Urinary System (Pt 2)
1/27
Earn XP
Description and Tags
Ch 24
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
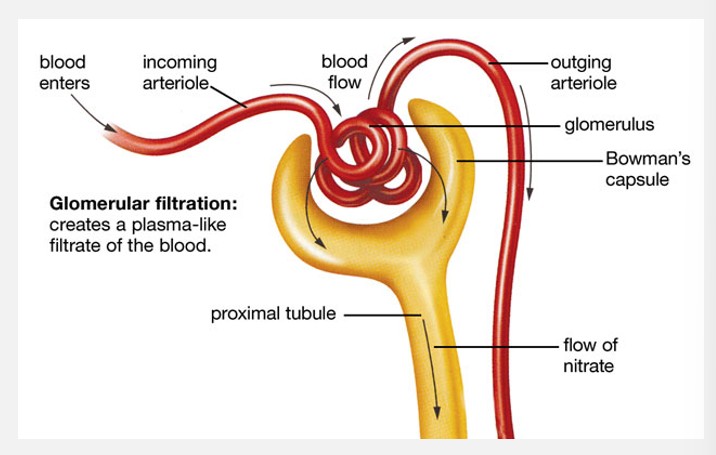
Filtrate, tubular fluid, and urine flow (pt 1)
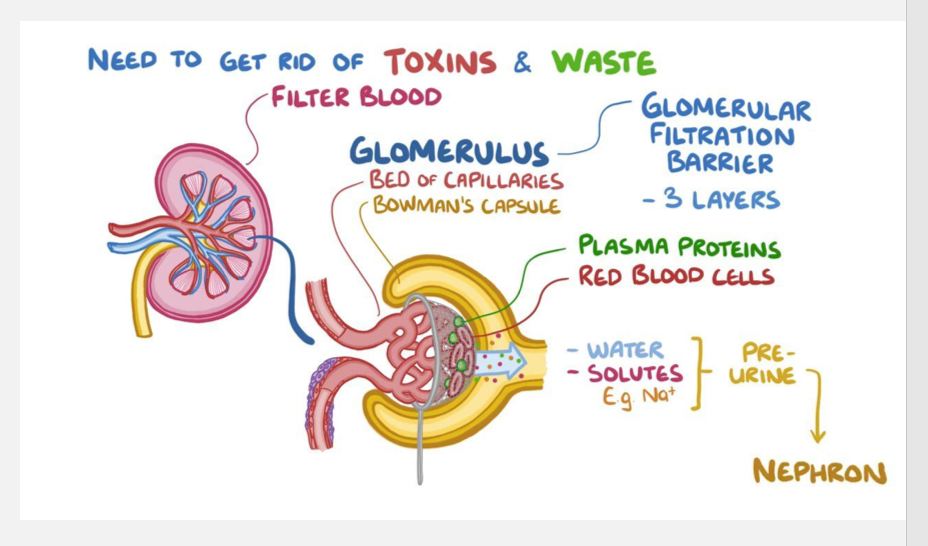
Filtrate
Blood flows through glomerulus
Both water and solutes filtered from blood plasma
Moves across wall of glomerular capillaries and into capsular space
Forms filtrate
The first step of urine formation is filtration
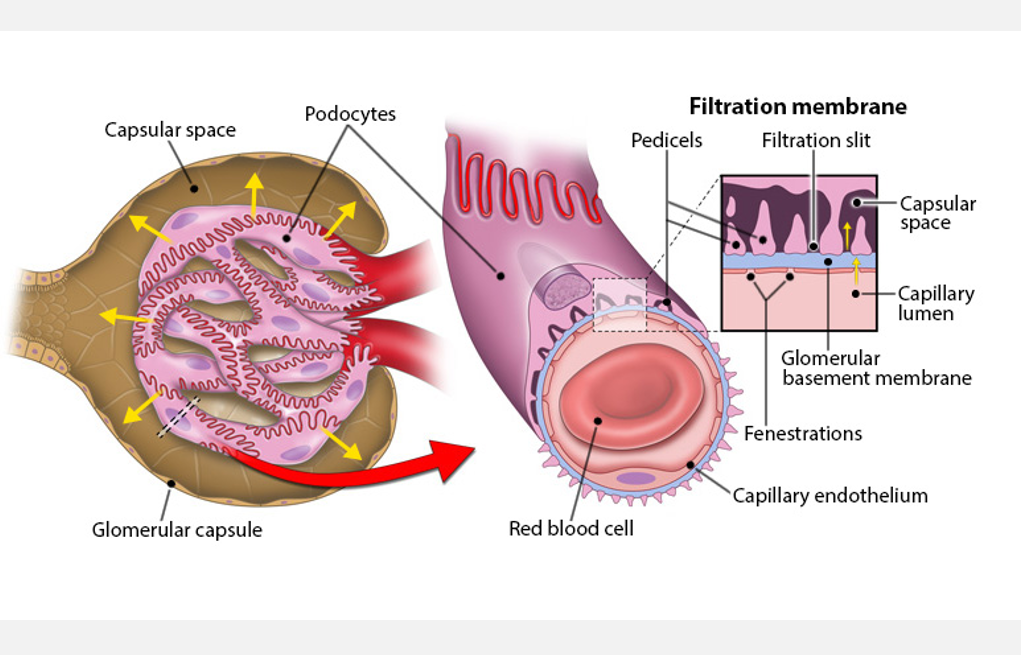
LAYERS OF THE FILTRATION BARRIER
1. Capillary endothelium
Fenestrated; very permeable
Allows passage of anything smaller than a cell
2. Basement membrane
Fused; not as permeable
Blocks all but small proteins
3. Podocytes of glomerular capsule
Pedicels create filtration slits
Prevents passage of most molecules
Overview of urine formation (pt 1)
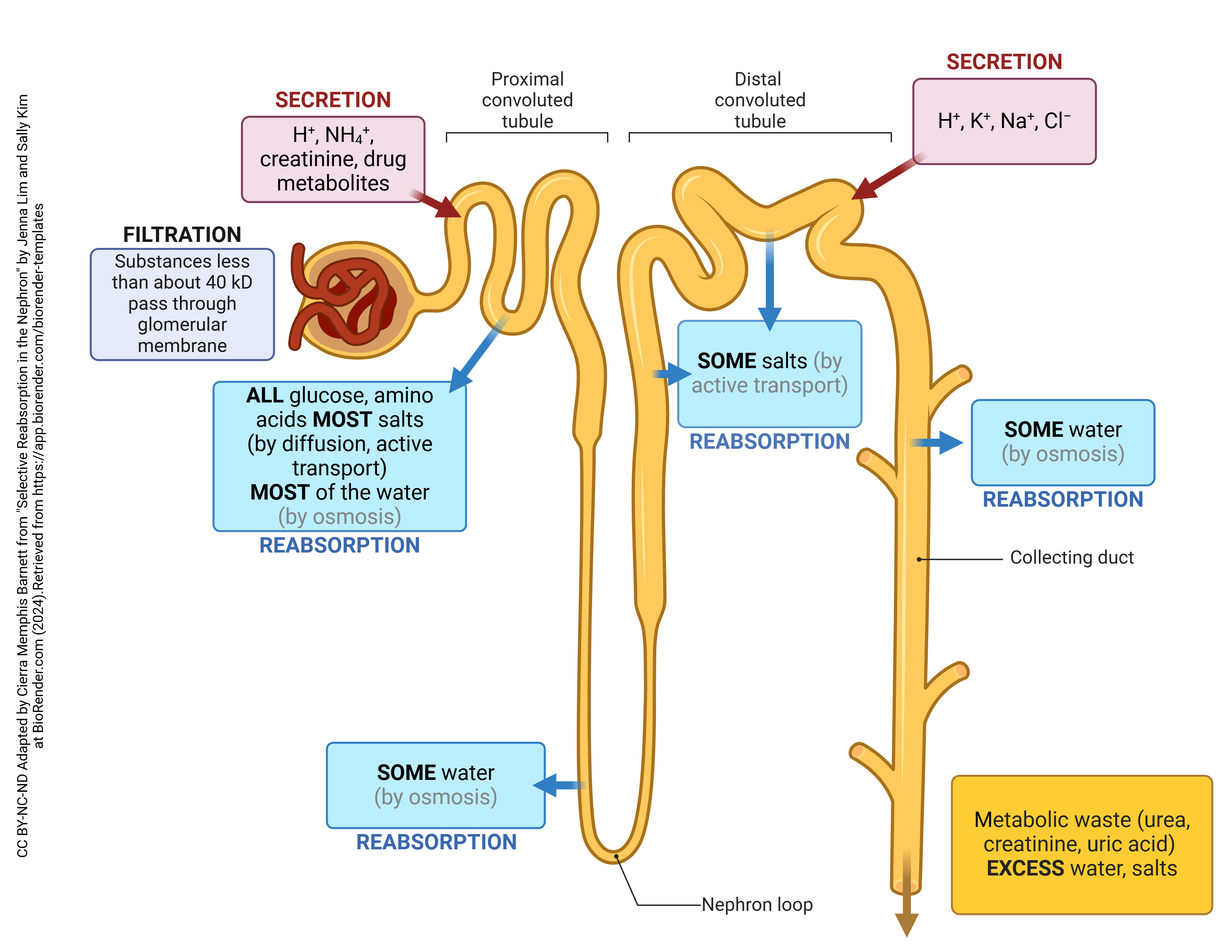
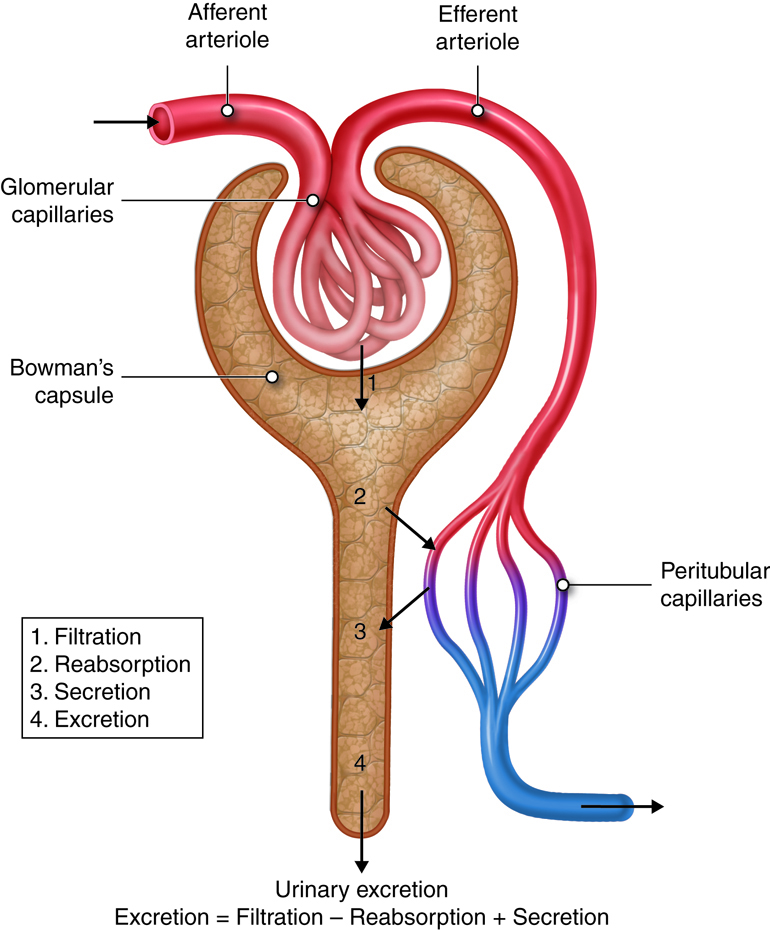
Urine formed through 3 interrelated processes
Filtration, reabsorption, and secretion
Steps of urine formation:
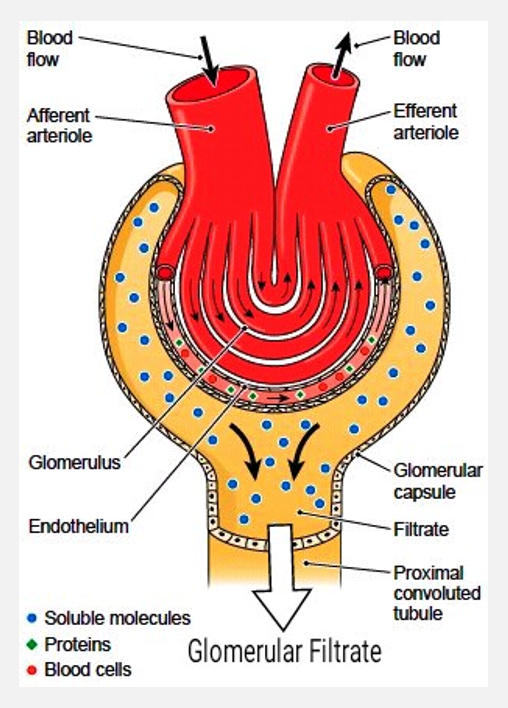
1. Glomerular filtration
In glomerular capillaries
