histology + pathology week 18
0.0(0)
Studied by 1 personCard Sorting
1/99
Earn XP
Description and Tags
Last updated 4:05 PM on 7/8/26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
1
New cards
the male reproductive system consists of…
testes, genital ducts, accessory glands and penis
2
New cards
dihydrotestosterone
metabolite of testosterone
acts on many tissues during puberty
acts on many tissues during puberty
3
New cards
testes
* produce sperm, contain endocrine cells that produce hormones
* testes develop %%__retroperitoneally__%% in the dorsal wall of the embryonic abdominal cavity → move during foetal development → suspended in the 2 halves of the scrotal sac/scrotum at the ends of the %%__*spermatic cords*__%%
* during migration, each testis carries the ==__tunica vaginalis__== (a serous sac) with it → derived from the peritoneum → consists of an outer parietal layer lining the scrotum and an inner visceral layer covering the ==__tunica albuginea__== on the anterior and lateral sides of the testes
* each testis/testicle is surrounded by the tunica albuginea (dense connective tissue) → thickens on the posterior side → mediastinum testis
septa penetrate the organ and divide it into testicular lobules
* each lobule contains:
1. connective tissue with endocrine interstitial cells (leydig cells) → secrete testosterone
2. 1-4 highly convoluted seminiferous tubules where sperm is produced
* a temp. of 34 degrees is maintained in the scrotal sac (certain molecular events cannot occur at 37 degrees)
each testicular artery is surrounded by a pampiniform venous plexus containing cooler blood from the testis, which draws heat from the arterial blood by a countercurrent heat exchange system
* dartos muscle of the scrotum and the cremaster muscles of the spermatic rodes move the tests away from or closer to the body respectively → allows further temp. control
==__INSERT PHOTOS__==
* testes develop %%__retroperitoneally__%% in the dorsal wall of the embryonic abdominal cavity → move during foetal development → suspended in the 2 halves of the scrotal sac/scrotum at the ends of the %%__*spermatic cords*__%%
* during migration, each testis carries the ==__tunica vaginalis__== (a serous sac) with it → derived from the peritoneum → consists of an outer parietal layer lining the scrotum and an inner visceral layer covering the ==__tunica albuginea__== on the anterior and lateral sides of the testes
* each testis/testicle is surrounded by the tunica albuginea (dense connective tissue) → thickens on the posterior side → mediastinum testis
septa penetrate the organ and divide it into testicular lobules
* each lobule contains:
1. connective tissue with endocrine interstitial cells (leydig cells) → secrete testosterone
2. 1-4 highly convoluted seminiferous tubules where sperm is produced
* a temp. of 34 degrees is maintained in the scrotal sac (certain molecular events cannot occur at 37 degrees)
each testicular artery is surrounded by a pampiniform venous plexus containing cooler blood from the testis, which draws heat from the arterial blood by a countercurrent heat exchange system
* dartos muscle of the scrotum and the cremaster muscles of the spermatic rodes move the tests away from or closer to the body respectively → allows further temp. control
==__INSERT PHOTOS__==
4
New cards
leydig cells
* interstitial cells between the seminiferous tubules
* develop as large round or polygonal cells with central nuclei and eosinophilic cytoplasm with small lipid droplets during puberty
* produce testosterone (synthesised in the SER and mitochondria)
* after the 3rd and 4th months of pregnancy/foetal life, they regress and become quiescent cells resembling fibroblasts until puberty when they resume testosterone synthesis in response to the pituitary gonadotropin (which is released in puberty, during the 3rd and 4th months, its released from the placenta)
* develop as large round or polygonal cells with central nuclei and eosinophilic cytoplasm with small lipid droplets during puberty
* produce testosterone (synthesised in the SER and mitochondria)
* after the 3rd and 4th months of pregnancy/foetal life, they regress and become quiescent cells resembling fibroblasts until puberty when they resume testosterone synthesis in response to the pituitary gonadotropin (which is released in puberty, during the 3rd and 4th months, its released from the placenta)
5
New cards
testosterone
* drives male reproductive physiology
* spermatogenesis
* sexual differentiation during embryonic and foetal development
* control of gonadotropin secretion in the pituitary
* testosterone secretion by interstitial cells is triggered by luteinising hormone (or interstitial cell stimulating hormone = a gonadotropin) → synthesis of testosterone begins at puberty
* in late embryonic testes, gonadotropin from the placenta stimulates interstitial cells to synthesise the testosterone needed for development of ducts and glands
* foetal interstitial cells are very active during the 3rd and 4th months of pregnancy
* spermatogenesis
* sexual differentiation during embryonic and foetal development
* control of gonadotropin secretion in the pituitary
* testosterone secretion by interstitial cells is triggered by luteinising hormone (or interstitial cell stimulating hormone = a gonadotropin) → synthesis of testosterone begins at puberty
* in late embryonic testes, gonadotropin from the placenta stimulates interstitial cells to synthesise the testosterone needed for development of ducts and glands
* foetal interstitial cells are very active during the 3rd and 4th months of pregnancy
6
New cards
seminiferous tubules
* where sperm is produced
* each tubule is lined with spermatogenic epithelium (specialised stratified epithelium) → consists of 2 types of cells:
1. sertoli cells → large, non dividing, physically and metabolically support developing sperm cell precursors
2. dividing cells of the spermatogenic lineage (spermatogonia)
* forms 4 or more concentric layers in the germinal epithelium
* develop from progenitor cells to fully formed sperm cells over a period of around 10 weeks
* next to the BM (and sertoli)
* BM is covered by fibrous tissue, the innermost layer contains flattened smooth muscle like myoid cells (allows weak contractions of the tubule)
* each tubule is a loop linked by the straight tubule (a very short narrower segment) to the rete testis = epithelium lined channels embedded in the mediastinum testis
* 10-20 efferent ductules connect the rete testis to the head of the epididymis
* each tubule is lined with spermatogenic epithelium (specialised stratified epithelium) → consists of 2 types of cells:
1. sertoli cells → large, non dividing, physically and metabolically support developing sperm cell precursors
2. dividing cells of the spermatogenic lineage (spermatogonia)
* forms 4 or more concentric layers in the germinal epithelium
* develop from progenitor cells to fully formed sperm cells over a period of around 10 weeks
* next to the BM (and sertoli)
* BM is covered by fibrous tissue, the innermost layer contains flattened smooth muscle like myoid cells (allows weak contractions of the tubule)
* each tubule is a loop linked by the straight tubule (a very short narrower segment) to the rete testis = epithelium lined channels embedded in the mediastinum testis
* 10-20 efferent ductules connect the rete testis to the head of the epididymis
7
New cards
spermatogenesis is followed by…
spermiogenesis
8
New cards
spermatogenesis
* begins at puberty with the proliferation of spermatogonia
* there are different stages of development (in order)
1. type A spermatogonia STEM cells (?) → dark ovoid nuclei, act as stem cells, divide infrequently, give rise to new stem cells and type A spermatogonia cells
2. type A spermatogonia PROGENITOR cells→ pale staining ovoid nuclei that divide more rapidly as transit amplifying (progenitor) cells → undergo clonal divisions that leave most of the cells interconnected as a syncytium → type B spermatogonia
3. type B spermatogonia → spherical and pale nuclei, undergo a final mitotic division to produce 2 cells that grow in size and become primary spermatocytes
\
__*up until here its mitosis (1,2,3)*__
\
4. primary spermatocytes (44 + XY) → spherical cells with euchromatic nuclei → disassemble the tight junctions of the blood testis barrier → moves from the tubules basal component to the adluminal compartment
at the same time they replicate their DNA → meiosis I → haploid cells (23 chromosomes) = secondary spermatocytes
5. secondary spermatocytes → meiosis II (separation the chromatids, there are 2 of them) → spermatids (this occurs near the lumen but still embedded in sertoli cells)
6. spermatids differentiate to form sperm (spermiogenesis)
\
==__INSERT PHOTOS__==
* there are different stages of development (in order)
1. type A spermatogonia STEM cells (?) → dark ovoid nuclei, act as stem cells, divide infrequently, give rise to new stem cells and type A spermatogonia cells
2. type A spermatogonia PROGENITOR cells→ pale staining ovoid nuclei that divide more rapidly as transit amplifying (progenitor) cells → undergo clonal divisions that leave most of the cells interconnected as a syncytium → type B spermatogonia
3. type B spermatogonia → spherical and pale nuclei, undergo a final mitotic division to produce 2 cells that grow in size and become primary spermatocytes
\
__*up until here its mitosis (1,2,3)*__
\
4. primary spermatocytes (44 + XY) → spherical cells with euchromatic nuclei → disassemble the tight junctions of the blood testis barrier → moves from the tubules basal component to the adluminal compartment
at the same time they replicate their DNA → meiosis I → haploid cells (23 chromosomes) = secondary spermatocytes
5. secondary spermatocytes → meiosis II (separation the chromatids, there are 2 of them) → spermatids (this occurs near the lumen but still embedded in sertoli cells)
6. spermatids differentiate to form sperm (spermiogenesis)
\
==__INSERT PHOTOS__==
9
New cards
spermiogenesis
* the process by which spermatids differentiate into sperm(atozoa)
* major changes are:
1. condensation, elongation and flattening of the nucleus
2. formation of an acrosome resembling a large lysosome
3. growth of a flagellum from the basal body
4. reorganisation of the mitochondria in the midpiece region
5. shedding of unneeded cytoplasm
* has 4 phases:
1. golgi phase → small proacrosomal vesicles from the golgi apparatus coalesce as a single membrane limited acrosomal cap on one end of the nucleus
centrioles migrate to a position farthest from the acrosomal cap and one acts as a basal body → ==axoneme== of the flagellum
2. cap phase → acrosomal cap spreads over half of the condensing nucleus
3. acrosome phase → the head of the sperm (containing the acrosome and the condensing nucleus) remains embedded in the sertoli cell while the growing axoneme extends into the lumen of the tubule
nuclei become more elongated and condensed
histones of nucleosomes are replaced by protamines
mitochondria aggregate around the flagellum → ==middle piece==
4. maturation phase → unneeded cytoplasm is shed as a residual body
* major changes are:
1. condensation, elongation and flattening of the nucleus
2. formation of an acrosome resembling a large lysosome
3. growth of a flagellum from the basal body
4. reorganisation of the mitochondria in the midpiece region
5. shedding of unneeded cytoplasm
* has 4 phases:
1. golgi phase → small proacrosomal vesicles from the golgi apparatus coalesce as a single membrane limited acrosomal cap on one end of the nucleus
centrioles migrate to a position farthest from the acrosomal cap and one acts as a basal body → ==axoneme== of the flagellum
2. cap phase → acrosomal cap spreads over half of the condensing nucleus
3. acrosome phase → the head of the sperm (containing the acrosome and the condensing nucleus) remains embedded in the sertoli cell while the growing axoneme extends into the lumen of the tubule
nuclei become more elongated and condensed
histones of nucleosomes are replaced by protamines
mitochondria aggregate around the flagellum → ==middle piece==
4. maturation phase → unneeded cytoplasm is shed as a residual body
10
New cards
what occurs in the middle piece
ATP is generated for flagellar movements
11
New cards
acrosome
a specialised type of lysosome containing hydrolytic enzymes, mainly hyaluronidase and a trypsin like protease called acrosin
enzymes are released when the spermatozoon encounters an oocyte and the acrosomal membrane fuses with the sperms plasma membrane → dissociate cells of the corona radiata and digest the zone pellucida
enzymes are released when the spermatozoon encounters an oocyte and the acrosomal membrane fuses with the sperms plasma membrane → dissociate cells of the corona radiata and digest the zone pellucida
12
New cards
most spermatocytes seen in sections of testis are in the … phase
meiotic prophase
13
New cards
largest cells of the spermatogenic lineage are….
primary spermatocytes
characterised by partially condensed chromosomes in various stages of synapsis and recombination
characterised by partially condensed chromosomes in various stages of synapsis and recombination
14
New cards
what doesnt occur between the first and second half of meiotic division
S phase = DNA replication
15
New cards
the stem cells produced by mitotic divisions of spermatogonia…
remain as separate cells
all subsequent divisions → become transit amplifying progenitor cells → have incomplete cytokinesis after telophase and the cells remain attached to one another by intercellular bridges = ==__spermatogenic syncytium__==
\
= type A stem cells are not interconnected but type A progenitor and onwards are (until spermatids have to differentiate into spermatozoa → no longer division)
all subsequent divisions → become transit amplifying progenitor cells → have incomplete cytokinesis after telophase and the cells remain attached to one another by intercellular bridges = ==__spermatogenic syncytium__==
\
= type A stem cells are not interconnected but type A progenitor and onwards are (until spermatids have to differentiate into spermatozoa → no longer division)
16
New cards
sertoli cells
* they have 3 general functions:
1. support, protection and nutrition of developing spermatogenic cells:
* each cell supports 30-50 developing germ cells
2. exocrine and endocrine secretion:
* continuously release water into the tubules that carries new sperm out of the testis
* produce nutrients and @@androgen binding protein@@ → concentrates testosterone to a level requires for spermiogenesis, promoted by FSH
* secrete ==inhibin== → feedback to APG → suppresses FSH
* secrete ==mullerian inhibiting substance== → causes regression of the embryonic mullerian ducts
if there is no MIS → female
3. phagocytosis:
* phagocytoses the residual bodies
* divide the seminiferous tubules into 2 (basal and adluminal) compartments (both are within the sertoli cells though?)
