621 unit 1 LOs Lec 1-2
5.0(1)
Card Sorting
1/36
Earn XP
Description and Tags
Last updated 12:43 AM on 2/3/23
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
37 Terms
1
New cards
Pharmacokinetics
the relationship between drug input (dose, dosage, frequency) and how the concentration of drug changes with time
2
New cards
Pharmacodynamics
the relationship between concentration at an active site & effects with time on the body
3
New cards
Systemic Absorption
the process by which unchanged drug proceeds from the site of administration to site of measurement
4
New cards
Distribution
Process of reversible transfer of the drug to and from the site of measurement and the peripheral tissues.
5
New cards
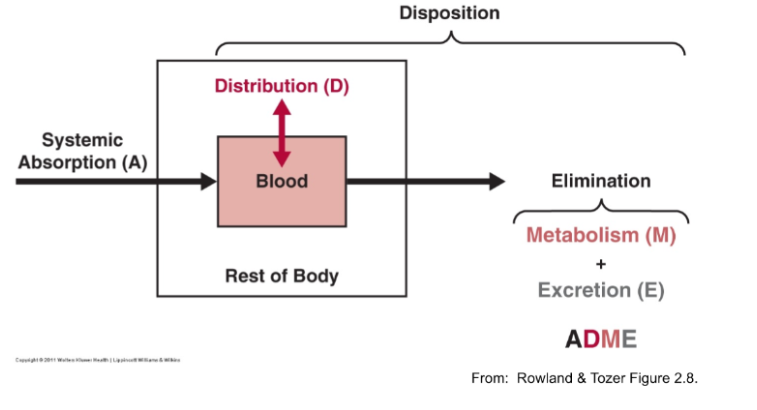
Disposition
sum of all kinetic processes that occur to a drug after systemic absorption
•elimination and distribution
•elimination and distribution
6
New cards
ADME
**A**bsorption **D**istribution **M**etabolism **E**xcretion
7
New cards
Therapeutic Window
• Exposure high enough to get desired response from drug but not too high to cause adverse effects
8
New cards
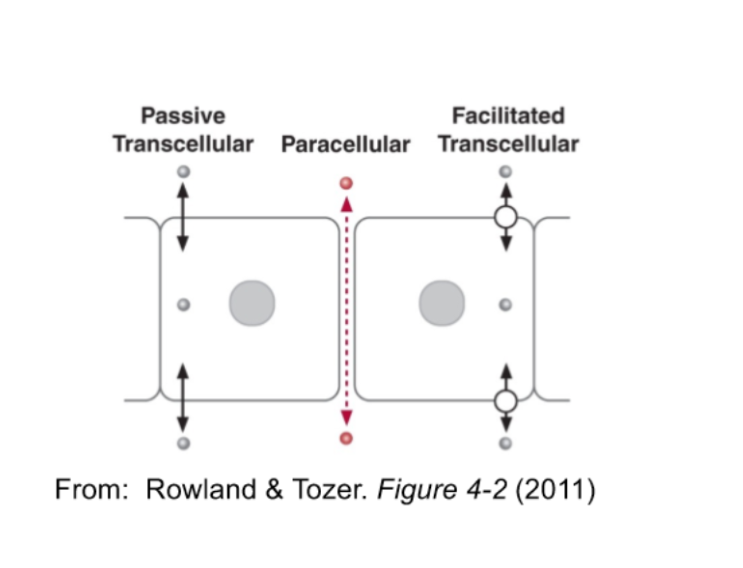
Transcellular vs Paracellular Transport
Trans: transport **through** a cell membrane
\
Para: Transport between cells
\
Para: Transport between cells
9
New cards
Intravascular Dosing
Drug is placed directly in the **blood**. Ex; intra venous
1)Distribution from blood to tissue across capillary membrane
2)Hepatic Elimination (metabolism) - transfer from blood to intracellular compartment of hepatocytes
3) Renal elimination (excretion)
1)Distribution from blood to tissue across capillary membrane
2)Hepatic Elimination (metabolism) - transfer from blood to intracellular compartment of hepatocytes
3) Renal elimination (excretion)
10
New cards
Extravascular Dosing
same steps as intra w addition of absorption step from admin site to blood
11
New cards
Systemic pathways for Extravascular dosing
oral, intramuscular, subcutaneous, sublingual, buccal, dermal, pulomnary, rectal
12
New cards
Regional pathways for Extravascular dosing
ventricular delivery to brain, pleural delivery to the lungs, peritoneal delivery to abdomen
13
New cards
Passive Diffusion
(most drugs)
molecules transfer from regions of high to low concentrations
molecules transfer from regions of high to low concentrations
14
New cards
Passive Facilitated Diffusion
Movement across the membrane facilitated by a transporter
15
New cards
Active transport
Can move drugs against an opposing gradient, The direction of movement can be either **influx (into the cell) or efflux (out of the cell)**
16
New cards
Which types of diffusion follow the concentration gradient
Passive & Facilitated
17