Separates some water and dissolved solutes from blood plasma
Water and solutes enter capsular space of renal corpuscle
Due to pressure differences across filtration membrane
Separated fluid is called filtrate
Substances filtered by filtration membrane
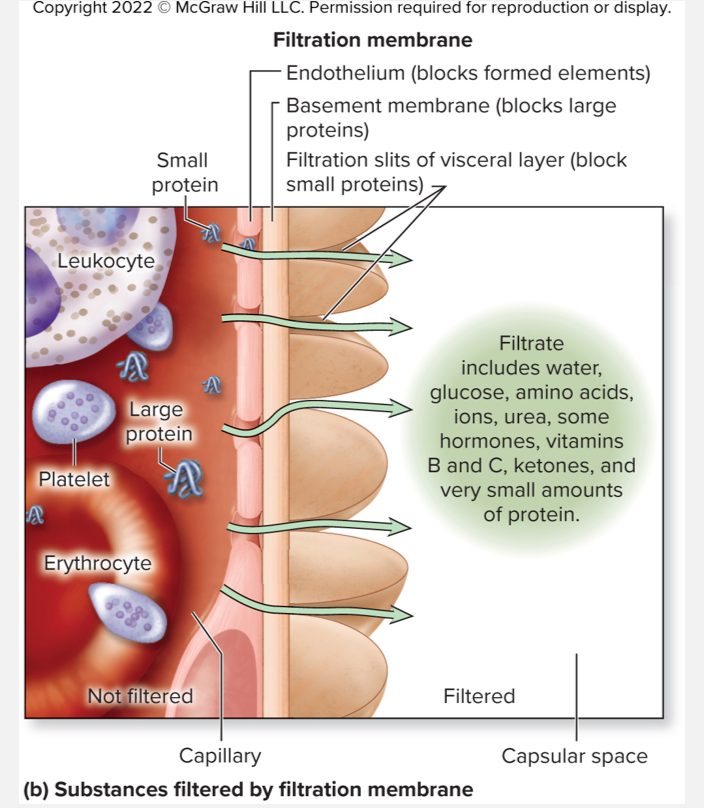
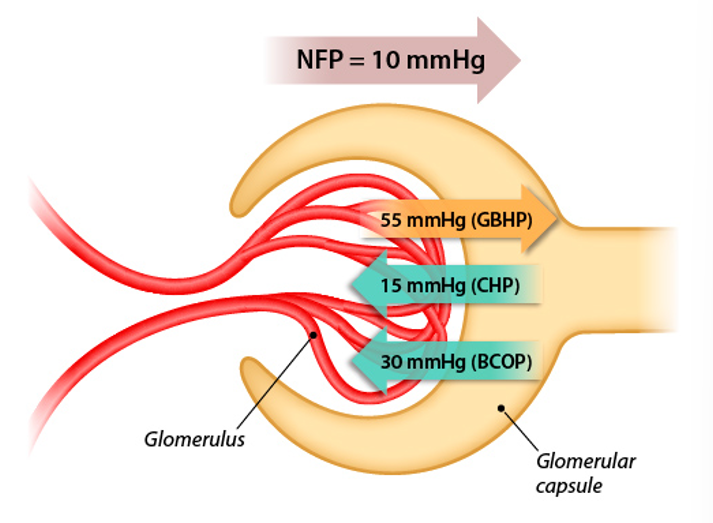
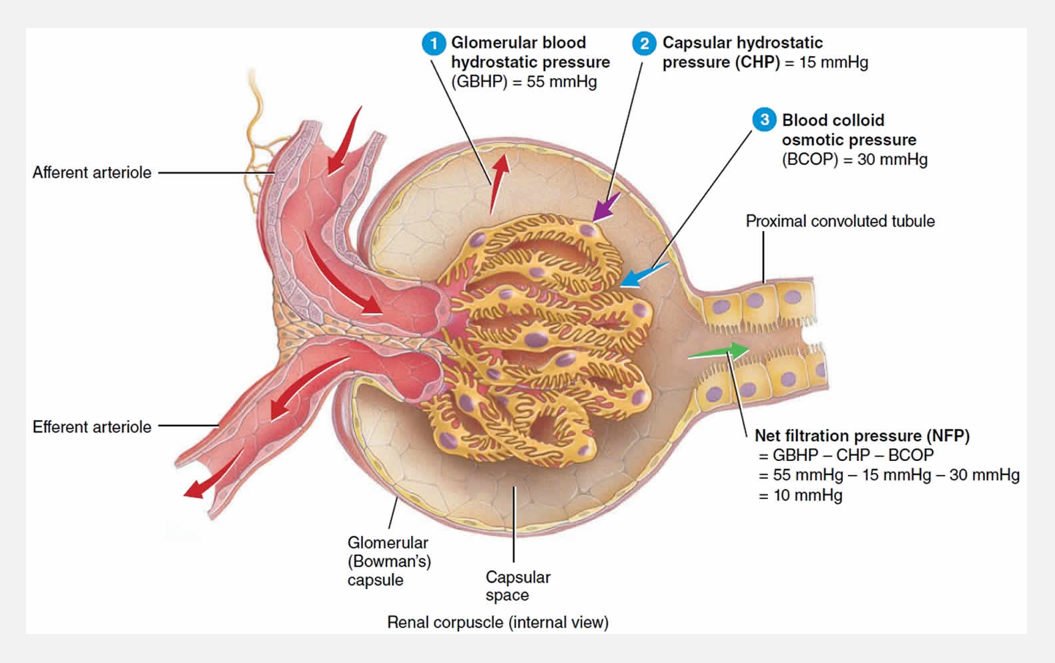
Filtration is driven by pressure differences
GBHP = glomerular blood hydrostatic pressure
Blood pressure w/in the glomerulus
Drives filtration
CHP = capsular hydrostatic pressure
Hydrostatic pressure inside glomerular capsule
Opposes filtration
BCOP = blood colloid osmotic pressure
Osmotic pull of proteins not being filtered
Opposes filtration
NFP = net filtration pressure
NFP = GBHP - (CHP + BCOP)
Pressures associated with glomerular filtration
Determining net filtration pressure
If pressures promoting filtration are greater than pressures opposing
Difference is net filtration pressure (NFP)
HPg - (OPg + HPc) = NFP
60 mm Hg - (32 mm Hg + 18 mm Hg) = NFP
60 mm - 50 mm Hg = 10 mm Hg
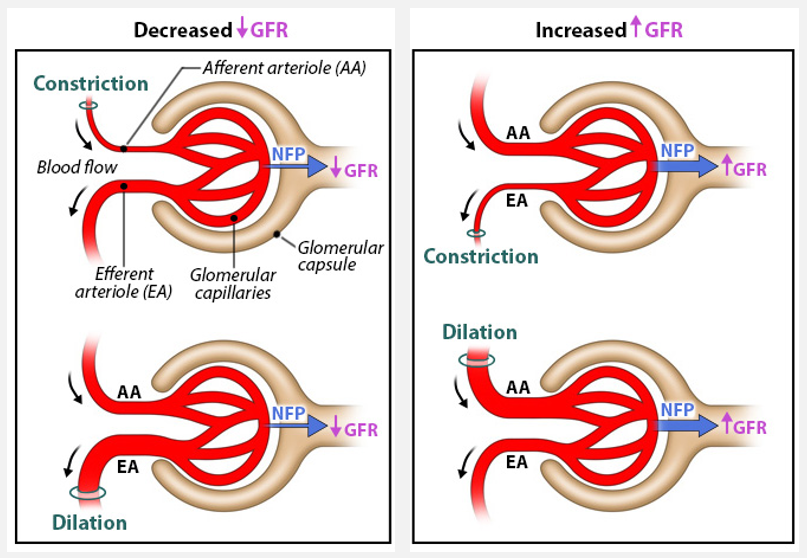
Glomerular filtration rate (GFR) and regulation of filtration
Glomerular filtration rate = the total volume of filtrate formed by all of the glomeruli of both kidneys each minute
The magnitude of NFP is directly proportional to GFR
Renal clearance and glomerular filtration
Renal clearance is a measurement of how quickly the kidneys remove a substance from plasma and excrete it in urine
Renal clearance is used to determine how quickly a drug/chemical is eliminated by the kidneys
A substance w/a high renal clearance is quickly removed from the blood
The renal clearance of a substance that is neither reabsorbed nor secreted by the tubules is equal to the GFR
Approximating GFR using renal clearance
C = rate of renal clearance, typically in mL/min
U = concentration of substance in the urine
V = rate of urine formation
P = concentration of substance in the blood plasma
Assumptions for substance to approximate GFR:
It must freely pass through the filtration membrane
It must neither be reabsorbed from nor secreted into the filtrate by the renal tubules
The renal clearance rate of inulin is equal to GFR. Based on the values below, calculate GFR.
