5 - Sleep-wake disorders
1/34
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
35 Terms
How is sleep defined?
A behavioural state characterised by: specific posture, reduced motor activity, suspension of consciousness, ↓ metabolism, ↓ interaction/reciprocity with env
What are the functions of sleep?
exact functions unknown, but thought to be memory/learning consolidation
Existing understanding comes from studies examining sleep loss/pathologica sleep conditions
What are the three assessment methods of sleep?
clinical interview - routine assessment, evaluation of nature/severity/hisotry of sleep problems
Self report questionnaire & symptom checklist - simple, quick, convenient
Sleep diary - eval of insomnia
What are the two ways to objectively measure sleep?
polysomnography (PSD) - in lab, controlled setting under supervision of technician, multiple channels of data collected - gold standard
Multiple physiological variables measures - air flow at nose, best around chest to measure breathing, sensor on finger to measure oxygen
Actigraphy - wrist-watch devises, measures wrist movement to assess sleep, can measure in natural setting
What are the three distinct states and stages of sleep?
states: wake, NREM, REM
Stage 1: between awake & falling asleep. Light sleep
Stage 2: disengaged from surrounding, body temp ↓, breathing and heart rate same - 40-55% of the night
Stage 3: slow wave sleep (deep sleep), deepest & restorative sleep, blood pressure ↓, 10-20% (declines with age)
REM sleep:brain is active, dreams occur, eye moves, body becomes immobile (paralysis), 25%
How does the sleep architecture as one ages generally?
child: less awakening, more and longer slow wake sleep ⇒ less waking, more REM sleep, most NREM sleep
Elderly: more awakening at night, less slow wake sleep ⇒ more waking, very little REM sleep, little NREM sleep
What are the two processes that regulates sleep?
homeostatic sleep process (“Process S”) - sleep drive/pressure to sleep, ↑ after each hour waking up
Circadian process (“process C”) - biological clock
Internal biological clock: suprachiasmatic nucleus in hypothalamus (light signals from retina conveyed to nucleus via nerve fibers
External cues: 24 hr light/dark cycle
Regulation of circadian rhythm - secretion of melatonin by pineal gland (melatonin reaches receptors in hypothalamus, body thinks it is dark)
When there is the greatest gap bw process s and c = greatest urge to sleep
What are the four categories of consequences of sleep deprivation?
physical - fatigue, daytime sleepiness
Psychological - irritability, low mood, anxiety (↓ emotional regulation), ↑ risk of developing mood disorder
Cognitive - ↓ vigilance, impaired concentration decision making memory, impact on academic performance
Behavioural: daydreaming, aggressive, hyper/hypoactive
Does sleep compensation (sleeping more in the weekend to make up for lost sleep in the weekdays) work?
no
Disturbs biological clock - e.g. difficulty falling asleep on Sunday
What are the two major types of sleep disorders?
Dyssomnias - disorder of falling/staying asleep. difficulties with timing/quantity/quality of sleep
E.g. insomnia, narcolepsy, circadian rhythm sleep-wake disorder
Parasomnias - disorders of arousal & abnormal physical activities during sleep. unwanted abnormal behaviours/movements/experiences during sleep
e.g. disorder of arousal, nightmare disorder, REM sleep behaviour disorder
Explain the DSM5 diagnostic criteria for insomnia disorder
difficulty initiating & maintaining sleep
Early morning awakening with inability to return to sleep
Frequency: at least three nights per week
Duration: for at least 3 months
Occurs despite adequate opportunity for sleep
What are some adverse consequences of insomnia
↑ risk of depression, anxiety, other mental illnesses
Insomnia bidirectional related to depression, insomnia is residual symptom in MDD
Hypertension
↑ susceptibility to cold & chronic pain
What is the old and new understanding of insomnia as a condition?
