Depression
1/36
Earn XP
Description and Tags
PEBC
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
depression
state of low mood that can affect emotional, physical, cognitive and behavioural well-being
persistent depressive disorder
≥2 yrs, a person has experienced a depressed mood more days than not PLUS ≥2 of the following:
appetite loss or overeating (changes in appetite)
sleep disturbances
low energy/ fatigue
low self-esteem
hopelessness
poor concentration or indecisiveness
major depressive disorder
≥5 of the following sx for at least 2 weeks; at least 1 must be depressed mood or loss of interest/ pleasure:
depressed mood
markedly reduced interest or pleasure in all activities
appetite loss or overeating
sleep disturbances
low energy/ fatigue
agitation or psychomotor retardation
feeling worthless or excessive/ inappropriate guilt
poor concentration
recurrent thoughts of death
medications:
takes at least 2-4 weeks to show any effect and 6-8 weeks for Full effect
clinical presentation
SADAFACES
Sleep changes
Anhedonia (reduced ability to experience pleasure)
Depressed mood
Appetite disturbance
Fatigue
Agitation (psychomotor) or psychomotor retardation
Concentration (diminished)
Esteem (low)
Suicidal ideation
PHQ9 scale
self administered screening tool for depression
MDD suggested if of the 9 items, 5+ are checked as at least “more than half the days”
either item 1 or 2 is checked as at least “more than half the days”
risk factors (depression)
Non-modifable:
Females (males catch up later in life)
Family history (1st degree)
Hx of adverse childhood experiences, traumatic life events, death of spouse
age 25-44
Potentially modifiable:
Chronic medical conditions and psychiatric comorbidities (DM, CVD, Anxiety, Chronic pain)
Alcohol and substance use disorders
Periods of hormonal changes
Significant life stressors
Bereavement
Environmental/ lifestyle factors
risk factors (suicide)
comorbid conditions:
PTSD
Substance use disorder (of family hx)
Comorbid personality disorders
Sleep disorders, chronic pain conditions
life events:
suicidal ideation, prior attempts
hopelessness, anxiety, impulsivity, psychosis
significant life stressors
increasing age, being widowed or unmarried
unemployed or living alone
anniversary of a loss
ethnicity - First Nations
Females = more prone to OD
drug induced causes
Antipsychotics