Inulin concentration in urine = 50 mg/mL
Inulin concentration in blood plasma = 1 mg/mL
Rate of urine formation = 2 mL/min
A: 50 mL/min
B: 25 mL/min
C: 200 mL/min
D: 100 mL/min
D: 100 mL/min
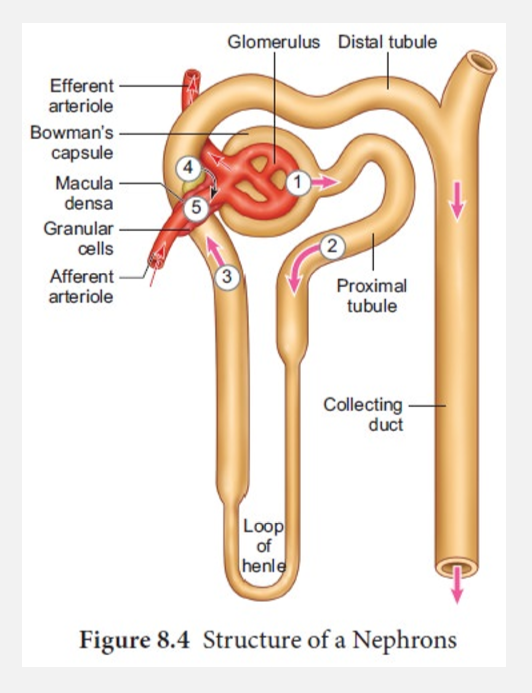
Filtrate, tubular fluid, and urine flow (pt 2)
Tubular fluid
New name for filtrate when enters PCT
Flows through
PCT
Nephron loop
DCT
Enters collecting tubules
Empties into collecting ducts
Enters papillary duct w/in renal papilla; now called urine
Overview of urine formation (pt 2)
Steps of urine formation (continued)
2. Tubular reabsorption
Movement of components w/in tubular fluid
Move by diffusion, osmosis, or active diffusion
Move from lumen of tubules and collecting ducts across walls
Return to blood w/in peritubular capillaries and vasa recta
All vital solutes and most water reabsorbed
Excess solutes, waste products, some water remaining in tubular fluid
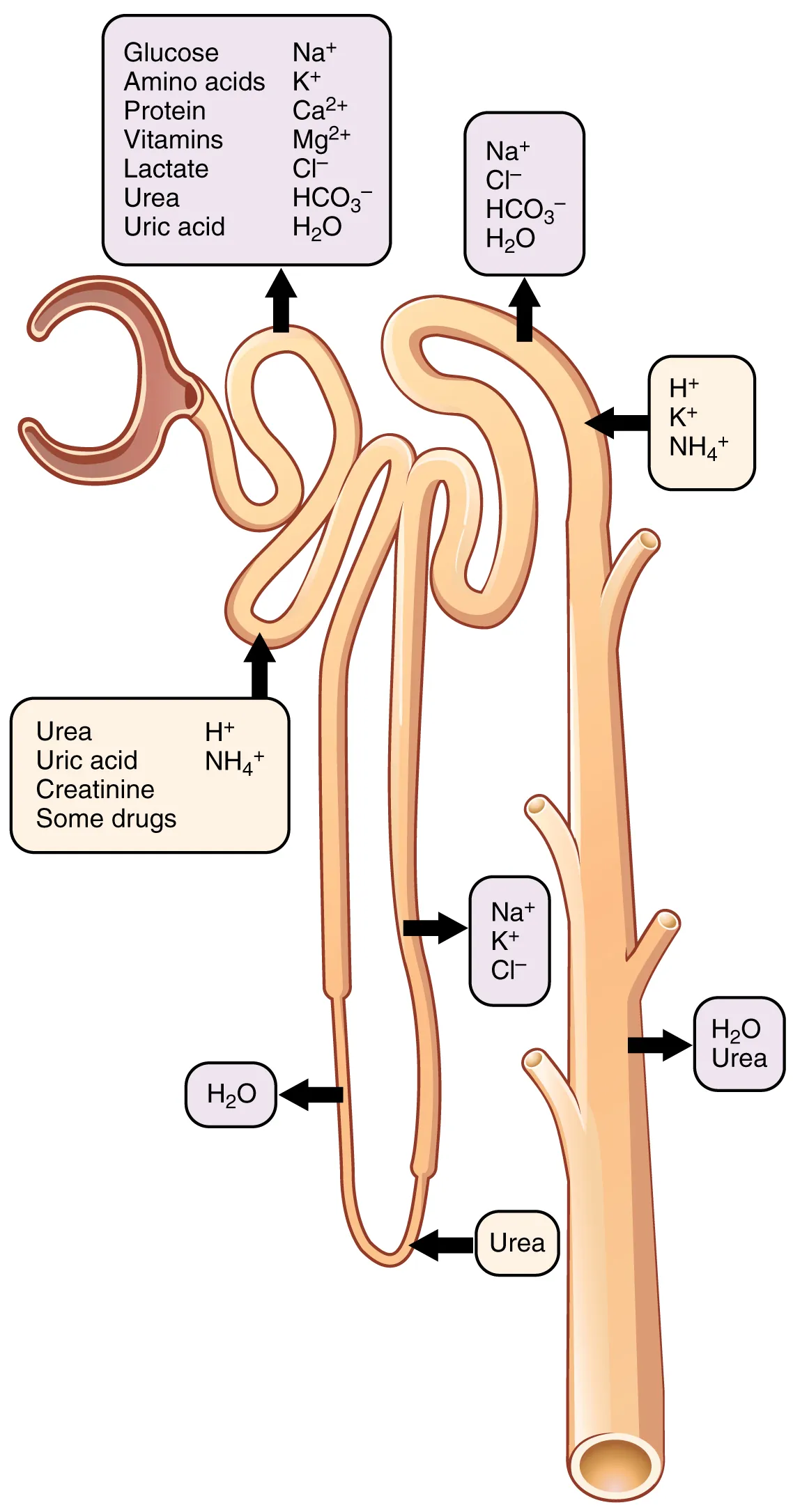
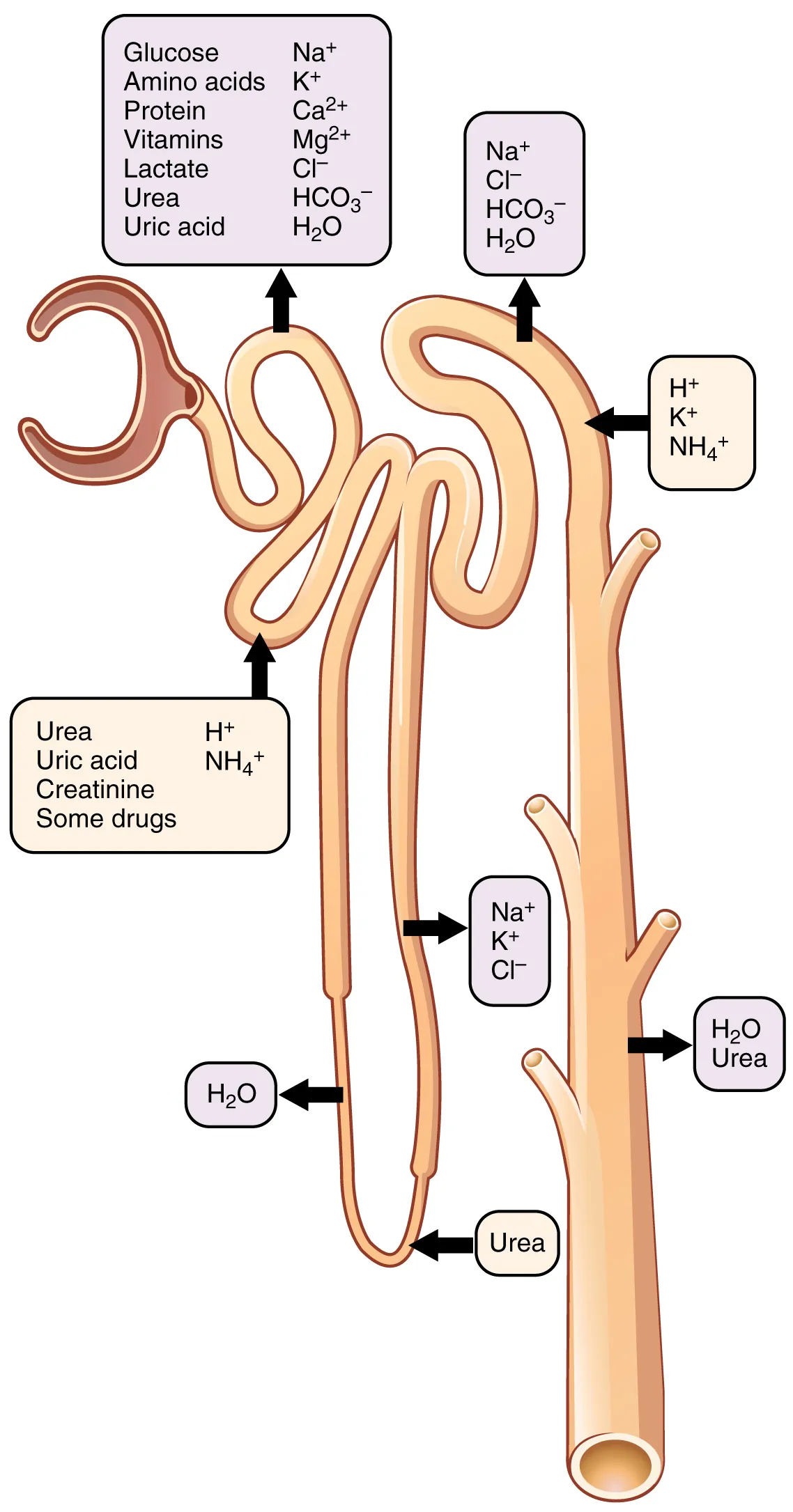
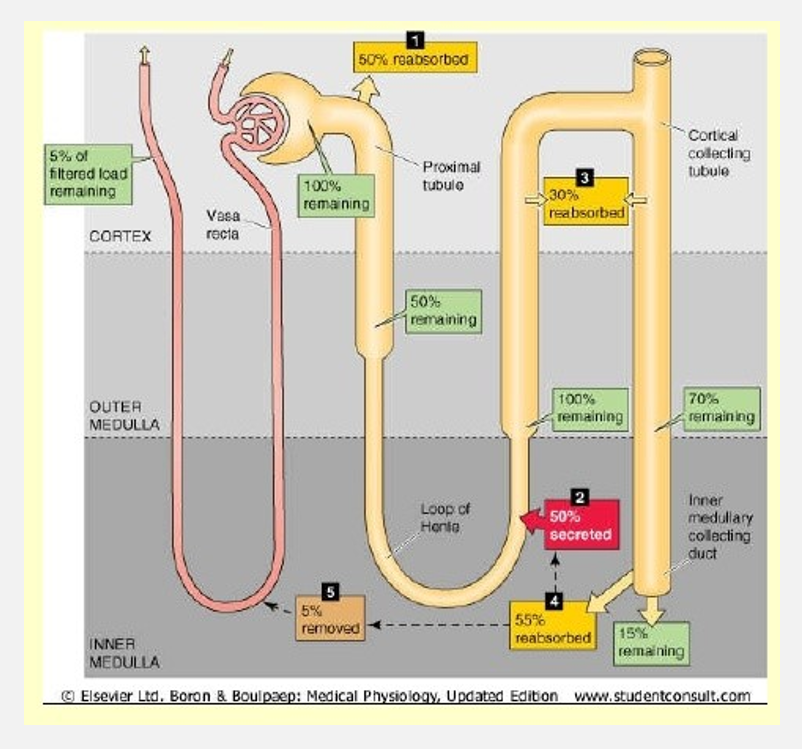
Tubular reabsorption in the collecting ducts and loops
PCT:
Na+ reabsorbed by primary active transport
Glucose, amino acids, proteins, vitamins reabsorbed by secondary active transport
HCO3-, Ca2+, Mg2+, PO43-, K+ also actively reabsorbed