old: insomnia as a symptom of underlying physical/mental disorders (e.g. assume treating depression removes insomnia)
New: insomnia as alone/comorbid clinical condition
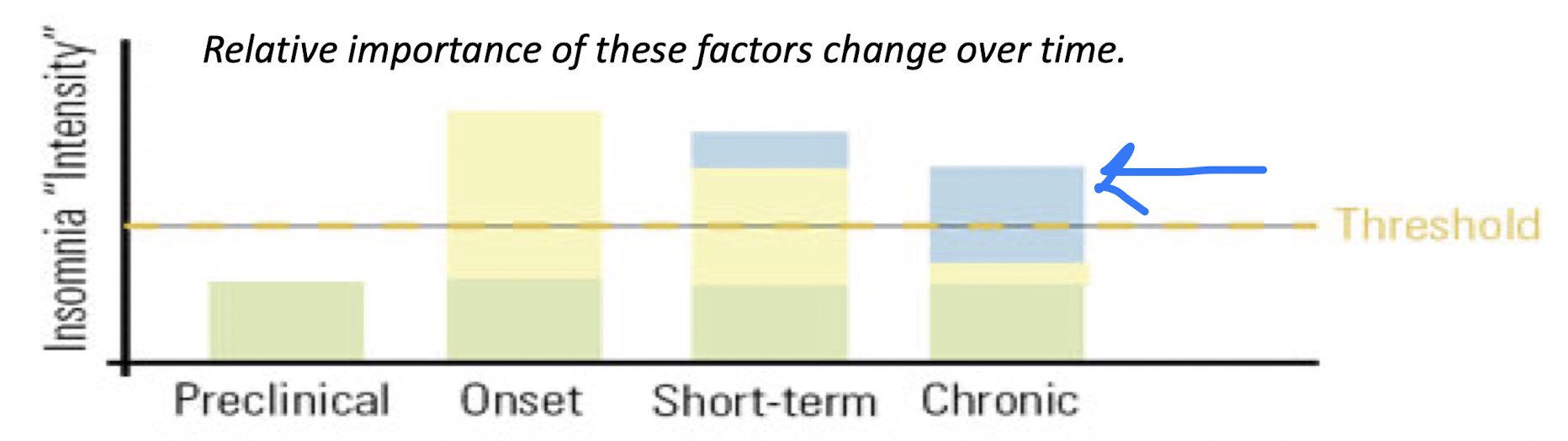
Explain the Three-Factor Model (cause of insomnia)
Combination of:
predisposing factors - biological, psychological, social factors
precipitating factors - medical, psychiatric illness, stressful life events
perpetuating factors - time in bed (perpetuates sleep difficulties), napping, conditioning (conditioned arousal)
What does an assessment entail?
sleep history - nature, frequency, duration, treatment history, other symptoms, sleep wake schedule, routine
E.g. assessed using sleep diary or insomnia severity index
Medical & psychiatric history, physical examination
Is a polysonography necessary for insomnia?
No, but can help rule out other sleep disorders (e.g. sleep apnea 0 breathing difficulties eating to waking at night)
What are some treatments for insomnia?
pharmacotherapy
Usually to treat comorbid medical/psychiatric illnesses
E.g. benzodiazepine, zopiclone, zolpidem, antihistamine, sedative antidepressants
Non-pharmacological treatment (first line treatment)
Psychoeducation/sleep hygiene
Behavioural treatment
Cognitive therapy
What are the advantages and disadvantages of using pharmacotherapy?
Adv
immediate relief of insomnia symptoms (but temporary)
Preventing learned insomnia due to increased anxiety at bedtime
Disadv
tolerance, dependence, sedation
Impairment of cognition, moot activity, performance
Parasomnia
Not long term
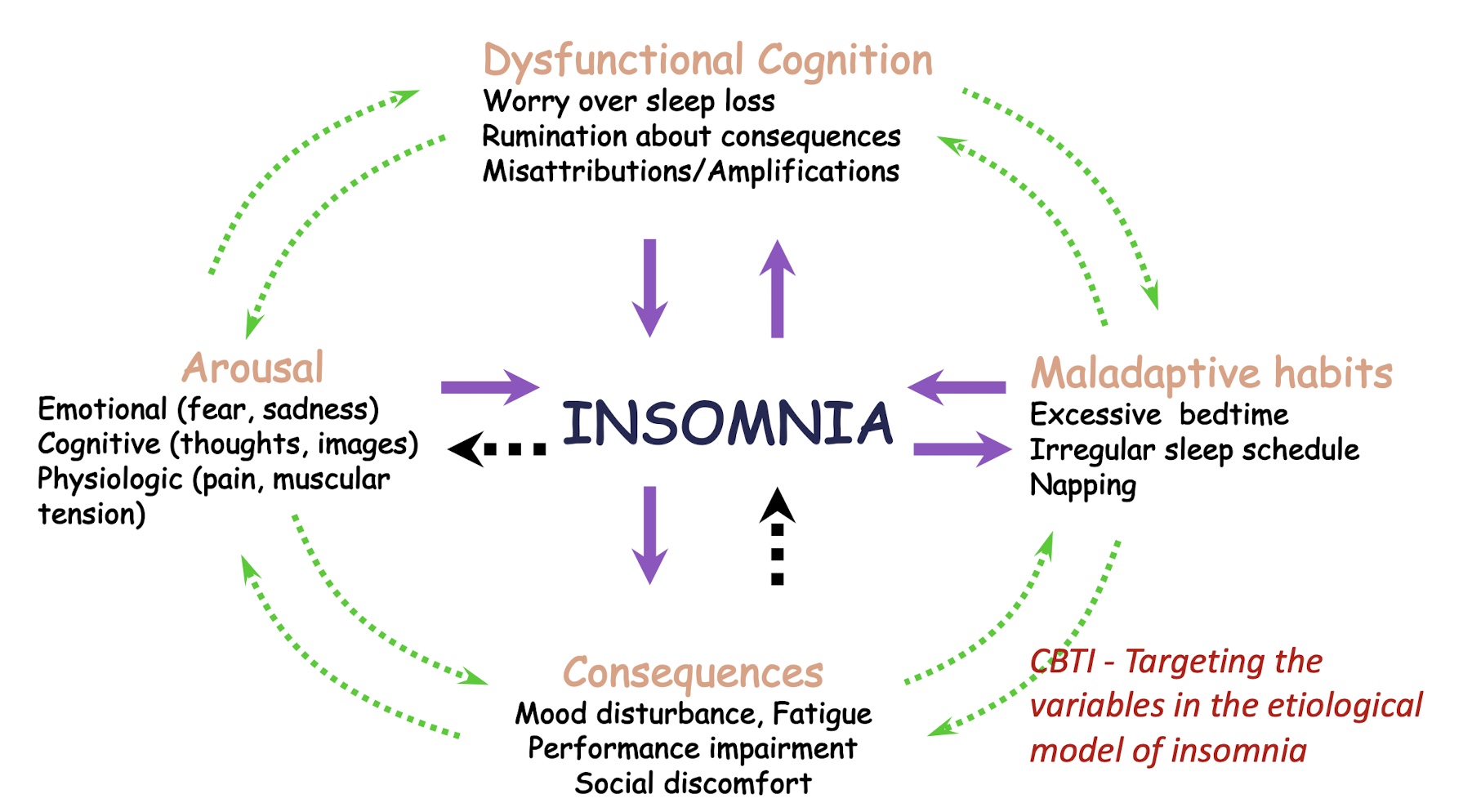
What is the CBT model of insomnia?