Anticonvulsants (levetiracetam, phenobarbital, primodine, phenytoin, tigabine, topiramate, vigabatrin)
Corticosteroids
Parkinsons disease drugs
Isotretinoin
Sex hormones (oral contraceptives, Tamoxifen, GnRH agonists)
stimulants
others:
anti-virals
Beta blockers
calcium channel blockers
clonidine
interferon alpha/beta
methyldopa
PPIs
H2RAs
Reserpine
sex hormones
statins
triptans
varenicline
goals of therapy
attain relief from depressive sx
treat concurrent sx/ disorders w minimal side effects
restore optimal functioning and QoL
prevent suicide
prevent future episodes
non pharm
Psychoeducation and self-management
as effective as drug therapy and preferred over meds
moderate MDD = choice btwn meds and/or psychotherapy
severe MDD = combo of meds and psychotherapy
most evidence = CBT, IPT and BA
psychotherapy combined with pharmacotherapy = more effective than either alone
Regular exercise (aerobic and resistance)
proven to prevent and treat depression (low intensity 30-40 mins 3-4x weekly min 9 weeks)
1st line monotherapy in mild depression
2nd line adjunct in moderate depression
ECT (electroconvulsive therapy)
1st line in severe and life threatening situations
Light therapy
1st line monotherapy in seasonal pattern MDD - improve in 1-3 weeks
2nd line for mild depression non-seasonal
algorithm
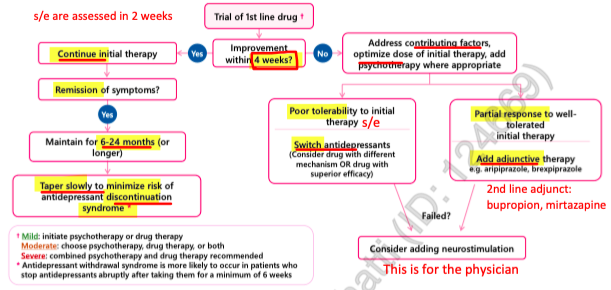
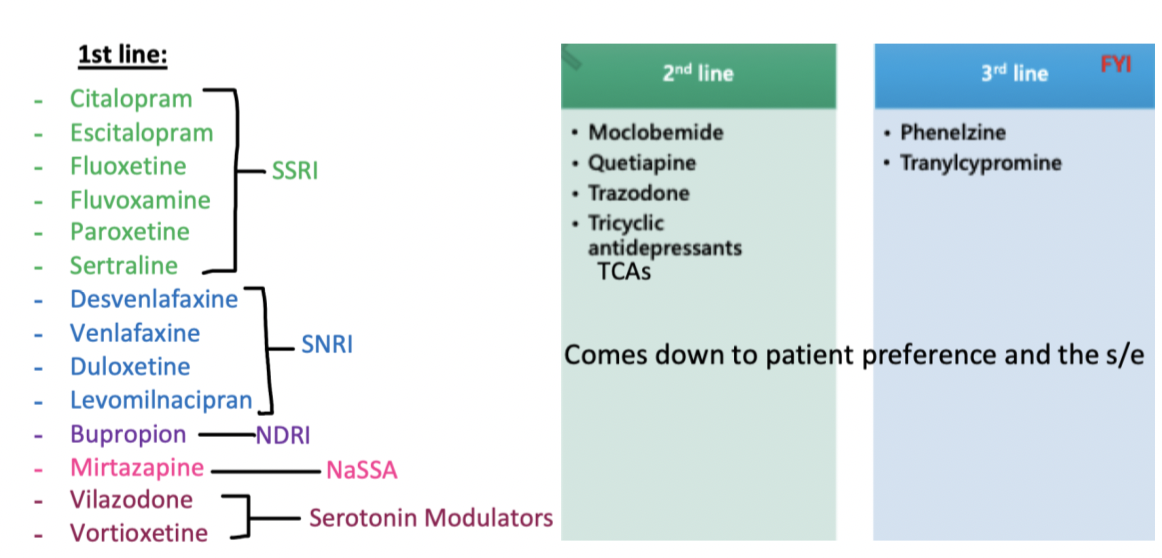
treatment options
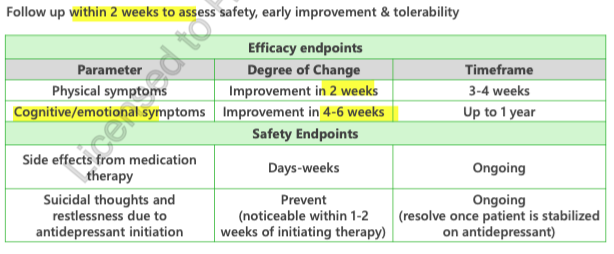
follow up within 2 weeks of starting anti-depressant
duration of therapy
acute phase (8-16 weeks until sx remission)
address pt safety
treat to sx remission and functional improvement
prevent suicide
overall = resolution of sx
maintenance (6-24 months) or longer
maintain remission
restore functioning
prevent recurrence
DC treatment when clinically indicated
all pts should be treated for 6-12 months after remission
treatment should be continued for ≥2 yrs if ANY of following RF for recurrence are present:
persistent residual sx (anhedonia, sleep problems, cognitive dysfunction)
Hx of childhood abuse
increased severity of depressive sx
chronic depressive episodes
psychiatric or non-psychiatric comorbidities
increase number of previous episodes (3+)
poor social support
persistent life events
8-16 weeks
duration of therapy for the acute phase
address patient safety
treat symptom remission and functional improvement
prevent suicide
6-24 months
duration of therapy for the Maintenance phase!
