PKP Kap. 6
1/5
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
6 Terms
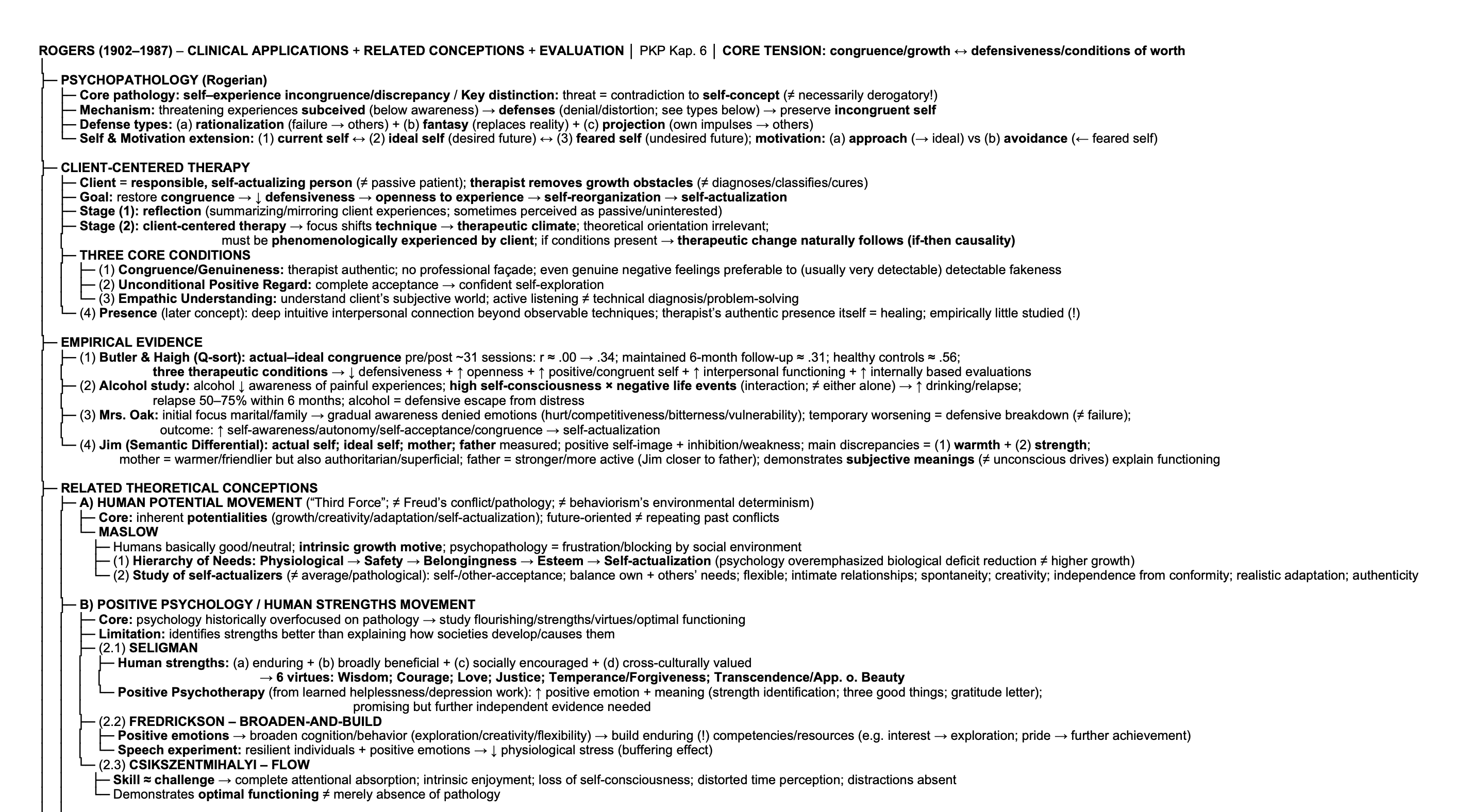
Describe the general and practical clinical applications of Carl Rogers’ theory of personality, and include a few empirical examples.
