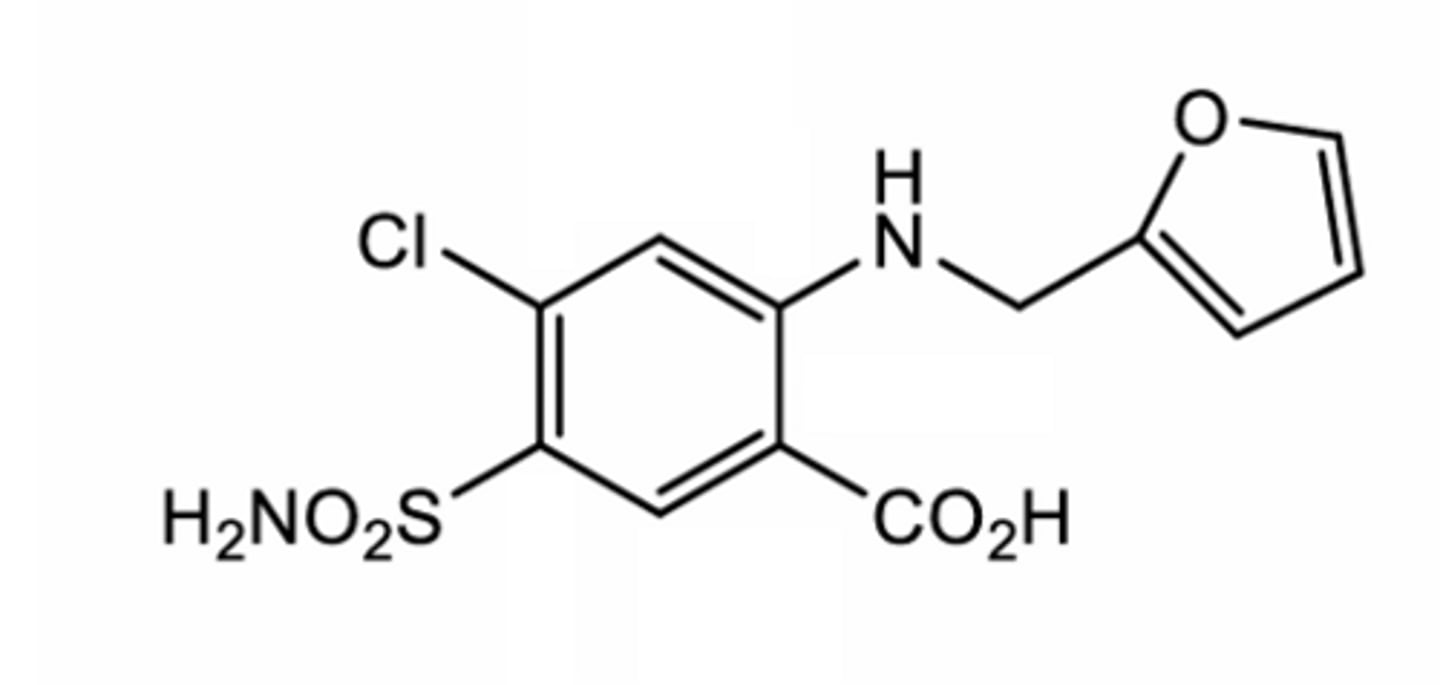
Furosemide
Loop diuretic (TAL)
Oral, IV, Or Sc infusion
Bumetanide
Loop diuretic (TAL)
Most potent: 40x more potent than furosemide
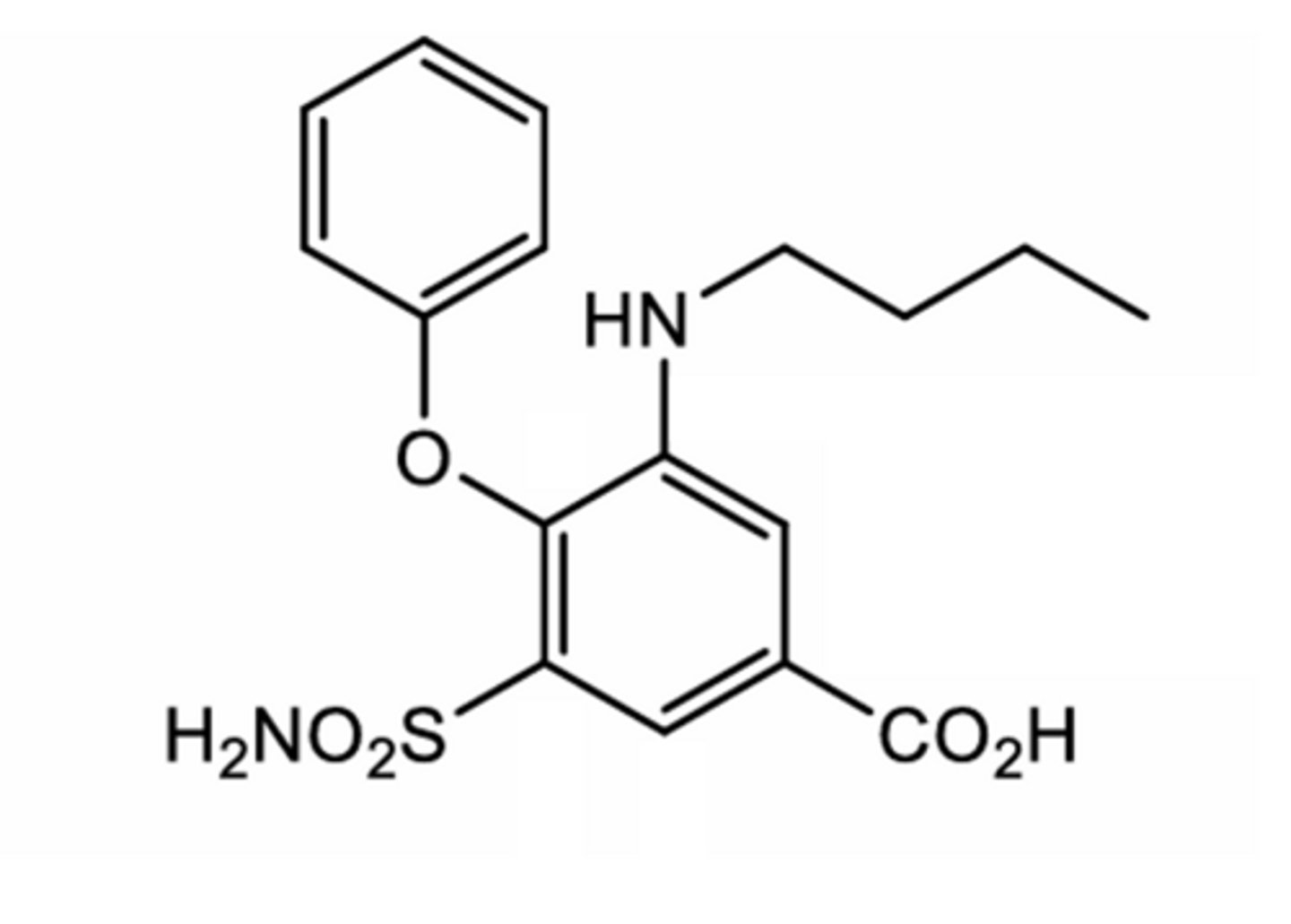
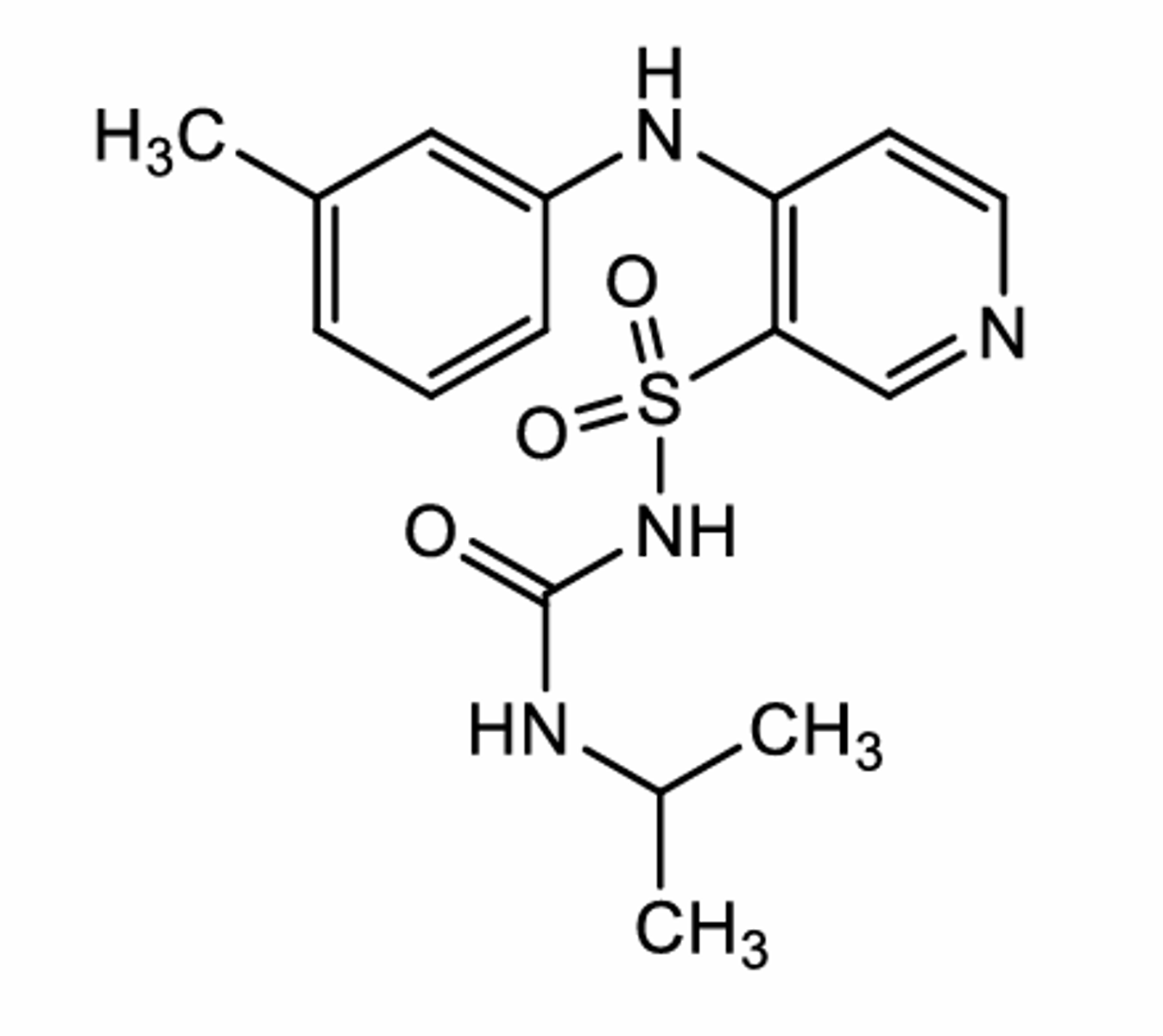
Torsemide
Loop diuretic (TAL)
Acidic proton pka= 7.1
Lonest T1/2
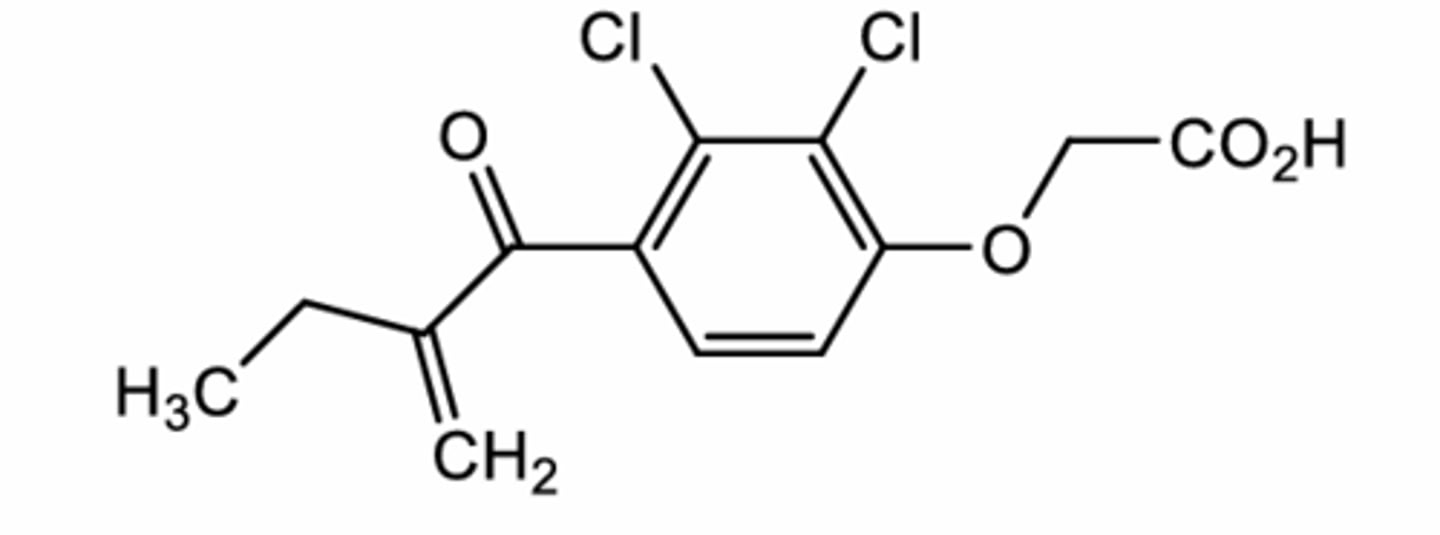
Ethacrynic Acid
Loop diuretic (TAL)
Lowest potency
Do not see much
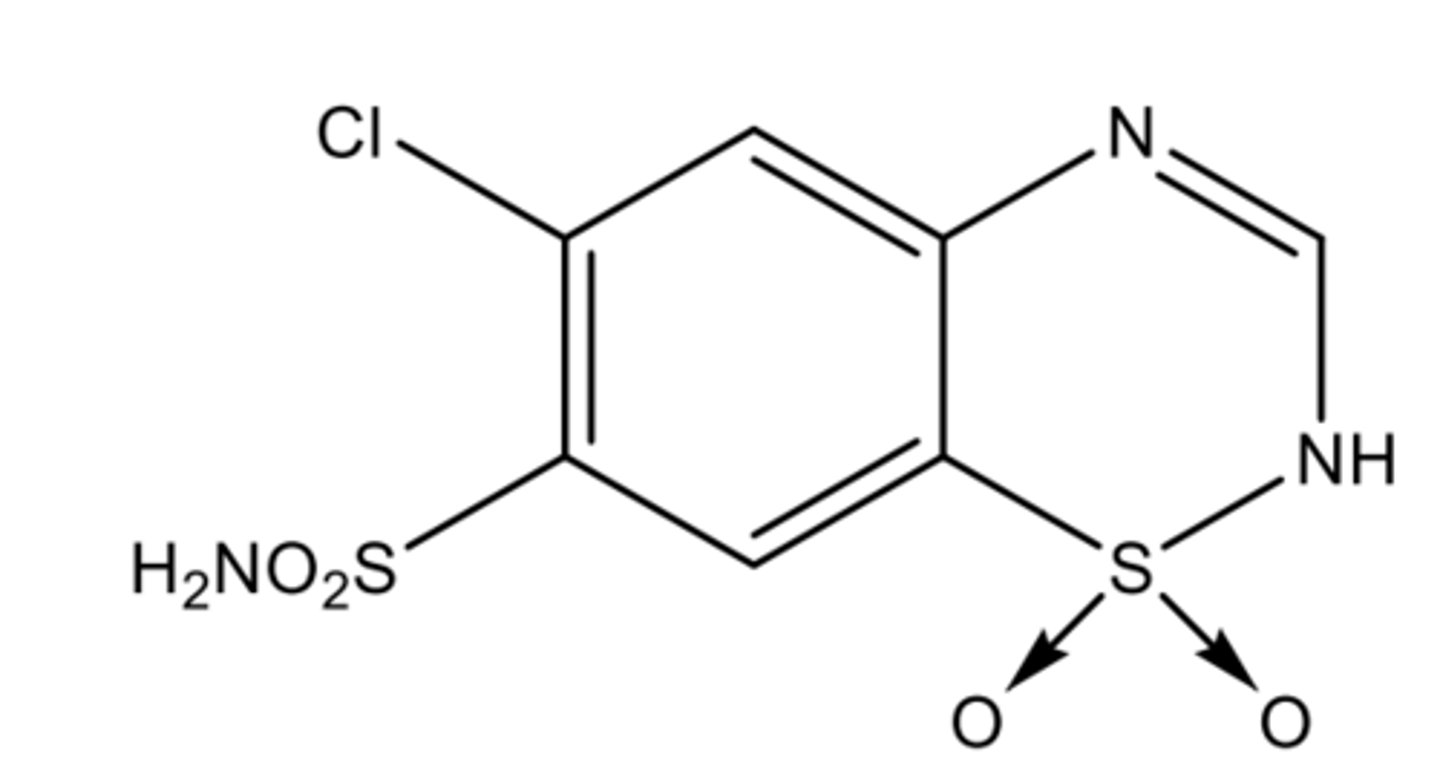
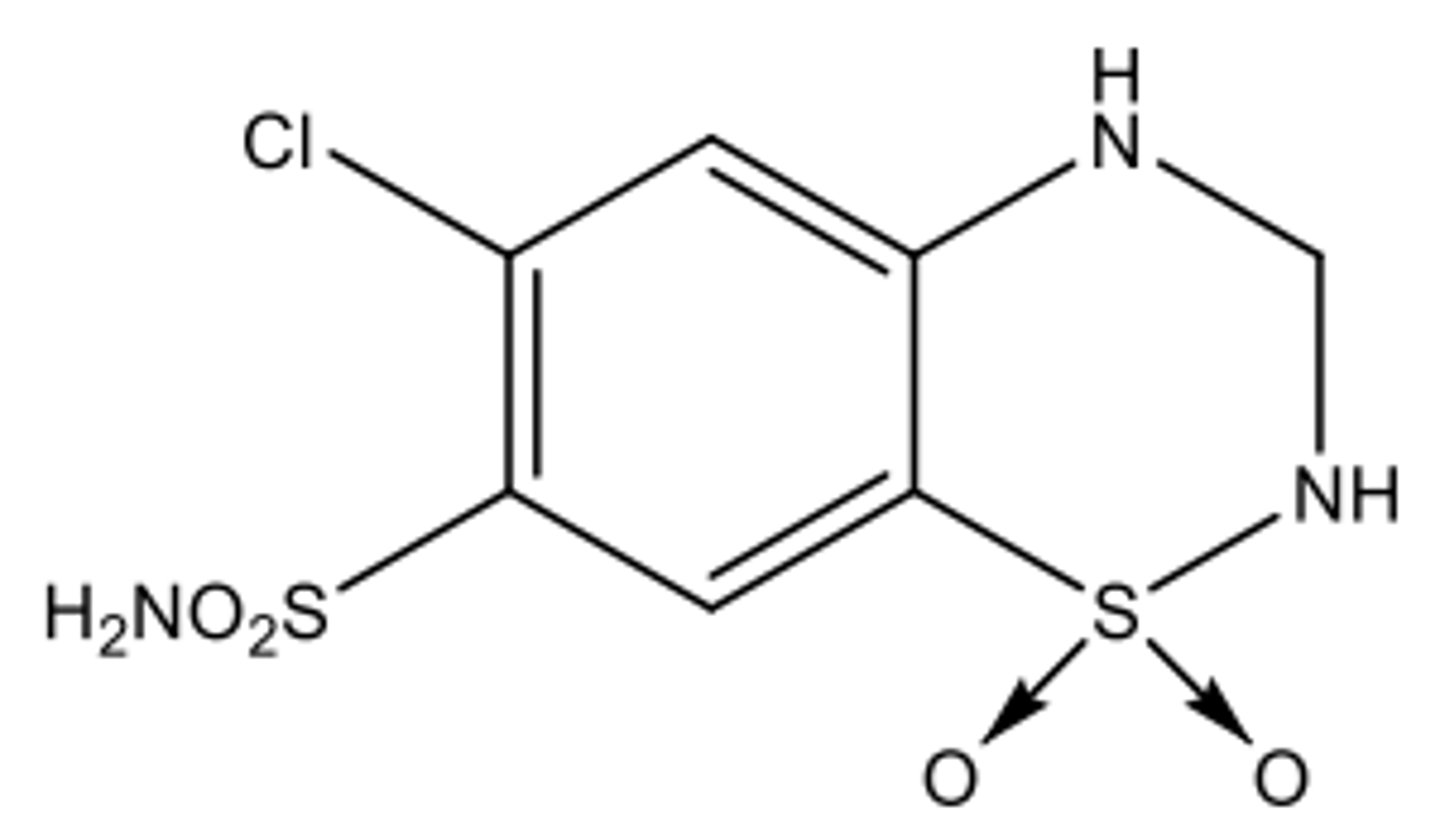
Chlorothiazide
Thiazide diuretic (DCT)
Only thiazide that can be formulated as a solution for injection (nitrogen next to the S gets protonated at pka 6.7)
Hydrochlorothiazide
Thiazide diuretic (DCT)
Decreased acidity from Chlorothiazide (pka 7.9)
Oral only
many combination products
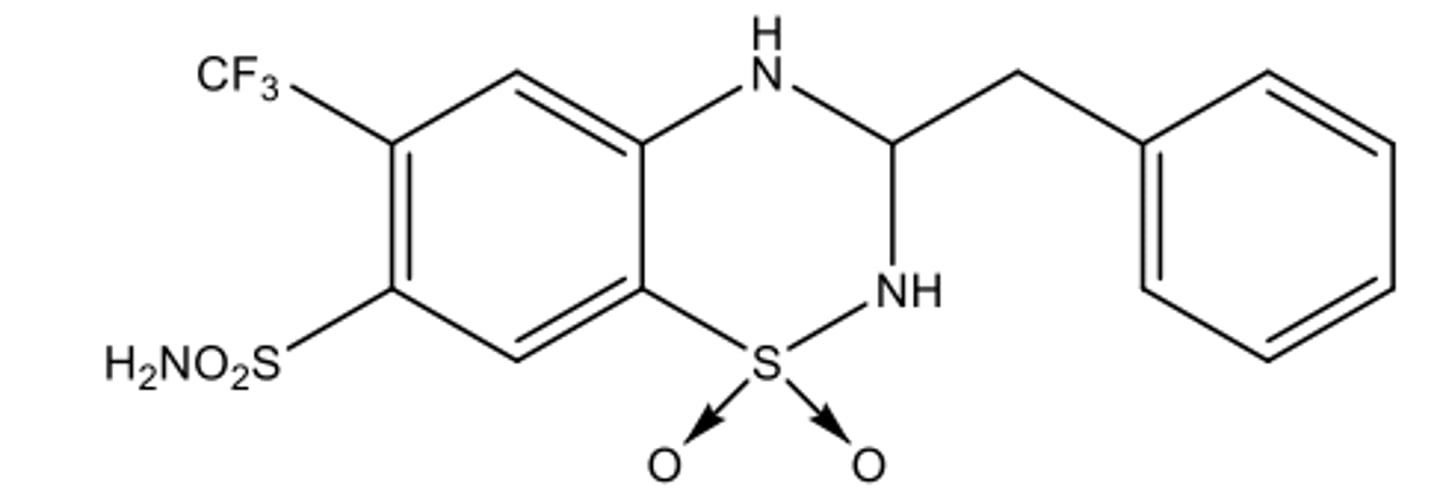
Bendroflumethiazide
Thiazide diuretic (DCT)