can be longer if clinically indicated
maintain symptomatic remission
restore functioning
prevent recurrence
discontinue treatment when clinically indicated
6-12 months
duration of therapy after remission
2+ years
duration of treatment when any of the following risk factors for recurrence are present:
persistent residual symptoms (anhedonia, sleep problems, cognitive dysfunction)
history of childhood abuse
increased severity of depressive episodes
chronic depressive episodes
psychiatric or nonpsychiatric comorbidities
increased # of previous episodes (3+ episodes)
poor social support
persistent life events
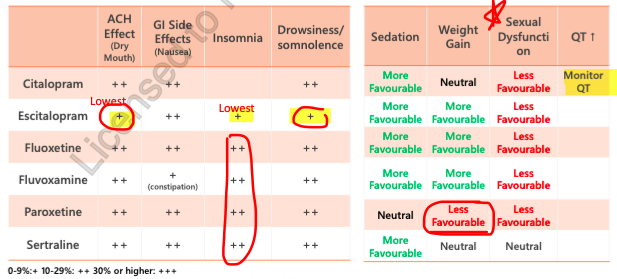
SSRI
Escitalopram, Citalopram, Fluoxetine, Fluvoxamine, Paroxetine, Sertraline
time to onset = 2-4 weeks
start low and titrate up gradually
fluoxetine = drug of choice in CHILDREN
lots of nausea
fluoxi-teen = for teens and kids
Combining with NSAIDs = increased GI Bleed risk
combining with diuretics = hyponatremia (esp in elderly)
most anticholinergic = Paroxetine
weight gain with paroxetine
s/e = HA, dizziness, anxiety/agitation (esp in first 1-2 weeks), Nausea, sleep disturbance, Sexual dysfunction
escitalopram and citalopram = QTc prolonging
Concurrent use with MAOIs, linezolid and methylene blue is contraindicated due to increased risk of serotonin syndrome.
SNRI
Venlafaxine, Desvenlafaxine, Duloxetine, Levomilnacipran
time to onset = 2-4 weeks
Duloxetine = benefits for comorbid pain; associated with drug induced liver injury
Desvenlafaxine = low incidence sexual dysfunction
s/e = tremor, agitation, sweating, palpitations, nausea, HA, insomnia, sexual dysfunction, hyponatremia, anticholinergic
Venlafaxine = Dose-related hypertension occurs rarely, particularly at doses ≥225 mg/day
Bupropion
Low incidence of sexual dysfunction!!! use this is pt is experiencing sexual dysfunction from other options
no weight gain
may increase anxiety
s/e = stimulating: agitation, insomnia, tremor, increase HR/BP, decrease appetite, decrease weight
lowers seizure threshold
C/I= Sz disorders, recent Hx of anorexia or bullimia
alcohol use can also lower Sz threshold
drug induced liver injury
caution: crcl <30, hepatic impairment
mirtazapine
high rate of drowsiness and weight gain, increase appetite and long term metabolic risks
low incidence of sexual dysfucntion
s/e = dry mouth, wt gain, increased appetite, drowsiness, edema, arthralgia, dizziness
trazodone
very sedating! and rarely tolerated at therapeutic doses
used as a sedative
no tolerance
s/e = sedation, decreased BP, dizziness, HA, priapism, increased QTc
vortioxetine
low incidence of sexual dysfunction
s/e = well tolerated, nausea, decreased sexual dysfunction
long half life
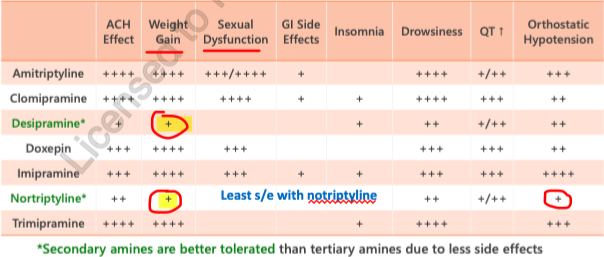
TCAs
Amitriptyline, Nortriptyline, Clomipramine, Desipramine, Impiramine, doxepin
2nd line
time to onset = 2-4 weeks
LOTS OF SE = sedation, decreased BP, dizziness, sexual dysfunction, sweating, tremor, anticholinergic, increased wt,
increased HR, QTc, ECG changes