* tall columnar epithelial cells, adhere to the basal lamina and their apical ends extend to the lumen
* abundant SER, some RER, well developed golgi, lots of mitochondria and lysosomes. ovoid or triangular nuclei, euchromatic with a prominent nucleolus
* have tight junctions between their basolateral membranes → forms the blood testis barrier
* spermatogonia lie in a basal compartment of the tubule, below the tight junctions (tight junctions are temporarily disassembled by primary spermatocytes which then move into the adluminal compartment)
1. support, protection and nutrition of developing spermatogenic cells:
* each cell supports 30-50 developing germ cells
2. exocrine and endocrine secretion:
* continuously release water into the tubules that carries new sperm out of the testis
* produce nutrients and @@androgen binding protein@@ → concentrates testosterone to a level requires for spermiogenesis, promoted by FSH
* secrete ==inhibin== → feedback to APG → suppresses FSH
* secrete ==mullerian inhibiting substance== → causes regression of the embryonic mullerian ducts
if there is no MIS → female
3. phagocytosis:
* phagocytoses the residual bodies
* divide the seminiferous tubules into 2 (basal and adluminal) compartments (both are within the sertoli cells though?)
* tall columnar epithelial cells, adhere to the basal lamina and their apical ends extend to the lumen
* abundant SER, some RER, well developed golgi, lots of mitochondria and lysosomes. ovoid or triangular nuclei, euchromatic with a prominent nucleolus
* have tight junctions between their basolateral membranes → forms the blood testis barrier
* spermatogonia lie in a basal compartment of the tubule, below the tight junctions (tight junctions are temporarily disassembled by primary spermatocytes which then move into the adluminal compartment)
17
New cards
adluminal migration occurs without…
compromising the blood testis barrier
18
New cards
where are spermatogonia found
in the basal compartment of the tubule
(attached to sertoli cells?)
(attached to sertoli cells?)
19
New cards
summary of histology and function of male genital ducts (photo)\*\*\*\*
table 21-1
20
New cards
intratesticular ducts
* = the straight tubules/tubuli recti, the rete testis and the efferent ductules → carry spermatozoa and liquid from the seminiferous tubules to the duct of the epididymis
* loops of the @@seminiferous tubules@@ join the @@rete testis@@ by the ^^short straight tubules^^ (initially only lined by sertoli cells) → empty into the @@rete testis@@ (cuboidal, supported by connective tissue of the mediastinum) → drains into around 20 @@efferent ductules@@ (cuboidal alternates with ciliated cells)
* non ciliated cells in the efferent ducts absorb some of the fluid secreted by the sertoli cells of seminiferous tubules and the ciliary activity creates flow → carries sperm passively out of the testis towards the epididymis
* efferent ductules also contain circularly oriented @@smooth muscle cells@@ → aids movement of sperm
* loops of the @@seminiferous tubules@@ join the @@rete testis@@ by the ^^short straight tubules^^ (initially only lined by sertoli cells) → empty into the @@rete testis@@ (cuboidal, supported by connective tissue of the mediastinum) → drains into around 20 @@efferent ductules@@ (cuboidal alternates with ciliated cells)
* non ciliated cells in the efferent ducts absorb some of the fluid secreted by the sertoli cells of seminiferous tubules and the ciliary activity creates flow → carries sperm passively out of the testis towards the epididymis
* efferent ductules also contain circularly oriented @@smooth muscle cells@@ → aids movement of sperm
21
New cards
excretory genital ducts are…
= epididymis, ductus/vas deferens and the urethra → transport sperm from the scrotum to the penis
22
New cards
epididymis
* duct is long and highly coiled (6m), surrounded by connective tissue, lies in the scrotum along the superior and posterior sides of each testis
* includes:
* head region → where the efferent ductules enter
* body → where sperm cells undergo further modifications
* tail → where sperm are stored until ejaculation, continuous with the ductus deferens
* lined with pseudostratified columnar epithelium consisting of columnar principal cells with stereocilia and small round stem cells
* principal cells → remove most of the water and residual bodies + secrete various products → change the fluid in which sperm are suspended
also release exosomes and other vesicles from multivesicular bodies by apocrine secretion → contain many different proteins
* surrounded by a thin circular layer of smooth muscle cells supplemented in the tail region + inner and outer longitudinal layers
* includes:
* head region → where the efferent ductules enter
* body → where sperm cells undergo further modifications
* tail → where sperm are stored until ejaculation, continuous with the ductus deferens
* lined with pseudostratified columnar epithelium consisting of columnar principal cells with stereocilia and small round stem cells
* principal cells → remove most of the water and residual bodies + secrete various products → change the fluid in which sperm are suspended
also release exosomes and other vesicles from multivesicular bodies by apocrine secretion → contain many different proteins
* surrounded by a thin circular layer of smooth muscle cells supplemented in the tail region + inner and outer longitudinal layers
23
New cards
how long does passage of sperm through the epididymis take and what happens
2-4 weeks
during which time the spermatozoa cell membranes bind and integrate many components secreted by the principal cells and released from their exosomes
^^__!! without these modifications, sperm cannot participate in fertilisation__^^
examples of what occurs:
1. development of competence for forwards motility
2. final modifications within the acrosome
3. reorganisation of the cell membrane surrounding the sperm head (addition of cholesterol and other decapacitation factors) which block the acrosomal reaction
during which time the spermatozoa cell membranes bind and integrate many components secreted by the principal cells and released from their exosomes
^^__!! without these modifications, sperm cannot participate in fertilisation__^^
examples of what occurs:
1. development of competence for forwards motility
2. final modifications within the acrosome
3. reorganisation of the cell membrane surrounding the sperm head (addition of cholesterol and other decapacitation factors) which block the acrosomal reaction
24
New cards
capacitation process
occurs to sperm in the female reproductive tract (cell membranes are modified again), until then, fertilising ability of spermatozoa is inhibited
25
New cards
ductus/vas deferens
* long straight tube with a thick muscular wall and a small lumen
* forms part of the ^^__spermatic cord__^^ which also contains the ^^__testicular artery, pampiniform plexus and nerves__^^
* leaves the scrotum and continues towards the prostatic urethra where it empties
* mucosa is slightly folded longitudinally, lamina propria contains elastic fibers, epithelial lining is pseudostratified (some cells have sparse sterocilia)
* muscle produces strong peristaltic contractions during ejaculation
* each duct passes over the urinary bladder where it enlarges as an ^^__ampulla__^^ where the epithelium is thicker and more extensively folded
within the ^^__prostate gland__^^, the ends of the 2 ampullae merge with the ducts of the 2 seminal vesicles → forms the ^^__ejaculatory ducts__^^ which open into the ^^__prostatic urethra__^^
* forms part of the ^^__spermatic cord__^^ which also contains the ^^__testicular artery, pampiniform plexus and nerves__^^
* leaves the scrotum and continues towards the prostatic urethra where it empties
* mucosa is slightly folded longitudinally, lamina propria contains elastic fibers, epithelial lining is pseudostratified (some cells have sparse sterocilia)
* muscle produces strong peristaltic contractions during ejaculation
* each duct passes over the urinary bladder where it enlarges as an ^^__ampulla__^^ where the epithelium is thicker and more extensively folded
within the ^^__prostate gland__^^, the ends of the 2 ampullae merge with the ducts of the 2 seminal vesicles → forms the ^^__ejaculatory ducts__^^ which open into the ^^__prostatic urethra__^^
26
New cards
accessory glands
= seminal vesicles/glands, prostate gland and the bulbourethral glands → produce secretions which become mixed with sperm during ejaculation to produce semen, essential for reproduction
27
New cards
seminal vesicles
* exocrine glands, production of the viscid yellow-ish secretion depends on testosterone
* its fluid makes up 70% of the ejaculate fluid, contains:
1. fructose → energy source for sperm + other metabolites
2. prostaglandins → stimulate activity in the female reproductive tract
3. fibrinogen → allows semen to coagulate after ejactulation
* consist of highly twisted tubes enclosed by a connective tissue capsule
* great number of thin complex folds which fill much of the lumen, lined with simple or pseudostratified columnar epithelial cells rich in secretory granules
* lamina propria contains elastin, surrounded by smooth (inner circular, outer longitudinal) muscle (empty the gland)
* its fluid makes up 70% of the ejaculate fluid, contains:
1. fructose → energy source for sperm + other metabolites
2. prostaglandins → stimulate activity in the female reproductive tract
3. fibrinogen → allows semen to coagulate after ejactulation
* consist of highly twisted tubes enclosed by a connective tissue capsule
* great number of thin complex folds which fill much of the lumen, lined with simple or pseudostratified columnar epithelial cells rich in secretory granules
* lamina propria contains elastin, surrounded by smooth (inner circular, outer longitudinal) muscle (empty the gland)
28
New cards
prostate gland
* dense organ surrounding the urethra below the bladder
* surrounded by a fibroelastic capsule from which septa extend and divide the gland into indistinct lobes
* structure and function depend on the level of testosterone (like the seminal vesicles)
* consists of a collection of 30-50 tubuloacinar glands embedded in a dense fibromuscular stroma where smooth muscle contracts during ejaculation
* tubuloacinar glands are lined by pseudostratified columnar epithelium, produce a fluid that contains a complex of exosomes, glycoproteins, enzymes etc → stored until ejaculation
==__prostate specific antigen (PSA)__== → helps liquefy coagulated semen, some may leak into the prostatic vasculature so if it is increased it may be a carcinoma or inflammation
* lumens of tubuloacinar glands contain corpora amylacea (partially calcified spherical concretions containing deposited glycogen and keratan sulfate)
* ducts from individual glands converge and empty directly into the prostatic urethra (runs through the center of the gland) → membranous urethra
* the glands are arranged in 3 major zones around the urethra:
1. transition zone → 5%, surrounds the superior portion of the urethra, contains the periurethral mucosal glands
2. central zone → 25% of the glands tissue, contains the periurethral submucosal glands with longer ducts
3. peripheral zone → 70%, contains the main glands with even longer ducts
* surrounded by a fibroelastic capsule from which septa extend and divide the gland into indistinct lobes
* structure and function depend on the level of testosterone (like the seminal vesicles)
* consists of a collection of 30-50 tubuloacinar glands embedded in a dense fibromuscular stroma where smooth muscle contracts during ejaculation
* tubuloacinar glands are lined by pseudostratified columnar epithelium, produce a fluid that contains a complex of exosomes, glycoproteins, enzymes etc → stored until ejaculation
==__prostate specific antigen (PSA)__== → helps liquefy coagulated semen, some may leak into the prostatic vasculature so if it is increased it may be a carcinoma or inflammation
* lumens of tubuloacinar glands contain corpora amylacea (partially calcified spherical concretions containing deposited glycogen and keratan sulfate)
* ducts from individual glands converge and empty directly into the prostatic urethra (runs through the center of the gland) → membranous urethra
* the glands are arranged in 3 major zones around the urethra:
1. transition zone → 5%, surrounds the superior portion of the urethra, contains the periurethral mucosal glands
2. central zone → 25% of the glands tissue, contains the periurethral submucosal glands with longer ducts
3. peripheral zone → 70%, contains the main glands with even longer ducts
29
New cards
bulbourethral/cowper glands
* located in the urogenital diaphragm, empty into the proximal part of the penile urethra
* each gland has several lobules with tubuloacinar secretory units surrounded by smooth muscles cells and lined by a mucus secreting simple columnar epithelium → testosterone dependent
* secrete a clear mucus like secretion which coats and lubricates the urethra during an erection in preparation for passing sperm
* each gland has several lobules with tubuloacinar secretory units surrounded by smooth muscles cells and lined by a mucus secreting simple columnar epithelium → testosterone dependent
* secrete a clear mucus like secretion which coats and lubricates the urethra during an erection in preparation for passing sperm
30
New cards
penis
* consists of 3 cylindrical masses of erectile tissue plus the penile urethra, surrounded by skin
* corpora cavernosa = the 2 dorsal erectile masses → each surrounded by the tunica albuginea (a dense fibroelastic layer)
* their central arteries branch to form nutritive arterioles and small coiling helicine arteries which leads to the cavernous vascular spaces