Fluoro group is more lipid soluble= longer DOA + Increased diuretic potency
Only available in combination with nadolol as "Corzide")
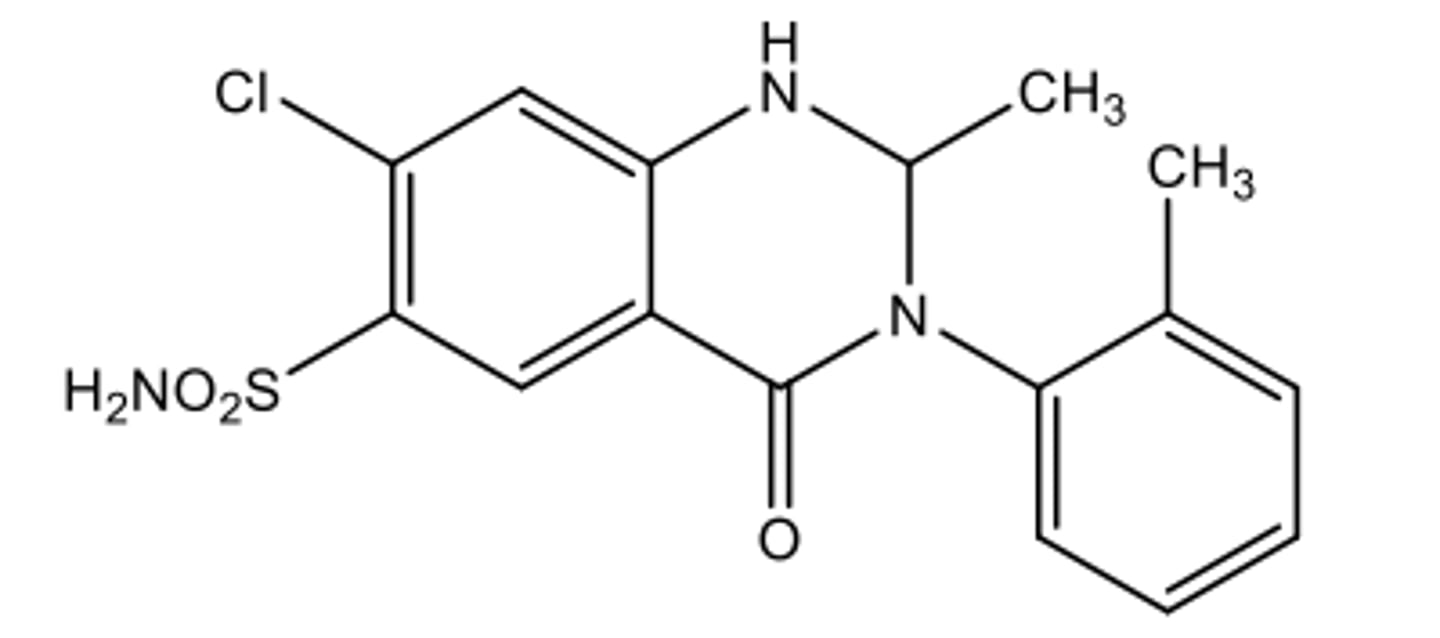
Metazolone
Thiazide-like diuretic (DCT)
Oral only
Can be used for edema in HF
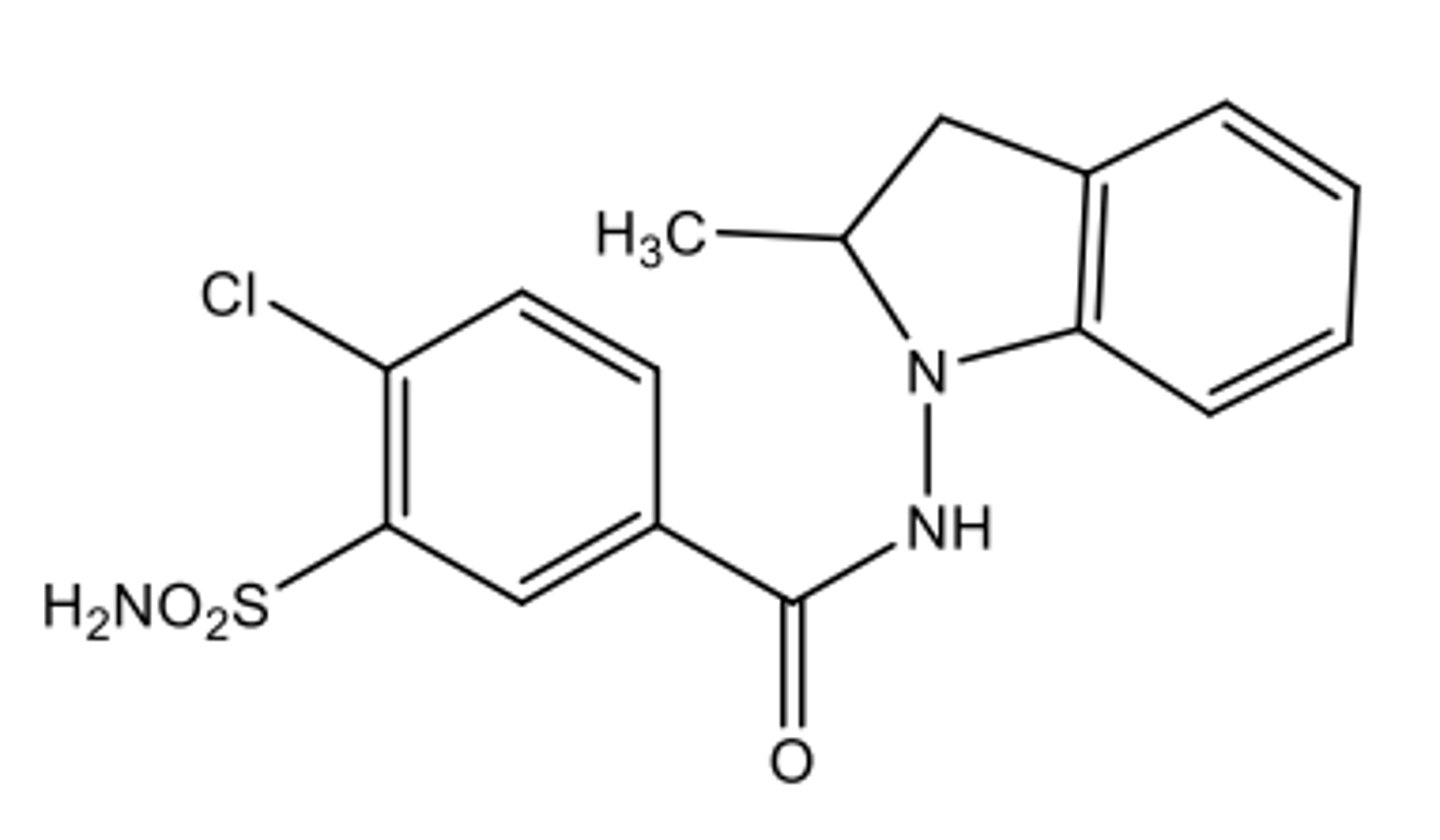
Indapamide
Thiazide-like diuretic (DCT)
Oral only
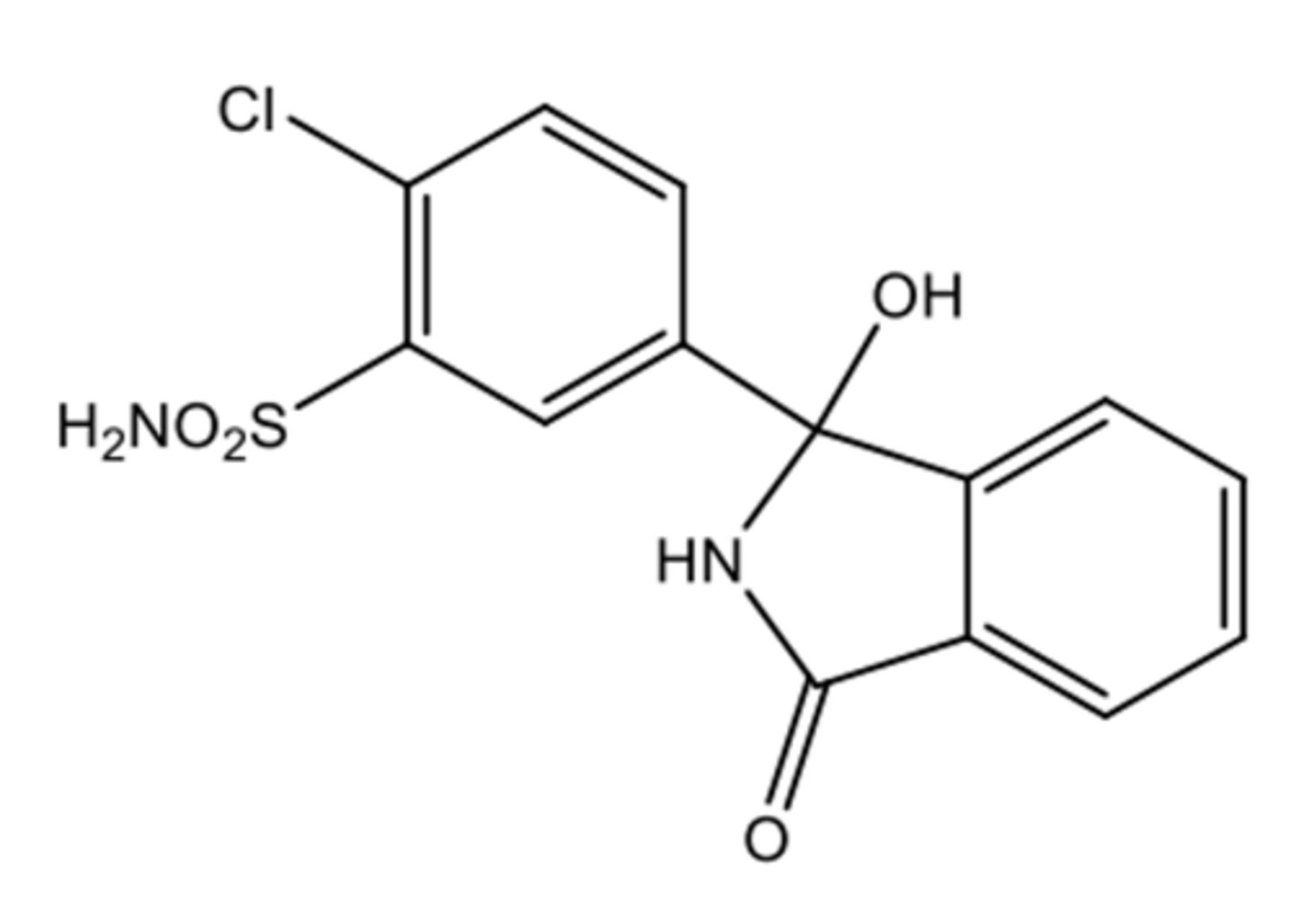
Chlorthalidone (masked carbonyl)
Thiazide-like diuretic (DCT)
in an equilibrium due to the masked carbonyl
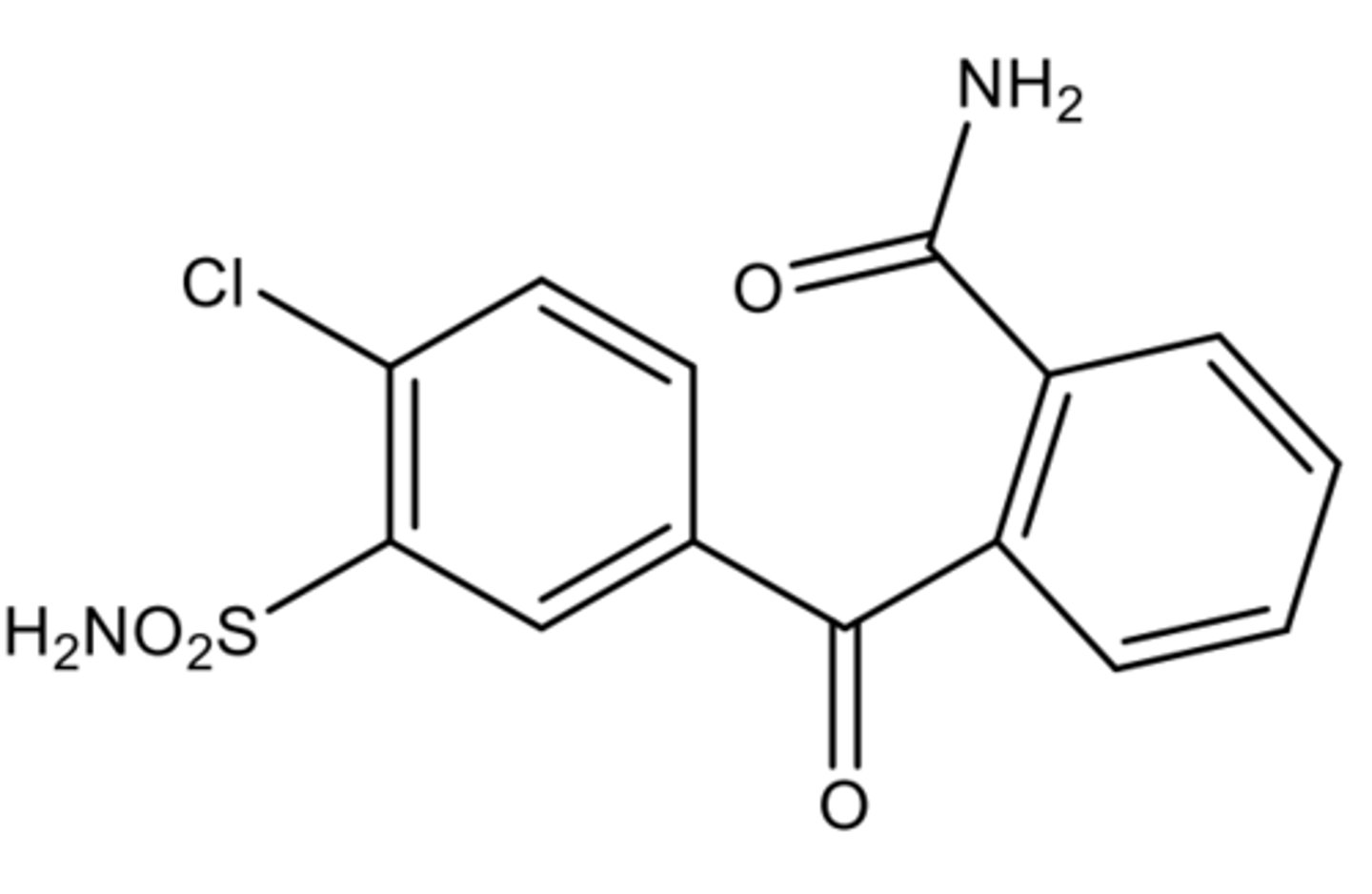
Chlorthalidone (unmaksed carbonyl)
in an equilibrium due to masked carbonyl
in an equilibrium due to masked carbonyl
Spironolactone
Potassium-Sparing Diuretic/MRA (DCT + CD)
2 active metabolites
Half-life after one dose is 1.3-2h but after multiple doses its 2-3 days
Used in HF because it blocks deleterious CV effects
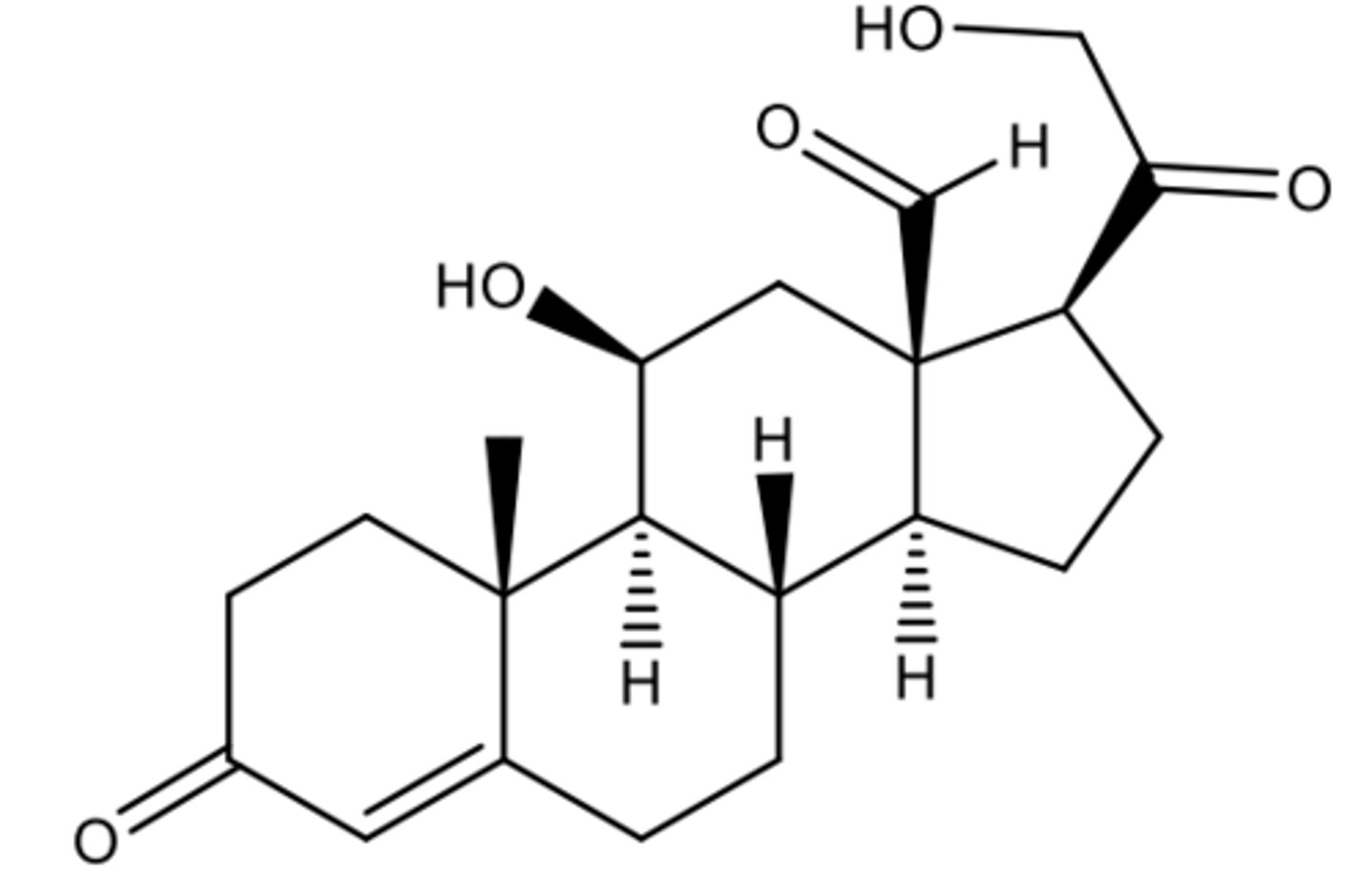