dysfunctional cognitive, maladaptive beliefs, consequences, arousal
How effective is CBT for chronic insomnia?
70-80% achieve therapeutic response w CBT
40% achieve clinical remission
CBT & benzodiazepine has comparable effectiveness during active treatment
But more sustainable, has long term, durable effects, better for sleep initiation problems
Explain what circadian rhythm sleep wake disorders is
misalignment between sleep-wake pattern and what is desired/norm
Diff types: delayed sleep phase (difficulty falling asleep), advanced sleep phase (sleeping/waking too early), irregular sleep-wake cycle, (jet lag + shift work)
What are the five treatment methods of CRSD?
sleep hygiene
Chronotherapy - progressive delay of sleep wake schedule until patient can consistently sleep earlier
Bright light therapy - trick brain’s biological clock, early exposure to light = early wake time
Melatonin
Co-morbid psychopathology treatment
What is narcolepsy?
disabling sleep order where people spontaneously sleep
DSM: recurrent periods with irrepressible need to sleep, lapses into sleep or napping in the same day. At least 3x per week over 3 months
0.034% prevalence
What is the pathophysiology of narcolepsy?
Hypocretin deficiency
(Hypocretin = NT involved in maintaining stable wakefulness and suppressing REM sleep)
What are the symptoms of narcolepsy?
sleep related hallucinations
Sleep paralysis
Cataplexy (temporary loss of muscle with preserved consciousness)
Excessive daytime sleepiness
Fragmented nocturnal sleep
What are some ways of managing excessive daytime sleepiness?
sleep hygiene (scheduled naps, regular sleep wake schedule) - rarely effective alone, often paired with pharmacological treatment
Pharmacological: methylphenidate, modafinik, sodium ox ate, selenite
What is parasomnia?
abnormal behavioural/physiological events that accompany sleep
During entry to sleep, within, or during arousals from sleep - not conscious
What are the two characteristic symptoms of NREM sleep arousal disorder?
sleep walking - rising from bed during sleep and walking, during first third of sleep episode, person is unresponsive during, has amnesia for the episode, no impairment of mental activity/behaviour
Sleep terrors - abrupt awakening from sleep, intense fear (e.g. tachycardia), relative unresponsiveness to efforts of comforting
What is the epidemiology of sleep walking? What are their aetiologies?
childhood - more common, 5-30%, ↓ w age
Due to genetics & delayed CNS maturity
Adults - less common, 2-5%, adult onset is rare (majority of adult sleepwalkers had childhood onset), associated with stress
Due to psychopathology, stress, medications, medical illnesses
What is REM Sleep behaviour disorder? (RBD)
dream-enacting behaviours (movement during dreaming)
Sleep related injuries
How is RBD linked to neurodegenerative disorders?
RBD = precursor of neurodegenerative disorders
38-45% of RBD patients dev ^
More than 80% of RBD patients develop Parkinson/dementia after 13 year follow up
How is RBD managed?
screen for neurodegenerative disease
Safety of sleeping env
Pharmacological
Clonazepam (only manages symptomatic presentation, but underlying neurodegeneration)
Has complete/partial response
Side effects = confusion, fall, exacerbation
What is nightmare disorder according to DSM?
repeated occurrence of extended, dysphoric, well-remembered dreams involving efforts to avoid threats - occurs during second half of major sleep episode
When awake, rapidly oriented and alert
Dream causes significant distress/impairment
Nightmares in children vs adults
children: more common, ↓ w age, more prevalent in girls
Adult: limited studies, varied prevalence due to diff operational def
Nightmares in context of psychopathology
PTSD - highly prevalent & persistent (e.g. 5 nightmares/week for SA victims, up to 80-90% of concentration camp survivors), implicated in clinical course of PTSD
MDD, panic disorder
BPD
schizophrenia
alcohol dependence & abuse
Comorbid w insomnia