AVOID in pts with hx of overdose due to risk of cardiotoxicity, altered mental status and seizures
MAOIs
Phenelzine, Tranylcypromine, Moclobemide (use this and avoid the others)
associated with potentially fatal food interactions: hypertensive crisis when using tyramine rich food = cured meats, mature cheese, fermented products (miso, kimchi)
interactions = dextromethorphan, SSRIs, St johns wort
s/e = dry mouth, insomnia, HA, nausea, decreased sexual dysfunction
highest risk of serotonin syndrome with irreversible MAOIs = Phenelzine and Tranylcypromine
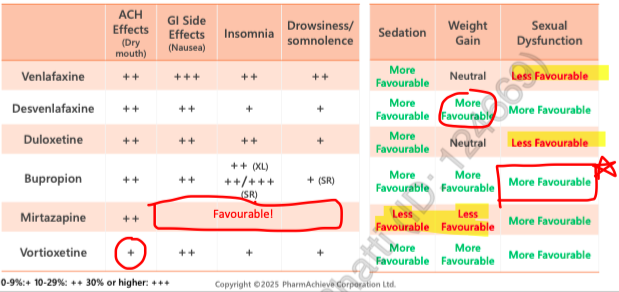
SSRI side effects
SNRI side effects
TCA side effects
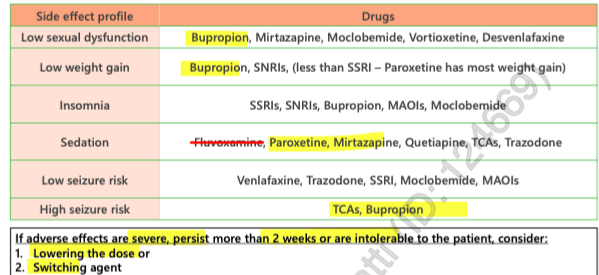
overview of side effects
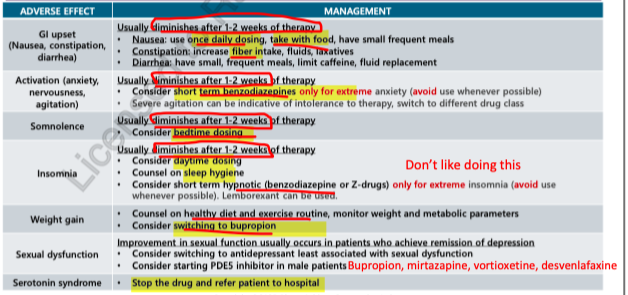
side effect management
serotonin syndrome
SHIVERS
Shivering
Hyperreflexia
Increased temperature
Vital signs unstable (Increased HR, RR, Low BP)
Encephalopathy (confused, altered mental status)
Restlessness
Sweating
when theres too much serotonin in body
when multiple serotonergic agents used concomitantly
AVOID when using other serotonergic agents:
linezolid, MAOIs, dye methylene blue
DC offending agents immediately! go to ER
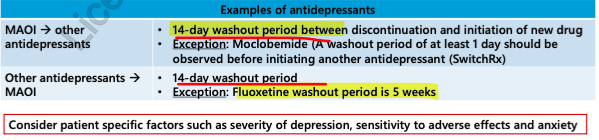
switching antidepressants
direct switch = stop 1st agent abruptly and start new antidepressant next day
Taper and switch immediately = gradually taper 1st agent and then start the new agent immediately after discontinuation ←- best way
taper and switch after washout = gradually withdraw 1st, then start new after washout period (depends on half life of 1st drug)
cross taper = taper the first (over 1-2 weeks or longer) and build up the dose of the new agent simultaneously
withdrawal/ discontinuation syndrome
rapid or abrupt d/c or dose reduction of most antidepressants may be associated with discontinuation syndrome —> esp if taken 6 weeks or more
FINISH
Flu-like sx
Insomnia
Nausea
Imbalance
Sensory changes
Hyperarousal
usually lasts 3 days - 3 weeks
can be prevented by counselling patients to not stop drug abruptly
resolve w/in 48 hr if SSRI/SNRI re-introduced
highest risk = paroxetine and venlafaxine bc they have short t1/2
bupropion doesnt cause withdrawal
fluoxetine = lowest incidence of withdrawal due to long half-life
pregnancy and breastfeeding
psychotherapy = 1st line
pharmacotherapy given if:
severe sx
high risk of relapse
unable to access or have inadequate response to psychotherapy
prefer to use meds
1st line:
citalopram, escitalopram, sertraline
2nd line:
bupropion, desvenlafaxine, venlafaxine, fluoxetine, fluvoxaine, duloxetine, mirtazapine
3rd line:
TCA, trazadone, Quetiapine
avoid paroxetine in pregnancy = cardiovascular malformations
AVOID DOXEPIN in breastfeeding = sedation in infant
st johns wort
mild depression = 1st line
moderate depression = 2nd line
potent inducer of CYP3A4 and P-gp = decrease bioavailability of many drugs
acupuncture
mild depression = 2nd line monotherapy
moderate - severe = 2nd line adjunct
monitoring