Aldosterone
The natural Potassium-Sparing Diuretic/MRA (DCT + CD)
Exists in the hemiacetal form
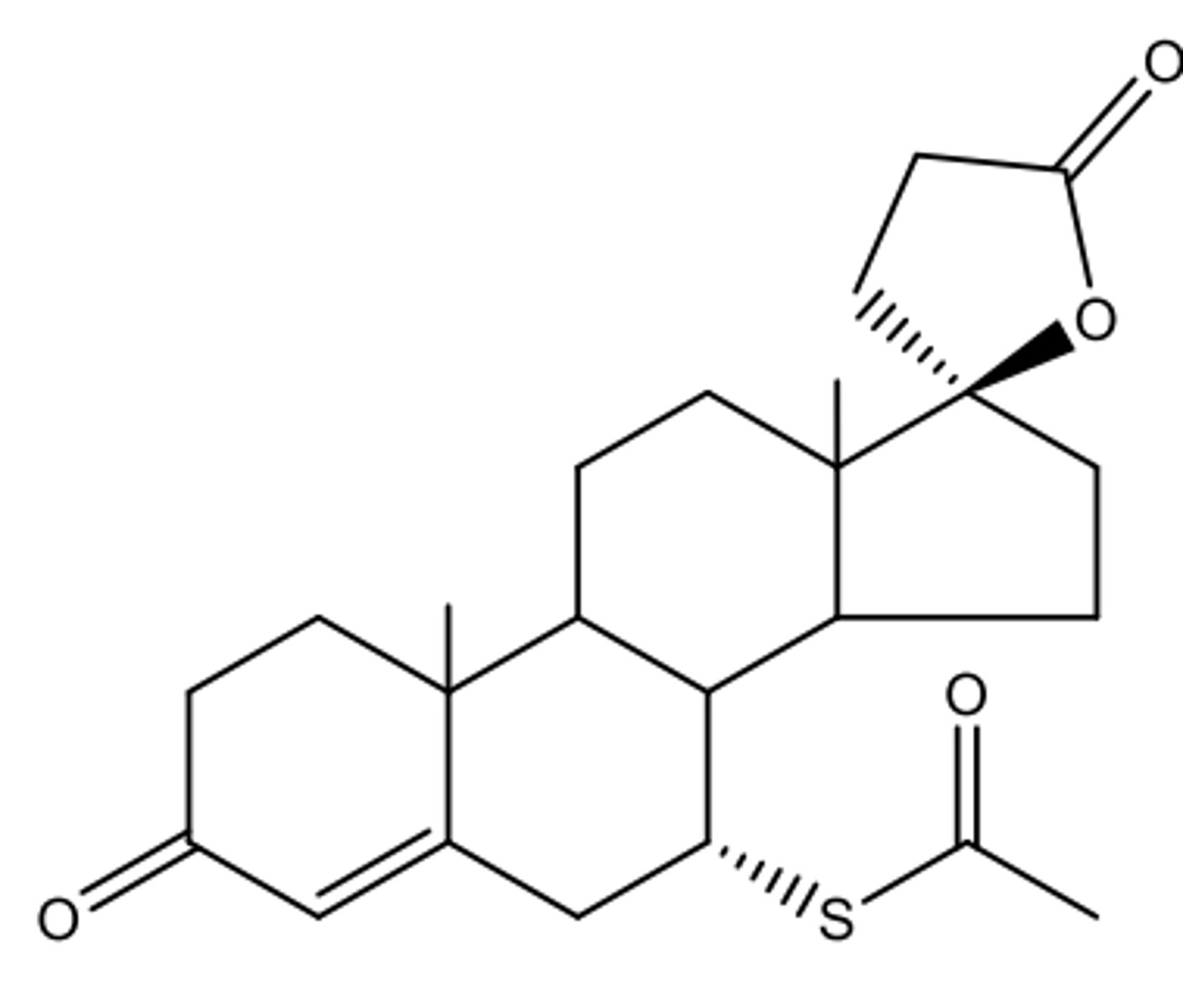
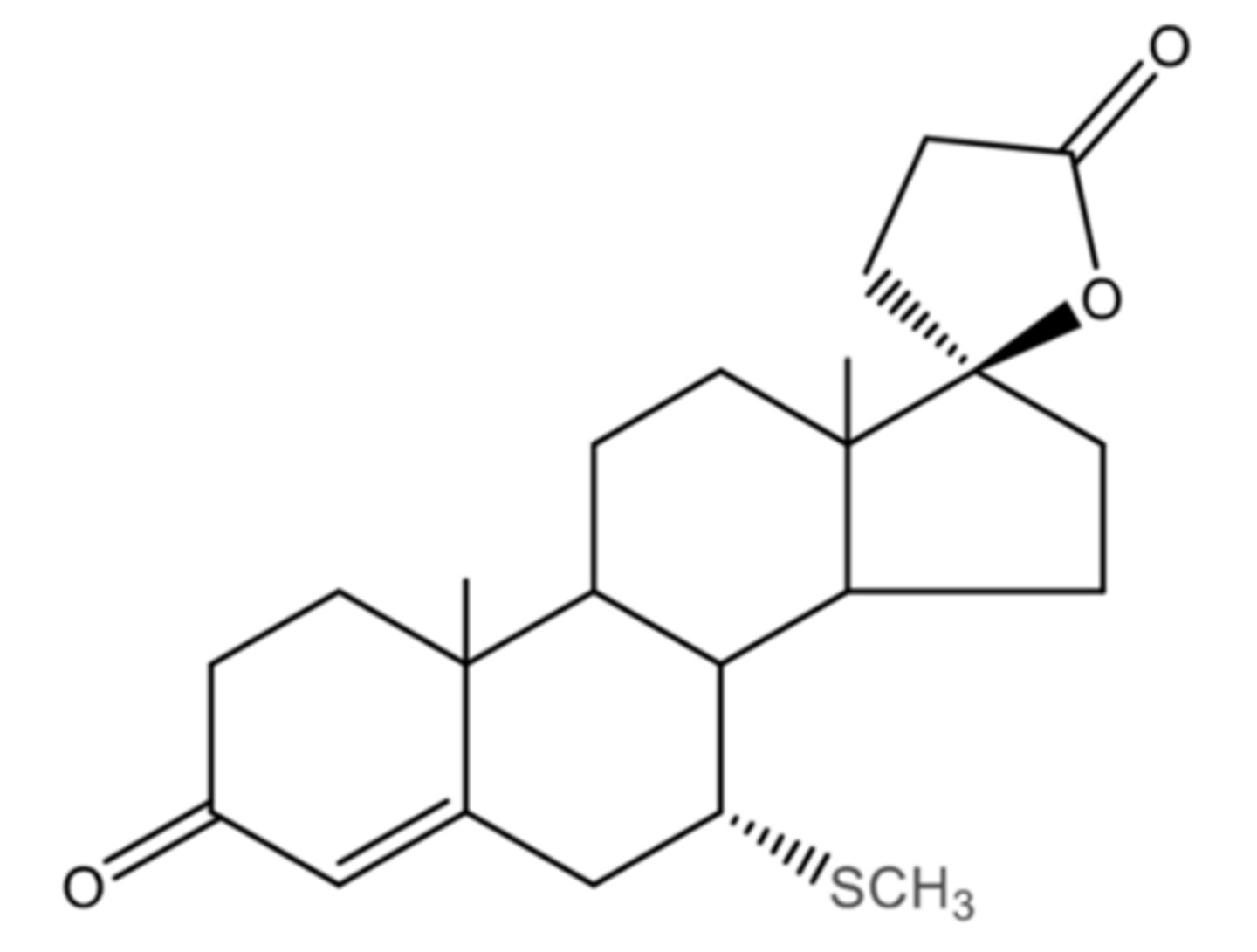
7a-Thiomethylspirolactone
Potassium-Sparing Diuretic/MRA (DCT + CD)
Major metabolite of spironolactone
Active
1. Thioester hydrolyzed
2. Thiol methylated
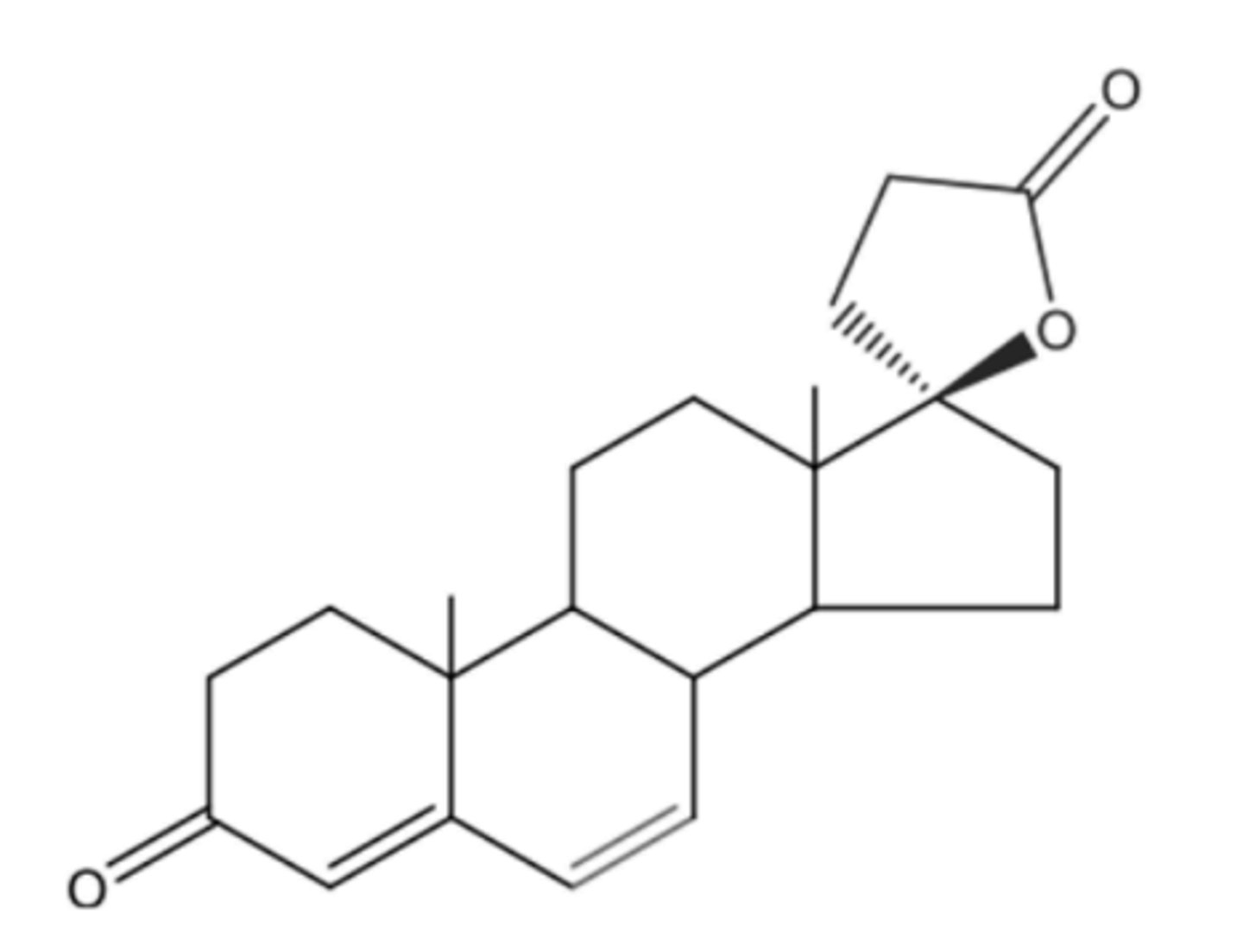
Canrenone
Potassium-Sparing Diuretic/MRA (DCT + CD)
Active (not major) metabolite of spironolactone
Lactone opens and closes (closed= active)
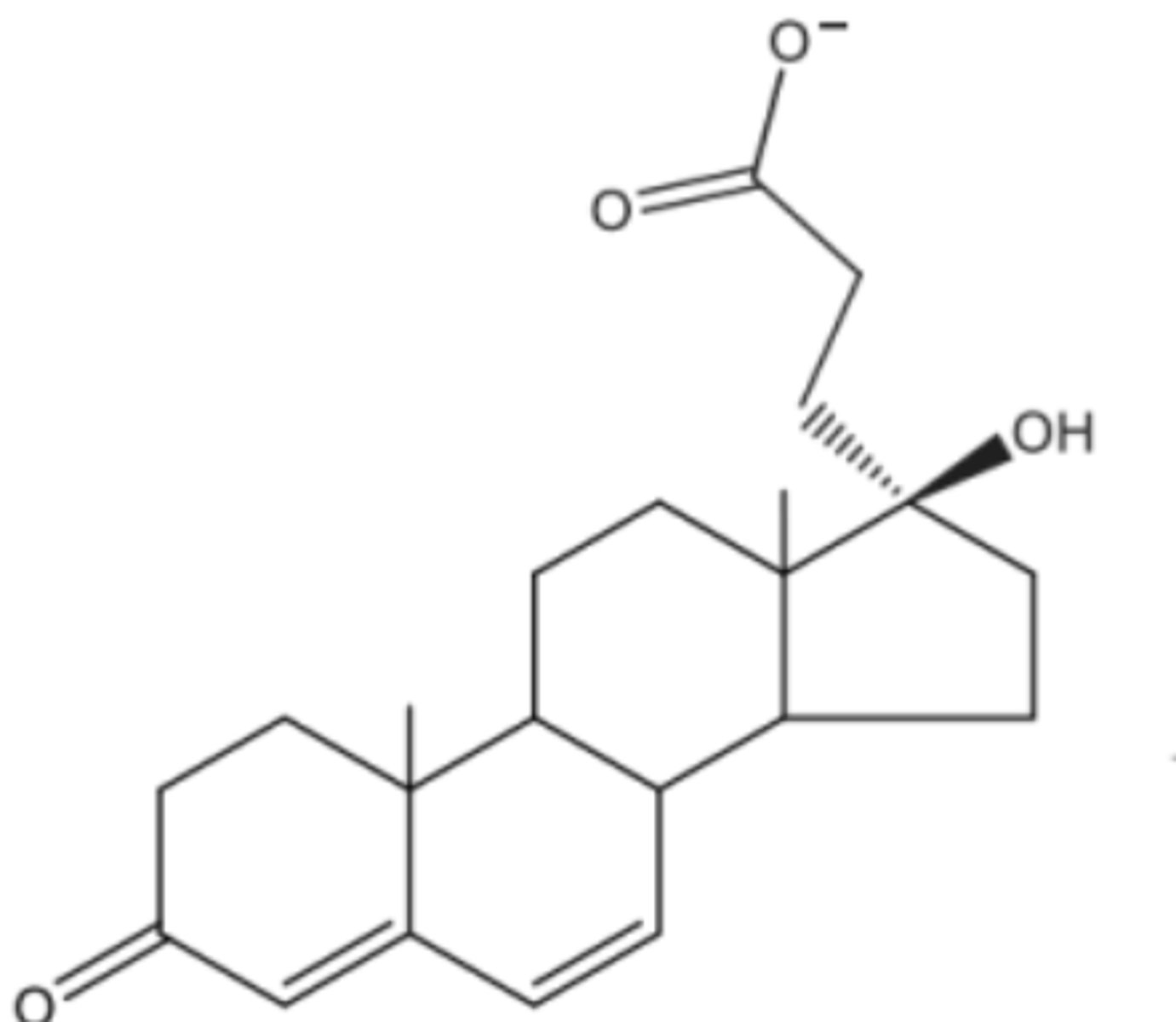
Canrenoate
Potassium-Sparing Diuretic/MRA (DCT + CD)
Active (not major) metabolite of spironolactone
Lactone opens and closes (open= inactive)
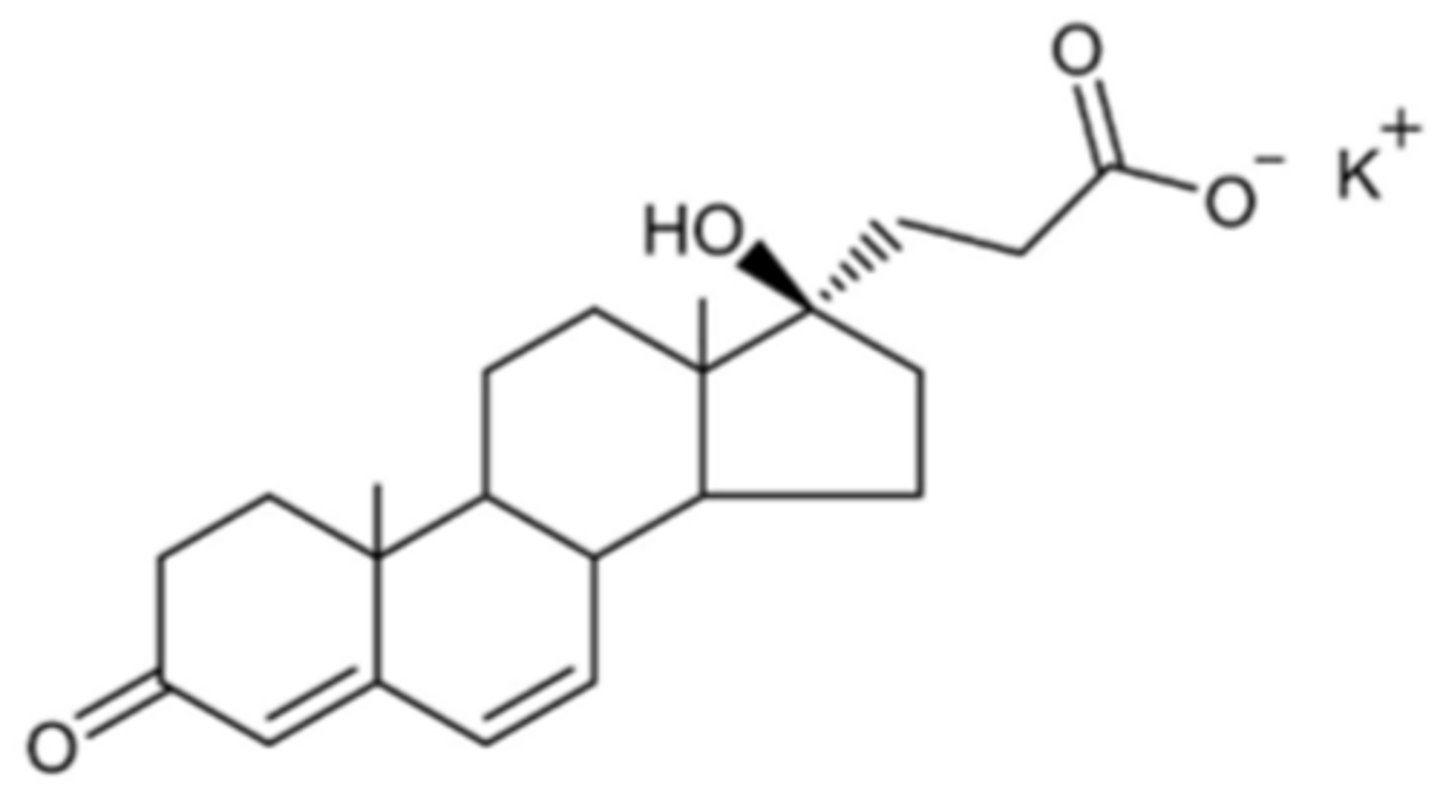
Potassium Canrenoate
Prodrug that gets turned into canrenoate:
active (not major) metabolite of spironolactone
not in the U.S.