corpus spongiosum = ventral, surrounds the urethra → it expands at its end to form the glans
* all 3 erectile tissues consist of many cavernous spaces lined with endothelium and separated by trabeculae with smooth muscle and connective tissue continuous with the surrounding tissue
* most of the penile urethra is lined with pseudostratified columnar epithelium, once it reaches the glans it is stratified squamous → continuous with the thin epidermis covering the glans surface
* urethral glands are found along the length of the penile urethra → secretes mucus
* if uncircumcised → glans is covered by the prepuce → a retractable fold of thin skin with sebaceous glands on the internal surface
* there are arteriovenous shunts between the central arteries and the dorsal veins
* erection = blood filling the cavernous spaces in the 3 masses of erectile tissue, controlled by autonomic nerves
para → relaxation of the trabecular smooth muscle + dilation of helicine arteries → increased blood flow → enlarges the corpora cavernosa → compress the dorsal veins against the tunica albuginea → blocks venous outflow → tumescence and rigidity in the erectile tissue
* ejaculation = sympathetic → opposite of ^
* corpora cavernosa = the 2 dorsal erectile masses → each surrounded by the tunica albuginea (a dense fibroelastic layer)
* their central arteries branch to form nutritive arterioles and small coiling helicine arteries which leads to the cavernous vascular spaces
corpus spongiosum = ventral, surrounds the urethra → it expands at its end to form the glans
* all 3 erectile tissues consist of many cavernous spaces lined with endothelium and separated by trabeculae with smooth muscle and connective tissue continuous with the surrounding tissue
* most of the penile urethra is lined with pseudostratified columnar epithelium, once it reaches the glans it is stratified squamous → continuous with the thin epidermis covering the glans surface
* urethral glands are found along the length of the penile urethra → secretes mucus
* if uncircumcised → glans is covered by the prepuce → a retractable fold of thin skin with sebaceous glands on the internal surface
* there are arteriovenous shunts between the central arteries and the dorsal veins
* erection = blood filling the cavernous spaces in the 3 masses of erectile tissue, controlled by autonomic nerves
para → relaxation of the trabecular smooth muscle + dilation of helicine arteries → increased blood flow → enlarges the corpora cavernosa → compress the dorsal veins against the tunica albuginea → blocks venous outflow → tumescence and rigidity in the erectile tissue
* ejaculation = sympathetic → opposite of ^
31
New cards
urothelium lines the…
\+ describe it
\+ describe it
renal pelves, ureters, urinary bladder and urethra
5-6 layers, oval nuclei, linear nuclear grooves, abundant cytoplasm
5-6 layers, oval nuclei, linear nuclear grooves, abundant cytoplasm
32
New cards
bladder lamina propria
contains wisps of smooth muscle that form a discontinuous muscularis mucosa
not to be confused with the detrusor muscle (muscularis propria)
not to be confused with the detrusor muscle (muscularis propria)
33
New cards
what happens if urine flow is obstructed
intravesical pressures increase and the bladder musculature undergoes hypertrophy
34
New cards
in what position do ureters lie
retroperitoneal
35
New cards
relaxation of pelvic support in women leads to…
prolapse (descent) of the uterus → pulls the floor of the bladder
bladder is close to the vagina → bladder protrudes into the vagina → pouch (cystocele) that fails to empty readily
bladder is close to the vagina → bladder protrudes into the vagina → pouch (cystocele) that fails to empty readily
36
New cards
enlargement of the prostate causes…
the seminal vesicles and prostate are also close to the bladder (posterior and inferior to the neck of the bladder) → enlarged prostate may cause urinary tract obstruction
37
New cards
most common cause of hydronephrosis in infants and children is… in adults…
uteropelvic junction obstruction (= the most common cause of congenital obstructive lesions)
* hydronephrosis = kidneys become stretched and swollen due to built up urine
* mostly affects males, bilateral in 20% of cases
* often associated with other anomalies
\
in ADULTS:
* UPJ obstruction is more common in women, most often unilateral
* abnormal organisation of smooth muscle bundles or excess stromal deposition of collagen between smooth muscle bundles at the UPJ
* hydronephrosis = kidneys become stretched and swollen due to built up urine
* mostly affects males, bilateral in 20% of cases
* often associated with other anomalies
\
in ADULTS:
* UPJ obstruction is more common in women, most often unilateral
* abnormal organisation of smooth muscle bundles or excess stromal deposition of collagen between smooth muscle bundles at the UPJ
38
New cards
tumours and tumour like lesions of the ureters
* primary tumours of the ureter are rate
* benign tumours are usually of mesenchymal origin
* primary malignant tumours of the ureter resemble those arising in the renal pelvis, calyces and bladder
* majority are urothelial carcinomas
* usually at 60-70
* usually occur with urothelial carcinomas of the bladder or renal pelvis
* fibroepithelial polyp → tumour LIKE lesion, often occur in children, composed of loose vascularies connective tissue overlaid by urothelium
* benign tumours are usually of mesenchymal origin
* primary malignant tumours of the ureter resemble those arising in the renal pelvis, calyces and bladder
* majority are urothelial carcinomas
* usually at 60-70
* usually occur with urothelial carcinomas of the bladder or renal pelvis
* fibroepithelial polyp → tumour LIKE lesion, often occur in children, composed of loose vascularies connective tissue overlaid by urothelium
39
New cards
major causes of ureteral obstruction
intrinsic:
* calculi (kidney stones)
impact at loci of ureteral narrowing → UPJ, where ureters cross iliac vessels and where they enter the bladder
cause renal colic
* strictures
* tumours
* blood clots
* neurogenic
extrinsic:
* pregnancy
* periureteral inflammation
* endometriosis
* tumours
* calculi (kidney stones)
impact at loci of ureteral narrowing → UPJ, where ureters cross iliac vessels and where they enter the bladder
cause renal colic
* strictures
* tumours
* blood clots
* neurogenic
extrinsic:
* pregnancy
* periureteral inflammation
* endometriosis
* tumours
40
New cards
obstructive lesions of the ureters
* may cause ==__hydroureter, hydronephrosis and pyelonephritis__==
* unilateral is usually due to internal or extrinsic causes
* bilateral are usually due to distal causes such as nodular hyperplasia of the prostate (==__how the fuck is that distal when they said its close to the bladder????__==)
\
sclerosing retroperitoneal fibrosis
* rare
* fibrotic proliferative inflammatory process of retroperitoneal structures
* fibrous tissue, infiltrate of lymphocytes often with germinal centers, plasma cells (IgG4 +) and eosinophils
* causes hydronephrosis
* m > f, middle to late age
* a subset is related to IgG4-related disease → increased IgG4, IgG4 secretin plasma cells in fibroinflammatory lesions, also affects other organs
* other causes of retroperitoneal fibrosis → drugs (ergot derivatives, beta blockers), inflammatory conditions (vasculitis, diverticulitis, crohns), malignancies
* most have no obvious cause
* treatment → corticosteroids, a lot become resistant so → ureteral stents or surgical extrication of the ureters from the surrounding fibrous tissue (uterolysis)
* unilateral is usually due to internal or extrinsic causes
* bilateral are usually due to distal causes such as nodular hyperplasia of the prostate (==__how the fuck is that distal when they said its close to the bladder????__==)
\
sclerosing retroperitoneal fibrosis
* rare
* fibrotic proliferative inflammatory process of retroperitoneal structures
* fibrous tissue, infiltrate of lymphocytes often with germinal centers, plasma cells (IgG4 +) and eosinophils
* causes hydronephrosis
* m > f, middle to late age
* a subset is related to IgG4-related disease → increased IgG4, IgG4 secretin plasma cells in fibroinflammatory lesions, also affects other organs
* other causes of retroperitoneal fibrosis → drugs (ergot derivatives, beta blockers), inflammatory conditions (vasculitis, diverticulitis, crohns), malignancies
* most have no obvious cause
* treatment → corticosteroids, a lot become resistant so → ureteral stents or surgical extrication of the ureters from the surrounding fibrous tissue (uterolysis)
41
New cards
congenital anomalies of the bladder
all are associated with increased risk of infection of neoplasia
1. vesicoureteral reflux:
* = urine also flows up from the bladder to the kidneys, may be caused by different things (can also be secondary)
* most common and most serious congenital anomaly
* predisposes to ascending pyelonephritis and loss of renal function
* congenital vesicouterine fistulae may occur
2. diverticula:
* congenital or acquired
* congenital → may be due to focal failure of development of the normal musculature or to a urinary tract obstruction during foetal development → increase in pressure → diverticulum
* acquired → most often associated with prostatic hyperplasia → urinary tract obstruction → same as ^
* most are small and asymptomatic but if not → predispose to infection and bladder calculi
* rarely, carcinoma may arise in bladder diverticula, they are much ==__more advanced__== in stage due to the thin or absent muscularis propria layer of diverticula
3. exstrophy of the bladder:
* development failure in the anterior wall of the abdomen and bladder → bladder communicates directly with the abdominal surface
* exposed bladder mucosa may undergo ==__colonic glandular metaplasia__== → risk of chronic infection that often spreads to the upper urinary tract
* associated with increased risk of ==__adenocarcinoma__==
4. urachal anomalies:
* urachus = the canal that drains the urinary bladder through the umbilicus in the foetus, usually closes at birth
* rarely stays, if so:
* if it remains fully → creates a fistulous urinary tract connection between the bladder and umbilicus
* if it is partially patent → a urachal cyst lined by urothelial or metaplastic glandular epithelium is formed
cysts → increased risk for ==__neoplastic transformation, especially adeno (20-40% of bladder adenocarcinomas not cancers)__==
1. vesicoureteral reflux:
* = urine also flows up from the bladder to the kidneys, may be caused by different things (can also be secondary)
* most common and most serious congenital anomaly
* predisposes to ascending pyelonephritis and loss of renal function
* congenital vesicouterine fistulae may occur
2. diverticula:
* congenital or acquired
* congenital → may be due to focal failure of development of the normal musculature or to a urinary tract obstruction during foetal development → increase in pressure → diverticulum
* acquired → most often associated with prostatic hyperplasia → urinary tract obstruction → same as ^
* most are small and asymptomatic but if not → predispose to infection and bladder calculi
* rarely, carcinoma may arise in bladder diverticula, they are much ==__more advanced__== in stage due to the thin or absent muscularis propria layer of diverticula
3. exstrophy of the bladder:
* development failure in the anterior wall of the abdomen and bladder → bladder communicates directly with the abdominal surface
* exposed bladder mucosa may undergo ==__colonic glandular metaplasia__== → risk of chronic infection that often spreads to the upper urinary tract
* associated with increased risk of ==__adenocarcinoma__==
4. urachal anomalies:
* urachus = the canal that drains the urinary bladder through the umbilicus in the foetus, usually closes at birth
* rarely stays, if so:
* if it remains fully → creates a fistulous urinary tract connection between the bladder and umbilicus
* if it is partially patent → a urachal cyst lined by urothelial or metaplastic glandular epithelium is formed
cysts → increased risk for ==__neoplastic transformation, especially adeno (20-40% of bladder adenocarcinomas not cancers)__==
42
New cards
exstrophy of the bladder is associated with…
an increased risk of adenocarcinoma
43
New cards
urachal cysts are at increased risk for…
neoplastic transformation (mostly adenocarcinoma)
44
New cards
acute and chronic cystitis
* cystitis = inflammation of the bladder = subset of UTIs
* usually the predecessor of bacterial pyelonephritis (= inflammation of the kidney = subset of UTIs) due to retrogade spread
* predisposing factors = bladder calculi, obstruction, DM, instrumentation (eg. catheters), immune deficiency
= usually anything that causes urinary stasis
* triad of symptoms = frequency, lower abdominal pain, dysuria
* mostly caused by the coliforms → E.coli followed by proteus, klebsiella and enterbacter
other causes:
* tuberculous cystitis is ==__almost always__== a sequel to renal tuberculosis
* candida albicans and less commonly cyrptococcal agents, especially in the immunosuppressed
* schistosomiasis is an important cause in certain african and middle eastern countries
* chlamydia and mycoplasma
* adenovirus and BK virus may cause haemorrhagic cystitis
* gas forming bacteria cause emphysematous cystitis
* women > men due to short ureters
* usually produce nonspecific inflammation
* acute → hyperemia of the mucosa, neutrophilic infiltrate, sometimes associated with exudate
chronic → mononuclear inflammatory infiltrates
* if non infectious → may be iatrogenic/radiation (eg. due to pelvic chemo or RT), follicular (lymphoid follicles in the mucosa and underlying wall) and eosinophilic cystitis (may be unspecific or due to a systemic allergic disorder)