Psychopathology; Core pathology = self–experience incongruence/discrepancy → self-experience discrepancy; threatening experiences subceived (below awareness) → defenses ( = denial/distortion; they preserve incongruent self, e.g. (a) rationalization (failure → others), (b) fantasy (replace reality), (c) projection (own impulses attributed to others), BUT threat = contradiction to self-concept (≠ necessarily derogatory!))
→ Result: client-centered therapy (see below); client = responsible, self-actualizing person (≠ passive patient); therapist removes growth obstacles (≠ diagnoses/cures/classify disorders); practical application of phenomenological theory
Self & Motivation; (1) Current self ↔ (2) ideal self (desired future) ↔ (3) feared self (undesired future) // Motivation: (a) approach (toward ideal self) vs (b) avoidance (away from feared self).
Therapeutic Process; Goal = restore congruence → reduce defensiveness → openness to experience → self-reorganization → self-actualization.
(1) Early stage: reflection (summarizing/mirroring client experiences; sometimes perceived as passive/uninterested) → (2) Later: client-centered therapy (focus shifts from technique → therapeutic climate; see relevant traits below; theoretical orientation irrelevant; must be phenomenologically experienced by client!! // If these conditions exist → therapeutic change naturally follows; assumption of causality! If-then-logic).
(1) Congruence/Genuineness (therapist authentic; no professional façade; even genuine negative feelings preferable to fakeness that’s OFTEN detectable!).
(2) Unconditional Positive Regard (complete acceptance; facilitates confident self-exploration).
(3) Empathic Understanding (understand client’s subjective world; active listening ≠ technical diagnosis/problem-solving).
Presence (Later concept; deep intuitive interpersonal connection beyond observable techniques; therapist’s authentic presence itself becomes healing; empirically little studied)
Empirical Evidence
(1) Butler & Haigh (Q-sort): actual self + ideal self measured pre/post therapy; ~31 sessions; Congruence: r ≈ .00 → .34; maintained 6-month follow-up ≈ .31; healthy controls ≈ .56 + Later findings: three therapeutic climate conditions → ↓ defensiveness; ↑ openness to experience; ↑ positive/congruent self; ↑ interpersonal functioning; ↑ internally based evaluations.
(2) Applied Research Example; alcohol reduces awareness of painful experiences; high self-consciousness × negative life events (interaction; ≠ either alone) predicts drinking/relapse; relapse 50–75% within 6 months; alcohol functions as defensive escape from distress.
(3) Clinical Case: Mrs. Oak
Initial focus: marital/family problems → gradual awareness of denied emotions (hurt, competitiveness, bitterness, vulnerability).
Temporary worsening = defensive breakdown (≠ therapeutic failure); may include blaming therapist, distress, instability before improvement.
Outcome: ↑ self-awareness; ↑ autonomy; ↑ self-acceptance; independent decisions (incl. divorce, employment); greater congruence → self-actualization.
(4) Assessment Application: Jim (Semantic Differential); Measures: actual self; ideal self; mother; father.
Findings: positive self-image + inhibition/weakness; main discrepancies = warmth & strength // Mother = warmer/friendlier (also authoritarian, superficial, selfish, unintelligent, intolerant); father = stronger, more active, industrious (closer to father!).
Demonstrates phenomenological assessment: subjective meanings (≠ unconscious drives) explain functioning; difficulties reflect actual–ideal incongruence hindering self-actualization.
What are the related theoretical conceptions to Rogers’ theory?
Related Theoretical Conceptions with purpose: extends Rogers beyond psychotherapy; complementary humanistic perspectives → emphasize growth, strengths, meaning ≠ pathology; reinterpret/expand Rogers before modern empirical research.
Human Potential Movement (“Third Force”; alternative to (a) Freud (conflict/pathology) + (b) Behaviorism (environmental determinism))
Core assumption: humans possess inherent potentialities (growth; creativity; adaptation; self-actualization); future-oriented striving → realizing capacities ≠ repeating past conflicts/conditioning.