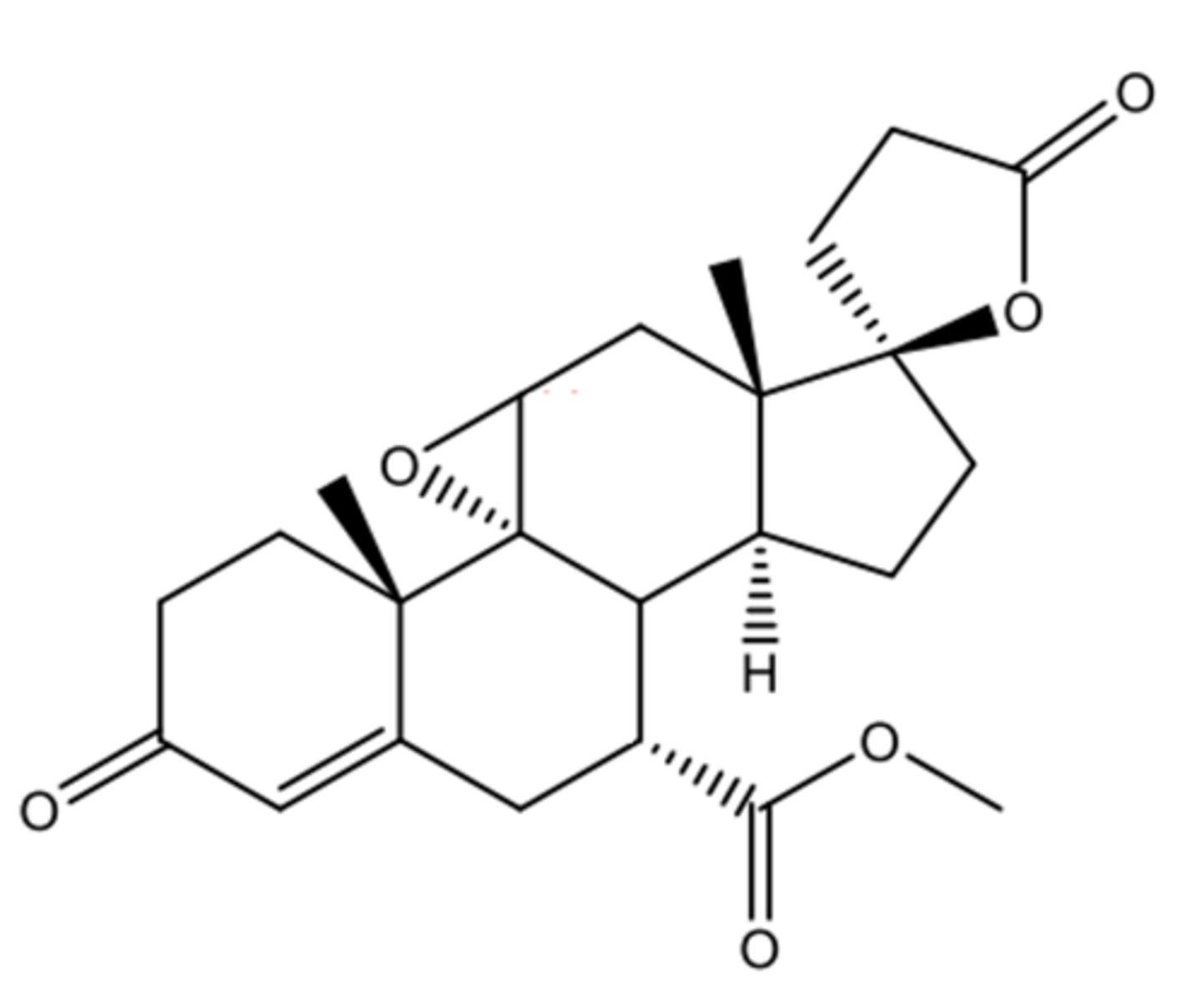
Eplerenone
Potassium-Sparing Diuretic/MRA (DCT + CD)
Selective Mineralocorticoid Receptor Antagonist
Epoxide and ester decrease its affinity, so its less potent but more selective
beneficial effects on long-term survival and cardiovascular outcomes
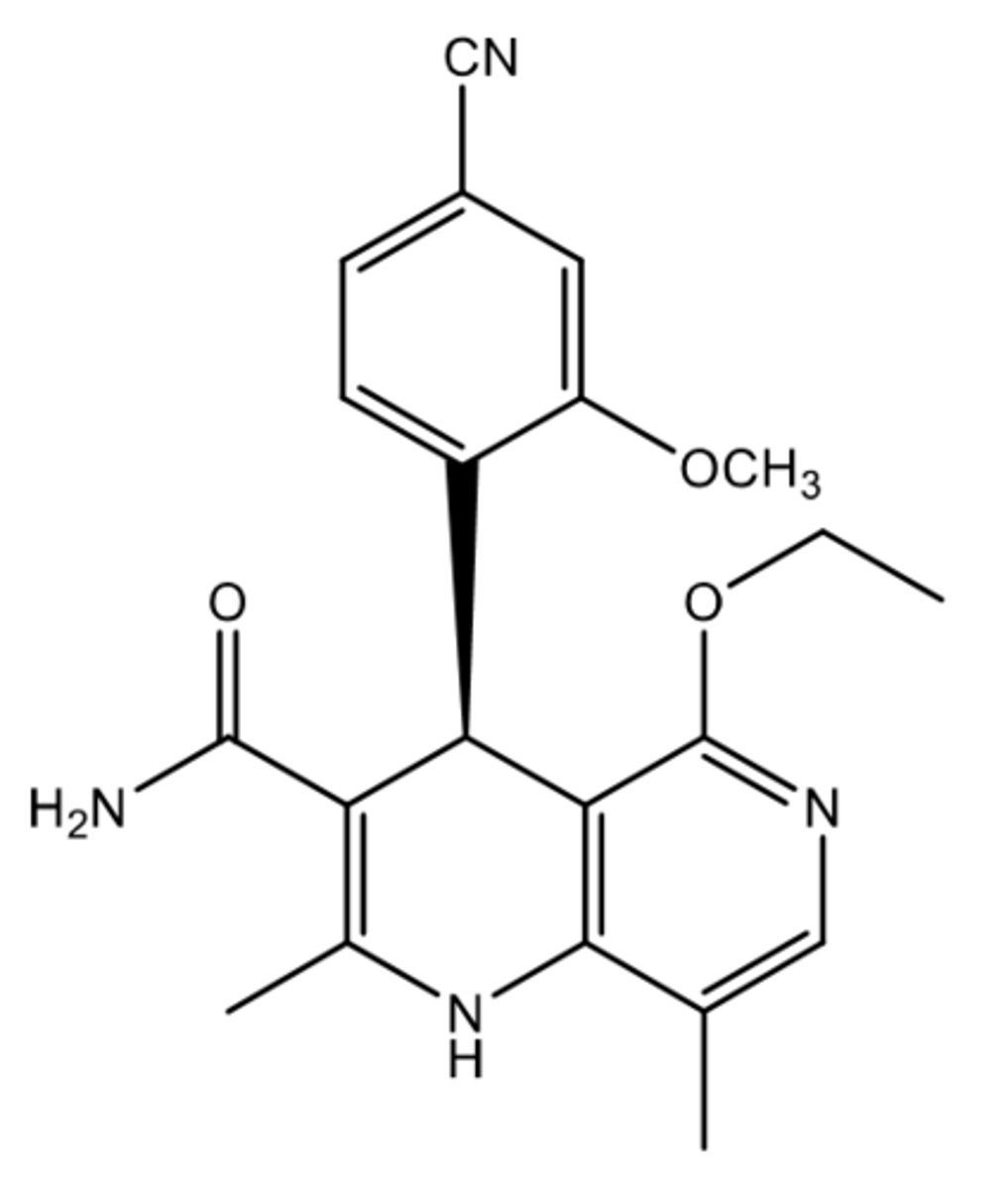
Finerenone
Potassium-Sparing Diuretic/MRA (DCT + CD)
Nonsteroidal selective Mineralocorticoid Receptor Antagonist
Indications:
• to reduce the risk of sustained eGFR decline, end-stage kidney disease, cardiovascular death, non-fatal myocardial infarction, and hospitalization for heart failure in adult patients with chronic kidney disease (CKD) associated with type 2 diabetes (T2D)
• to reduce the risk of cardiovascular death, hospitalization for heart failure, and urgent heart failure visits in adult patients with heart failure with left ventricular ejection fraction (LVEF) ≥ 40%
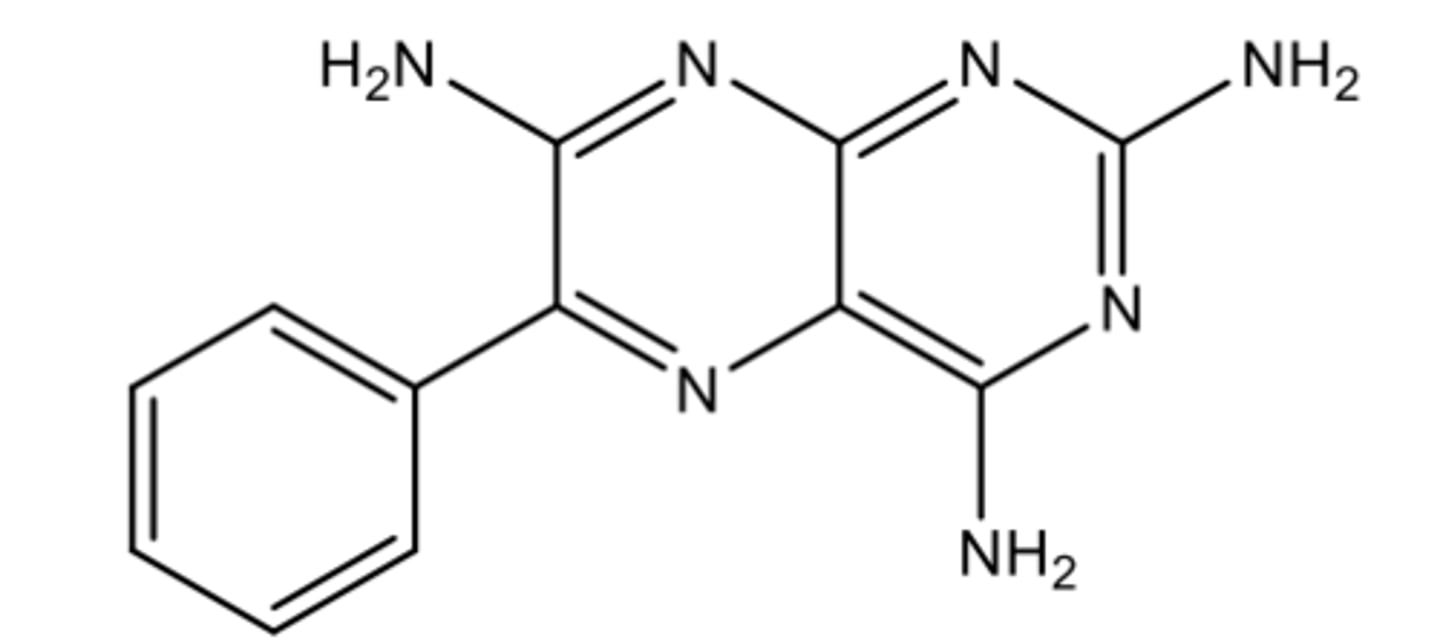
Triamterene
Potassium-Sparing Diuretic/MRA (DCT + CD)
Non-aldosterone Mineralocorticoid Receptor Antagonist
Gets para hydroxylated by CYP1A2 then conjugated to a sulfate (Sulfate conjugate is active)
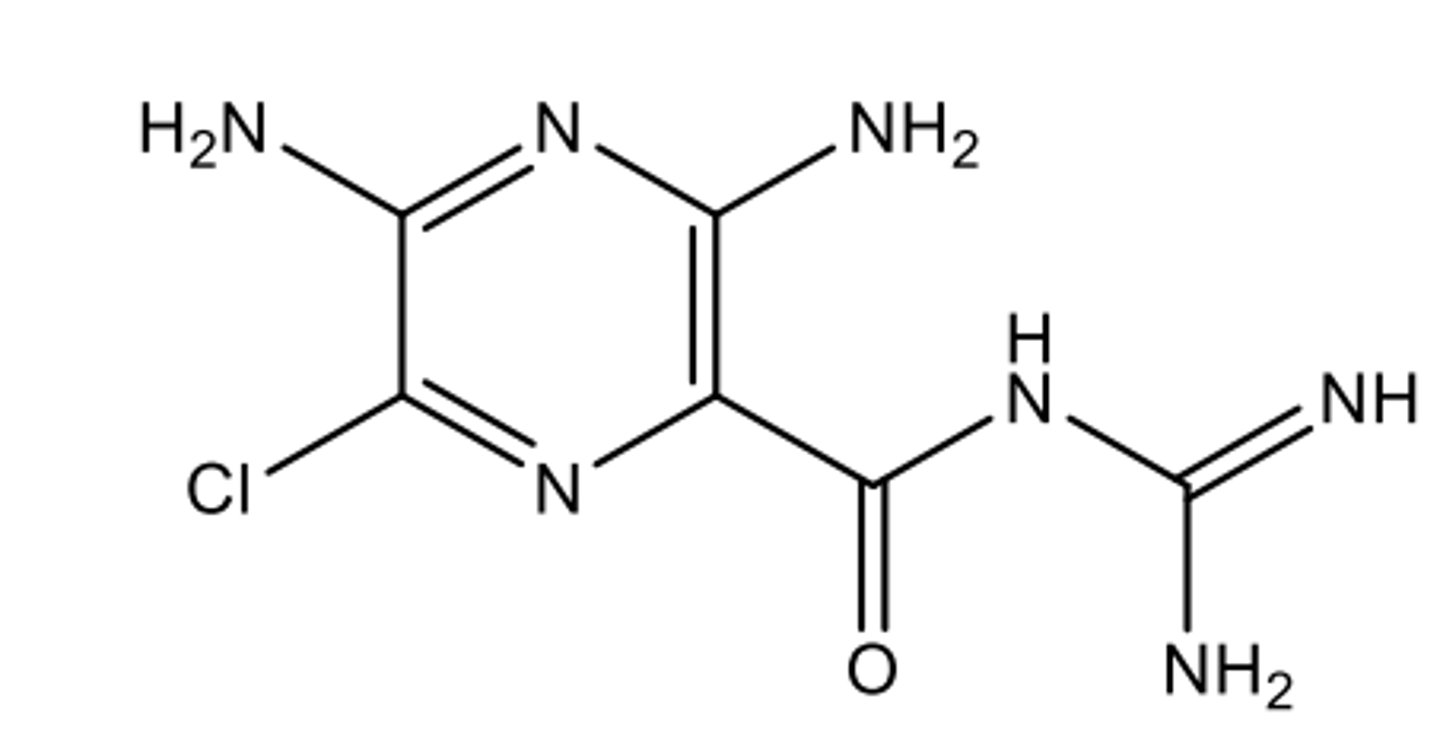
Amiloride
Triamterene
Potassium-Sparing Diuretic/MRA (DCT + CD)
Non-aldosterone Mineralocorticoid Receptor Antagonist
100x more potent than triamterene
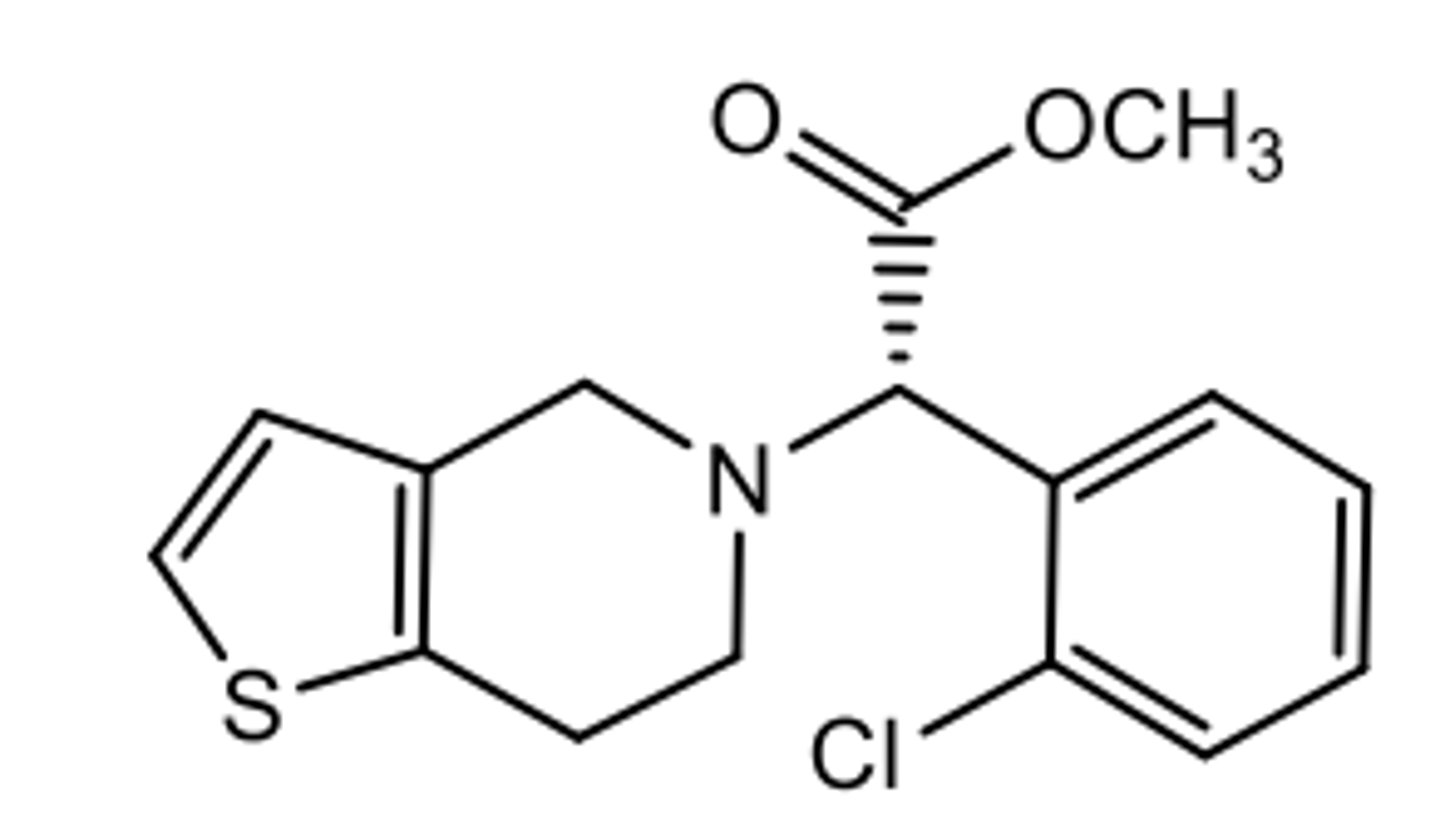
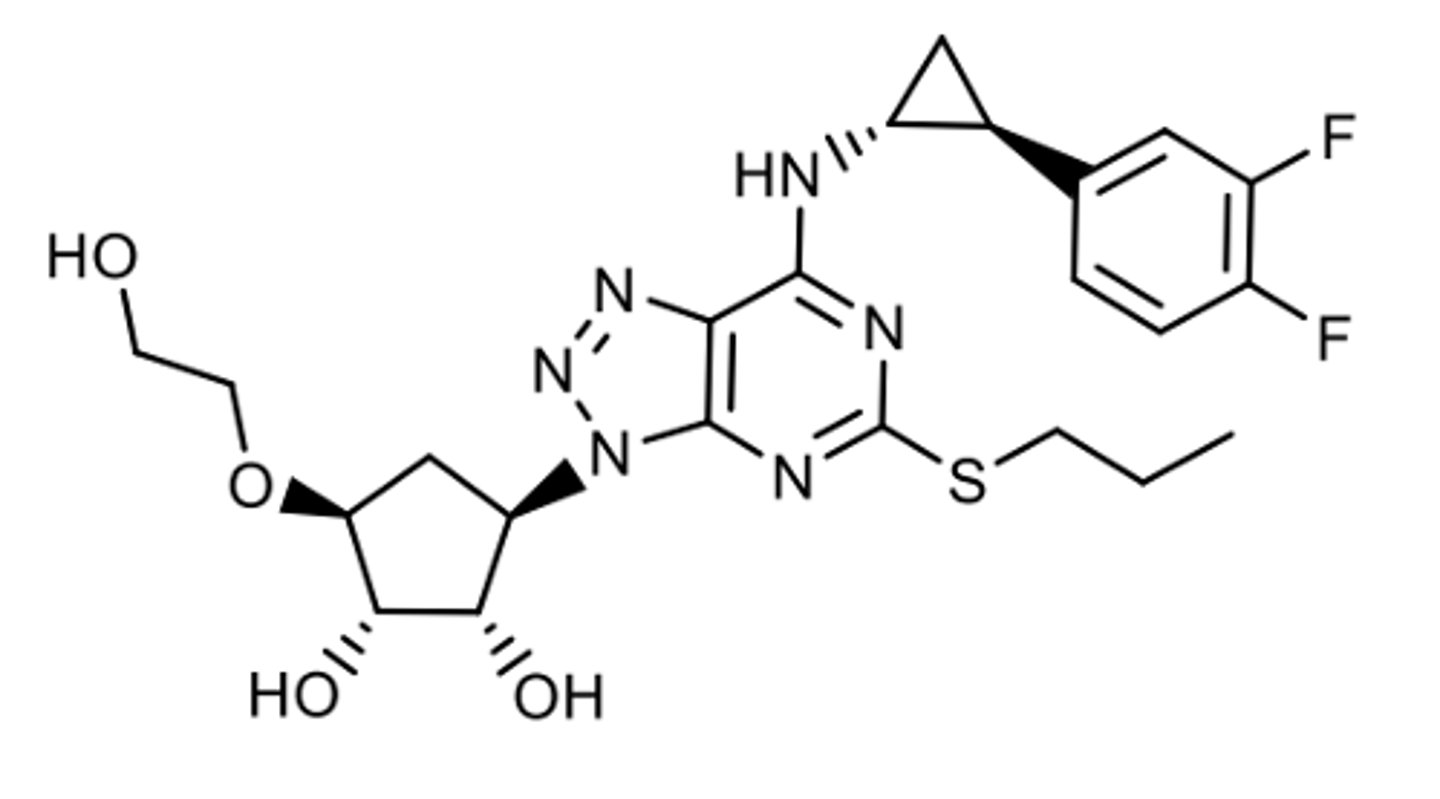
Clopidogrel
P2Y12 antagonist
Prodrug (main= CYP2C19)
Irreversible (forms covalent disulfide bond with the receptor)
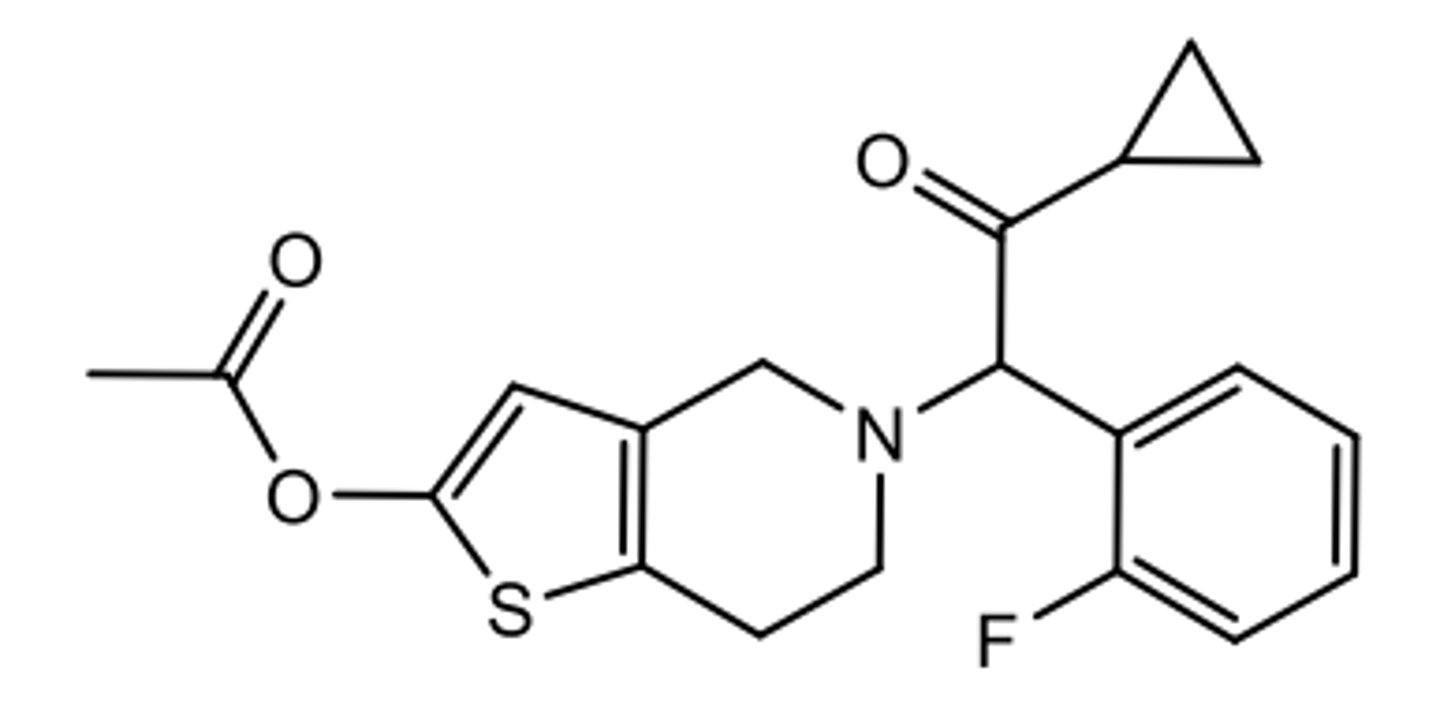
Prasugrel
P2Y12 antagonist
Prodrug (hCE2/hCE1)
Irreversible (forms covalent disulfide bond with the receptor)