cytotoxic agents (eg. cyclophosphamide) may cause haemorrhagic cystitis
\
special forms → interstitial cystitis, malakoplakia and polypoid cystitis
* usually the predecessor of bacterial pyelonephritis (= inflammation of the kidney = subset of UTIs) due to retrogade spread
* predisposing factors = bladder calculi, obstruction, DM, instrumentation (eg. catheters), immune deficiency
= usually anything that causes urinary stasis
* triad of symptoms = frequency, lower abdominal pain, dysuria
* mostly caused by the coliforms → E.coli followed by proteus, klebsiella and enterbacter
other causes:
* tuberculous cystitis is ==__almost always__== a sequel to renal tuberculosis
* candida albicans and less commonly cyrptococcal agents, especially in the immunosuppressed
* schistosomiasis is an important cause in certain african and middle eastern countries
* chlamydia and mycoplasma
* adenovirus and BK virus may cause haemorrhagic cystitis
* gas forming bacteria cause emphysematous cystitis
* women > men due to short ureters
* usually produce nonspecific inflammation
* acute → hyperemia of the mucosa, neutrophilic infiltrate, sometimes associated with exudate
chronic → mononuclear inflammatory infiltrates
* if non infectious → may be iatrogenic/radiation (eg. due to pelvic chemo or RT), follicular (lymphoid follicles in the mucosa and underlying wall) and eosinophilic cystitis (may be unspecific or due to a systemic allergic disorder)
cytotoxic agents (eg. cyclophosphamide) may cause haemorrhagic cystitis
\
special forms → interstitial cystitis, malakoplakia and polypoid cystitis
45
New cards
interstitial cystitis
* = chronic pelvic pain syndrome
* unknown etiology, women >, urinary tract symptoms for more than 6 weeks in the absence of infections or other causes
* characterised by intermittent often severe suprapubic pain, urinary frequency and urgency, haematuria and dysuria
* mucosal fissures and ==__punctate haemorrhages__== (glomerulations), increased __mast cells__
* biopsy to rule out carcinoma in situ which mimics it
* some cases are associated with chronic mucosal ulcers (hunner ulcers) = late (classic, ulcerative) phase
* transmural fibrosis may eventually lead to a ==__contracted bladder__== (overactive bladder → keeps constricting on its own)
* unknown etiology, women >, urinary tract symptoms for more than 6 weeks in the absence of infections or other causes
* characterised by intermittent often severe suprapubic pain, urinary frequency and urgency, haematuria and dysuria
* mucosal fissures and ==__punctate haemorrhages__== (glomerulations), increased __mast cells__
* biopsy to rule out carcinoma in situ which mimics it
* some cases are associated with chronic mucosal ulcers (hunner ulcers) = late (classic, ulcerative) phase
* transmural fibrosis may eventually lead to a ==__contracted bladder__== (overactive bladder → keeps constricting on its own)
46
New cards
malakoplakia
* chronic inflammatory reaction in the setting of chronic bacteria infection (usually E.coli or proteus)
* seems to stem from acquired defects in phagocyte function
* occurs more in the immunosuppressed
* soft yellow slightly raised mucosal plaques
* aggregated of large foamy macrophages with occasional multinucleate giant cells and lymphocytes
* macrophages have abundant glanular cytoplasm
* laminated mineralised concretions resulting from deposition of calcium in enlarged lysosomes = michaelis gutmann bodies
* similar lesions are seen in other organs
* seems to stem from acquired defects in phagocyte function
* occurs more in the immunosuppressed
* soft yellow slightly raised mucosal plaques
* aggregated of large foamy macrophages with occasional multinucleate giant cells and lymphocytes
* macrophages have abundant glanular cytoplasm
* laminated mineralised concretions resulting from deposition of calcium in enlarged lysosomes = michaelis gutmann bodies
* similar lesions are seen in other organs
47
New cards
polypoid cystitis
* commonly as a result of instrumentation
* broad bulbous polypoid projections due to marked submucosal oedema
* may be mistaken for papillary urothelial carcinoma (literally looks the exact same)
* broad bulbous polypoid projections due to marked submucosal oedema
* may be mistaken for papillary urothelial carcinoma (literally looks the exact same)
48
New cards
metaplastic lesions of the bladder
may be true or conditions that mimic metaplasia
1. cystitis glandularis and cystitis cystica:
* common
* nests of urothelium (von brunn nests) grow downwards into the lamina propria → epithelial cells in the center undergo metaplasia and take one of 2 forms
* cuboidal or columnar appearance = cystitis glandularis
* retract to produce cystic spaces lined by flattened urothelium = cystitis cystica
* degeneration in the center? → luminal spaces
* glandularis goblet cells (glandularis), epithelium resembles intestinal mucosa (glandularis intestinal type)
* extensive and multifocal intestinal metaplasia = risk of ==__adenocarcinoma__==
2. squamous metaplasia:
* as a response to chronic injury
* should be distinguished from glycogenated squamous epithelium
* precursor to dysplastic lesions and in situ and invasive squamous cell carcinoma → bladder schistosomiasis is a classic example
3. nephrogenic adenoma:
* may not be a form of true metaplasia, in renal transplant patients some of these lesions are caused by implantation and growth of renal tubular cells at sites of bladder mucosa erosion
* overlying urothelium is replaced by cuboidal epithelium, may have a papillary growth pattern
* tubular proliferation may infiltrate the lamina propria and superficial detrusor muscle → mimics a malignant process
1. cystitis glandularis and cystitis cystica:
* common
* nests of urothelium (von brunn nests) grow downwards into the lamina propria → epithelial cells in the center undergo metaplasia and take one of 2 forms
* cuboidal or columnar appearance = cystitis glandularis
* retract to produce cystic spaces lined by flattened urothelium = cystitis cystica
* degeneration in the center? → luminal spaces
* glandularis goblet cells (glandularis), epithelium resembles intestinal mucosa (glandularis intestinal type)
* extensive and multifocal intestinal metaplasia = risk of ==__adenocarcinoma__==
2. squamous metaplasia:
* as a response to chronic injury
* should be distinguished from glycogenated squamous epithelium
* precursor to dysplastic lesions and in situ and invasive squamous cell carcinoma → bladder schistosomiasis is a classic example
3. nephrogenic adenoma:
* may not be a form of true metaplasia, in renal transplant patients some of these lesions are caused by implantation and growth of renal tubular cells at sites of bladder mucosa erosion
* overlying urothelium is replaced by cuboidal epithelium, may have a papillary growth pattern
* tubular proliferation may infiltrate the lamina propria and superficial detrusor muscle → mimics a malignant process
49
New cards
squamous metaplasia should be differentiated from…
glycogenated squamous epithelium which is found in the trigone area of the bladder in most women → normal
50
New cards
what may clinically or histologically mimic bladder cancer
malakoplakia, polypoid cystitis, cystitis cystica et glandularis and nephrogenic adenoma
51
New cards
bladder neoplasms (names)
most are of epithelial origin (>95%), within them, urothelium neoplasms are the most common followed by squamous and glandular neoplasms
\
1. urothelial neoplasms
2. adenocarcinoma
3. squamous cell carcinoma
4. mixed carcinoma
5. small cell carcinoma
6. sarcomas
\
1. urothelial neoplasms
2. adenocarcinoma
3. squamous cell carcinoma
4. mixed carcinoma
5. small cell carcinoma
6. sarcomas
52
New cards
urothelial neoplasms
* represent 90% of all bladder tumours
* most are multifocal at presentation
* most common in the bladder but occur where there is urothelium
* men > female, 80% are 50-80, not familial
* risk factors:
* cigarette smoking → 7x risk, 50-80% of bladder cancers among men are associated with smoking)
* exposure to aryl amines
* schistosoma haematobium (70% are squamous, the rest are urothelial or glandular)
* long term use of analgesics and cyclophosphamide (increased risk of haemorrhagic cystitis → increased risk of bladder cancer)
* irradiation
* 2 distinct precursor lesions to invasive urothelial carcinoma
1. non invasive papillary neoplasms → most common
* usually gain of function of ==__FGFR3__== → activating mutations of ==__RAS__== and PI3K
* often recur but ==__only 20% invade the muscle__==
* red, elevated, attached to the mucosa by a stalk (what if their precursors are inverted papillomas?)
2. flat non invasive urothelial carcinoma in situ (CIS)
* mutations of ==__p53__== and ==__RB__== (usually in all muscle invasive cancers)
* more likely to invade the muscle
* invasion into the lamina propria worsens the prognosis but the major decrease in survival is associated with invasion of the muscularis propria (once the muscle is reached, the 5 year mortality is 30%)
* non invasive ==__papillary__== urothelial tumours AND those that __*solely invade the lamina propria*__ (= non muscle invasive) cause 70-80% of urothelial neoplasms
20-30% are muscle invasive
* types (?) → papillomas, papillary urothelial neoplasms of low malignant potential, low grade papillary urothelial carcinomas, high grade papillary urothelial carcinomas, CIS, invasive urothelial carcinoma (associated with papillary or CIS tumours)
* most are multifocal at presentation
* most common in the bladder but occur where there is urothelium
* men > female, 80% are 50-80, not familial
* risk factors:
* cigarette smoking → 7x risk, 50-80% of bladder cancers among men are associated with smoking)
* exposure to aryl amines
* schistosoma haematobium (70% are squamous, the rest are urothelial or glandular)
* long term use of analgesics and cyclophosphamide (increased risk of haemorrhagic cystitis → increased risk of bladder cancer)
* irradiation
* 2 distinct precursor lesions to invasive urothelial carcinoma
1. non invasive papillary neoplasms → most common
* usually gain of function of ==__FGFR3__== → activating mutations of ==__RAS__== and PI3K
* often recur but ==__only 20% invade the muscle__==
* red, elevated, attached to the mucosa by a stalk (what if their precursors are inverted papillomas?)
2. flat non invasive urothelial carcinoma in situ (CIS)
* mutations of ==__p53__== and ==__RB__== (usually in all muscle invasive cancers)
* more likely to invade the muscle
* invasion into the lamina propria worsens the prognosis but the major decrease in survival is associated with invasion of the muscularis propria (once the muscle is reached, the 5 year mortality is 30%)
* non invasive ==__papillary__== urothelial tumours AND those that __*solely invade the lamina propria*__ (= non muscle invasive) cause 70-80% of urothelial neoplasms
20-30% are muscle invasive
* types (?) → papillomas, papillary urothelial neoplasms of low malignant potential, low grade papillary urothelial carcinomas, high grade papillary urothelial carcinomas, CIS, invasive urothelial carcinoma (associated with papillary or CIS tumours)
53
New cards
clinical features and treatments of urothelial neoplasms
* painless haematuria (= ==__most common__==), frequency, urgency and dysuria
* obstruction of the ureteral orifice may cause pyelonephritis or hydronephrosis
\
if non muscle invasive:
* if small, localised low grade papillary tumours → transurethral resection ONLY
* CIS and papillary tumours that are large, high grade, multifocal, have a history of recurrence or are associated with lamina propria invasion → intravesical instillation of an attenuated strain of mycobacterium bovis called bacillus calmette guerin → causes local inflammatory reaction → destroys the tumour
\
muscle invasive:
* high tendency to recur/going to a higher stage
* most recurrence sites appear at sites other than that of the original lesion yet are clonally related → seems to be from shedding and implantation of cells from the original tumour at a distant site
* radical cystectomy or cystoprostatectomy or RT with (neo/)adjuvant chemo
* lifelong surveillance and follow up → cystoscopy, biopsies and urine cytologic examinations
\
metastatic tumours respond poorly to CT → 5 year survival = 15%
* obstruction of the ureteral orifice may cause pyelonephritis or hydronephrosis
\
if non muscle invasive:
* if small, localised low grade papillary tumours → transurethral resection ONLY
* CIS and papillary tumours that are large, high grade, multifocal, have a history of recurrence or are associated with lamina propria invasion → intravesical instillation of an attenuated strain of mycobacterium bovis called bacillus calmette guerin → causes local inflammatory reaction → destroys the tumour
\
muscle invasive:
* high tendency to recur/going to a higher stage
* most recurrence sites appear at sites other than that of the original lesion yet are clonally related → seems to be from shedding and implantation of cells from the original tumour at a distant site
* radical cystectomy or cystoprostatectomy or RT with (neo/)adjuvant chemo
* lifelong surveillance and follow up → cystoscopy, biopsies and urine cytologic examinations
\
metastatic tumours respond poorly to CT → 5 year survival = 15%
54
New cards
when is radical cystectomy done if its not muscle invasive
1. CIS or high grade papillary cancer refractory BCG and other intravesical therapies
2. CIS extending into the prostatic urethra and ducts, sites where instilled BCG does not come into contact with the neoplastic cells
3. occasional cases of non muscle invasive papillary urothelial high grade carcinoma such as multifocal lesions that are too large
