accommodation and indirect fusional
1/72
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
73 Terms
Relative accommodation
the total amount of accommodation which the eyes can exert, both relax and stimulate, relative to the vergence system.
Negative relative accommodation (NRA)
the patient's ability to relax accommodation relative to the vergence system
plus, relaxation, PFVBO
During NRA, (plus or minus) lenses are used and (stimulation or relaxation) of accommodation is required to make the target clear. Additionally, (PFVBO or NFVBI) is required to keep the target single.
Positive relative accommodation (PRA)
the patient's ability to stimulate accommodation relative to the vergence system
minus, stimulation, NFVBI
During PRA, (plus or minus) lenses are used and (stimulation or relaxation) of accommodation is required to make the target clear. Additionally, (PFVBO or NFVBI) is required to keep the target single.
blur
indicates the end of fusional reserves and the recruitment of accommodation (relaxation or stimulation) to keep the object single
double
indicates the end of both fusional reserves and accommodation
NRA
should you start with NRA or PRA first to avoid inducing accommodative spasm?
accommodation is limiting
At the end of NRA/PRA, if you occlude one eye and the image remains blurry what does this mean?
vergence is limiting
At the end of NRA/PRA, if you occlude one eye and the image clears what does this mean?
2.50 D
what is the expected value for NRA?
45% of the accommodative amp
what is the test distance for accommodative facility?
30% of the accommodative amp
what is the flipper value for accommodative facility?
32 cm
If a patient has an accommodative amp of 7D, what is the test distance to perform accommodative facility?
+/- 1
If a patient has an accommodative amp of 7D, what is the flipper that should be used to perform accommodative facility?
subjective
what is one disadvantage to accommodative facility testing?
accommodation
While performing accommodative facility testing, if the patient struggles even monocularly, what system is limiting?
vergence
While performing accommodative facility testing, if the patient improves monocularly, what system is limiting?
10-13 cpm
what is the normative value for BAF?
12-17 cpm
what is the normative value for MAF?
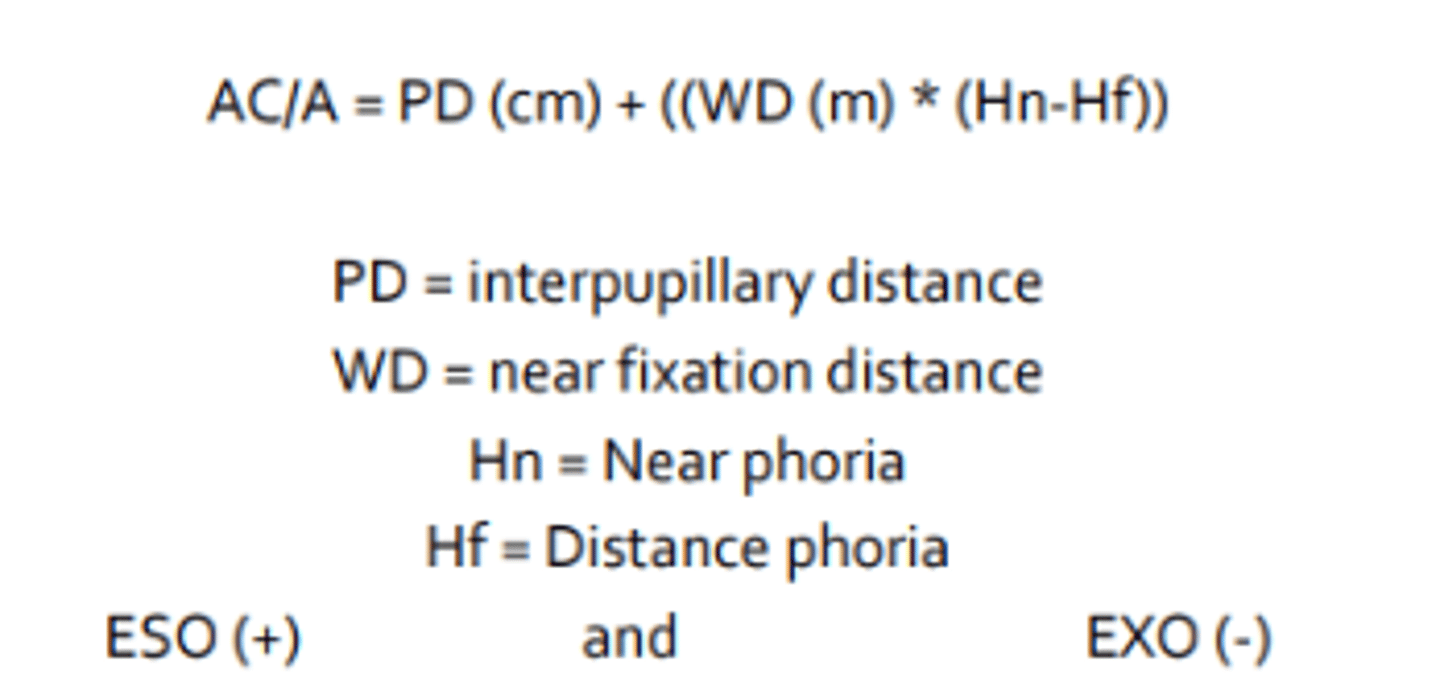
AC/A ratio
the amount of accommodative convergence (in prism diopters) evoked by 1 diopter of accommodation. A fundamental aspect of an individual's oculomotor system.