New cards
Which types of diffusion are structure specific
Facilitated & Active because of the transporters
18
New cards
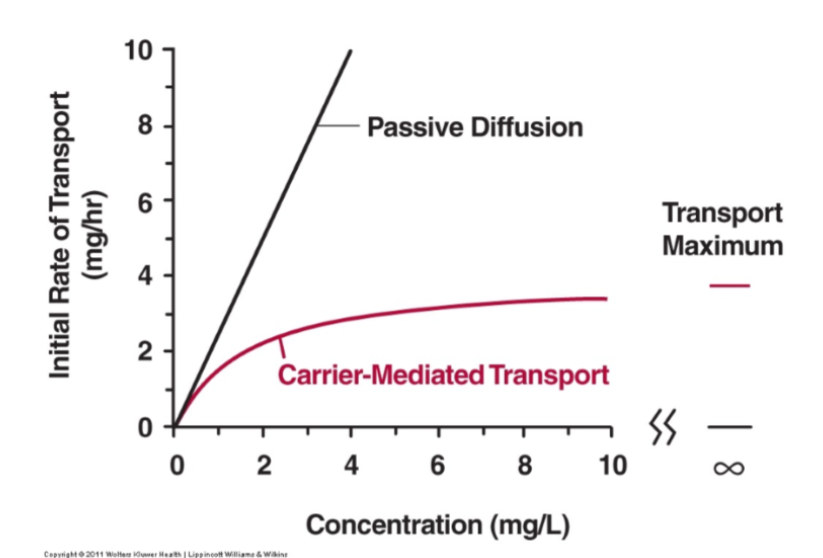
Which types of diffusion have saturable transport
Facilitated & Active because of the transporters
19
New cards
Which types of diffusion can be inhibited by structurally related compounds
Facilitated & Active because of the transporters
20
New cards
Which types of diffusion require energy
Active transport
21
New cards
Which types of diffusion can be inhibited by metabolic poisons
Active transport
\
Because active transport mechanisms depend on cellular metabolism for energy, they are sensitive to many metabolic poisons that interfere with the supply of ATP
\
Because active transport mechanisms depend on cellular metabolism for energy, they are sensitive to many metabolic poisons that interfere with the supply of ATP
22
New cards
What types of diffusion can go from lower to higher concentrations
Active transport
23
New cards
What does the transport maximum look like graphically
24
New cards
What factors affect drug transport across a membrane barrier
1. Molecular Size
2. Lipophilicity
3. Degree of protein binding
4. Charge (degree of ionization)
25
New cards
Ficks First Law
Rate= \[ (D K SA)/ h\] (Cside1-Cside2)
amount/time
D= diffusion coef
K= lipid/water partition coef
SA= Surface area (cm^2)
h= membrane thickness
c= drug concern on each side
\
Describes the passage of drugs through membranes by Diffusion
amount/time
D= diffusion coef
K= lipid/water partition coef
SA= Surface area (cm^2)
h= membrane thickness
c= drug concern on each side
\
Describes the passage of drugs through membranes by Diffusion
![Rate= \[ (D K SA)/ h\] (Cside1-Cside2)
amount/time
D= diffusion coef
K= lipid/water partition coef
SA= Surface area (cm^2)
h= membrane thickness
c= drug concern on each side
\
Describes the passage of drugs through membranes by Diffusion](https://knowt-user-attachments.s3.amazonaws.com/c544a30c87dd4199b8c6d56c25b4855d.jpeg)
26
New cards
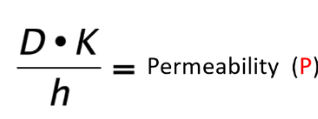
Permeability
(D \* K)/ h = P in distance/time
\
expression of ease of membrane penetration
\
expression of ease of membrane penetration
27
New cards
Diffusion Coefficient D (Stokes Einstein)
D= ( R \* T) / (6 \* N \* pi \* r \*n)
R= gas constant
N= avogadro number
r= radius
n= viscosity
R= gas constant
N= avogadro number
r= radius
n= viscosity
28
New cards
As the membrane SA increases the rate of absorption….
increases
29
New cards
As the functional membrane height increases the rate of absorption….
decreases
30
New cards
As the lipid water partition coefficient increases the rate of absorption…
increases
31
New cards
As molecular size increases, the rate of absorption…