55
New cards
p53 and RB mutations…
occur early in CIS and later in papillary cancers
→ related to muscle invasion
→ related to muscle invasion
56
New cards
urothelial papillomas\*\*\*
* might be precursors to non invasive/invasive papillary tumours
* they are BENIGN and represent <1% of all bladder cancers (which means that most bladder cancers are malignant)
* often seen in younger patients
* may be exophytic → each papillae has a central core of loose fibrovascular tissue covered by epithelium identical to urothelium
recurrences and progression are rare but may occur
* may be inverted → completely benign (as in they dont progress? but how? they stimulate an invasive process??) higher risk of malignancy than exophytic
inter anastomosing cords of cytologically bland urothelium that extend down into the lamina propria
* they are BENIGN and represent <1% of all bladder cancers (which means that most bladder cancers are malignant)
* often seen in younger patients
* may be exophytic → each papillae has a central core of loose fibrovascular tissue covered by epithelium identical to urothelium
recurrences and progression are rare but may occur
* may be inverted → completely benign (as in they dont progress? but how? they stimulate an invasive process??) higher risk of malignancy than exophytic
inter anastomosing cords of cytologically bland urothelium that extend down into the lamina propria
57
New cards
papillary urothelial neoplasms of low malignant potential (PUNLMP)
* share histologic features with papillomas but they have thicker urothelium with greater density of cells
* tend to be larger than papillomas and may be indistinguishable from papillary cancers
* tend to be larger than papillomas and may be indistinguishable from papillary cancers
58
New cards
what looks like papillomas
papillary urothelial neoplasms of low malignant potential
59
New cards
low grade papillary urothelial carcinomas
* orderly architectural appearance and low grade cytologic atypia, evenly spaced cells (= ==__maintain polarity__==) and cohesive
* scattered hyperchromatic nuclei, infrequent mitotic figures mainly towards the base, slight variation in nuclear size and shape
* may recur, rarely invade
* scattered hyperchromatic nuclei, infrequent mitotic figures mainly towards the base, slight variation in nuclear size and shape
* may recur, rarely invade
60
New cards
high grade papillary urothelial carcinoma
* dyscohesive cells with large hyperchromatic nuclei, irregular nuclear chromatin and prominent nucleoli
* frequent mitotic figures
* higher incidence of progression to muscle invasive bladder cancer, significant potential for metastasis
* lead to death in 25% of cases
* frequent mitotic figures
* higher incidence of progression to muscle invasive bladder cancer, significant potential for metastasis
* lead to death in 25% of cases
61
New cards
CIS
* = flat urothelial carcinoma
* defined by the presence of cytologically malignant cells within a flat urothelium
* may range from full thickness cytologic atypia to scattered malignant cells in an otherwise normal urothelium (pagetoid spread)
* lack of cohesiveness → shedding of malignant cells into the urine (so much might be shed that only a few cells are actually left in the urothelium)
similar to high grade papillary carcinoma in this sense
* mucosal reddening, granularity or thickening without an evident intraluminal mass
* usually multifocal, may involve most of the bladder surface and extend into the ureters and urethra
* 50-75% progress to invasive cancer if untreated
* defined by the presence of cytologically malignant cells within a flat urothelium
* may range from full thickness cytologic atypia to scattered malignant cells in an otherwise normal urothelium (pagetoid spread)
* lack of cohesiveness → shedding of malignant cells into the urine (so much might be shed that only a few cells are actually left in the urothelium)
similar to high grade papillary carcinoma in this sense
* mucosal reddening, granularity or thickening without an evident intraluminal mass
* usually multifocal, may involve most of the bladder surface and extend into the ureters and urethra
* 50-75% progress to invasive cancer if untreated
62
New cards
the degree of atypia in urothelial neoplasms dictates…
the type of lesion, eg. in order:
if exophytic: papilloma (no atypia) → PUNLMP → low grade papillary urothelial carcinoma → high grade papillary urothelial carcinoma → invasive
\
if flat: normal epithelium → urothelial hyperplasia → urothelial dysplasia → CIS → invasive
\
(i dont think they have to exactly follow this order)
if exophytic: papilloma (no atypia) → PUNLMP → low grade papillary urothelial carcinoma → high grade papillary urothelial carcinoma → invasive
\
if flat: normal epithelium → urothelial hyperplasia → urothelial dysplasia → CIS → invasive
\
(i dont think they have to exactly follow this order)
63
New cards
grading urothelial neoplasms\*\*\* (photo)
64
New cards
other causes of bladder cancer
1. squamous cell:
* make up 3-7% of bladder cancers
* more frequent in areas where urinary schistosomiasis is endemic
* pure squamous cell carcinoma arise from atypical keratinising mucosa (squamous dysplasia and CIS) and are nearly always associated with chronic bladder irritation and infection
2. mixed urothelial carcinoma with areas of squamous:
* more common than pure squamous
* most are invasive, fungating tumours or are infiltrative and ulcerative
3. adenocarcinoma:
* rare
* histologically identical to those in the GI
* some arise from urachal remnants or in association with extensive intestinal metaplasia (eg. in exstrophy of the bladder etc)
4. small cell carcinoma:
* indistinguishable from small cell of the lungs → very aggressive, associated with loss of function of p53 and RB
* often associated with urothelial, squamous or adenocarcinoma
5. mesenchymal tumours:
1. benign tumours:
* collectively (all mesenchymal tumours) are rare
* most common = leiomyoma
* tend to grow as isolated intramural (submucosal), encapsulated, oval to spherical masses
2. sarcomas:
* uncommon in the bladder
* inflammatory myofibroblastic tumours and various carcinomas that look have sarcomatoid growth patterns are more common than true sarcomas
* protrude into the vesicle lumen
* soft, fleshy grey-white appearance suggests their mesenchymal origin
* most common bladder sarcoma in infancy or childhood = embryonal rhabdomyosarcoma
in some cases they manifest as polypoid grape like masses (sarcoma botryoides)
* most common in adults = leiomyosarcoma
6. secondary tumours:
* usually due to direct extension of cancers arising in adjacent organs
* metastatic spread of solid tumours is very rare
65
New cards
obstruction of the bladder outlet
* may eventually affect the kidneys
* more common in males, usually due to enlargement of the prostate gland due to ==__benign prostatic hyperplasia__== (BPH)
* in women it is usually caused by ==__cystocele__== of the bladder (still rare)
* in early stages there is only thickening of the bladder wall due to smooth muscle hypertrophy
then: individual muscle bundles enlarge and produce ==__trabeculation__== of the bladder wall → crypts form and may be converted into diverticula
* if enlarged then it lacks trabeculae (?)
* more common in males, usually due to enlargement of the prostate gland due to ==__benign prostatic hyperplasia__== (BPH)
* in women it is usually caused by ==__cystocele__== of the bladder (still rare)
* in early stages there is only thickening of the bladder wall due to smooth muscle hypertrophy
then: individual muscle bundles enlarge and produce ==__trabeculation__== of the bladder wall → crypts form and may be converted into diverticula
* if enlarged then it lacks trabeculae (?)
66
New cards
inflammation of the urethra
* divided into gonococcal and non gonococcal causes
* gonococcal urethritis is one of the earliest manifestations of this venereal infection
* nongonococcal urethritis is common and can be caused by different organisms
chlamydia strains are the cause in 25-60% of men and 20% in women
may also be caused by mycoplasma
* some urethritis is non infectious in origin eg. in ==__reactive arthritis__==
* gonococcal urethritis is one of the earliest manifestations of this venereal infection
* nongonococcal urethritis is common and can be caused by different organisms
chlamydia strains are the cause in 25-60% of men and 20% in women
may also be caused by mycoplasma
* some urethritis is non infectious in origin eg. in ==__reactive arthritis__==
67
New cards
tumour and tumour like lesions of the urethra
* urethral caruncle → inflammatory lesion, small red painful mass about the external urethral meatus, typically in older females
inflamed granulation tissue covered by mucosa which may ulcerate and bleed with the slightest trauma
surgical excision
* benign epithelial tumours → squamous and urothelial tumours, inverted urothelial papillomas and condylomas
* primary carcinomas are uncommon
proximal urethra → show more urothelial differentiation
distal → more squamous and HPV related
inflamed granulation tissue covered by mucosa which may ulcerate and bleed with the slightest trauma
surgical excision
* benign epithelial tumours → squamous and urothelial tumours, inverted urothelial papillomas and condylomas
* primary carcinomas are uncommon
proximal urethra → show more urothelial differentiation
distal → more squamous and HPV related
68
New cards
congenital penis abnormalities
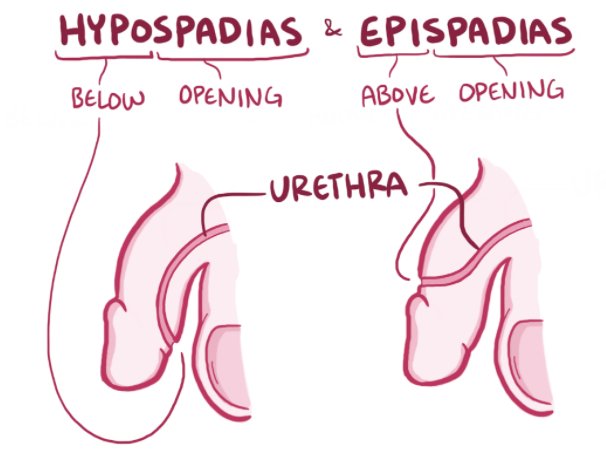
1. hypospadias and epispadias:
* hypo → abnormal opening of the urethral meatus on the ventral surface of the penis → more common
* epi → abnormal opening on the dorsal surface
* both may be associated with failure of normal descent of the testes with malformations of the urinary tract
* the abnormal opening is often constricted → urinary tract obstruction → ascending infections
* when the orifices (openings) are near the base of the penis, normal ejaculation and insemination are hampered → sterility
2. phimosis:
* = when the orifice of the prepuce (foreskin) is too small to permit retraction
* usually due to repeated infections that cause scarring of the preputial ring (the very top of the foreskin surrounding the urethral meatus)
* interferes with cleanliness and permits the accumulation of secretions and detritus → secondary infections → risk of ==__penile carcinoma__==
69
New cards
inflammation of the penis
* almost always involves the glands and prepuce
* specific infections are sexually transmitted → syphylis, gonorrhea, chancroid, granuloma inguinale, lymphopathia, venerea, genital herpes
* non specific infections= balanoposthitis = infections of the glans and prepuce by a variety of organisms, commonly C.albicans, anaerobic bacteria, Gardnerella and pyogenic bacteria
usually due to poor hygiene in uncircumcised males → accumulation of desquamated epithelial cells, sweat and debris (= smegma) acts as a local irritant → inflammatory scarring → a common cause (and consequence) of phimosis
* specific infections are sexually transmitted → syphylis, gonorrhea, chancroid, granuloma inguinale, lymphopathia, venerea, genital herpes
* non specific infections= balanoposthitis = infections of the glans and prepuce by a variety of organisms, commonly C.albicans, anaerobic bacteria, Gardnerella and pyogenic bacteria
usually due to poor hygiene in uncircumcised males → accumulation of desquamated epithelial cells, sweat and debris (= smegma) acts as a local irritant → inflammatory scarring → a common cause (and consequence) of phimosis
70
New cards
penile tumours (benign and tumour like)
* uncommon
* most common = SCC and benign genital warts (condyloma acuminatum)
\
__**benign tumours and tumour like conditions:**__
1. condyloma acuminatum:
* benign, sexually transmitted by HPV (usually 6 and 11 → ‘low risk’)
* may arise in the external genitalia or perineal areas (area between genitals and anus, bottom of the pelvic cavity)
* usually in the coronal sulcus (bottom of the foreskin) and inner surface of the prepuce
* single or multiple sessile or pedunculated red papillary excrescences, covered by epithelium, may have superficial hyperkeratosis and thickening of the underlying epidermis (acanthosis)
* lining cells display perinuclear cytoplasmic vacuolisation (koilocytosis)
2. peyronie disease:
* reactive rather than neoplastic
* hard penile plaques due to deposition of collagen in the connective tissue between the corpora cavernosa (the 2 dorsal erectile tissues) and the tunica albuginea (surrounds it, also found in the testes?)
* might be due to microvascular trauma → sclerosing chronic inflammation
* causes penile curvature ==__towards__== the side of the lesion + pain during intercourse
* treatment = surgery and injection of ==__collagenase__==
* most common = SCC and benign genital warts (condyloma acuminatum)
\
__**benign tumours and tumour like conditions:**__
1. condyloma acuminatum:
* benign, sexually transmitted by HPV (usually 6 and 11 → ‘low risk’)
* may arise in the external genitalia or perineal areas (area between genitals and anus, bottom of the pelvic cavity)
* usually in the coronal sulcus (bottom of the foreskin) and inner surface of the prepuce
* single or multiple sessile or pedunculated red papillary excrescences, covered by epithelium, may have superficial hyperkeratosis and thickening of the underlying epidermis (acanthosis)
* lining cells display perinuclear cytoplasmic vacuolisation (koilocytosis)
2. peyronie disease:
* reactive rather than neoplastic
* hard penile plaques due to deposition of collagen in the connective tissue between the corpora cavernosa (the 2 dorsal erectile tissues) and the tunica albuginea (surrounds it, also found in the testes?)
