The Shoulder and Scapula
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
42 Terms
Shoulder Joint
glenohumeral joint; very mobile
Sternum
sterno-clavicular joint (only bony attachment of girdle to torso)
Scapula
-spine of scapula
-acromium process (most lateral)
-coracoid process (anterior)
-glenoid fossa (shoulder socket), almost flat; has glenoid labrum that will deform with stress; good for mobility but can tear
-does not attach to ribs or back; floating on the ribcage; supported by muscles
Humerus
head of the humerus- small; does not fit tight within the glenoid fossa
Bones of the Shoulder Girdle
sternum, clavicle, scapula, humerus
Possible Actions of the Scapula
-elevation
-depression
-abduction (protraction)
-adduction (retraction)
-upward rotation
-downward rotation
-forward tilt
-return from forward tilt
Possible Actions of the Shoulder
-Sagittal Plane: flexion (180 degrees to your ear), extension (to 0 degrees), hyperextension (about 45 degrees)
-Frontal Plane: abduction (180 degrees but must outwardly rotate humerus to not hit acromion), adduction (movement of arm to your side)
-Transverse Plane: inward (internal) rotation (60-80 degrees), outward (external) rotation (80-90 degrees)
-Combination: horizontal flexion (flexion + aDDuction), horizontal extension (extension + aBDuction)
Scapulohumeral Rhythm
-shoulder and scapular movement are “integrally tied” to each other; one affects the other
-to obtain full range in shoulder movement the scapulae also most move
Rules of Association
-when the humerus is more than 2-3 degrees away from a position of extension, the scapula is upwardly rotated, except then the shoulder joint is hyperextended and adducted, the scapula is downwardly rotated
-when the humerus is anterior to the frontal plane bisecting the shoulder joint, the scapula is abducted
-when the humerus is posterior to the frontal plane bisecting the shoulder joint, the scapula is adducted
-when the shoulder is hyperextended, with inward rotation, the scapula is forward tilted