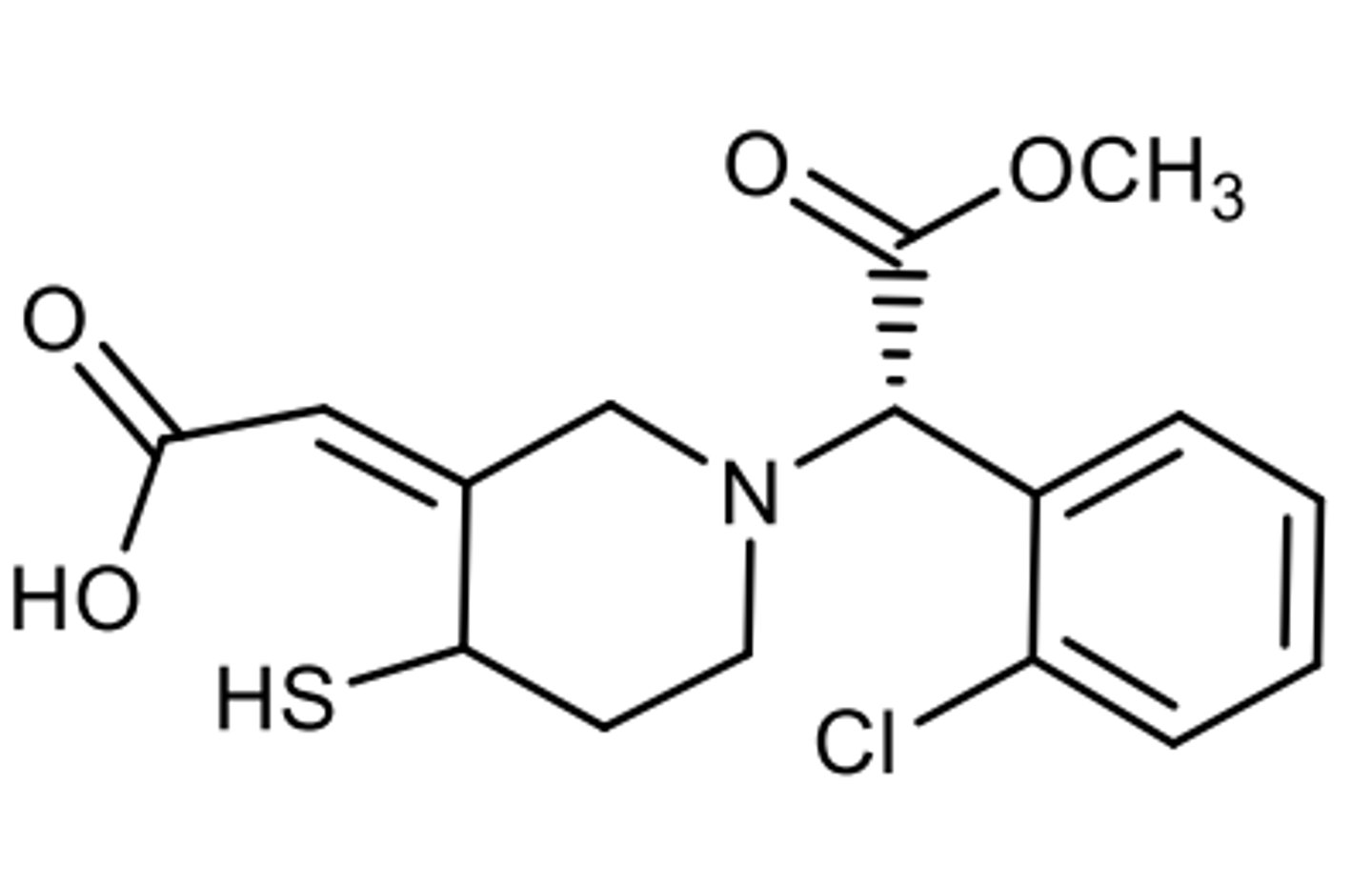
Active metabolite of clopidogrel that forms a disulfide bond with P2Y12
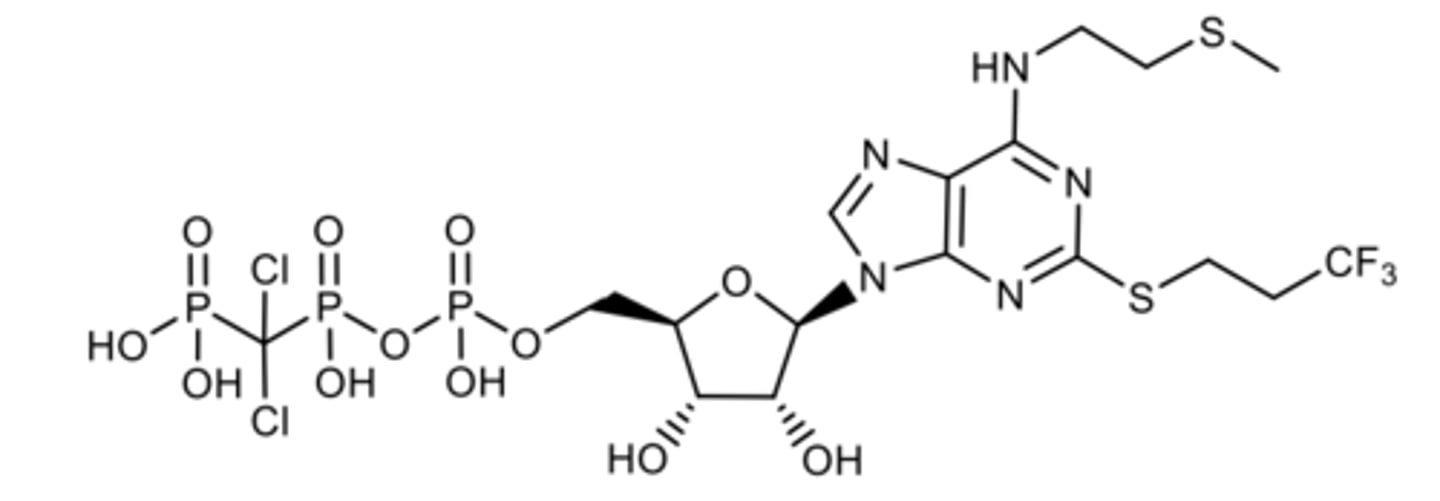
Cangrelor
Nucleotide P2Y12 antagonist (reversible)
SOFT DRUG
--metabolized by ectonucleases
--phosphates into OH
--T1/2= 3-6min
Highly selective for P2Y12
Rapid onset/short DOA= good for acute settings
IV adjucnt to PCI
Chloro groups give it resistance to metabolism
Ticagrelor
Nucleoside P2Y12 antagonist (reversible)
Oral drug
Metabolized by CYP3A4
OH does not get glucuronidated
Selatogrel
Subcutaneous P2Y12 antagonist under investigation (in phase 3 rn)
For use pre-hospital Tx of Mi: for people to self admin if they've had a previous MI
Has portion (aminopyridine) of ticgrelor
Phosphonic acid has more potency and less metabolism, allowing its quick onset (T1/2= 4-7h)
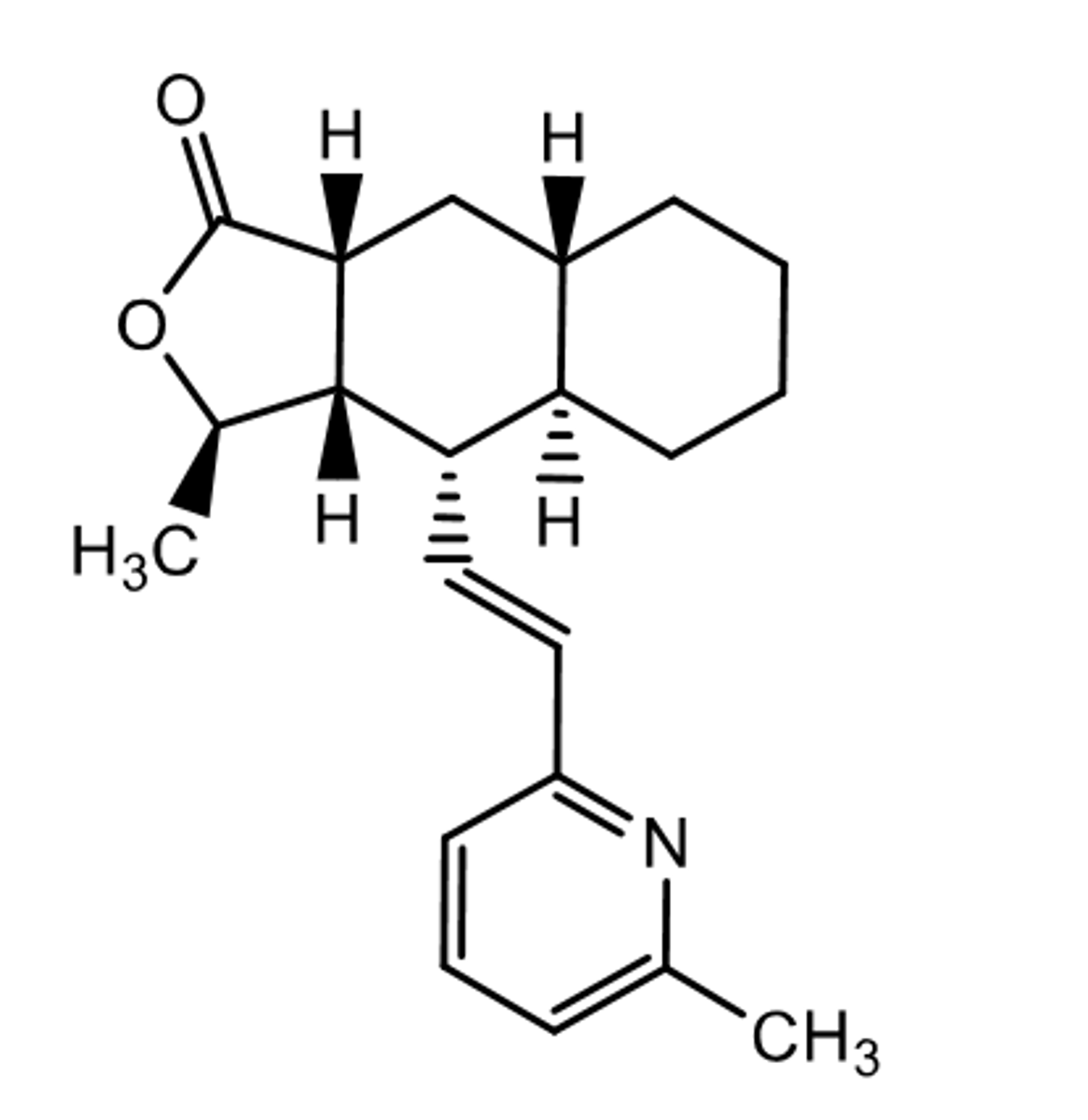
Himbacine
NO PAR-1 Activity
Used as template for antithrombin
The active enantiomer of a lead compound found in high throughput screen for the design of vorapaxar
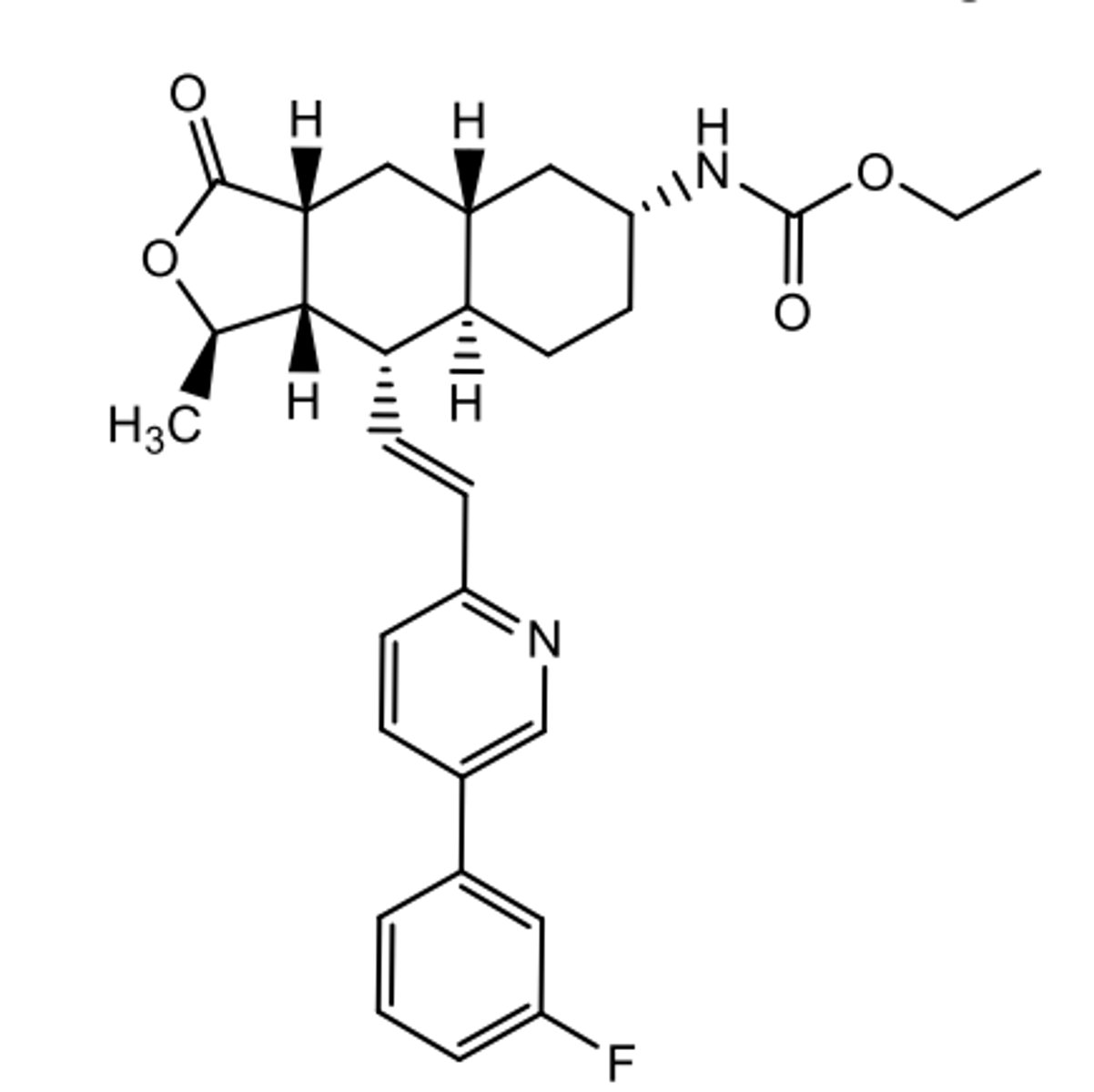
Vorapaxar
competitive + selective PAR-1 antagonist
reversible
dissociation 1/2 off the receptor is 12h (good for tethered ligand)
decreases CV events in people with MI and PAD
Metabolized by CYP3A4 + 2j2
M20
Active metabolite of Vorapaxar metabolized by CYP3A4 + 2j2 (omega hydroxylation)
23% of the circulating drug
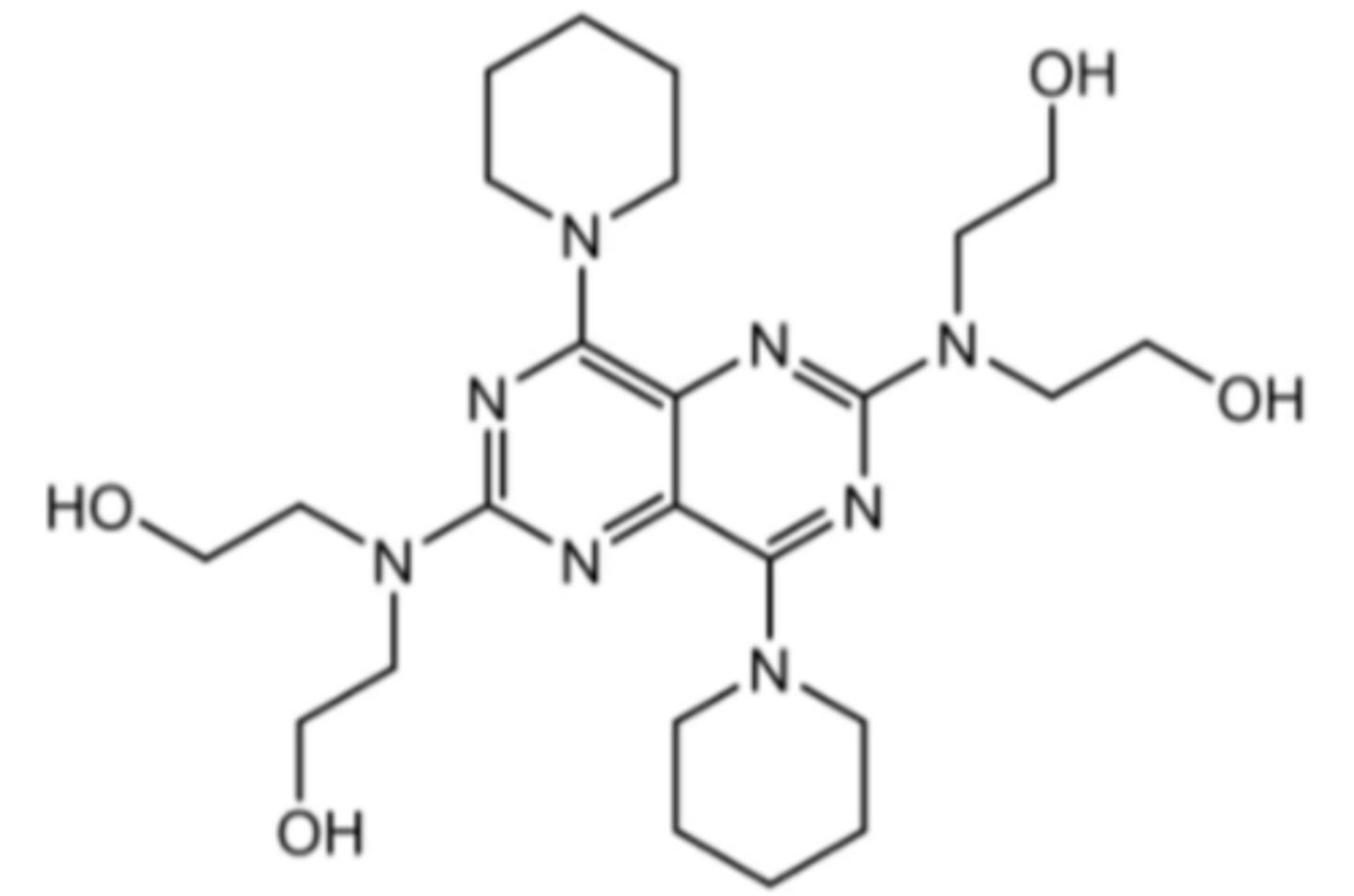
Dipyridamole
Phosphodiester ease inhibitor (increases cAMP= vasodilation)
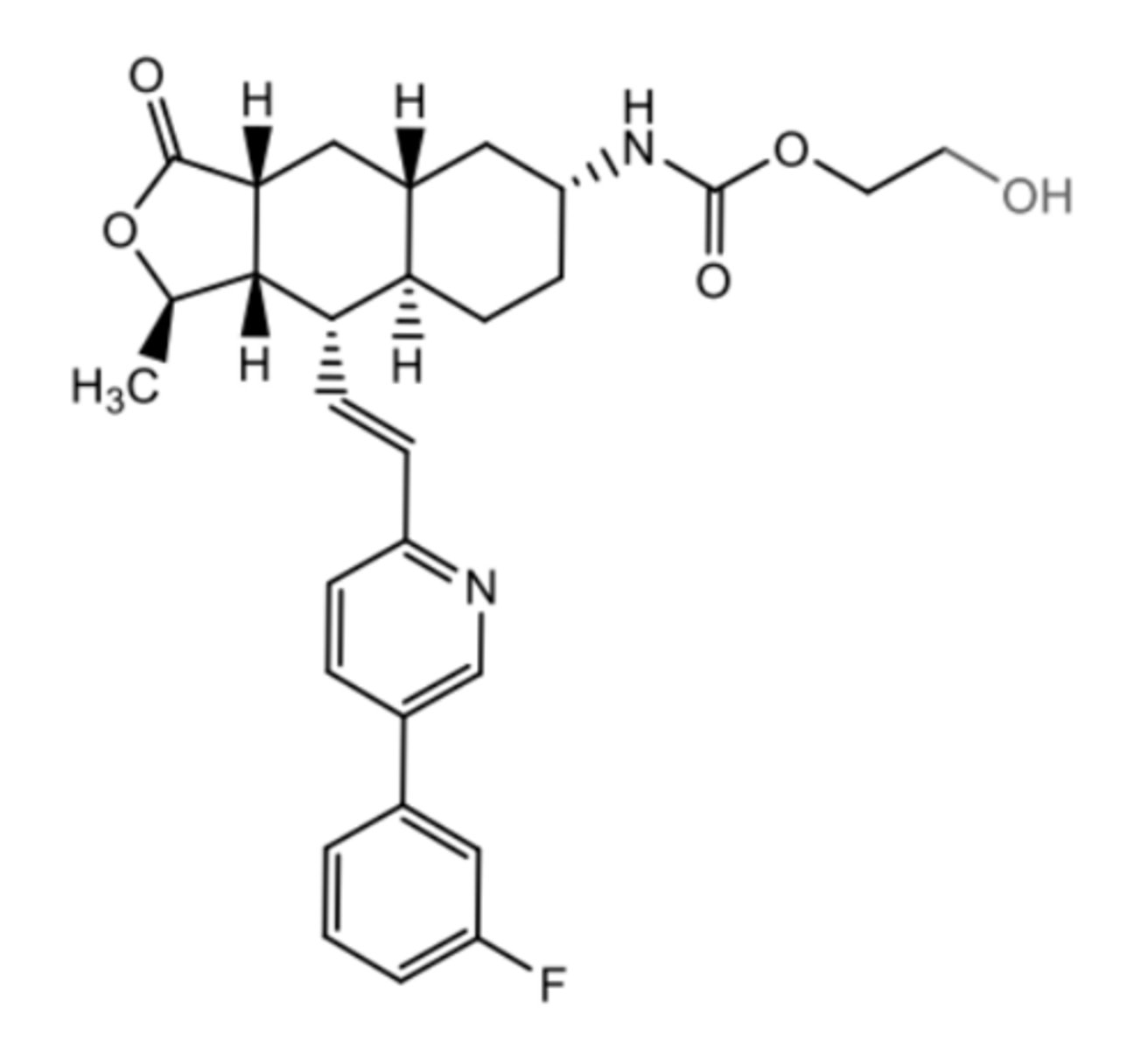
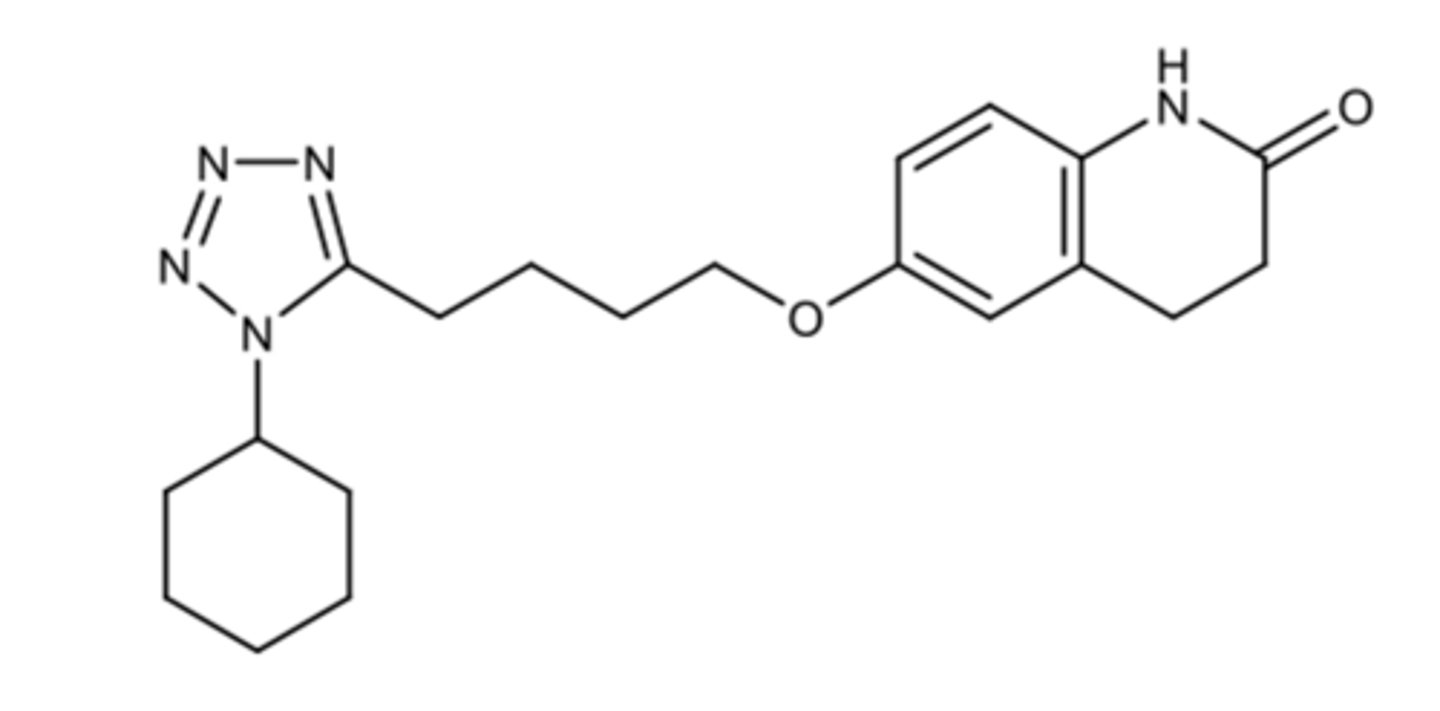
Cilostazol
Used in the Tx of intermittent claudication of PAD (painful walking due to ischemia)