* might be due to microvascular trauma → sclerosing chronic inflammation
* causes penile curvature ==__towards__== the side of the lesion + pain during intercourse
* treatment = surgery and injection of ==__collagenase__==
71
New cards
what is characteristic of HPV infection
lining cells display perinuclear cytoplasmic vacuolisation (koilocytosis)
72
New cards
penile tumours (malignant)
__**malignant tumours:**__
1. SCC in situ/penile intraepithelial neoplasia:
* lesions can vary but their umbrella term is penile intraepithelial neoplasia (PeIN) → all are squamous lesions confined to the epidermis by an intact BM
* PeIN may be HPV related (==__undifferentiated__==) or not (==__differentiated__==)
* differentiated PeIN is associated with balanitis xerotica obliterans (BXO) → retains a degree of squamous maturation
* undifferentiated PeIN → composed of more malignant cells and may manifest as 2 distinct lesions
both are associated with high risk HPV, mostly ==__HPV 16__==
1. bowen disease:
* usually affects the penile shaft and scrotum (skin that holds protects the testicles) of older men
* solitary, thickened, grey-white opaque plaque
* if it affects the glans (uncommon) → red, velvety
* dysplastic squamous cells with large hyperchromatic irregular nuclei, no orderly maturation
* numerous mitosis
* in 10% it causes infiltrating SCC
2. bowenoid papulosis:
* occurs in sexually active adults
* different from ^ due to: younger age, multiple rather than solitary reddish brown papular lesions
* indistinguishable from ^ histologically
* never develops into invasive SCC and usually regresses spontaneously
2. invasive SCC:
* associated with poor hygiene and high risk HPV infection
* 40-70
* circumcision acts as protection → better hygiene, may also reduce exposure to carcinogens that may be concentrated in smegma
* risks → cigs, chronic inflammatory conditions (eg. BXO)
* high risk HPV → encodes for E6 and E7 → inactivate p53 and RB
E6 → stimulates telomerase expression
E7 → induces feedback loops that increase levels of p16 (==__is this not the opposite of what cancer would want???__==)
1. SCC in situ/penile intraepithelial neoplasia:
* lesions can vary but their umbrella term is penile intraepithelial neoplasia (PeIN) → all are squamous lesions confined to the epidermis by an intact BM
* PeIN may be HPV related (==__undifferentiated__==) or not (==__differentiated__==)
* differentiated PeIN is associated with balanitis xerotica obliterans (BXO) → retains a degree of squamous maturation
* undifferentiated PeIN → composed of more malignant cells and may manifest as 2 distinct lesions
both are associated with high risk HPV, mostly ==__HPV 16__==
1. bowen disease:
* usually affects the penile shaft and scrotum (skin that holds protects the testicles) of older men
* solitary, thickened, grey-white opaque plaque
* if it affects the glans (uncommon) → red, velvety
* dysplastic squamous cells with large hyperchromatic irregular nuclei, no orderly maturation
* numerous mitosis
* in 10% it causes infiltrating SCC
2. bowenoid papulosis:
* occurs in sexually active adults
* different from ^ due to: younger age, multiple rather than solitary reddish brown papular lesions
* indistinguishable from ^ histologically
* never develops into invasive SCC and usually regresses spontaneously
2. invasive SCC:
* associated with poor hygiene and high risk HPV infection
* 40-70
* circumcision acts as protection → better hygiene, may also reduce exposure to carcinogens that may be concentrated in smegma
* risks → cigs, chronic inflammatory conditions (eg. BXO)
* high risk HPV → encodes for E6 and E7 → inactivate p53 and RB
E6 → stimulates telomerase expression
E7 → induces feedback loops that increase levels of p16 (==__is this not the opposite of what cancer would want???__==)
73
New cards
morphology and clinical features of penile SCC
* usually in the glans or inner surface of the prepuce near the coronal sulcus
* irregular, fungating masses OR flat, indurated lesions OR large verruciform/papillary tumours
1. verrucous:
* exophytic, warty, well differentiated, ==__non HPV__== related
* invades locally along a broad pushing border but rarely metastasises
2. basaloid:
* HPV related
* small hyperchromatic cells
* destructive pattern of invasion, usually aggressive
* invasive → slow growing, locally invasive, non painful until they undergo secondary ulceration and infection
metastasis to inguinal lymph nodes may occur early on
prognosis is strongly correlated with tumour stage at diagnosis
* irregular, fungating masses OR flat, indurated lesions OR large verruciform/papillary tumours
1. verrucous:
* exophytic, warty, well differentiated, ==__non HPV__== related
* invades locally along a broad pushing border but rarely metastasises
2. basaloid:
* HPV related
* small hyperchromatic cells
* destructive pattern of invasion, usually aggressive
* invasive → slow growing, locally invasive, non painful until they undergo secondary ulceration and infection
metastasis to inguinal lymph nodes may occur early on
prognosis is strongly correlated with tumour stage at diagnosis
74
New cards
balanitis xerotica obliterans
a progressive sclerosing inflammatory dermatosis of the glans penis and foreskin
can lead to phimosis and urethral stenosis
can lead to phimosis and urethral stenosis
75
New cards
what affects the testis and epididymis respectively the most
epi → inflammatory diseases
testis → tumours
testis → tumours
76
New cards
congenital anomalies of the testis and epididymis
* congenital anomalies are extremely rare EXCEPT for cryptorchidism
1. cryptorchidism:
* = complete or partial failure of the intra abdominal testes to descend into the scrotal sac
* associated with testicular dysfunction and ==__increased risk of testicular cancer__==
* found in 1% of 1 y/o boys
* usually isolated but may be seen with other malformations of the genitourinary tract (eg. hypospadias)
* testicular descent occurs in 2 phases → testes may arrest anywhere in this phase
* even though testicular descent is controlled by hormonal factors, cryptorchidism is only rarely associated with a well defined hormonal disorder
* usually unilateral (75%), testes are small and firm
* thickening of the BM of the spermatic tubules → loss of spermatogonia → only sertoli cells
* scarred tubules may appear as dense cords of hyaline connective tissue associated with a concomitant increase in interstitial stroma
* ==__it is a marker of an intrinsic defect in gonadal development__==
* asymptomatic, comes to attention when the scrotal sac is empty
* causes sterility, may also be associated with other morbidities (==__crushing injuries due to trauma to the inguinal region and inguinal hernia, 10-20%????__==)
* the majority of inguinal cryptorchid testes ==__descend spontaneously__== into the scrotum
* if they dont descend → surgical correction by ==__orchiopexy__== preferably prior to development of histologic changes (10-60% still have deficient spermatogenesis)
1. cryptorchidism:
* = complete or partial failure of the intra abdominal testes to descend into the scrotal sac
* associated with testicular dysfunction and ==__increased risk of testicular cancer__==
* found in 1% of 1 y/o boys
* usually isolated but may be seen with other malformations of the genitourinary tract (eg. hypospadias)
* testicular descent occurs in 2 phases → testes may arrest anywhere in this phase
* even though testicular descent is controlled by hormonal factors, cryptorchidism is only rarely associated with a well defined hormonal disorder
* usually unilateral (75%), testes are small and firm
* thickening of the BM of the spermatic tubules → loss of spermatogonia → only sertoli cells
* scarred tubules may appear as dense cords of hyaline connective tissue associated with a concomitant increase in interstitial stroma
* ==__it is a marker of an intrinsic defect in gonadal development__==
* asymptomatic, comes to attention when the scrotal sac is empty
* causes sterility, may also be associated with other morbidities (==__crushing injuries due to trauma to the inguinal region and inguinal hernia, 10-20%????__==)
* the majority of inguinal cryptorchid testes ==__descend spontaneously__== into the scrotum
* if they dont descend → surgical correction by ==__orchiopexy__== preferably prior to development of histologic changes (10-60% still have deficient spermatogenesis)
77
New cards
phases of testicular descent
1. transabdominal phase:
* testis come to lie within the lower abdomen or brim of the pelvis
* controlled by mullerian inhibiting substance
2. inguinoscrotal phase:
* testes descend through the inguinal canal into scrotal sac
* androgen dependent, thought to be mediated by androgen induced released of calcitonin gene related peptide from the genitofemoral nerve
78
New cards
regressive changes of the testis and epididymis
atrophy and decreased fertility:
testicular atrophy may be caused by → progressive atherosclerotic narrowing of the blood supply in old age, end stage inflammatory orchitis, cryptorchidism, hypopituitarism, generalised malnutrition or cachexia, irradiation, prolonged antiandrogens (eg. for treating prostate carcinoma), cirrhosis, genetics, exhaustion atrophy
testicular atrophy may be caused by → progressive atherosclerotic narrowing of the blood supply in old age, end stage inflammatory orchitis, cryptorchidism, hypopituitarism, generalised malnutrition or cachexia, irradiation, prolonged antiandrogens (eg. for treating prostate carcinoma), cirrhosis, genetics, exhaustion atrophy
79
New cards
inflammation and infection of the testis and epididymis
more common in the epididymitis
(syphilis involves the testis first but TB and gonorrhea affects the epi first and then testis secondarily)
1. nonspecific epididymitis and orchitis:
* commonly related to UTIs which reach them through the vas deferens or the lymphatics of the spermatic cord
* uncommon in children but if so, usually associated with a congenital genitourinary abnormality and infection with gram negative rods
* in sexually active men <35 it is usually C.trachomatis and neisseria gonnorrhoea
if >35 → E.coli and pseudomonas
* acute inflammation characterised by congestion, oedema and infiltration by neutrophils
* usually starts in the interstitial connective tissues but then rapidly extends to the tubules and then secondarily the testis
* often followed by fibrous scarring which may cause sterility
2. granulomatous (autoimmune) orchitis:
* middle age
* tender testicular mass of sudden onset sometimes with fever, painless
* mimics a testicular tumour
* granulomas restricted to spermatic tubules
* must be distinguished from mycobacterial infections which cause caseous necrosis
3. infections:
1. gonorrhoea
2. mumps → usually children, testis involvement is uncommon at their age but orchitis occurs in 20-30% of older boys
acute interstitial orchitis develops 1 week after the onset of swelling of the parotid glands
3. TB
4. syphilis → 2 forms
* obliterative endarteritis → perivascular cuffs of lymphocytes and plasma cells → hallmark of syphilis
* gumma → granulomatous inflammation
(syphilis involves the testis first but TB and gonorrhea affects the epi first and then testis secondarily)
1. nonspecific epididymitis and orchitis:
* commonly related to UTIs which reach them through the vas deferens or the lymphatics of the spermatic cord
* uncommon in children but if so, usually associated with a congenital genitourinary abnormality and infection with gram negative rods
* in sexually active men <35 it is usually C.trachomatis and neisseria gonnorrhoea
if >35 → E.coli and pseudomonas
* acute inflammation characterised by congestion, oedema and infiltration by neutrophils
* usually starts in the interstitial connective tissues but then rapidly extends to the tubules and then secondarily the testis
* often followed by fibrous scarring which may cause sterility
2. granulomatous (autoimmune) orchitis:
* middle age
* tender testicular mass of sudden onset sometimes with fever, painless
* mimics a testicular tumour
* granulomas restricted to spermatic tubules
* must be distinguished from mycobacterial infections which cause caseous necrosis
3. infections:
1. gonorrhoea
2. mumps → usually children, testis involvement is uncommon at their age but orchitis occurs in 20-30% of older boys
acute interstitial orchitis develops 1 week after the onset of swelling of the parotid glands
3. TB
4. syphilis → 2 forms
* obliterative endarteritis → perivascular cuffs of lymphocytes and plasma cells → hallmark of syphilis
* gumma → granulomatous inflammation
80
New cards
vascular disorders of the testis and epididymis
__**torsion:**__
* twisting of the spermatic cord → cuts off venous drainage
* if untreated → testicular infarction
* thick walled arteries remain patent → vascular engorgement followed by haemorrhagic infarction
* occurs in 2 settings:
1. neonatal torsion:
* in utero or shortly after birth
* no anatomical cause
2. ‘adult’ torsion
* sudden onset of pain
* often occurs without any inciting injury
* if the testis are manually untwisted within 6 hours → spares orchiectomy
* results from a bilateral anatomic defect that leads to increased mobility of the testes
* contralateral orchiopexy is performed to prevent recurrence in the unaffected testis
* twisting of the spermatic cord → cuts off venous drainage
* if untreated → testicular infarction
* thick walled arteries remain patent → vascular engorgement followed by haemorrhagic infarction
* occurs in 2 settings:
1. neonatal torsion:
* in utero or shortly after birth
* no anatomical cause
2. ‘adult’ torsion
* sudden onset of pain
* often occurs without any inciting injury
* if the testis are manually untwisted within 6 hours → spares orchiectomy
* results from a bilateral anatomic defect that leads to increased mobility of the testes
* contralateral orchiopexy is performed to prevent recurrence in the unaffected testis
81
New cards
spermatic cord and paratesticular tumours
* lipomas are common lesions involving the proximal spermatic cord, discovered at the time of inguinal hernia repair
* theyre not actually lipomas, many of them represent retroperitoneal adipose tissue that has been pulled into the inguinal canal along with the hernia sac
* most common benign paratesticular tumour = adenomatoid tumour, mesothelial in origin but not referred to as such