Water and other ions passively reabsorbed by osmosis
Ascending and descending loops:
Majority of remaining water, Na+, Cl- and K+ is reabsorbed
Opposing permeability: descending loop is permeable to water, ascending loop is permeable to solutes
Overview of urine formation (pt 3)
Steps of urine formation (continued)
3. Tubular secretion
Movement of solutes, usually by active transport
Move out of blood w/in peritubular and vasa recta capillaries
Move into tubular fluid
Materials moved selectively into tubules to be excreted
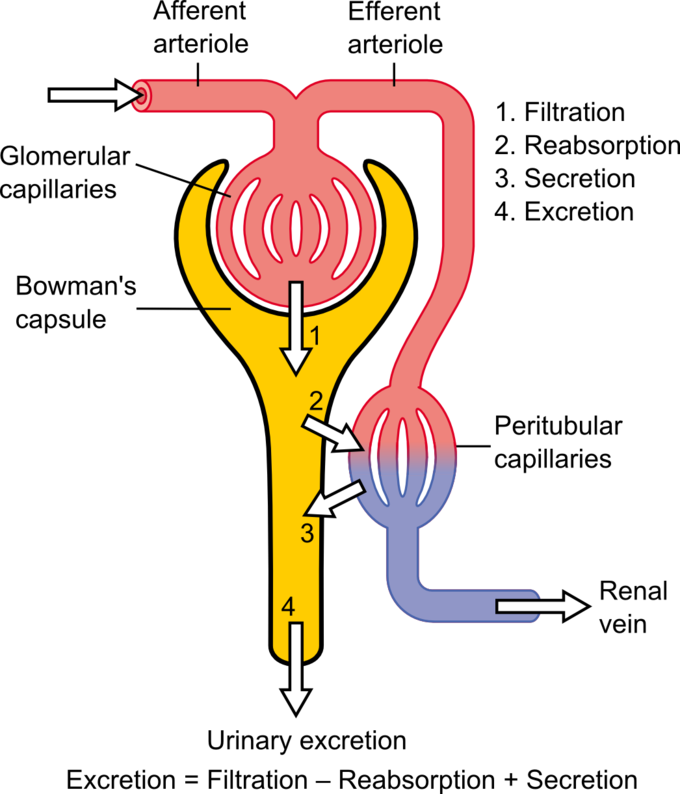
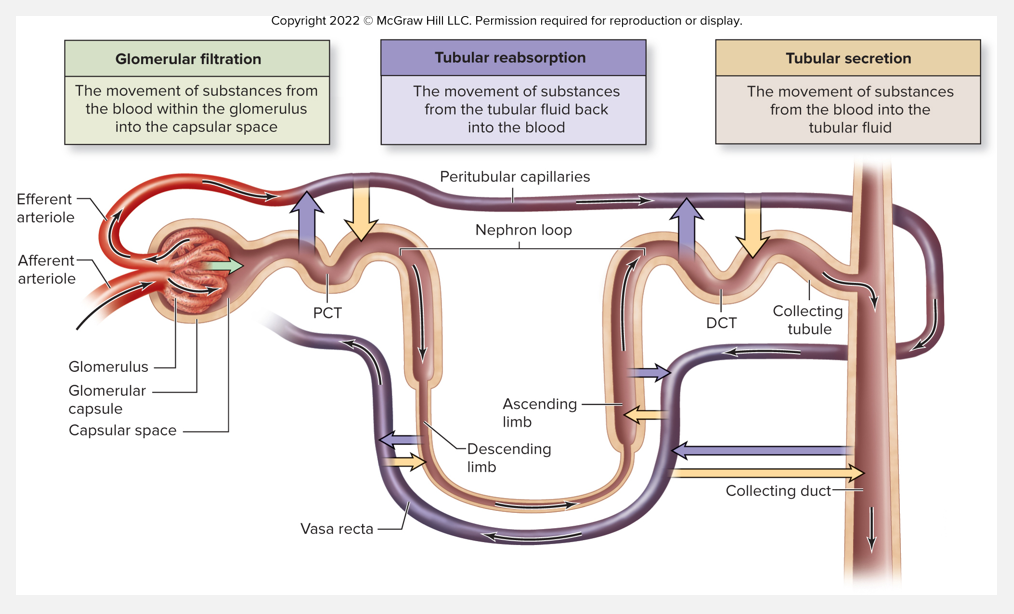
Overview of the processes of urine formation
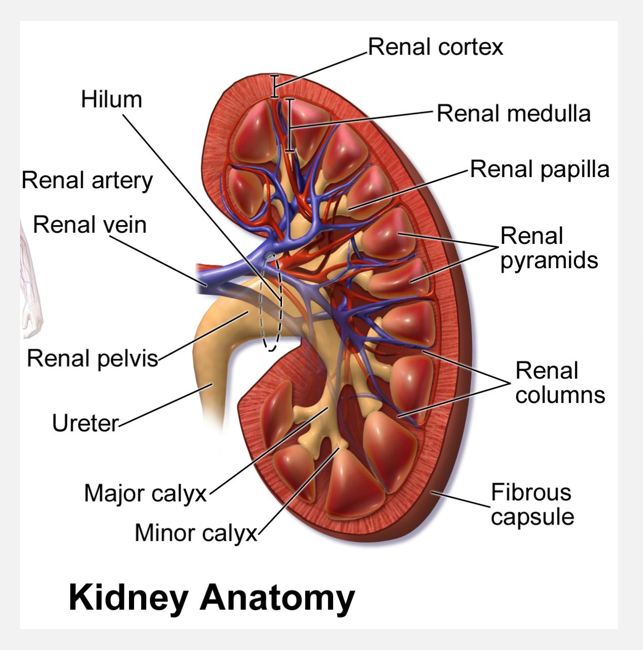
Filtrate, tubular fluid, and urine flow (pt 3)
Urine
Enters papillary duct located w/in renal papilla
Minor calyx—>major calyx—>renal pelvis
Renal pelvis connects to ureter
Ureter connects to urinary bladder
Stores and excretes from body through urethra
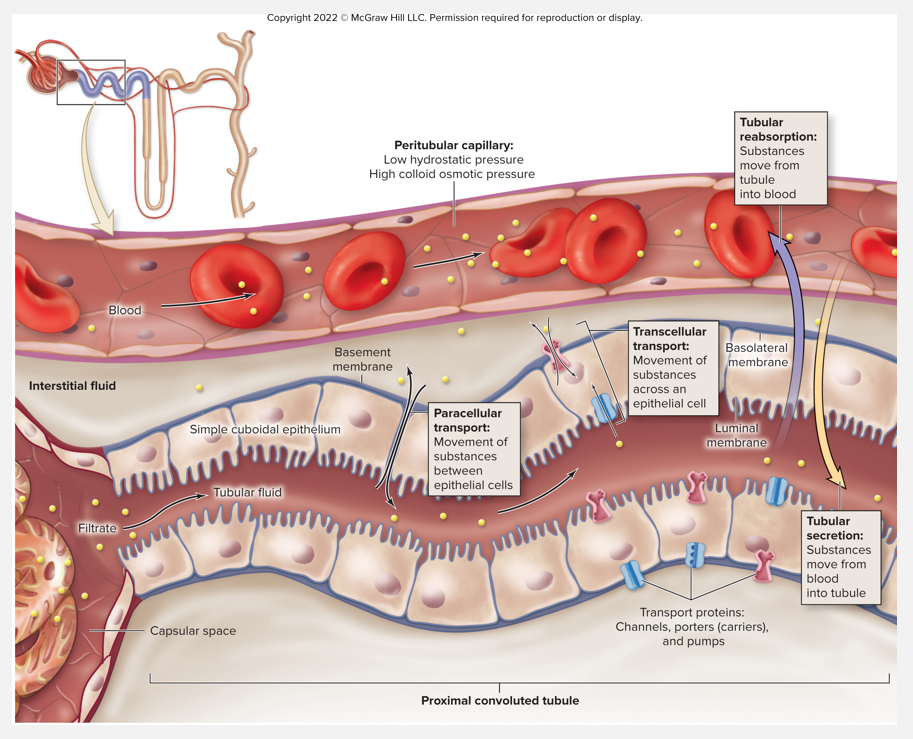
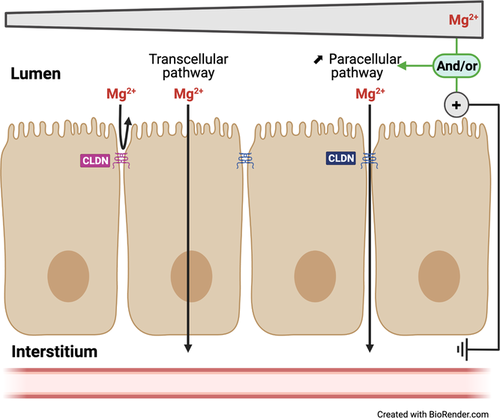
Overview of transport processes (pt 1)
Overview of structures and conditions that influence reabsorption and secretion
Simple epithelium of tubule wall = transport barrier
Paracellular transport
Movement of substances between epithelial cells