decreases
32
New cards
As concentration on side 1 increases, the rate of absorption…
increases
33
New cards
As viscosity increases, the rate of absorption …
decreases
34
New cards
Cite active transport example of particularly p-glycoprotein
Active transporters play major roles in removing drug metabolites and foreign substances from cells and tissues
\n
EX: Tumor resistance to specific anticancer drugs
\n
•MDR1 was found to efflux many drugs that had entrees cancer cells, P-glycoprotein was found to be responsible, it is located in many organs and tissues and plays a big role in the hepatic secretion of many drugs into bile
\n
•P-gp recognizes hundreds of compounds, it works as a **hydrophobic vacuum cleaner**, pulls substances from the lipid bilayer, expelling them to promote multi drug resistance
\
\n
EX: Tumor resistance to specific anticancer drugs
\n
•MDR1 was found to efflux many drugs that had entrees cancer cells, P-glycoprotein was found to be responsible, it is located in many organs and tissues and plays a big role in the hepatic secretion of many drugs into bile
\n
•P-gp recognizes hundreds of compounds, it works as a **hydrophobic vacuum cleaner**, pulls substances from the lipid bilayer, expelling them to promote multi drug resistance
\
35
New cards
Protein binding- lipophilic drugs
•Only unbound, nonpolar drugs are able to cross lipid membranes
**•Unbound concentration provides the driving force for drug transport**
•At distribution equilibrium, Unbound drug concentration will be equal on both sides of the membrane
**•Unbound concentration provides the driving force for drug transport**
•At distribution equilibrium, Unbound drug concentration will be equal on both sides of the membrane
36
New cards
Degree of Ionization
•pH partition hypothesis: only un ionized nonpolar drugs are able to cross lipid membranes
•pH partition hypothesis applies @ equilibrium- used to predict the influence of pH on the rates of absorption and distribution
\n
*For 2 drugs with equal lipophilicity/molecular size/ protein binding that are not subject to carrier-mediated transport, t****he drug which is more unionized at a given pH will nearly always exhibit a faster rate of penetration across the membrane***
•pH partition hypothesis applies @ equilibrium- used to predict the influence of pH on the rates of absorption and distribution
\n
*For 2 drugs with equal lipophilicity/molecular size/ protein binding that are not subject to carrier-mediated transport, t****he drug which is more unionized at a given pH will nearly always exhibit a faster rate of penetration across the membrane***
37
New cards
Henderson Hasselbalch equation
pH= pka + log \[unpronotated / protonated\]