-ALWAYS ANALYZE THE SHOULDER ACTIONS FIRST TO APPLY THE RULES OF ASSOCIATION!
Muscles of the Scapula
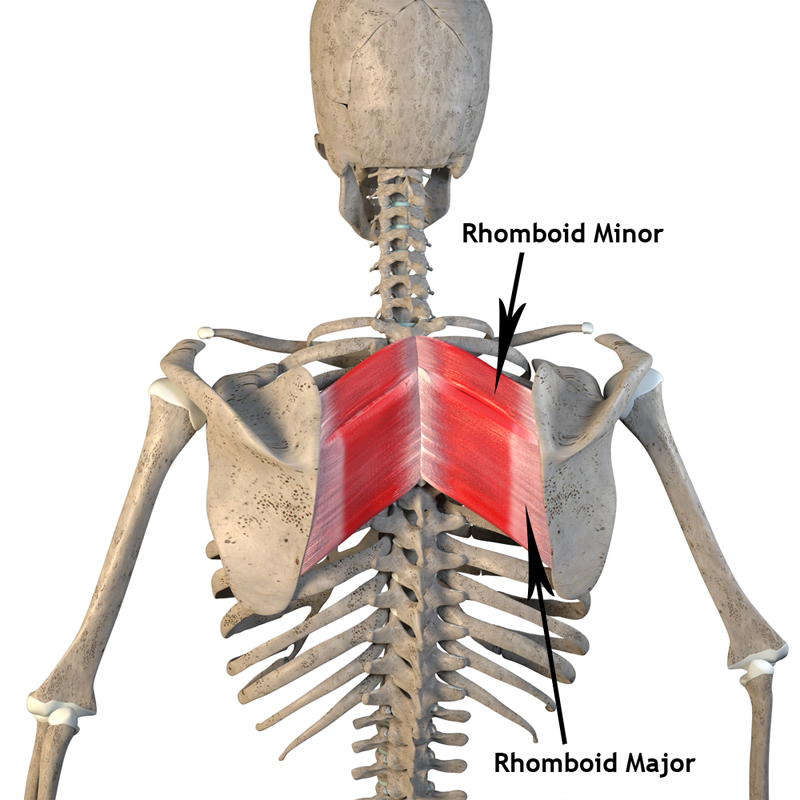
-rhomboids: major/minor
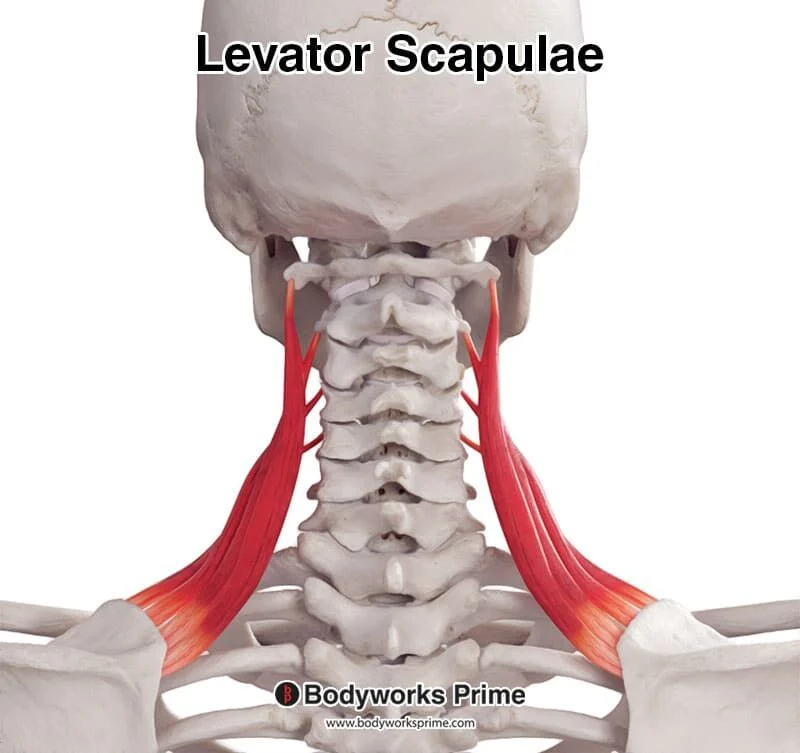
-levator scapulae
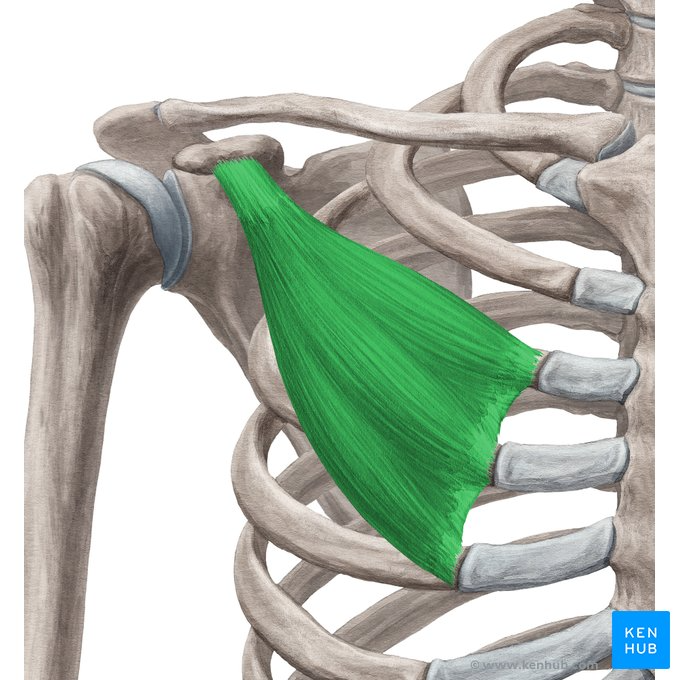
-pectoralis minor
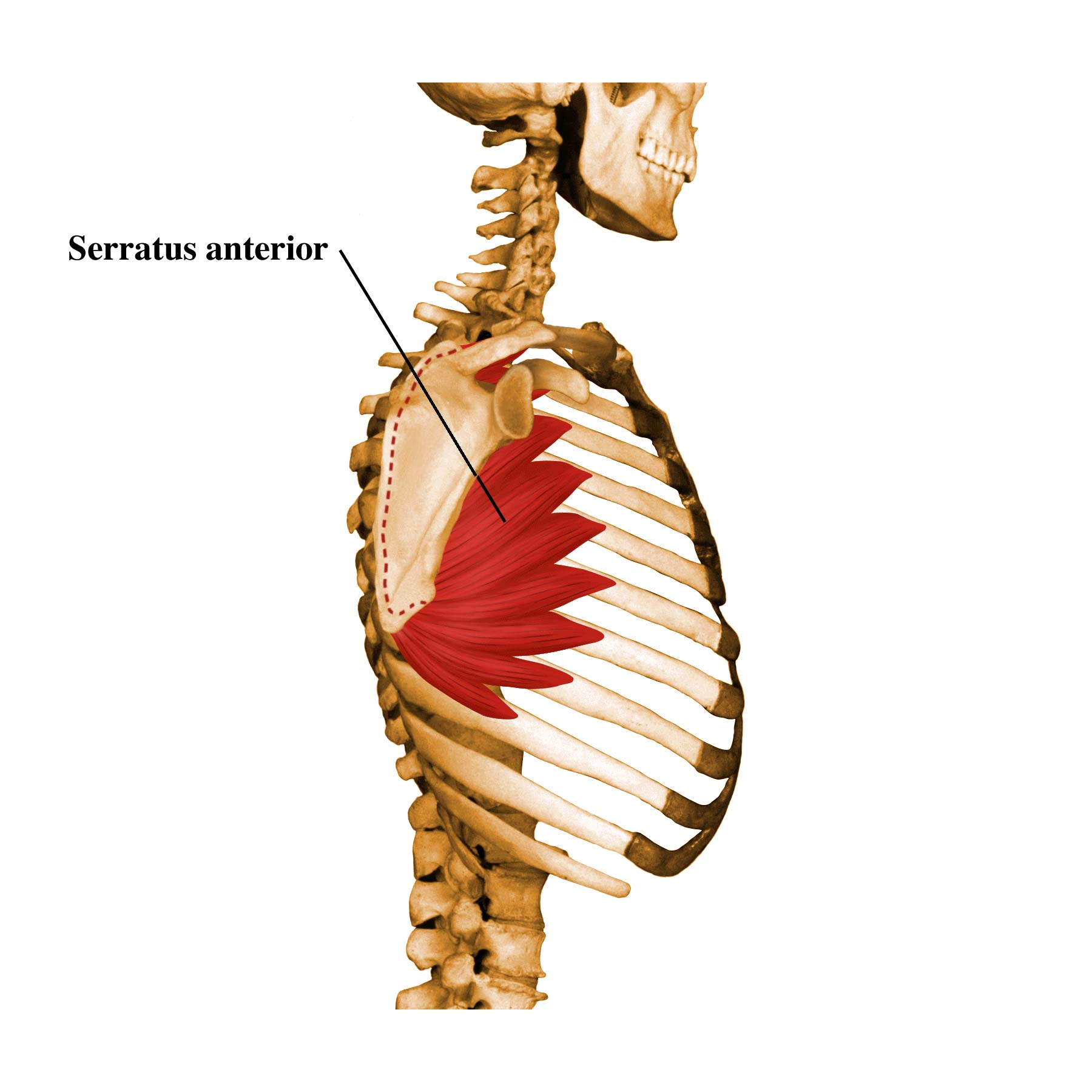
-serratus anterior
-subclavius
-trapezius
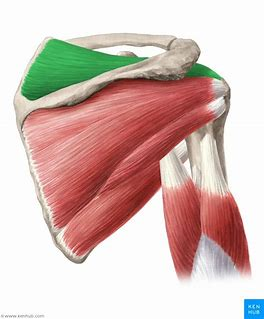
Rhomboids
adduction, elevation, downward rotation
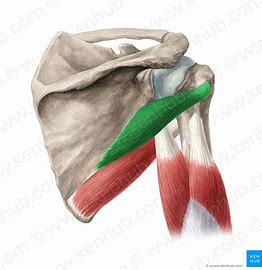
Levator Scapulae
elevation, assists in adduction and downward rotation
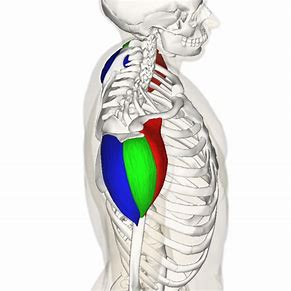
Pectoralis Minor
forward tilt, assists in depression and abduction
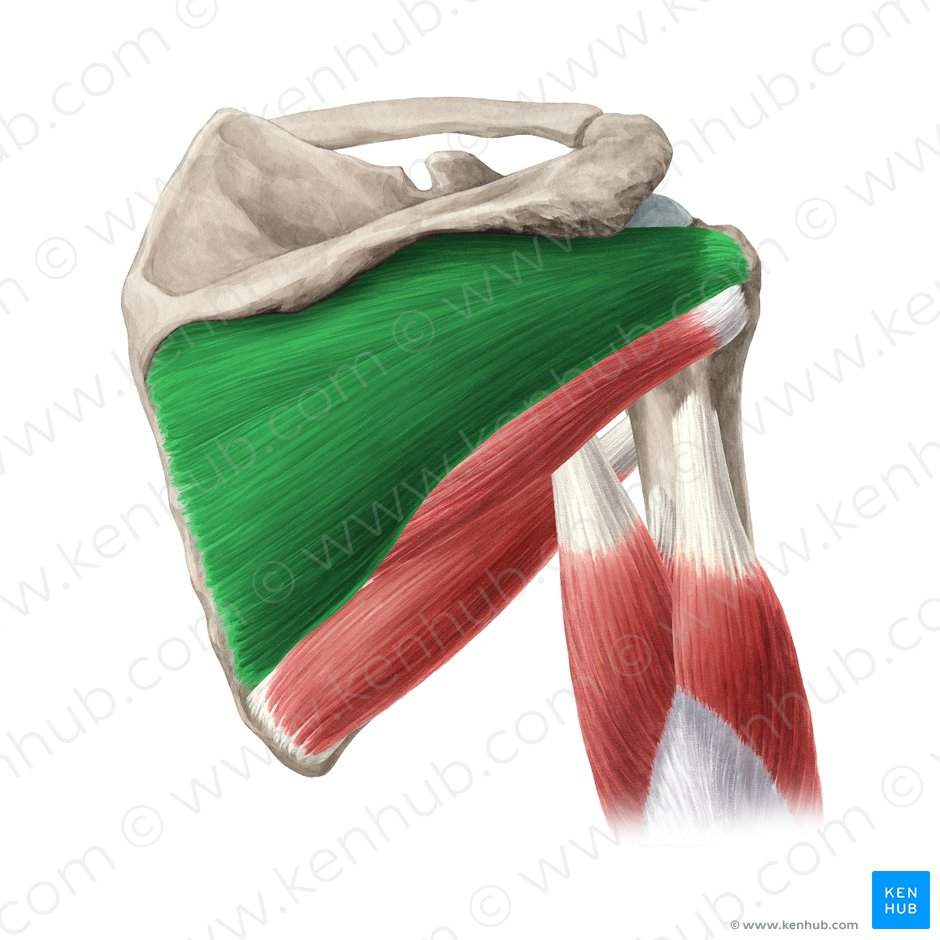
Serratus Anterior
abduction, lower fibers upwardly rotate
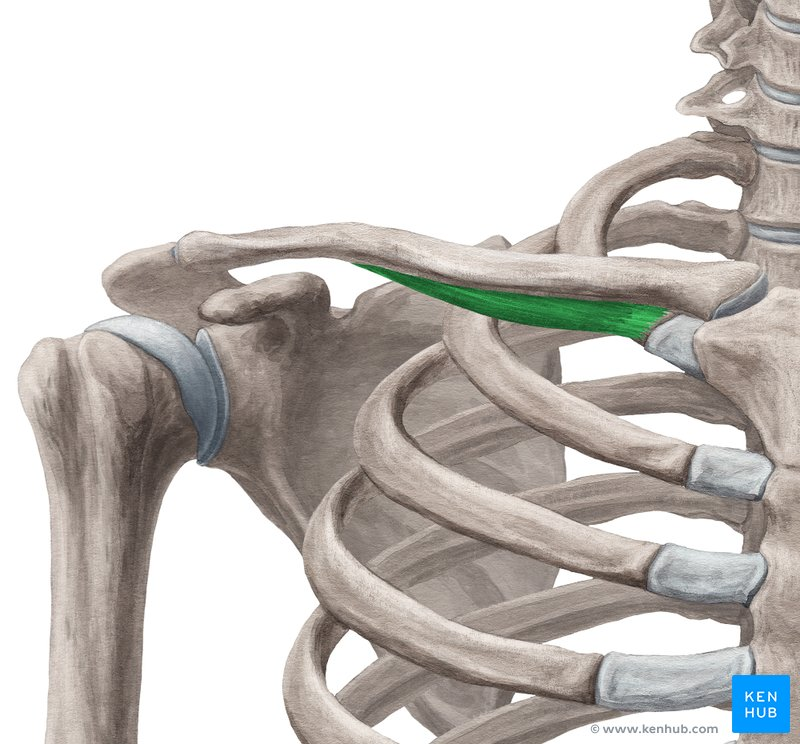
Subclavius
depression, may assist with forward tilt and abduction (slightly)
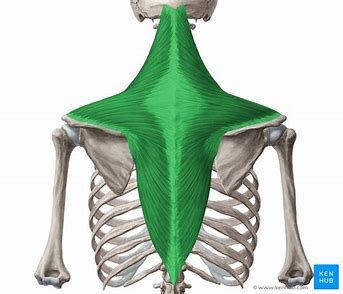
Trapezius
adduction and upward rotation
-upper: elevate, upward rotate, adduct