* small nodules. usually near the upper pole of the epididymis
* one of the few benign tumours that occur near the testis
* most common malignant paratesticular tumour in children = rhabdomyosarcoma, in adults = liposarcomas
* theyre not actually lipomas, many of them represent retroperitoneal adipose tissue that has been pulled into the inguinal canal along with the hernia sac
* most common benign paratesticular tumour = adenomatoid tumour, mesothelial in origin but not referred to as such
* small nodules. usually near the upper pole of the epididymis
* one of the few benign tumours that occur near the testis
* most common malignant paratesticular tumour in children = rhabdomyosarcoma, in adults = liposarcomas
82
New cards
inguinal canal, hernia and spermatic cord (photo)
83
New cards
testicular tumours (basics)
* different categories → germ cell tumours derived from germ cell neoplasia in situ, germ cell tumours unrelated to germ cell neoplasia in situ, sex cord stromal tumours, tumours containing both germ cell and sex cord stromal elements
* germ cell tumours are the most common (95%) followed by sex cord stromal tumours
* germ cell tumours are the most common (95%) followed by sex cord stromal tumours
84
New cards
germ cell testicular tumours
* mostly affect caucasian males between 15 and 45 → most common cancer in this age group
* environmental exposure and inherited and acquired genetic abnormalities contribute to its development
* associated with a spectrum of disorders called testricular dysgenesis syndrome → cryptorchidism, hypospadias and poor sperm quality
might be caused by increased in utero exposure to pesticides and nonsteroidal oestrogens
==__most important association is with cryptorchidism (seen in 10% of those with testicular GCTs)__==
* more likely to get it if your brother has it rather than father
* linked to the genes encoding the ligand for the receptor tyrosine kinase KIT and BAK which is an inducer for apoptosis
\
steps in its development:
1. origin = primordial germ cell with an acquired defect in differentiation
2. activation of growth factor receptor signalling, usually by activating the KIT receptor tyrosine kinase → proliferation and formation of the precursor lesion, germ cell neoplasia in situ
precursor lesion is found in 90% of GCTs except spermatocytic tumour and those that arise in infancy
==__precursor lesion believed to arise in utero and stay dormant till puberty (may be hormone affected)__==
3. germ cell neoplasia in situ
4. reduplication of the short arm of chromosome 12 (isochromosome 12p)
progression to GCT in those with germ cell neoplasia in situ (eg. in those with cryptorchid testes) is ==__70%__== within 7 years of diagnosis
==__!! lesions retain the expression of OCT3/4 and NANOG (transcription factors)__==
* environmental exposure and inherited and acquired genetic abnormalities contribute to its development
* associated with a spectrum of disorders called testricular dysgenesis syndrome → cryptorchidism, hypospadias and poor sperm quality
might be caused by increased in utero exposure to pesticides and nonsteroidal oestrogens
==__most important association is with cryptorchidism (seen in 10% of those with testicular GCTs)__==
* more likely to get it if your brother has it rather than father
* linked to the genes encoding the ligand for the receptor tyrosine kinase KIT and BAK which is an inducer for apoptosis
\
steps in its development:
1. origin = primordial germ cell with an acquired defect in differentiation
2. activation of growth factor receptor signalling, usually by activating the KIT receptor tyrosine kinase → proliferation and formation of the precursor lesion, germ cell neoplasia in situ
precursor lesion is found in 90% of GCTs except spermatocytic tumour and those that arise in infancy
==__precursor lesion believed to arise in utero and stay dormant till puberty (may be hormone affected)__==
3. germ cell neoplasia in situ
4. reduplication of the short arm of chromosome 12 (isochromosome 12p)
progression to GCT in those with germ cell neoplasia in situ (eg. in those with cryptorchid testes) is ==__70%__== within 7 years of diagnosis
==__!! lesions retain the expression of OCT3/4 and NANOG (transcription factors)__==
85
New cards
when is germ cell neoplasia in situ found
in 90% of GCTs (except spermatocytic tumour and those that arise in infancy) and in testes at high risk for developing GCTs such as cryptorchid testes
86
New cards
cryptorchid testes are associated with…
GCTs
87
New cards
classification/types of GCTs
__**GCTs derived from germ cell neoplasia in situ:**__
1. seminomatous tumours:
* composed of cells that resemble primordial germ cells or early gonocytes
* most common (50% of all GCTs)
* peak incidence at 40
* its identical tumour in the ovaries = dysgerminoma, in the CNS = germinoma
* bulk masses, homogenous gray white lobulated cut surface, devoid of haemorrhage or necrosis
* tunica albuginea is usually not penetrated but it may occasionally extend to the epididymis, spermatic cord or scrotal sac
* sheets of uniform cells
* classic → round to polyhedral, distinct cell membrane, clear or watery cytoplasm, large central nucleus with 1 or 2 prominent nuclei
* ill defined granulomas may be found (host response)
* positive for KIT, OCT3/4 and podoplanin, negative for cytokeratin
2. nonseminomatous tumours:
* may be composed of undifferentiated cells that resemble embryonic stem cells but they can differentiate along other lineages
1. embryonal carcinoma:
* 20-30, more aggressive than seminomas, may be pure or admixed with other germ cell components
* locally aggressive, ==__frequently extend through the tunica albuginea__== into the epididymis or spermatic cord
* foci of haemorrhage or necrosis → variegated appearance
* alveolar or tubular pattern with papillary folds
* epithelial appearance, large and anaplastic, hyperchromatic nuclei with prominent nucleoli
* indistinct cell borders, variation in cell and nuclear size and shape, mitotic figures and tumour giant cells
* vascular lymphatic invasion is common
* stains positive for OCT3/4 like seminoma but is also positive for cytokeratin and negative for KIT and podoplanin
2. choriocarcinoma:
* highly malignant type of GCT
* serum hCG is elevated
* widespread metastasis often associated wit haemorrhage at sites of involvement may be seen
* small
* haemorrhage and necrosis are common
* composed of 2 cell types → syncytiotrophoblast and cytotrophoblasts
3. teratoma:
* refers to GCTs having various cellular or organoid components reminiscent of the normal derivates of more than one germ layer (including neural, muscle etc)
* may occur at any age
* second most common GCTs in children but rare in adults
* also ==__not__== associated with germ cell neoplasia in situ or isochromosome 12p
* in adults they are usually large
* teratoma with somatic type malignant transformation = when malignant non germ cell (somatic) tumours arise in postpubertal teratoma
* if prepubertal → GCT unrelated to GCN in situ
\
__**GCTs not derived from germ cell neoplasia in situ:**__
1. spermatocytic tumour:
* uncommon (1-2% of all testicular GCTs)
* not associated with germ cell neoplasia in situ
* affects older patients, >65
* slow growing, does not metastasise
* associated with a gain of ==__chromosome 9p__== not isochromosome 12p
* circumscribed, fleshy, myxoid sometimes with cystic regions
* contains 3 intermized cell populations:
1. medium sized cells, round nucleus, spireme type chromatic, occasional nucleoli, eosinophilic cytoplasm
2. small cells with dense chromatin, narrow rim of eosinophilic cytoplasm ==__resembling secondary spermatocytes__==
3. scattered giant cells, uni/multinucleate
* lacks inflammatory infiltrates and syncytiotrophoblasts, does not occur at extratesticular sites
2. yolk sac tumour (can also be of germ line origin if postpubertal):
* prepubertal = endodermal sinus tumour
most common testicular tumour in infants and children up to 3
‘pure’
* postpubertal → usually occurs in combination with embryonal carcinoma or other germ cell components
* lace like network of medium sized cuboidal, flattened or spindled cells which generally show less cytologic atypia than embryonal carcinoma
* papillary structures, solid cords of cells etc → different growth patterns
* ==__schiller duval bodies__== are seen in 50% → mesodermal core with a central capillary and a visceral and parietal layer of cells resembling primitive glomeruli
* eosinophilic hyaline like globules containing alpha fetoprotein and alpha antitrypsin → ==__typical__==
3. mixed tumours → about 60% of GCTs are mixed
1. seminomatous tumours:
* composed of cells that resemble primordial germ cells or early gonocytes
* most common (50% of all GCTs)
* peak incidence at 40
* its identical tumour in the ovaries = dysgerminoma, in the CNS = germinoma
* bulk masses, homogenous gray white lobulated cut surface, devoid of haemorrhage or necrosis
* tunica albuginea is usually not penetrated but it may occasionally extend to the epididymis, spermatic cord or scrotal sac
* sheets of uniform cells
* classic → round to polyhedral, distinct cell membrane, clear or watery cytoplasm, large central nucleus with 1 or 2 prominent nuclei
* ill defined granulomas may be found (host response)
* positive for KIT, OCT3/4 and podoplanin, negative for cytokeratin
2. nonseminomatous tumours:
* may be composed of undifferentiated cells that resemble embryonic stem cells but they can differentiate along other lineages
1. embryonal carcinoma:
* 20-30, more aggressive than seminomas, may be pure or admixed with other germ cell components
* locally aggressive, ==__frequently extend through the tunica albuginea__== into the epididymis or spermatic cord
* foci of haemorrhage or necrosis → variegated appearance
* alveolar or tubular pattern with papillary folds
* epithelial appearance, large and anaplastic, hyperchromatic nuclei with prominent nucleoli
* indistinct cell borders, variation in cell and nuclear size and shape, mitotic figures and tumour giant cells
* vascular lymphatic invasion is common
* stains positive for OCT3/4 like seminoma but is also positive for cytokeratin and negative for KIT and podoplanin
2. choriocarcinoma:
* highly malignant type of GCT
* serum hCG is elevated
* widespread metastasis often associated wit haemorrhage at sites of involvement may be seen
* small
* haemorrhage and necrosis are common
* composed of 2 cell types → syncytiotrophoblast and cytotrophoblasts
3. teratoma:
* refers to GCTs having various cellular or organoid components reminiscent of the normal derivates of more than one germ layer (including neural, muscle etc)
* may occur at any age
* second most common GCTs in children but rare in adults
* also ==__not__== associated with germ cell neoplasia in situ or isochromosome 12p
* in adults they are usually large
* teratoma with somatic type malignant transformation = when malignant non germ cell (somatic) tumours arise in postpubertal teratoma
* if prepubertal → GCT unrelated to GCN in situ
\
__**GCTs not derived from germ cell neoplasia in situ:**__
1. spermatocytic tumour:
* uncommon (1-2% of all testicular GCTs)
* not associated with germ cell neoplasia in situ
* affects older patients, >65
* slow growing, does not metastasise
* associated with a gain of ==__chromosome 9p__== not isochromosome 12p
* circumscribed, fleshy, myxoid sometimes with cystic regions
* contains 3 intermized cell populations:
1. medium sized cells, round nucleus, spireme type chromatic, occasional nucleoli, eosinophilic cytoplasm
2. small cells with dense chromatin, narrow rim of eosinophilic cytoplasm ==__resembling secondary spermatocytes__==
3. scattered giant cells, uni/multinucleate
* lacks inflammatory infiltrates and syncytiotrophoblasts, does not occur at extratesticular sites
2. yolk sac tumour (can also be of germ line origin if postpubertal):
* prepubertal = endodermal sinus tumour
most common testicular tumour in infants and children up to 3
‘pure’
* postpubertal → usually occurs in combination with embryonal carcinoma or other germ cell components
* lace like network of medium sized cuboidal, flattened or spindled cells which generally show less cytologic atypia than embryonal carcinoma
* papillary structures, solid cords of cells etc → different growth patterns
* ==__schiller duval bodies__== are seen in 50% → mesodermal core with a central capillary and a visceral and parietal layer of cells resembling primitive glomeruli
* eosinophilic hyaline like globules containing alpha fetoprotein and alpha antitrypsin → ==__typical__==
3. mixed tumours → about 60% of GCTs are mixed
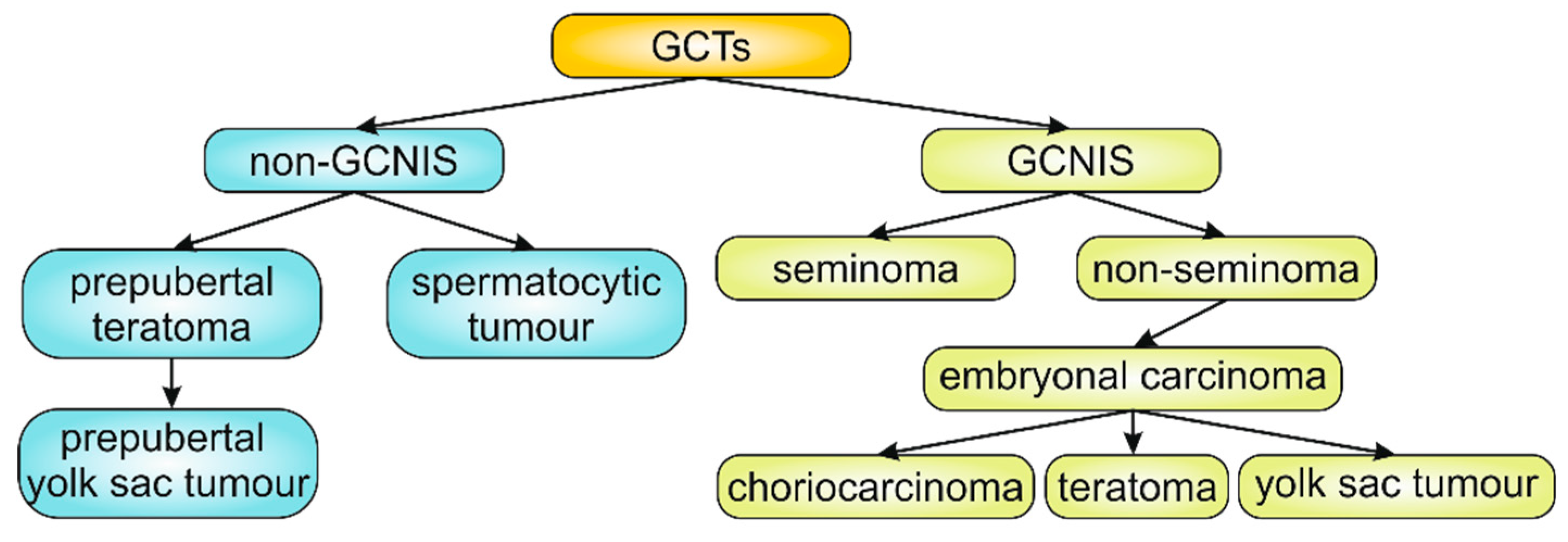
88
New cards
what differentiates spermatocytic tumours from seminomas
they lack inflammatory infiltrates and syncytiotrophoblasts
they do not occur at extratesticular sites
never admixed with other GCTs
they do not occur at extratesticular sites
never admixed with other GCTs
89
New cards
15% of seminomas have…
syncytiotrophoblasts
serum human chorionic gonadotropin levels are elevated
serum human chorionic gonadotropin levels are elevated
90
New cards
biopsy of a testicular neoplasm is associated with…
tumour spillage
91
New cards
spread of testicular tumours
lymphatic spread is common to all forms (retro peritoneal para aortic nodes seem to be the first usually then mediastinal and supraclavicular)
haematogenous spread is primarily to the lungs (others → liver, brain and bones)
haematogenous spread is primarily to the lungs (others → liver, brain and bones)
92
New cards
serum biomarkers in germ cell tumours
* GCTs secrete polypeptide hormones and enzymes such as hCG, AFP and lactate dehydrogenase
* levels of lactate dehydrogenase correlate with the size of the tumour
* yolk sac tumours have marked AFP
* syncytiotrophoblastic elements have marked hCG
* AFP and hCG are elevated in 80% of those with nonseminomatous GCTs
* levels of lactate dehydrogenase correlate with the size of the tumour
* yolk sac tumours have marked AFP
* syncytiotrophoblastic elements have marked hCG
* AFP and hCG are elevated in 80% of those with nonseminomatous GCTs
93
New cards
tumours of sex cord-gonadal stroma
* large size, necrosis, infiltrative borders, anaplasia, mitotic activity, vascular lymphatic invasion and extratesticular extension
1. leydig cell tumours:
* produce hormones? (andorgens etc?)