oral PDE3 inhibitor (increases cAMP= vasodilation)
CONTRAINDICATED in HF due to increased mortality
Active metabolite accounts for 15% of activity= reduce dose 50% when co-administered with CYP3A4 and CYP2C19 inhibitors
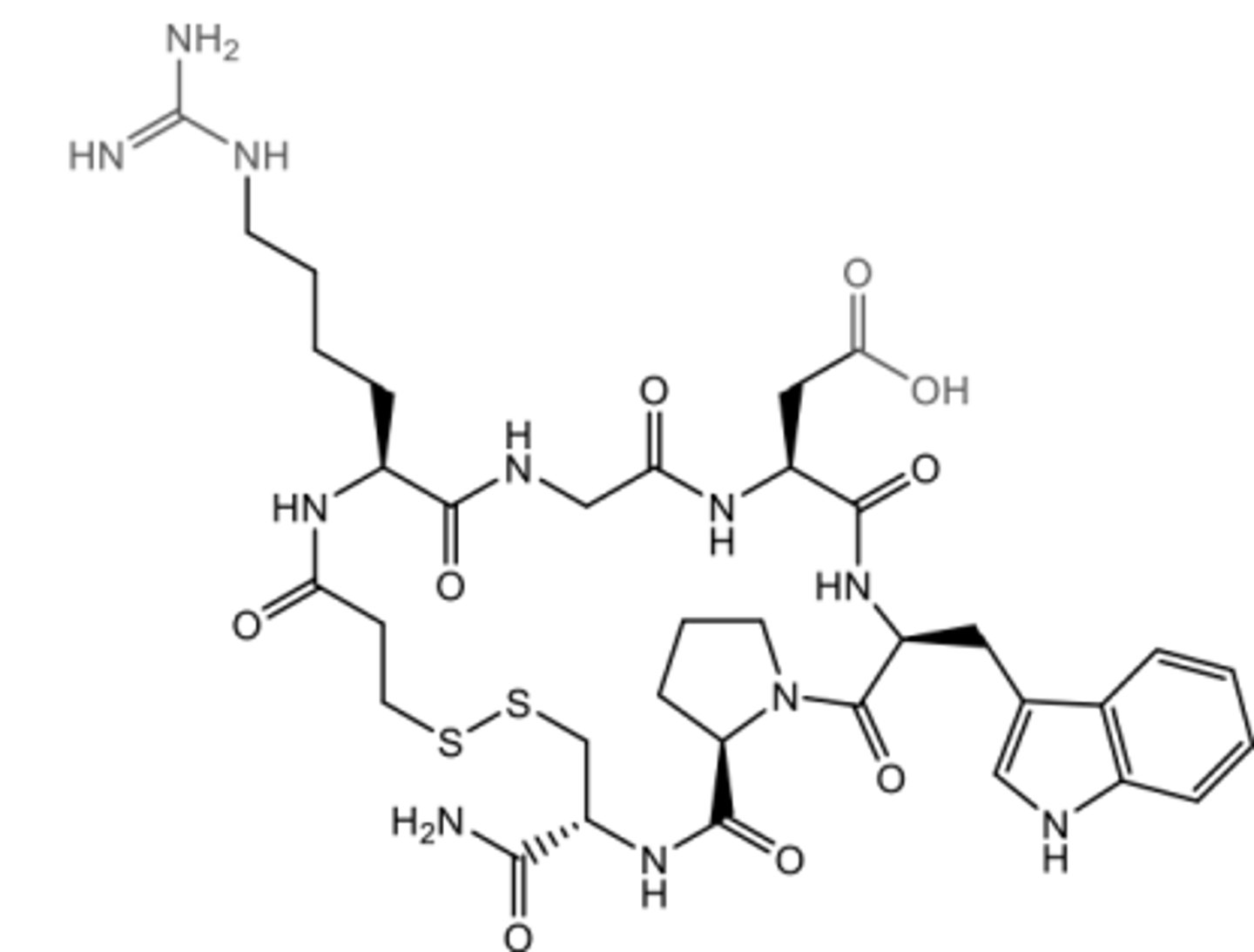
Eptifibatide
Intravenous GPIIb/IIIa Receptor Antagonist
Reversible
Mimics RGD sequence of fibrinogen
Amine and Carboxylic acid have appropriate distance from each other to resemble RGD best
Cyclic Peptide
Mimics RGD sequence of fibrinogen
Ionized homoarginine mimics arginine of RGD and increases potency (positions charges correctly)
Indole ring + Cys also increases potency
Proline restricts the flexibility for spacing
Binding:
Binds to Mg on the beta 3 subunit MIDAS (metal-ion adhesion site)
Causes thrombocytopenia!!
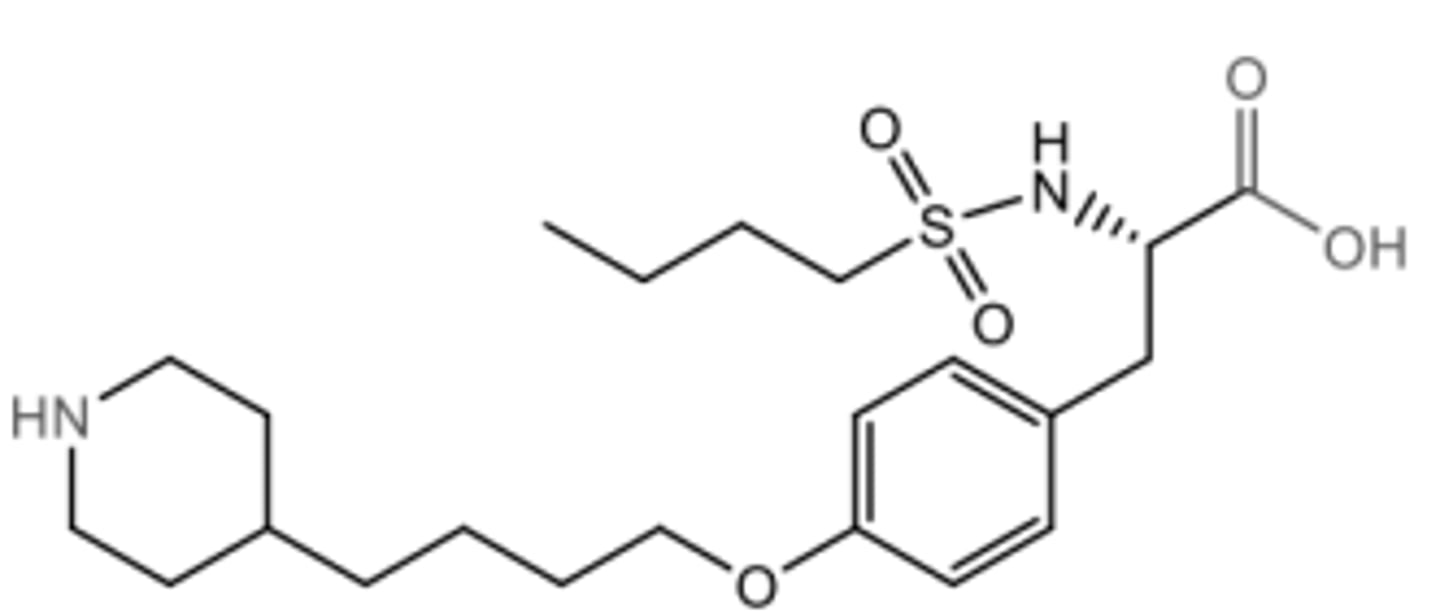
Tirofiban
Intravenous GPIIb/IIIa Receptor Antagonist
Mimics RGD sequence of fibrinogen
Reversible
Amine and Carboxylic acid have appropriate distance from each other to resemble RGD best
More potent that eptifibatide due to sulfonamide
Binding:
Binds to Mg on the beta 3 subunit MIDAS (metal-ion adhesion site)
Causes thrombocytopenia!!
Zalunfiban (RUC-4)
a non-RGD-mimetic GPIIb/IIIa antagonist
For SC injection for prehospital admin in patients with an ST level elevation in MI
In an autoinjector for EMS to use
Rapid onset of 15mn and DOA 2h
In phase 3 trials
Metabolism: glycine cleaved and excreted in urine
Binding:
No arginine mimetic because no Arginine; Instead has primary amine
Primary amine binds to the glutamate residue instead of Mg= no conformational change
Displaces Mg in the MIDAS binding site
No thrombocytopenia!!