Transcellular transport
Movement of substances across epithelial cells
Must cross luminal membrane in contact w/fluid
Must cross basolateral membrane on basement membrane
Order depends on whether being reabsorbed or secreted
Overview of transport processes (pt 2)
Transport proteins embedded w/in luminal and basolateral membranes
Ctrl movement of various substances
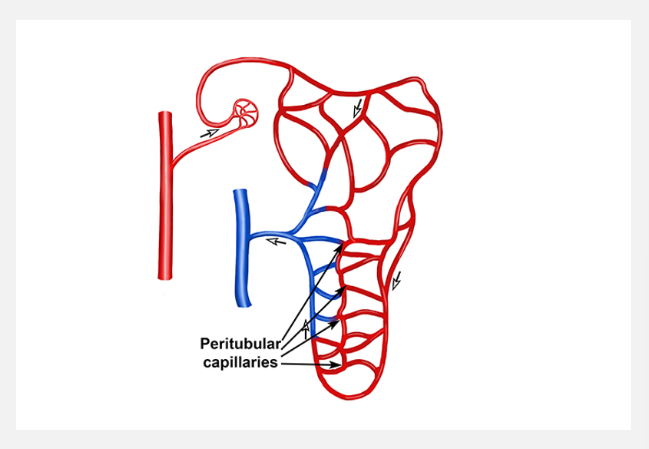
Peritubular capillaries (Vasa Recta)
Low hydrostatic pressure and high oncotic pressure
Facilitate reabsorption of substances through bulk flow
Most reabsorption in PCT
Aided by microvilli increasing surface area
Convoluted tubules and peritubular capillaries
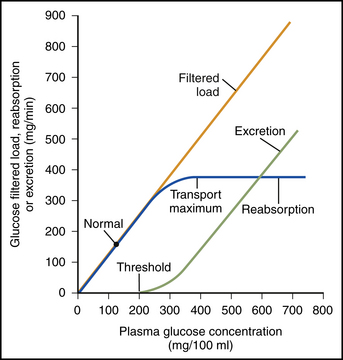
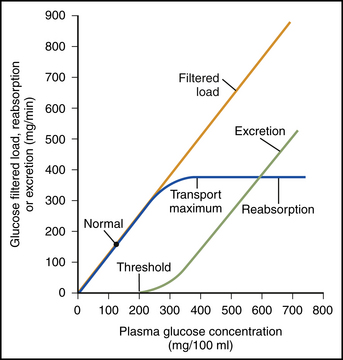
Transport maximum and renal threshold
Transport maximum (Tm)
Maximum rate of substance that can be reabsorbed (or secreted) across tubule epithelium per a certain time
Depends on number of transport proteins in membrane
If no more than 375 mg/min, glucose in tubule all reabsorbed
If greater than 375 mg/min, excess glucose excreted in urine
Renal threshold
Max plasma concentration of a substance that can be transported in the blood w/o appearing in the urine
Renal threshold for glucose = 180 mg/dl