Abraham Maslow assumed that humans are basically good/neutral; intrinsic growth motive; psychopathology → frustration/blocking of natural development by social environment.
Contribution 1: Hierarchy of Needs; Physiological (food; water) → Safety → Belongingness → Esteem → Self-actualization (Psychology overemphasized biological deficit reduction ≠ higher psychological growth)
Contribution 2: Study of self-actualizers; Study exceptionally healthy individuals ≠ average/pathological populations
Characteristics: self-/other-acceptance; balance own + others’ needs; flexible (≠ stereotyped); intimate relationships; spontaneity; creativity; independence from conformity; realistic adaptation; authenticity.
Positive Psychology / Human Strengths Movement
Core claim: psychology historically overfocused on pathology (e.g., Freud’s clinical samples); study flourishing, strengths, virtues, optimal functioning.
Limitation: identifies strengths better than explaining how societies systematically develop them.
(2.1) Seligman
Human strengths: (a) enduring; (b) broadly beneficial; (c) socially encouraged; (d) cross-culturally valued → 6 virtues: Wisdom; Courage; Love; Justice; Temperance (forgiveness); Transcendence (appreciation of beauty).
Positive Psychotherapy (because early work on learned helplessness & depression): ↑ positive emotion + meaning (strength identification; three good things; gratitude letter); promising but further independent evidence needed (!)
(2.2) Fredrickson: Broaden-and-Build Theory
Positive emotions → broaden cognition/behavior (exploration; creativity; flexibility) → build enduring competencies/resources (e.g. interest → exploration; pride → further achievement)
Speech experiment: resilient individuals experiencing positive emotions → ↓ physiological stress (buffering effect).
(2.3) Csikszentmihalyi: Flow
Skill ≈ challenge; complete attentional absorption; intrinsic enjoyment; loss of self-consciousness; distorted time perception; distractions absent.
Demonstrates optimal functioning ≠ merely absence of pathology.
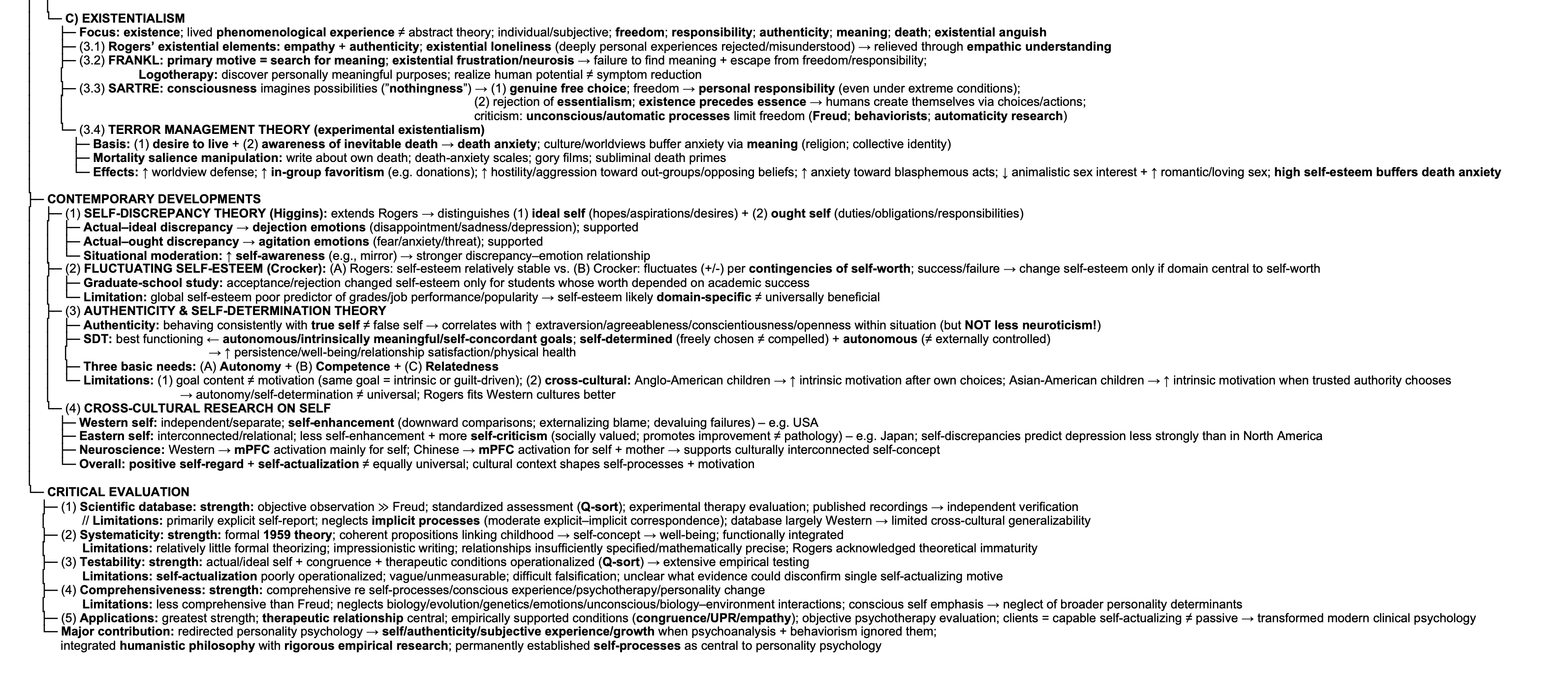
Existentialism
Focus: existence; human condition; lived (phenomenological) experience ≠ abstract theories/general law; individual; subjective experience; freedom; responsibility; authenticity; meaning; death; existential anguish.
(3.1) Rogers’ existential elements