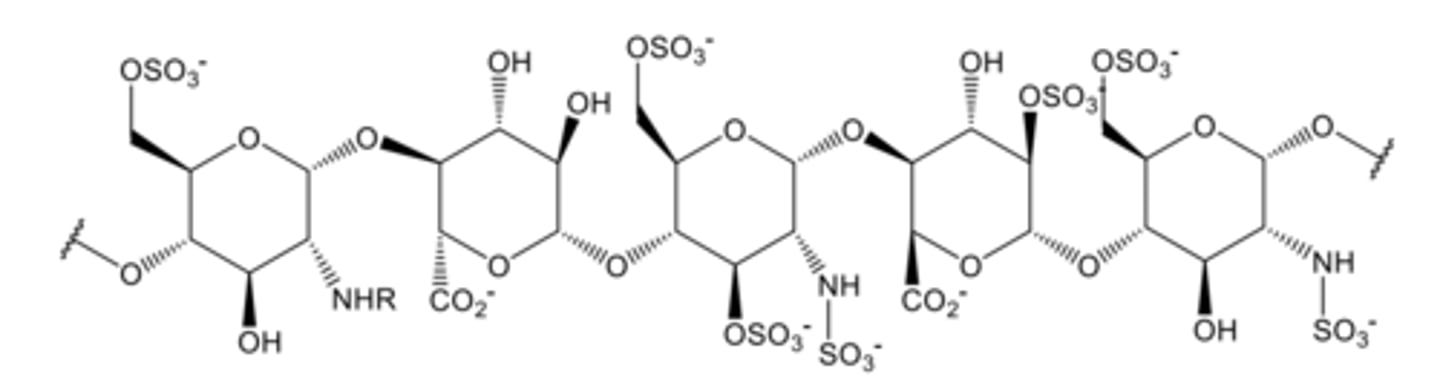
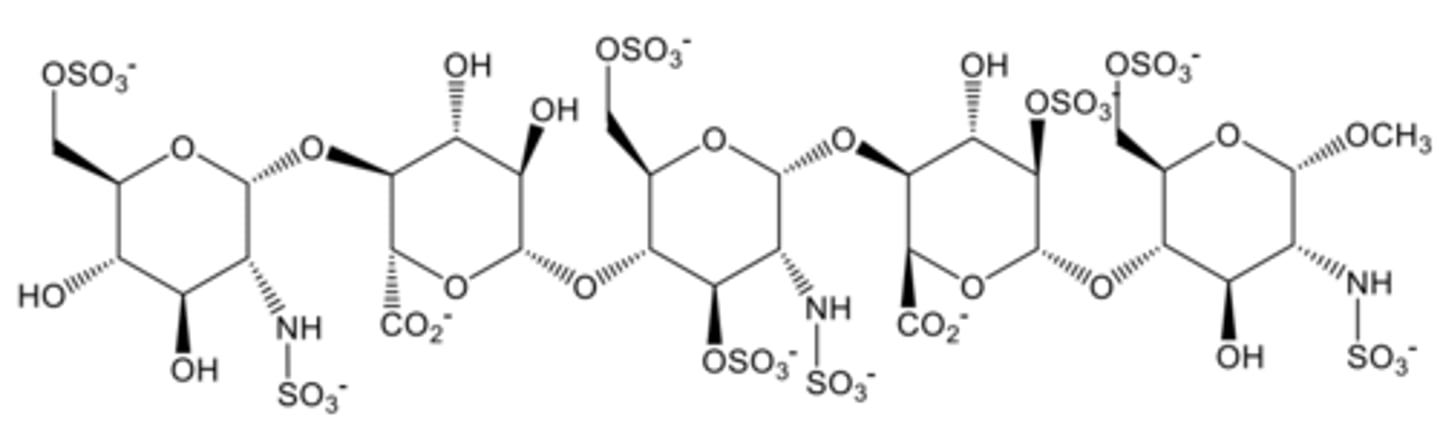
Heparin (Unfractionated Heparin, UFH) MOA
Composed of a mixture of fragments from 3,000 to 30,000 daltons
Partial structure pictured because fragment sizes vary:
--To have IIa activity it requires at least 18 saccharide units (larger)
--Xa just requires the typical Penta saccharide unit
Ratio of anti-factor 10a:2a is 1:1
The negative charges on heparin form ionic links to ATIII (antithrombin III) at positively charged lysine residues
T1/2= 1-6h depending on patient
Binds platelet factor 4; it undergoes and conformational change and exposes epitopes that IgG antibodies can bind to= associated with HIT
Not orally active because it’s too big\polar and glycosidic linkages would be hydrolyzed in the stomach
It’s IV and SQ- too painful and too high risk for I
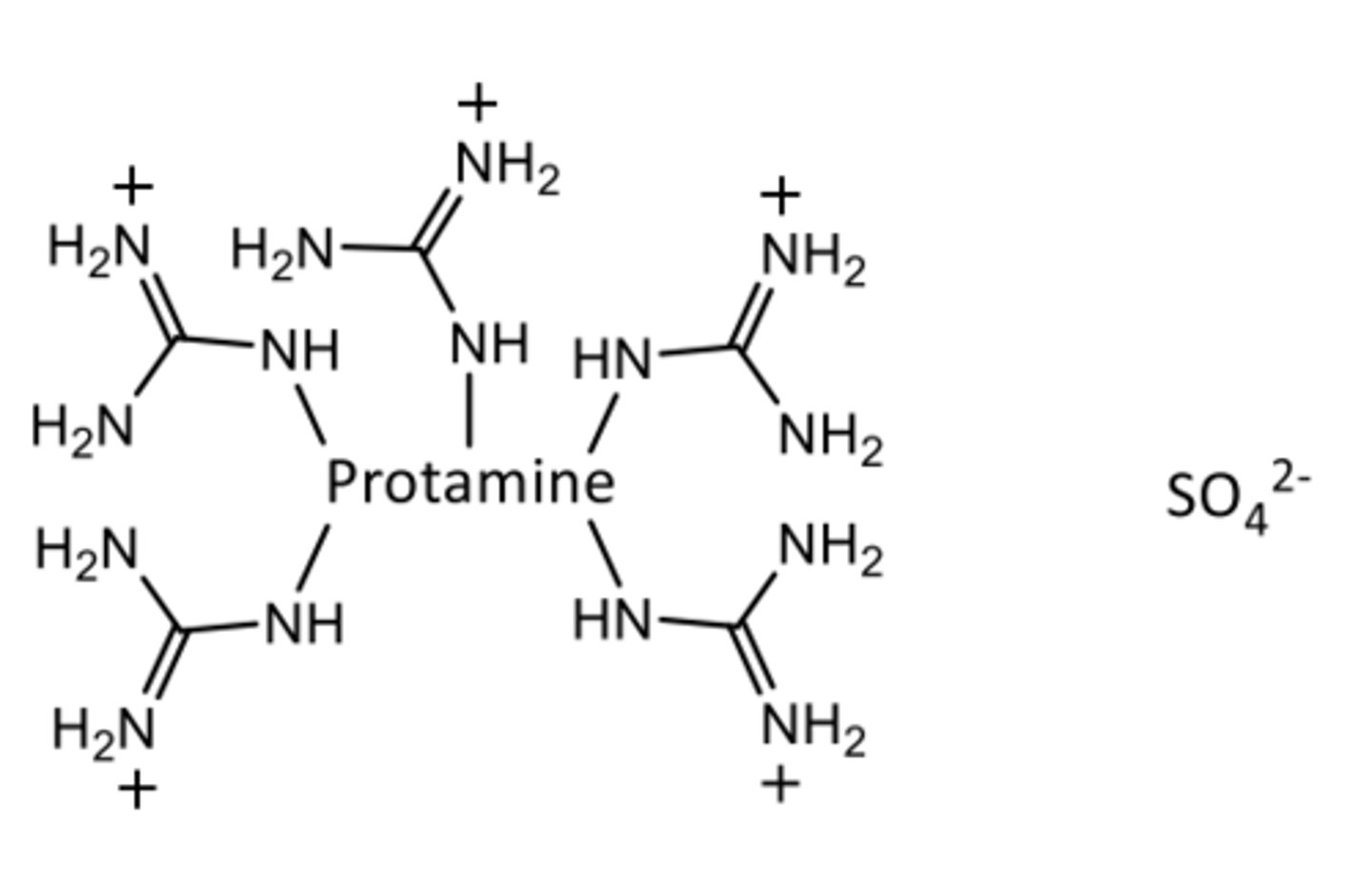
Protamine sulfate
Heparin antidote
Mostly Arg residues that ionically bind to UFH's polyanionic structure
Administered IV and will neutralize heparin in ~5min
May work on 60% of LMWH= need two doses for Delteparin/Enoxaparin
Fondaparinux
Indirect factor Xa inhibitor
Contains only the Essential Penta saccharide sequence that binds to antithrombin 3
Has indirect Xa activity= indirect because it binds antithrombin 3 (Avoids non specific binding)
More potent (94% binds antithrombin 3)
Not protein bound
T1/2= 17h once a day dosing
No HIT + No monitoring
Too small for protamine to work as an antidote
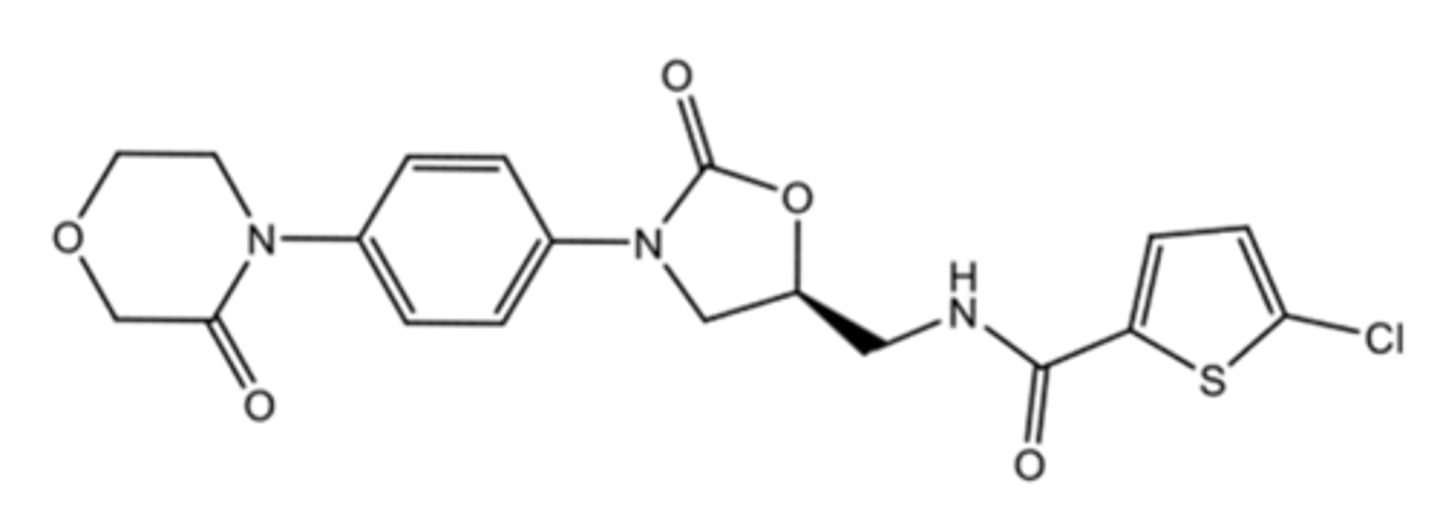
Rivaroxaban
DOAC
Binds directly to Xa
Used in preventing a thrombus from forming or growing (so many PE and CV indications/to decrease stroke risk)
Small molecule oral drug with predictable pharmacokinetics
No monitoring required
Binds the S4 ad S1 pockets in the active site of factor Xa (V-shape)
--Rivaroxabans Cl group has an electrostatic interaction with edges of Tyr residue
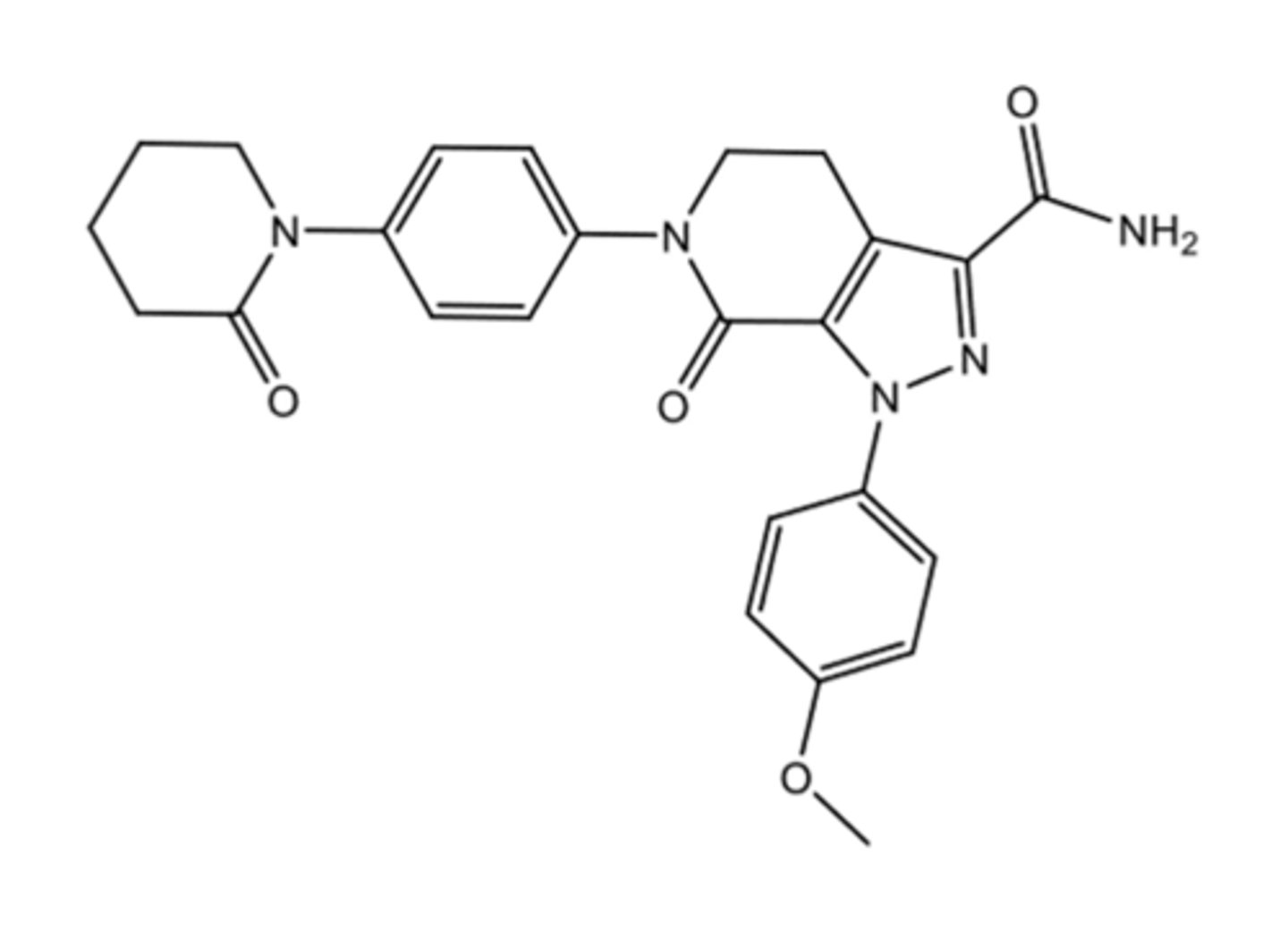
Apixaban
DOAC
Binds directly to Xa
Used in preventing a thrombus from forming or growing (so many PE and CV indications/to decrease stroke risk)
Small molecule oral drug with predictable pharmacokinetics
No monitoring required
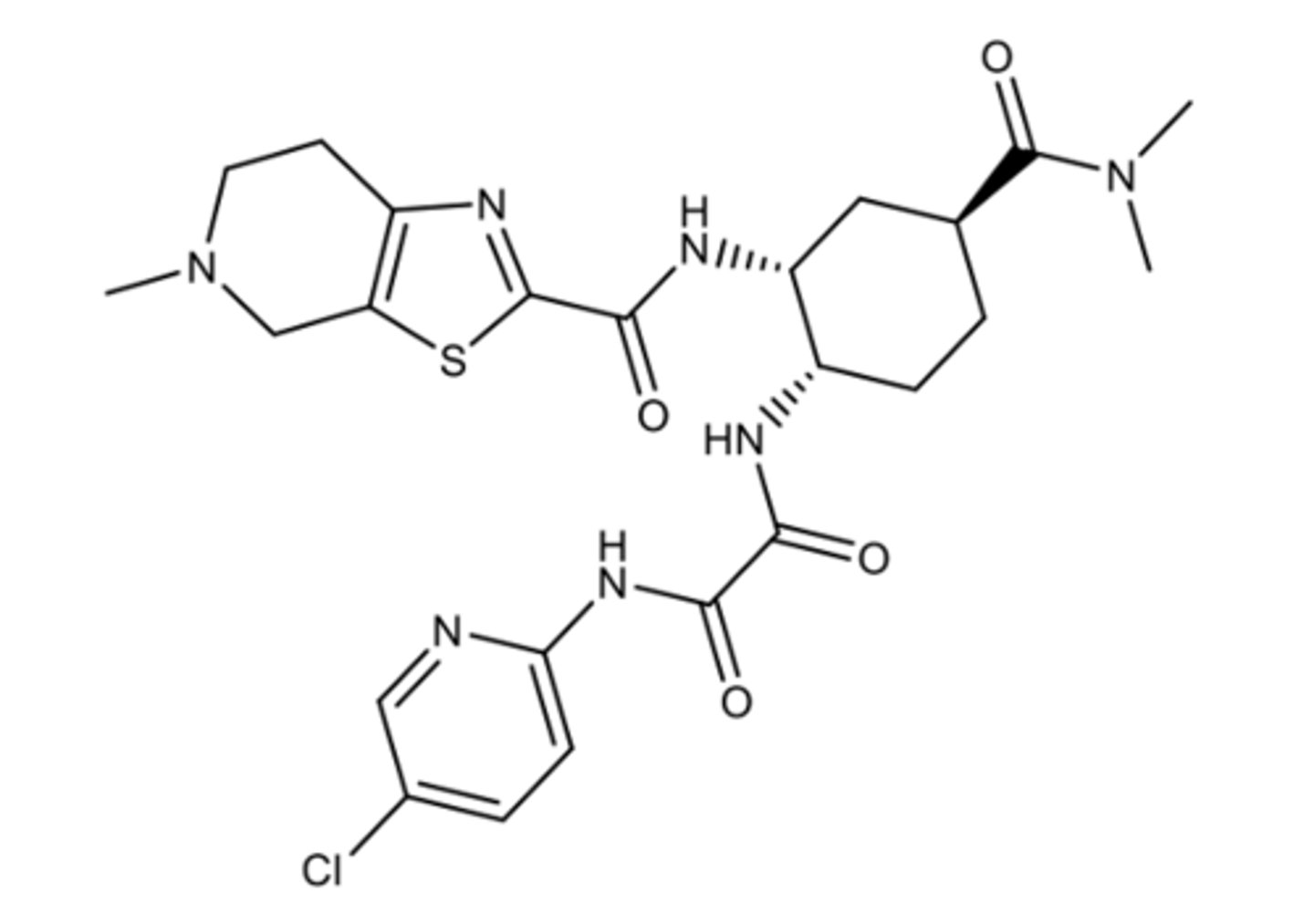