-middle: adduct
-lower: adduct, upward rotation, depression
Upper Back Tension
shoulder down dilemma: co-contraction of the elevators (upper trapezius and depressors (low traps, pectoralis minor, subclavius)- this does not allow scapulae to upwardly rotate when arms go up in frontal or sagittal plane and creates tension
Pectoralis Minor Syndrome
can be caused by the “shoulders down dilemma”; referred pain in rhomboids and neck, possible numbness in fingers due to tightness of pectoralis minor
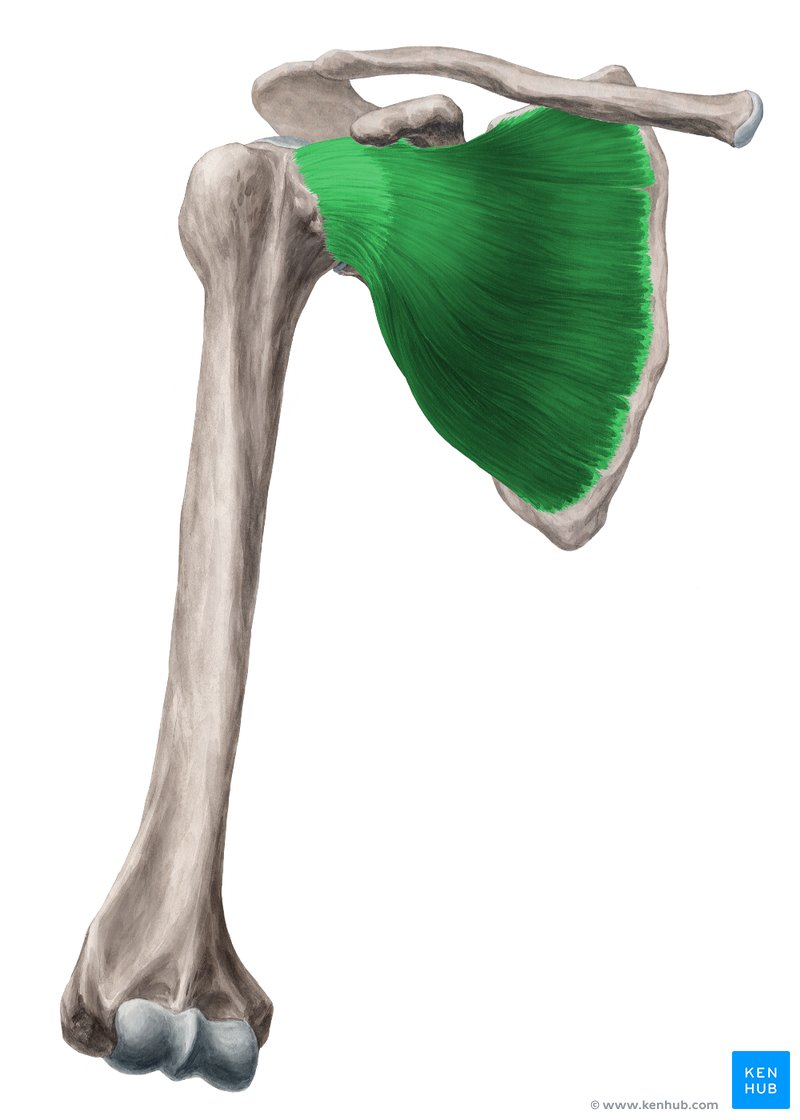
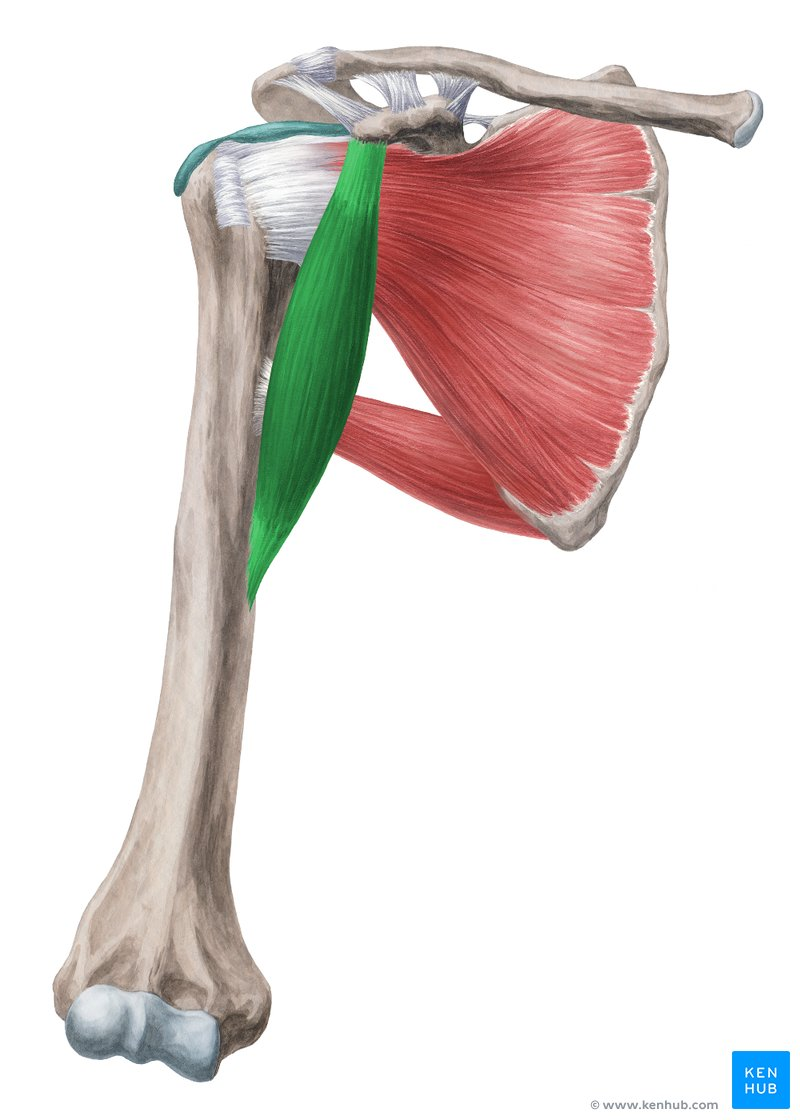
Muscles that Move the Shoulder
-pectoralis major
-latissimus dorsi
-teres major and minor
-infraspinatus & supraspinatus
-deltoids: anterior/middle/posterior
-subscapularis
-coracobrachialis
-biceps brachii
-triceps brachii (longhead)
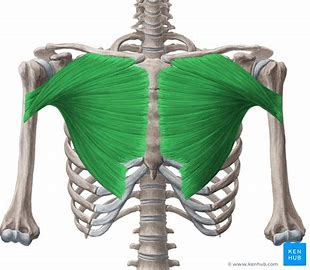
Pectoralis Major
-upper: flexion, adduction, inward rotation
-middle: adduction, inward rotation, horizontal flexion
-lower: extension, adduction, inward rotation