If an ion moves between 2 renal tubule cells to enter the PCT, it is using
A: Autocrine transport
B: Transcellular transport
C: Paracellular transport
D: Symport
C: Paracellular transport
If transport maximum for a molecule is exceeded, that molecule will
A: Be excreted into the urine
B: Be broken down
C: Be absorbed into the Vasa Recta
D: Be kept in tubule cells
A: Be excreted into the urine
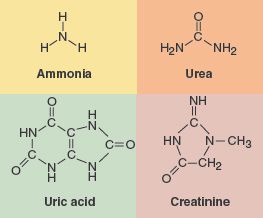
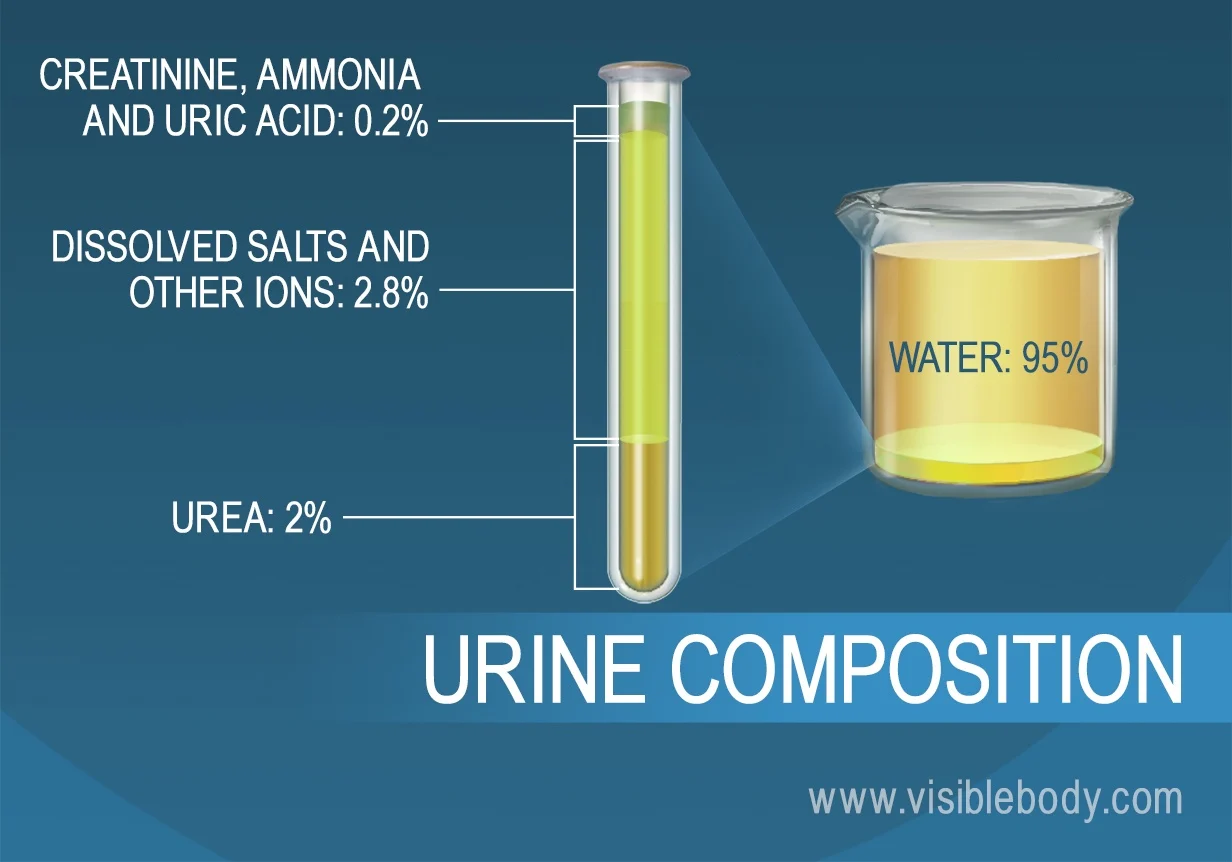
Substances eliminated as waste products (pt 1)
Elimination of nitrogenous waste
Nitrogenous waste: metabolic waste containing nitrogen
Main nitrogenous waste products
Urea, molecule produced from protein breakdown
Both reabsorbed and secreted
50% excreted in the urine
Helps establish concentration gradient in the interstitial fluid
Uric acid, produced from nucleic acid breakdown in liver
Both reabsorbed and secreted
Creatinine, produced from creatinine metabolism in muscle
Only secreted
Substances eliminated as waste products (pt 2)
Elimination of drugs and bioactive substances
Most secretion occurring in PCT
Certain drugs
Ex. penicillin, sulfonamides, aspirin
Other metabolic wastes
Ex. urobilin, hormone metabolites
Some hormones
Ex. human chorionic gonadotropin, epinephrine
Substances eliminated as waste products (pt 3)