* most common presenting symptom = testicular swelling but gynecomastia may also be one
* associated with klinefelter syndrome, cryptorchidism and hereditary leiomyomatosis and renal cell carcinoma syndrome
* circumscribed nodules, golden brown homogenous appearance, large, round or polygonal cell outlines, abundant granular eosinophilic cytoplasm and a round central nucleus
* cytoplasm frequently contains lipid droplets, vacuoles or lipofuscin pigment
* most characteristic → ==__crystalloids of reinke__==
2. sertoli cell tumours:
* hormonally silent
* associated with carney complex, peutz jeghers syndrome and familial adenomatosis polyposis syndrome
* small firm nodules with a homogenous gray white to yellow surface cut
* tumour cells form trabeculae
1. leydig cell tumours:
* produce hormones? (andorgens etc?)
* most common presenting symptom = testicular swelling but gynecomastia may also be one
* associated with klinefelter syndrome, cryptorchidism and hereditary leiomyomatosis and renal cell carcinoma syndrome
* circumscribed nodules, golden brown homogenous appearance, large, round or polygonal cell outlines, abundant granular eosinophilic cytoplasm and a round central nucleus
* cytoplasm frequently contains lipid droplets, vacuoles or lipofuscin pigment
* most characteristic → ==__crystalloids of reinke__==
2. sertoli cell tumours:
* hormonally silent
* associated with carney complex, peutz jeghers syndrome and familial adenomatosis polyposis syndrome
* small firm nodules with a homogenous gray white to yellow surface cut
* tumour cells form trabeculae
94
New cards
gonadoblastoma, testicular lymphoma\*\*\*\*\*\*\*\*\*\*
95
New cards
lesions of tunica vaginalis
* tunica vaginalis = mesothelial lined surface exterior to the testis that may accumulate serous fluid (hydrocele)
* accumulation of blood = hematocele → uncommon
* chylocele = accumulation of lymph, almost always found in patients with elephantiasis who have widespread sever lymphatic obstruction
* spermatocele = small cystic accumulation of semen in dilated efferent ducts or ducts of the rete testis
* varicocele = a dilated vein in the spermatic cord
* accumulation of blood = hematocele → uncommon
* chylocele = accumulation of lymph, almost always found in patients with elephantiasis who have widespread sever lymphatic obstruction
* spermatocele = small cystic accumulation of semen in dilated efferent ducts or ducts of the rete testis
* varicocele = a dilated vein in the spermatic cord
96
New cards
prostate
* a retroperitoneal organ circling the neck of the bladder and urethra
* divided into 4 regions (peripheral, central, transition and periurethral)
* most hyperplasias occur in the transition zone while most carcinomas occur in the peripheral zone
* consists of glands separated by fibromuscular stroma
glands are lined by 2 cell layers → basal layer of low cuboidal basal epithelium covered by a layer of columnar secretory cells which often contain small papillary infoldings
* dihydrotestosterone is the main androgen in the prostate where it is formed from testosterone through the action of type 2 5alpha-reductase
* type 2 5alpha-reductase is expressed mainly on stromal cells and not prostatic epithelial cells
* type 1 5alpha-reductase mediates DHT production from testosterone in extraprostatic locations → extra DHT for the prostate
* it binds to and activates androgen receptors in both stromal and epithelial prostate cells → more potent that testosterone because it has a higher affinity for ARs and forms a more stable complex
* DHT x AR → ARs translocate from the cytoplasm to the nucleus → activate transcription of androgen dependent genes which encode growth factors (mainly FGF and TGF beta)
* divided into 4 regions (peripheral, central, transition and periurethral)
* most hyperplasias occur in the transition zone while most carcinomas occur in the peripheral zone
* consists of glands separated by fibromuscular stroma
glands are lined by 2 cell layers → basal layer of low cuboidal basal epithelium covered by a layer of columnar secretory cells which often contain small papillary infoldings
* dihydrotestosterone is the main androgen in the prostate where it is formed from testosterone through the action of type 2 5alpha-reductase
* type 2 5alpha-reductase is expressed mainly on stromal cells and not prostatic epithelial cells
* type 1 5alpha-reductase mediates DHT production from testosterone in extraprostatic locations → extra DHT for the prostate
* it binds to and activates androgen receptors in both stromal and epithelial prostate cells → more potent that testosterone because it has a higher affinity for ARs and forms a more stable complex
* DHT x AR → ARs translocate from the cytoplasm to the nucleus → activate transcription of androgen dependent genes which encode growth factors (mainly FGF and TGF beta)
97
New cards
prostatitis
divided into several categories
1. acute bacterial prostatitis:
* usually the same bacteria that cause UTIs (so mostly E.coli)
* organisms usually reach the prostate through reflux but occasionally distant foci of infection seed the prostate through lymphohematogenous routes
* sometimes follows surgical manipulation
* fever, chills and dysuria, on rectal examination it is very tender
* ==__biopsy is contraindicated since it may lead to sepsis__==
2. chronic bacterial prostatitis:
* presents with low back pain, dysuria and perineal and suprapubic discomfort though it may also be asymptomatic
* often a history of UTIs caused by the same organism
* ==__antibiotics penetrate the prostate poorly__==
* diagnosis depends on leukocytosis in expressed prostatic secretion and positive bacterial cultures
3. chronic abacterial prostatitis:
* most common form of prostatitis
* also called ==__chronic pelvic pain syndrome__==
* indistinguishable from ^ except that there is no history of recurrent UTIs
4. granulomatous prostatitis:
* may be caused by a specific infectious agent or may refer to a pattern of tissue reaction to noninfectious stimuli
* most common cause is instillation of BCG for treatment of bladder cancer in which case it requires no treatment
* fungal granulomatous prostatitis is usually seen in the immunocompromised
5. others: adenoviral and IgG4 associated autoimmune prostatitis
1. acute bacterial prostatitis:
* usually the same bacteria that cause UTIs (so mostly E.coli)
* organisms usually reach the prostate through reflux but occasionally distant foci of infection seed the prostate through lymphohematogenous routes
* sometimes follows surgical manipulation
* fever, chills and dysuria, on rectal examination it is very tender
* ==__biopsy is contraindicated since it may lead to sepsis__==
2. chronic bacterial prostatitis:
* presents with low back pain, dysuria and perineal and suprapubic discomfort though it may also be asymptomatic
* often a history of UTIs caused by the same organism
* ==__antibiotics penetrate the prostate poorly__==
* diagnosis depends on leukocytosis in expressed prostatic secretion and positive bacterial cultures
3. chronic abacterial prostatitis:
* most common form of prostatitis
* also called ==__chronic pelvic pain syndrome__==
* indistinguishable from ^ except that there is no history of recurrent UTIs
4. granulomatous prostatitis:
* may be caused by a specific infectious agent or may refer to a pattern of tissue reaction to noninfectious stimuli
* most common cause is instillation of BCG for treatment of bladder cancer in which case it requires no treatment
* fungal granulomatous prostatitis is usually seen in the immunocompromised
5. others: adenoviral and IgG4 associated autoimmune prostatitis
98
New cards
benign prostatic hyperplasia/nodular hyperplasia
* most common benign prostatic disease in men >50
* histologic evidence of BPH is found in up to 90% of men by age 80
* it is not a premalignant lesion
* affects the transition zone, hyperplastic nodules
individual nodules contain cystically dilated glands that are separated by spindle shaped stromal cells
* main symptoms are due to urinary obstruction caused by prostatic enlargement and stromal smooth muscle mediated contraction
* resitance to urine outflow → bladder hypertrophy and distention + urine retention (may cause infections)
* may be caused by DHT induced growth factors increasing the proliferation of stromal cells and decreasing the death of epithelial cells
* androgens play a permissive role in BPH pathogenesis but oestrogen also has a role → tips the balance towards proliferation
* ERalpha receptors have a proliferative effect
* ERbeta receptors have an antiproliferative effect
* treatment: alpha adrenergic blockers (decreases prostate smooth muscle tone) and 5alpha reductase inhibitors (shrinks the prostate)
* histologic evidence of BPH is found in up to 90% of men by age 80
* it is not a premalignant lesion
* affects the transition zone, hyperplastic nodules
individual nodules contain cystically dilated glands that are separated by spindle shaped stromal cells
* main symptoms are due to urinary obstruction caused by prostatic enlargement and stromal smooth muscle mediated contraction
* resitance to urine outflow → bladder hypertrophy and distention + urine retention (may cause infections)
* may be caused by DHT induced growth factors increasing the proliferation of stromal cells and decreasing the death of epithelial cells
* androgens play a permissive role in BPH pathogenesis but oestrogen also has a role → tips the balance towards proliferation
* ERalpha receptors have a proliferative effect
* ERbeta receptors have an antiproliferative effect
* treatment: alpha adrenergic blockers (decreases prostate smooth muscle tone) and 5alpha reductase inhibitors (shrinks the prostate)
99
New cards
prostate neoplasms
* prostate cancer is the 2nd cause of cancer related death in men
* risk increases from 20% in their 50s to 70% in their 70-80s
* most common mutation = TMPRSS-ETS fusion gene (50%)
others → silencing of p27, amplification of MYC, deletion of PTEN
* in late stage disease, p53 and RB mutations are common
* ==__other mutations? GSTP1? BRCA2, HOXB13__==
* %%__alpha methylacyl coenzyme A racemase__%% is upregulated
* growth and survival are dependent on androgens but most tumours become resistant to androgen blocking by:
* acquisition of hypersensitivity to low levels of androgen (eg. through AR gene amplification)
* ligand independent AR activation
* mutations in AR that allow it to be activated by non androgen ligands
* haematogenous spread occurs mainly to the bones
* usually asymptomatic if it is localised, discovered by accident in a rectal exam or by elevated serum %%__prostate specific antigen__%%
\
* around 80% have ==__prostatic intraepithelial neoplasia__== (= precursor lesion)
1. adenocarcinoma:
* most common form of cancer in men
* the glands are typically smaller than benign glands and are lined by a single uniform layer of cuboidal or low columnar epithelium
* malignant glands do not have the outer basal layer and they are more tightly packed (compared to benign glands)
\
* most common treatment is radical prostatectomy, if not eligible → RT
if metastasised → androgen deprivation usually by orchiectomy or administration of synthetic analogues of LHRH which desensitises pituitary cells expressing LHRH receptors → %%__suppresses the release of LH which is required for testosterone production by leydig cells__%%
* however most become resistant to testosterone withdrawal
* risk increases from 20% in their 50s to 70% in their 70-80s
* most common mutation = TMPRSS-ETS fusion gene (50%)
others → silencing of p27, amplification of MYC, deletion of PTEN
* in late stage disease, p53 and RB mutations are common
* ==__other mutations? GSTP1? BRCA2, HOXB13__==
* %%__alpha methylacyl coenzyme A racemase__%% is upregulated
* growth and survival are dependent on androgens but most tumours become resistant to androgen blocking by:
* acquisition of hypersensitivity to low levels of androgen (eg. through AR gene amplification)
* ligand independent AR activation
* mutations in AR that allow it to be activated by non androgen ligands
* haematogenous spread occurs mainly to the bones
* usually asymptomatic if it is localised, discovered by accident in a rectal exam or by elevated serum %%__prostate specific antigen__%%
\
* around 80% have ==__prostatic intraepithelial neoplasia__== (= precursor lesion)
1. adenocarcinoma:
* most common form of cancer in men
* the glands are typically smaller than benign glands and are lined by a single uniform layer of cuboidal or low columnar epithelium
* malignant glands do not have the outer basal layer and they are more tightly packed (compared to benign glands)
\
* most common treatment is radical prostatectomy, if not eligible → RT
if metastasised → androgen deprivation usually by orchiectomy or administration of synthetic analogues of LHRH which desensitises pituitary cells expressing LHRH receptors → %%__suppresses the release of LH which is required for testosterone production by leydig cells__%%
* however most become resistant to testosterone withdrawal
100
New cards
prostate cancer grading