-all: horizontal flexion, inward rotation
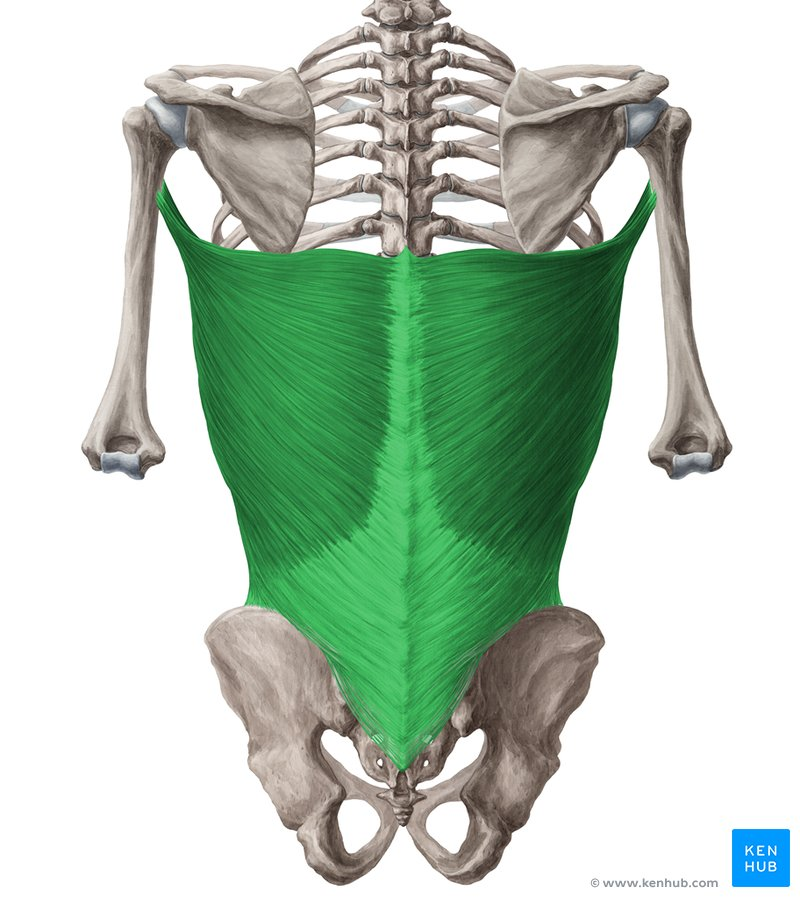
Latissimus Dorsi
extension, adduction, inward rotation, horizontal extension only with inward rotation
Teres Major
extension, adduction, inward rotation, assist with horizontal extension only with inward rotation

Teres Minor
extension, adduction, outward rotation, horizontal extension when the shoulder is outwardly rotated
Infraspinatus
extension, adduction, outward rotation, horizontal extension when the shoulder is outwardly rotated
Deltoids
-anterior: flexion, adduction, inward rotation, horizontal flexion
-middle: abduction
-posterior: extension, outward rotation, adduction, horizontal extension
-all: abduction
Supraspinatus
abduction (synergistic with middle deltoid)
Subscapularis
inward rotation, assists with horizontal flexion and adduction
Coracobrachialis
flexion, adduction, horizontal flexion
Biceps Brachii
-long head: flexion, assists in abduction; originates above glenoid cavity