Calculated AC/A
method of finding AC/A ratio by measuring the change in vergence related to the change in accommodation when fixation is altered from one distance to another
Gradient AC/A
method of finding AC/A ratio by measuring the change in vergence related to the change in accommodation by holding the distance of the target constant, but change the lenses in from of the eyes to change the magnitude of accommodation.
4-6 prism diopters
what is the normative value for AC/A ratio?
presbyopic
AC/A ratio has little value for patients who are...
larger
Because calculated AC/A takes into account proximal convergence, it estimates a (smaller or larger) AC/A
smaller
Because modified gradient AC/A takes into account lag of accommodation, it estimates a (smaller or larger) AC/A
high
A high or low AC/A results in MORE ESO AT NEAR
low
A high or low AC/A results in LESS ESO AT NEAR
Accommodation
The process by which the optical system of the eye varies its focal length in response to visual stimuli by changing the dioptric power of the crystalline lens.
ciliary muscle contracts
ciliary rings moves forward and inward
posterior zonules contract
anterior zolunes relax
lens becomes more spherical increasing in plus power
five steps of accommodation
blur
the initial stimulus for accommodation
retinal cones
during accommodation, defocus stimulates these cells
LGN and visual cortex
during accommodation, after retinal cones are stimulated by blur the signal travels to...
sensory blur signals
during accommodation, after blur reaches the LGN and visual cortex, cortical cells generate...
cerebellum and parietotemporal areas
sensory blur signals generated by cortical cells are transmitted to these areas for processing
midbrain and EW nucleus
after being process in the cerebellum and parietotemporal areas, sensory blur is transmitted to these areas for the formation of motor commands
ciliary muscle via CN 3, ciliary ganglion, short ciliary nerve
name the three sequential destinations of motor commands comming from the midbrain and EW nucleus to cause ciliary muscle contraction
traumatic brain injury
Because accommodation is highly depended on cortical processing, it is often affected by
Tonic accommodation
residual accommodation present in the absence of a blur stimulus. Reflects baseline innervation from the midbrain to the ciliary muscle. Only measurable using special devics in a totally dark room. A typical amount of 1-2 D that reduces with age.
Reflex accommodation
automatic adjustment of accommodation in response to small amounts of blur input (less than 2 D). The largest and most important component of accommodation.
Vergence accommodation
accommodation induced by the neurological linking to fusional vergence. Give rise to the convergence accommodation/convergence ratio The second most important component of accommodation.
Proximal accommodation
accommodation triggered by the influence or knowledge of a near object within 3 m.
Amplitude of accommodation
the full range of accommodation from the far point (minimum accommodation) to the near point (maximum accommodation). If the far point is at infinity (emmetrope or fully corrected ametrope), this value is each to the dioptric value of the near point.
3 months
amplitude of accommodation increases rapidly in the first ____ of life.
6 months
at what age does accommodation become adult like?
55-60 years
around what age does amplitude of accommodation reach zero?
Depth of field
the extent to which an object can be moved toward or away from the patient and still remain in focus
smaller
Depth of field is increased in patients with(smaller or larger) pupils, increasing the amplitude of accommodation
medication use
Pupil size is commonly affected by
monocularly
Accommodation is tested _____ to negate the stimulus of convergent eye movements.
put the far point at infinity
why must habitual rx be worn by the patient during amplitude of accommodation testing?
9.50 D (do not forget to add working distance 40 cm, 2.50 D)
Starting lens: +0.75
After minus lens build up: -6.25
What is the amplitude of accommodation?
high
Uncorrected myope will have an artificially (high or low) amplitude of accommodation
low
Uncorrected hyperope will have an artificially (high or low) amplitude of accommodation
over
Push up method (over or under) under amplitude of accommodation because the target gets larger and easier to see as it gets closer to the patient
under
Minus lens build up method (over or under) estimates amplitude of accommodation because minus lenses minify the target making it more difficult to see
pull away
what is the best method of choice for measuring amplitude of accommodation?
15-0.25(age)
what is the equation for minimum amplitude of accommodation?
18.5-0.3(age)
what is the equation for the average amplitude of accommodation?
25-0.40(age)
what is the equation for the maximum amplitude of accommodation?
double
In order for a patient to focus compfortable up close, the amplitude of accommodation should be ______ the accommodative demand.
Accommodative accuracy
the behavior of the patient's accommodative system when an actual near task is being carried out
Lag
less accommodation than what is needed is being employed initially. It is normal for there to be a lack of accommodative response of about 0.50 D
Lead
more accommodation than what is needed is being employed initially
lead (due to pupil constriction and increased depth of focus)
very dim lighting during FCC is important to avoid measuring an artificial...
plus, lag
During FCC, what lens is needed if the horizontal lines appear clearer first? Does this represent a lag or a lead?
minus, lead
During FCC, what lens is needed if the vertical lines appear clearer first? Does this represent a lag or a lead?
harmon distance
distance from middle knuckle to elbow. Used for determining working distance when performing MEM on children.
plano to +0.50 lag
what is the normative value for FCC?
plano to +0.75
what is the normative value for MEM retinoscopy?
accommodative insufficiency
low muscle tone of ciliary body
presbyopia
high ESO with little NFV
a large lag of accommodation can indicate these four conditions
accommodative spasm
accommodative excess
large EXO with little PFV
A large lead of accommodation can indicate these three conditions