Empathy; authenticity + Existential loneliness: deeply personal experiences rejected/not understood → relieved through empathic understanding.
(3.2) Frankl
Primary motive = search for meaning; Existential frustration/neurosis → failure to find meaning; escape from freedom/responsibility.
Logotherapy: discover personally meaningful purposes; realize human potential ≠ merely symptom reduction.
(3.3) Sartre
(a) Consciousness imagines possibilities (“nothingness”) → genuine free choice; Freedom → personal responsibility (even under extreme conditions).
(b) Rejects essentialism: existence precedes essence; people create themselves through choices/actions; Humans ≠ objects/animals (e.g., painting a brown horse white ≠ changes essence; humans create identity).
Criticism: Freud; behaviorists; automatic-process research → unconscious/automatic determinants limit freedom.
(3.4) Terror Management Theory (Experimental Existentialism)
Basis: (1) desire to live + (2) awareness of inevitable death → potential death anxiety (terror) // Culture/worldviews buffer anxiety by providing meaning (religion; collective identity).
Mortality salience manipulation: write about own death; death-anxiety scales; gory fatal-accident films; subliminal death primes → Effects: ↑ worldview defense; ↑ in-group favoritism (e.g., donations); ↑ hostility/physical aggression toward out-groups/opposing beliefs; ↑ anxiety toward blasphemous cultural/religious acts; ↓ interest in purely animalistic sex; ↑ interest in romantic/loving sex; high self-esteem buffers death anxiety → Existential concepts become experimentally testable.

Describe contemporary developments of Rogers’ theory.
(1) Self-Discrepancy Theory (Higgins):
Extends Rogers by distinguishing: (1) Ideal self: hopes; aspirations; desires; (2) Ought self: duties; obligations; responsibilities.
(a) Actual–ideal discrepancy → dejection emotions (disappointment; sadness; depression; supported!), (b) Actual–ought discrepancy → agitation emotions (fear; anxiety; threat; supported!).
Situational moderation: Greater self-awareness (e.g., mirror) → stronger discrepancy–emotion relationship.
(2) Fluctuations in Self-Esteem (Crocker)
(A) Rogers: self-esteem relatively stable vs (B) Crocker: self-esteem fluctuates according to contingencies of self-worth; Success → ↑ self-esteem; failure → ↓ self-esteem only if domain is central to self-worth.