Edoxaban
DOAC
Binds directly to Xa
Used in preventing a thrombus from forming or growing (so many PE and CV indications/to decrease stroke risk)
Small molecule oral drug with predictable pharmacokinetics
Edoxaban also binds an "cation hall" due to the methyl on the nitrogen, causing it to have a positive charge
No monitoring required
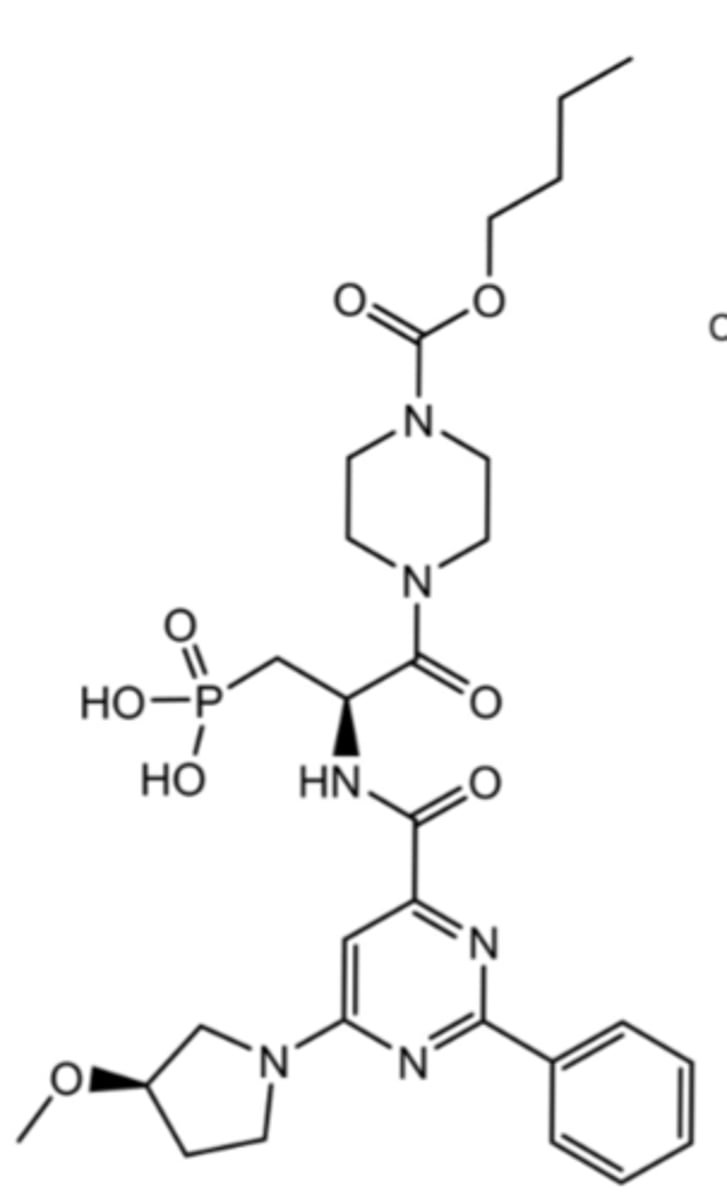
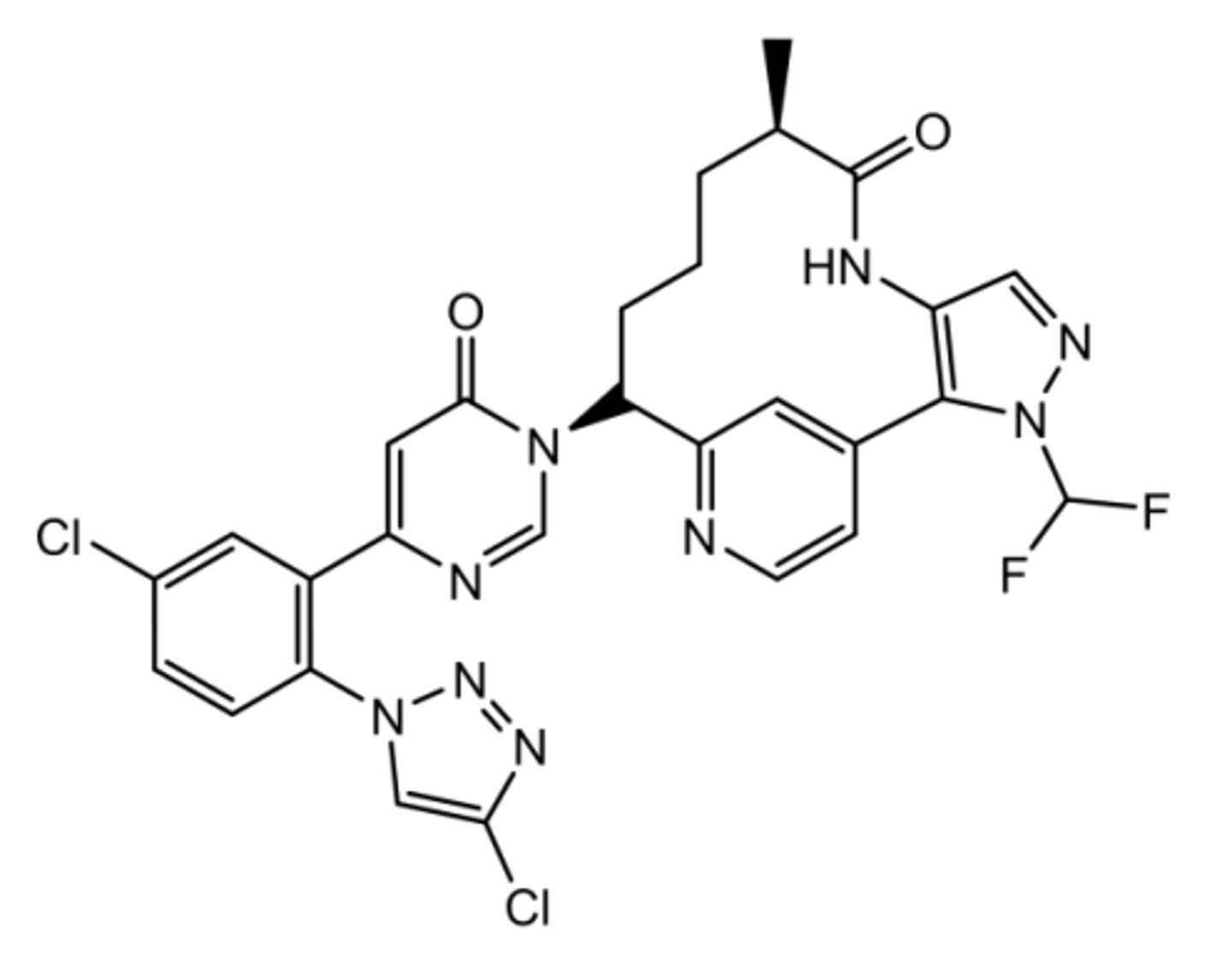
Milvexian
Oral Factor XIa inhibitor in phase 3 right now
Binds S1 (due to phenyl- triazole) and S2' of factor 11a
Patients who are deficient in factor Xia have a lower risk for VTE AND Ischemic stroke + rarely have spontaneous bleeding
Factor 11a is an important driver for thrombus growth but not really important for homeostasis= ideal for pathological thrombosis
Overall benefit is less bleeding risk
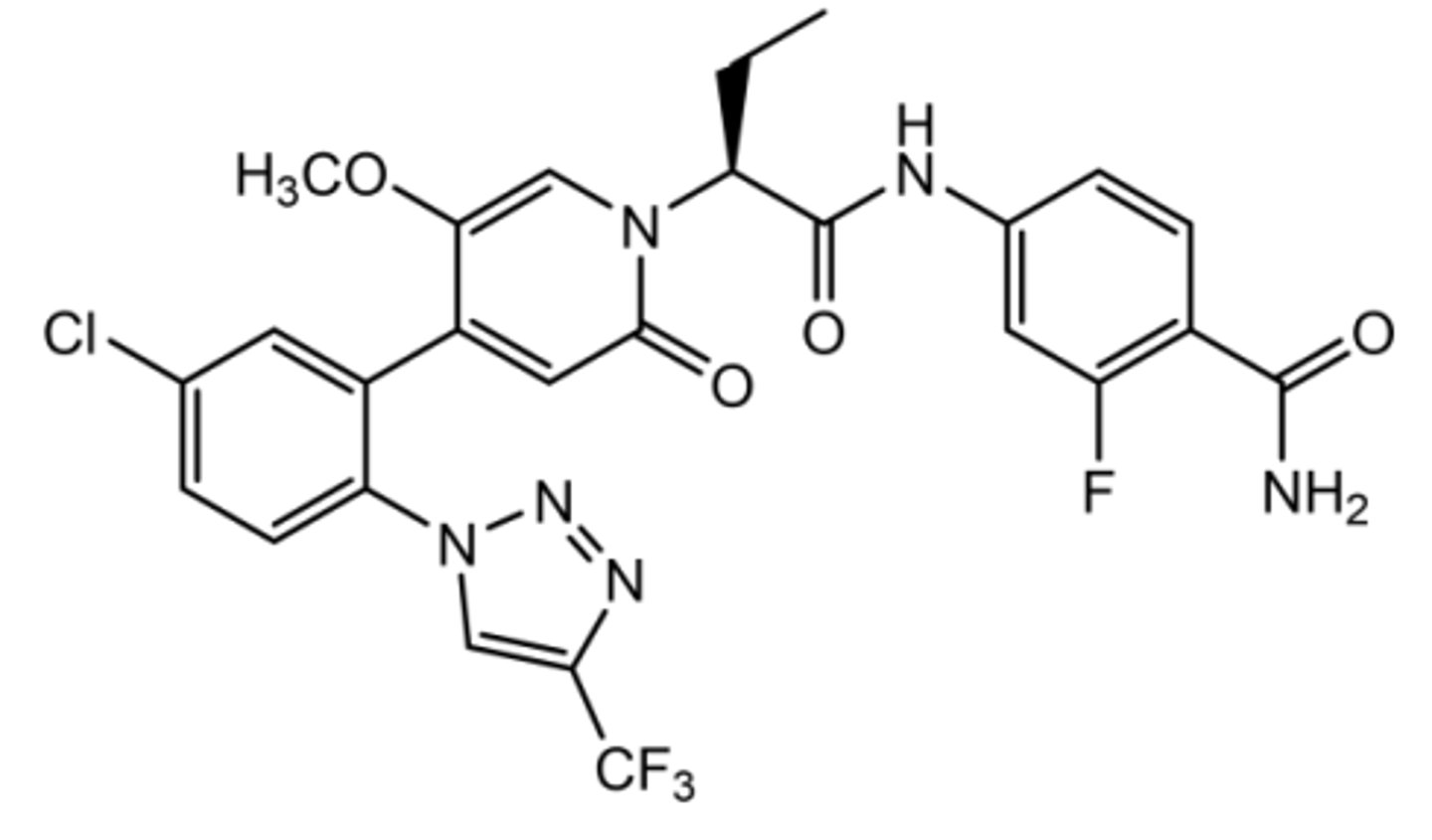
Asundexian
Oral Factor XIa inhibitor in phase 3 right now
Binds S1 (due to phenyl- triazole) and S2' of factor 11a
Patients who are deficient in factor Xia have a lower risk for VTE AND Ischemic stroke + rarely have spontaneous bleeding
Factor 11a is an important driver for thrombus growth but not really important for homeostasis= ideal for pathological thrombosis
Overall benefit is less bleeding risk
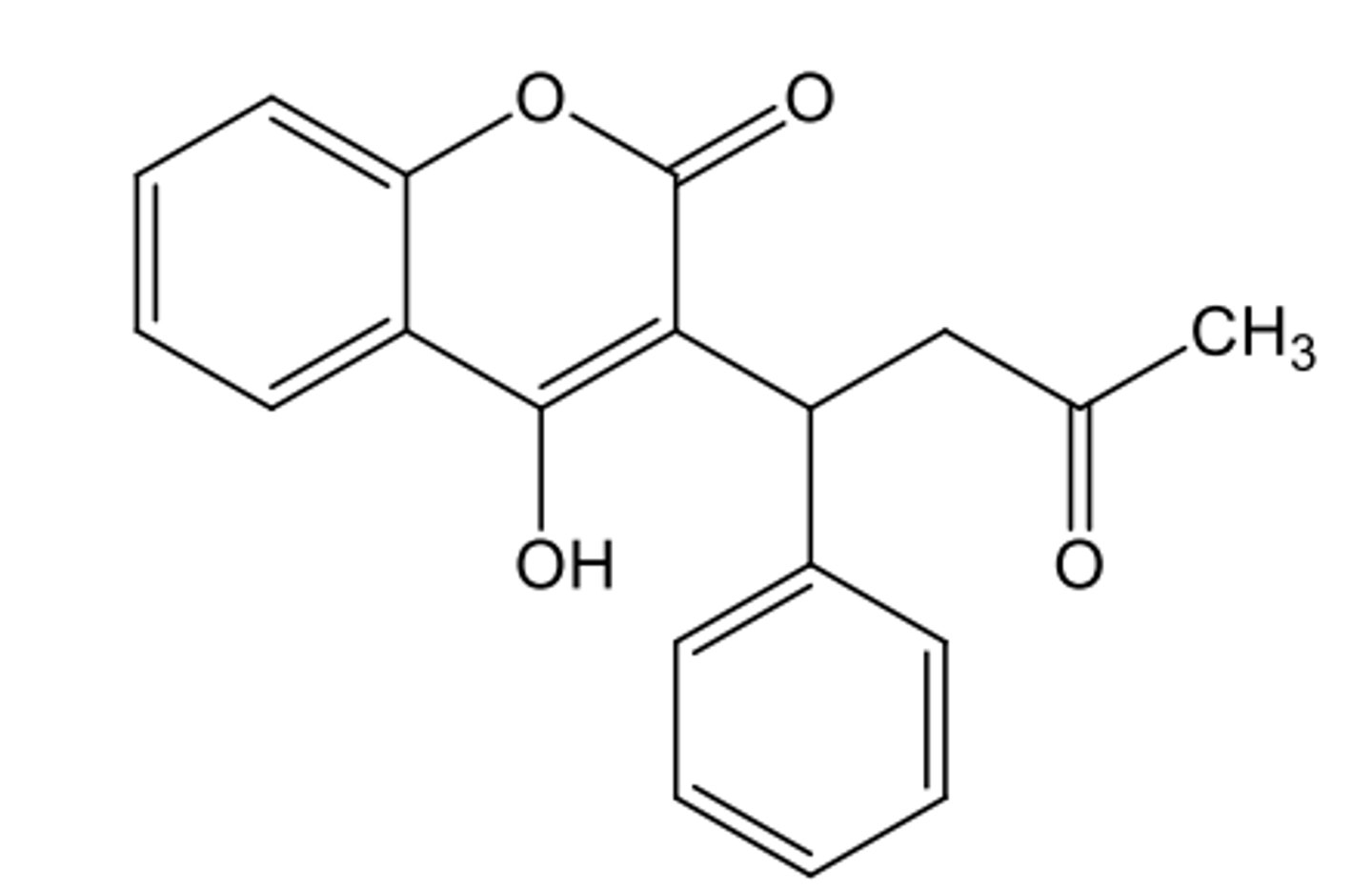
Warfarin
Vitamin K antagonist--> inhibits factors II, VII, IX, and X (also proteins C and S)
Coumarin derivative
Antagonizes by inhibiting VKOR
1,3-dicrbonyls make it acidic= comes as sodium salt
Sold as racemic mixture but S isomer accounts for all important activity (R=weakly active)
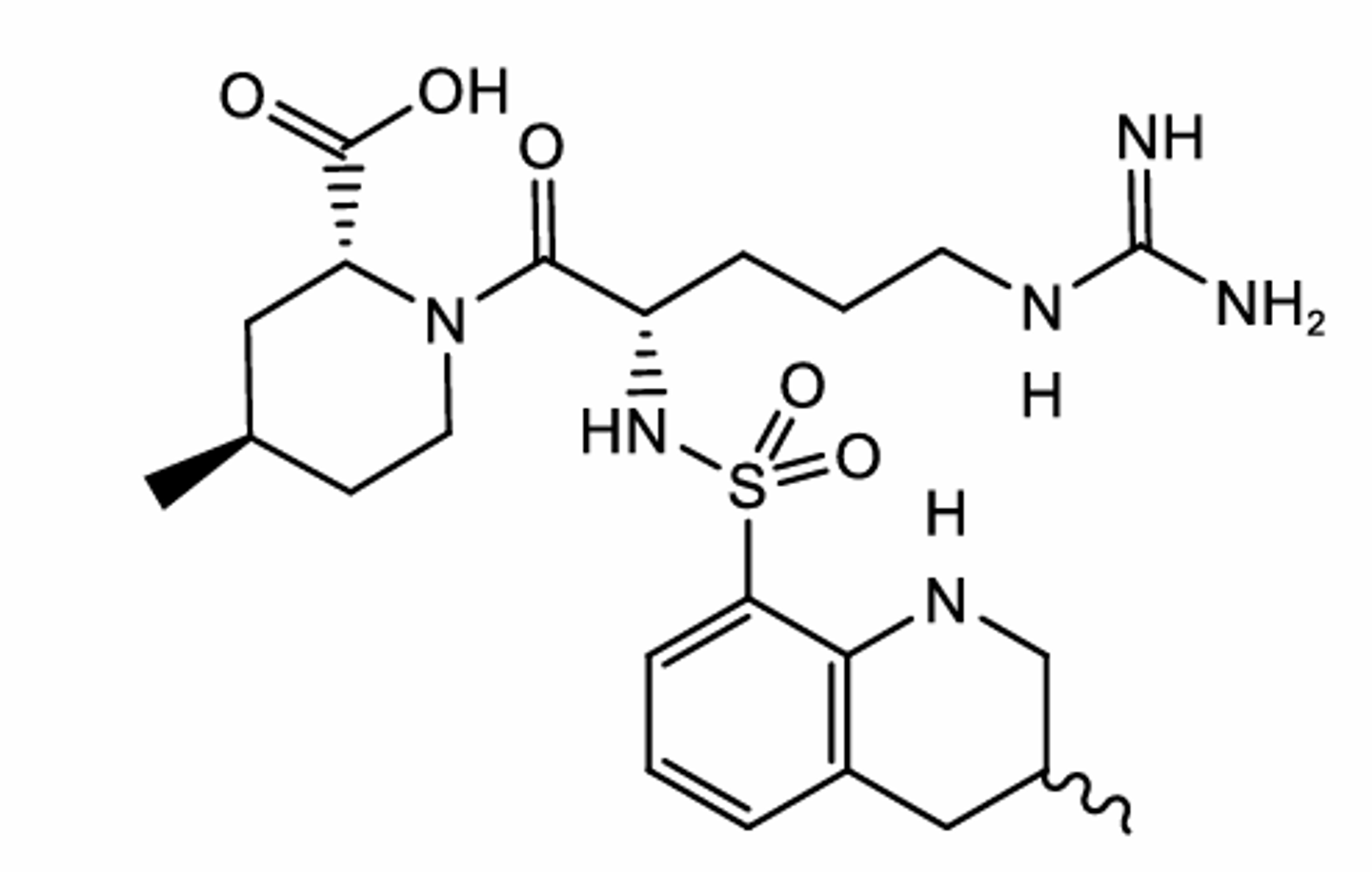
Argatroban
Univalent DTI
Reversible
Peptidomimetic small molecule
Still administered IV because low lipophilicity
USED TO TREAT HIT
May increase INR so caution when bridging with warfarin
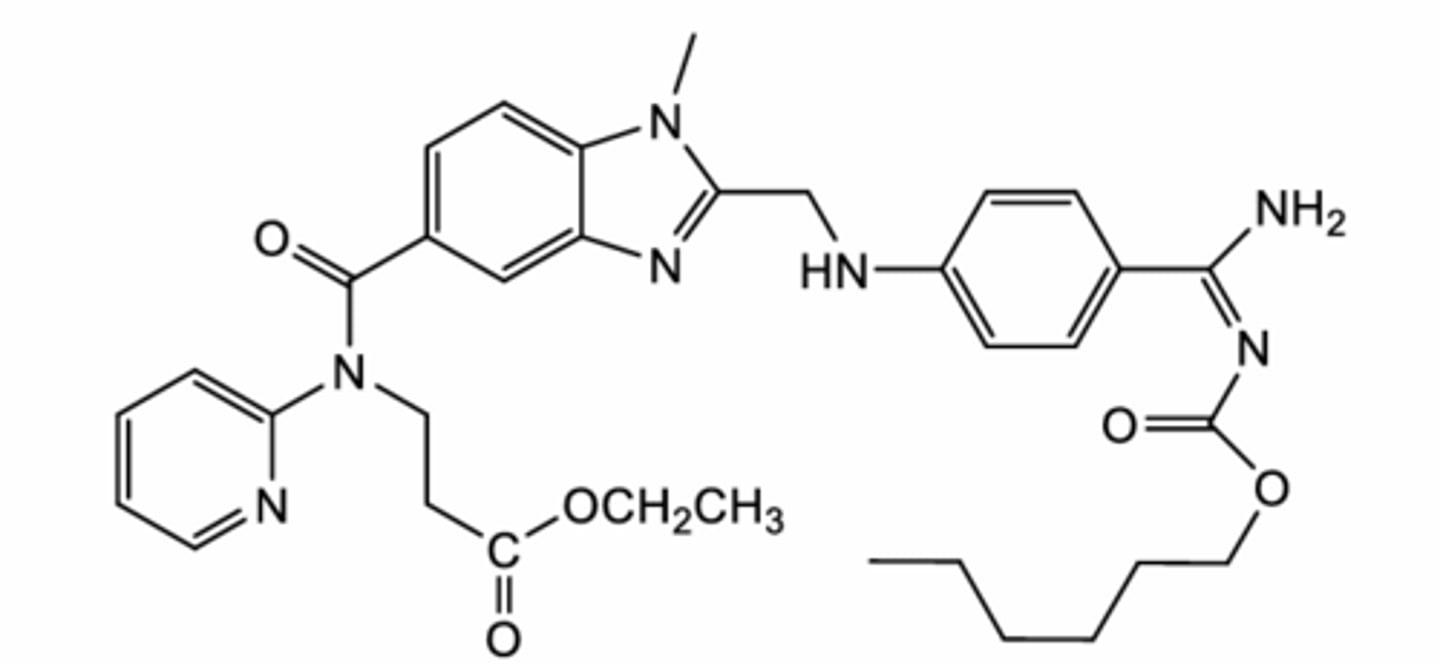
Dabigatran
Type of DOAC + DTI (double)
PRODRUG
Binds S1, S2, and S4 sites of thrombin
Once ester and carbamide are cleaved= active
Glucuronide metabolite is still pharmacologically active (not a part of binding site; CA makes it more lipophilic)
Activation is esterase-mediated (hCE1/hCE2), NOT CYP450= less drug interactions compared to CYP-metabolized drugs