Urea recycling
Urea is a toxic chemical at high levels, but moderate amounts can help drive osmotic gradient
Help concentrating process in interstitial fluid
Urea removed from tubular fluid in collecting duct by uniporters
Diffuses back into tubular fluid in thin segment of ascending limb
Remains w/in tubular fluid until it reaches collecting duct
Urea “cycled” between collecting tubule and nephron loop
Ion imbalance can have negative effects on the body (pt 1)
Hyponatremia
Low plasma Na+
Renal disease, congestive heart failure, Addison’s disease
Symptoms are all CNS dysfunction
Hypernatremia
High plasma Na+
Dehydration, vomiting, diarrhea
Symptoms are all CNS dysfunction
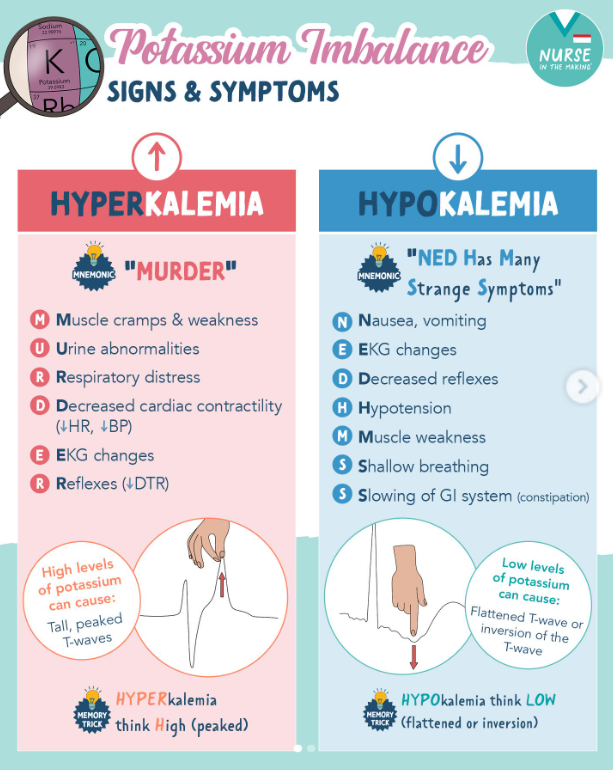
Ion imbalance can have negative effects on the body (pt 2)
Hypokalemia
Low plasma K+
Vomiting, diarrhea, Cushing’s disease
Muscle weakness
Hyperkalemia
High plasma K+
Renal failure, Addison’s disease
Muscle fatigue, heart abnormalities
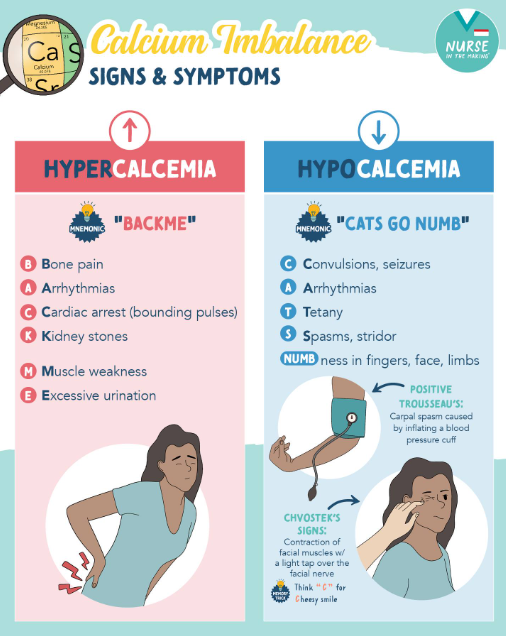
Ion imbalance can have negative effects on the body (pt 3)
Hypocalcemia
Low plasma Ca2+
Muscle stiffness, spasms
Hypotension, heart failure, arrhythmia
Hypercalcemia
High plasma Ca2+
Frequent urination, nausea, vomiting
Muscle weakness, heart abnormalities