-short head: flexion, assists in adduction, and horizontal flexion; originates at coracoid process

Triceps Brachii-Long Head:
extension, adduction; originates below glenoid fossa

Rotator Cuff Muscles
-teres minor, infraspinatus, supraspinatus, subscapularis
-muscles responsible for stabilizing the very shallow glenohumeral joint
-need to be balanced in strength and flexibility
Shoulder Problems
dislocations common at the front high diagonal (3/4 flexed), requires strong latissimus dorsi and teres major
Conditioning
necessary for lifting, partnering, and inversions
“Itis”
bicipital tendonitis (inflammation of long head of biceps at bicipital groove), bursitis of the anterior deltoid bursa
Principles of Lifting
1) start with and maintain good alignment
2) lower your own center of gravity before lifting
3) apply as much force as possible with your legs
4) apply the force at the lifted dancer’s center of gravity
5) apply force in a vertical direction
6) keep the lifted dancer’s center of gravity over your own base of support
Why do injuries occur?
-technique adaptations: poor posture, poor muscle control, decreased flexibility, compensation (learned behaviors)
-nutrition: calcium/vitamin D (bone health), fad diets (can lack essential nutrients), good carbs (need whole grains and fiber), good proteins (leaner white meat, turkey, chicken), good fat (unsaturated, nuts, fish, olive oil), supplements (not regulated so use with caution, vitamins not needed with healthy diet (vitamin D important in colder climates), hydration (water is usually sufficient for rehydration, your body is 70% water, can’t lose much without an effect
-strength/flexibility imbalances
-smoking
-sleep: > 7 hours/night ideal, naps < 60 minutes, sleep debt = intoxication
Concussions
-mild traumatic brain injury: blunt or shear trauma to brain
-symptoms: headache, blurred vision, personality change, nausea, vomiting, amnesia, LOC
-diagnosis: testing by doctor and possible CT scan to check for bleeding
-cervical spine injury: no neck pain is good after trauma
-do not give medication right away, can mask symptoms
-return to activity is individualized based on resolution of symptoms and cognitive recovery
Acute Injuries
-concussions, fracture, dislocation, subluxation, sprains and strains
-pops, snaps, crackles, zings, burning, tingling, numbness
-pain, loss of function, obvious deformity, bleeding, constitutional symptoms (fever nausea, etc)
Chronic Injuries
uncontrolled pain, loss of function, unresolving, new or worsening symptoms
PRICE
P- protection
I- ice
C- compression
E- elevation
R- rest
RICE Research
old research- use ice in first 24-72 hours 20 minutes at a time no more than once per hour to reduce swelling and inflammation
new research- ice can slow metabolic processes and nerve conduction velocity impeding inflammatory process
PRICE Protection/Prevention
-protection: taping, wrapping, bracing, walking boot, crutches, wheelchair, etc
-prevention: balanced strength/flexibility, cross-train, efficient alignment