Graduate-school study: Acceptances/rejections changed self-esteem only for students whose self-worth depended on academic success.
Extension of Rogers: (1) Explains both stable self-esteem and day-to-day fluctuations + (2) Objective events matter only when personally valued / Limitation of global self-esteem: Poor predictor of objective outcomes (grades; job performance; popularity) → self-esteem likely domain-specific rather than universally beneficial.
(3) Authenticity & Self-Determination Theory
Authenticity: behaving consistently with the true self ≠ false self-presentation → correlation w/ healthier functioning and greater extraversion, agreeableness, conscientiousness, opennesswithin that situation.
Self-Determination Theory
(1) Best functioning → autonomous, intrinsically meaningful, self-concordant goals; (a) Self-determined = freely chosen (≠ compelled) + (b) autonomous/self-initiated (≠ externally controlled) → ↑ persistence; well-being; relationship satisfaction; physical health.
(2) Three basic psychological needs: (A) Autonomy (self-directed action), (B) Competence (feeling effective), (C) Relatedness (connection with others).
Limitations: (1) Goal content ≠ motivation (same goal may be intrinsic or guilt-driven); (2) Cross-cultural variation (see below): Anglo-American children → greater intrinsic motivation after own choices VS Asian-American children → greater intrinsic motivation when trusted authority figures choose → Autonomy/self-determination may not operate universally; Rogers may fit Western cultures better.
(4) Cross-Cultural Research on the Self
(W) Western self: independent; separate // (E) Eastern self: interconnected; relational / (W) United States; Self-enhancement: downward comparisons, externalising blame; devaluing failures / (E) Japan; Less self-enhancement, More self-criticism (socially valued; promotes continual self-improvement rather than pathology) → Self-discrepancies predict depression less strongly than in North America.
Neuroscience evidence: (W) Western participants: (mPFC activation mainly when thinking about self), (E) Chinese participants (MPFC activation for self + mother) → Supports culturally interconnected self-concept.
Overall implication Positive self-regard and self-actualization are not equally universal; cultural context shapes self-processes and motivation.
Evaluate Rogers’ theory.
Major Contributions: Redirected personality psychology toward self, authenticity, subjective (phenomenological) experience, and personal growth when psychoanalysis and behaviorism largely ignored them + Integrated humanistic philosophy with rigorous empirical psychotherapy research; permanently established self-processes as central to personality psychology.
Scientific Database
Strengths: objective scientific observation ≫ Freud; standardized assessment (Q-sort); experimental evaluation of therapy; published recordings/transcripts → independent verification; objective outcome measurement.
Limitations: primarily explicit self-report measures; neglects implicit processes (only moderate explicit–implicit correspondence); conscious awareness emphasized; database largely Western → limited cross-cultural generalizability.
Theory: Systematic?
Strengths: formal 1959 theory = coherent propositions linking childhood experiences → self-concept → psychological well-being; concepts functionally integrated.
Limitations: relatively little formal theorizing; impressionistic writing style; relationships insufficiently specified/mathematically precise; Rogers acknowledged theoretical immaturity.
Theory: Testable?
Strengths: actual self; ideal self; congruence; therapeutic conditions operationalized (Q-sort etc.) → extensive empirical testing.
Limitations: self-actualization poorly operationalized; vague definition; no clear measurement; difficult falsification; unclear evidence that could disconfirm single self-actualizing motive.
Theory: Comprehensive?
Strengths: comprehensive regarding self-processes, conscious experience, psychotherapy, personality change.
Limitations: less comprehensive than Freud; limited treatment of biology, evolution, genetics, emotions, unconscious processes, and biology–environment interactions; emphasis on conscious self/growth → neglect of broader determinants of personality.
Applications
Greatest strength of the theory; therapeutic relationship central; empirically supported therapeutic conditions (congruence; unconditional positive regard; empathic understanding); objective psychotherapy evaluation; clients treated as capable, self-actualizing individuals ≠ passive patients; transformed modern clinical psychology.
Tree (PKP Kap. 6) 1/2
Tree (PKP Kap. 6) 2/2