Looks like no one added any tags here yet for you.
How much water weight are humans
50-60%
What determined body water as fraction of weight
muscle and fat
fat has very little water, muscle has most water weight
as we age we loose muscle mass (65% as infants and 46-52% when 60+)
women have less muscle = less body water mass
Most important determinants of body water weight
age
sex
fat %
3 places water is found
interstitial space
inside cells
inside vascular spaces
Distribution of body water - where is it found the most?
2/3 is intracellular
1/3 is extracellular (80% of this interstitial fluid and 20% in plasma)
Aquaporin
integral membrane proteins
channels for rapid movement of water across all plasma membranes
10 types in humans, but 5 types in the plasma membranes of PCT cells
discovered in 1990
Osmotic force
movement of water across plasma membrane in response to osmotic gradient
moves from high to low osmolarity
Where is sodium most abundant
plasma and intertitial space
Where is potassium most abundant
cells
What happens to ICF and ECF volumes if we drink water
water is absorbed from gut into ECF
ECF sodium osmolatity is lowered via dilution
water will move from ECF to ICF to normalize
both volumes increase and cell will increase because it is growing with water inside
what happens to ICF and ECF if we eat salt
sodium will increase in ECF and stay there because it does not normalize like water
water will move from ICF to ECF to normalize
ICF volume decreases and ECF volume increases
cells shrink
Leaky exchange epithelium
allows for movement through gaps between the cells
water can move across from ICF to plasma inside vessels between these pores
what determines ICF and Plasma volume and their relationship
NOT solutes and osmolality
Starling forces: hydrostatic (heart) pressure and oncotic pressure (albumin)
capillary permeability to water
Albumin
main protein in plasma
capillaries have limited permeability to it because it has high molecular weight
provides oncotic pressure in plasma > ISF
Fluid Flux
Permability X (hydrostatic pressure - oncotic pressure gradients)
Jv = Kf(delta P - delta pi) → this is how it looks
How much does kidney filter each day
144 litres via plasma (at 1L/min total and 500ml/min per kidney)
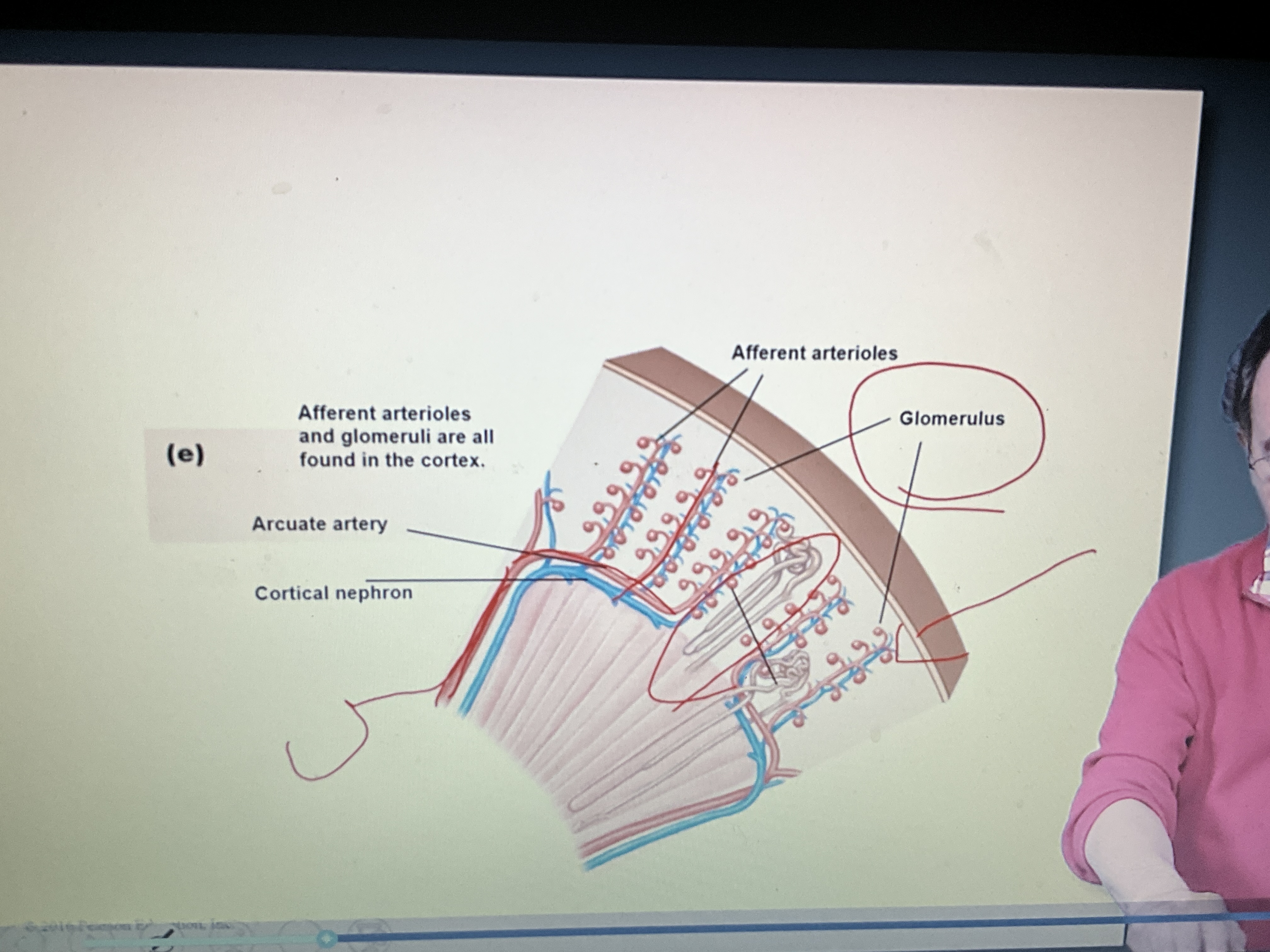
How is a kidney structured
increasing complexity from middle outwards
filtration takes place along perimeter of kidneys inside
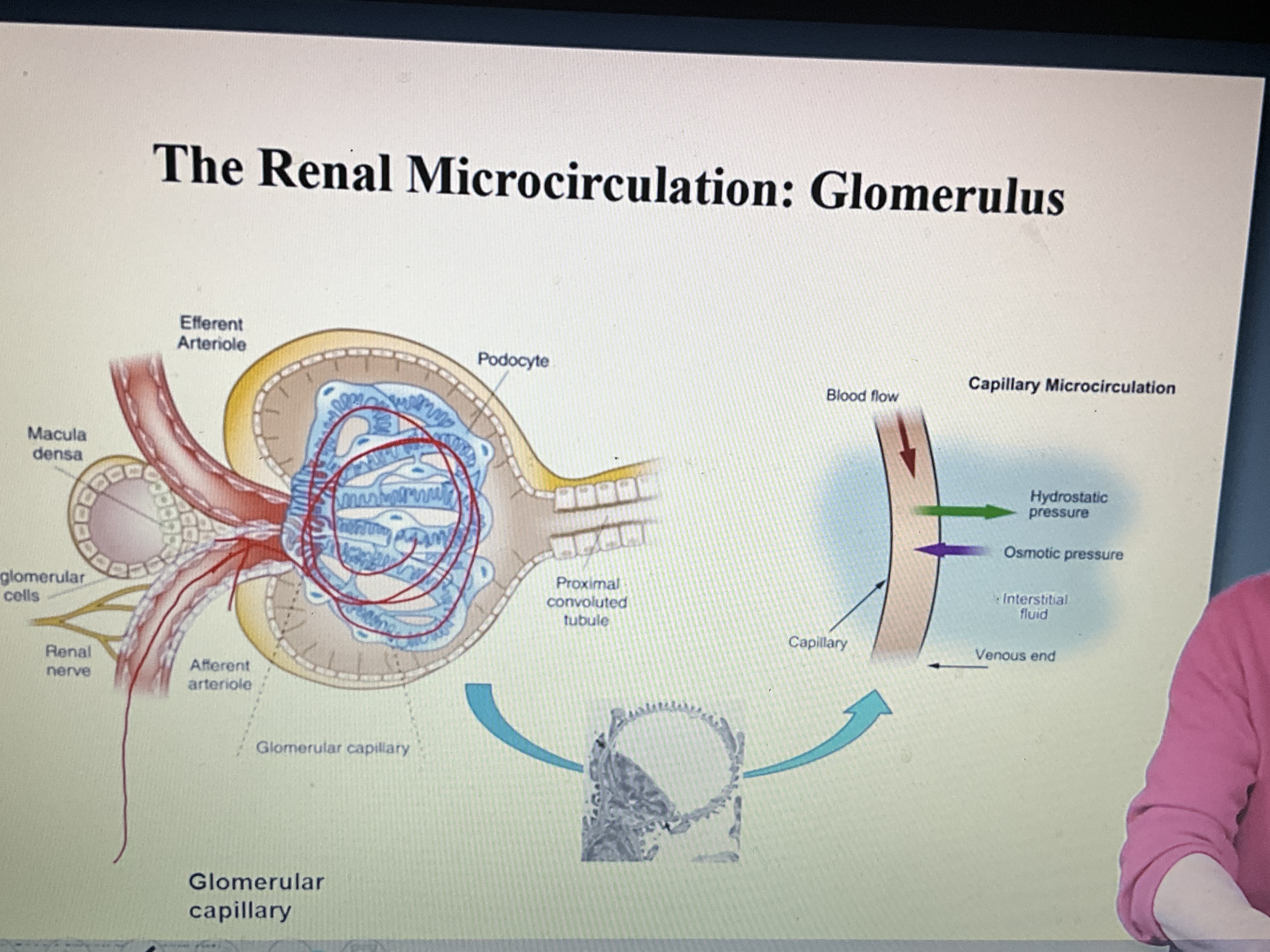
Glomerulus
allows transfer from plasma in capillary to intersistial fluid
forms an ultra-filter, many found in each kidney which filter plasma
Starling forces that governing movement of water from capillary to bowmans space
Glomerular Capillary pressure (PGC)
Tubular Hydrostatic pressure (PT) - PUSH water into bowmans space
Oncotic Pressure - KEEP water in capillary space
Ultrafiltration Coefficient (Kf)
Plasma Flow (QA) - maintaining starling forces
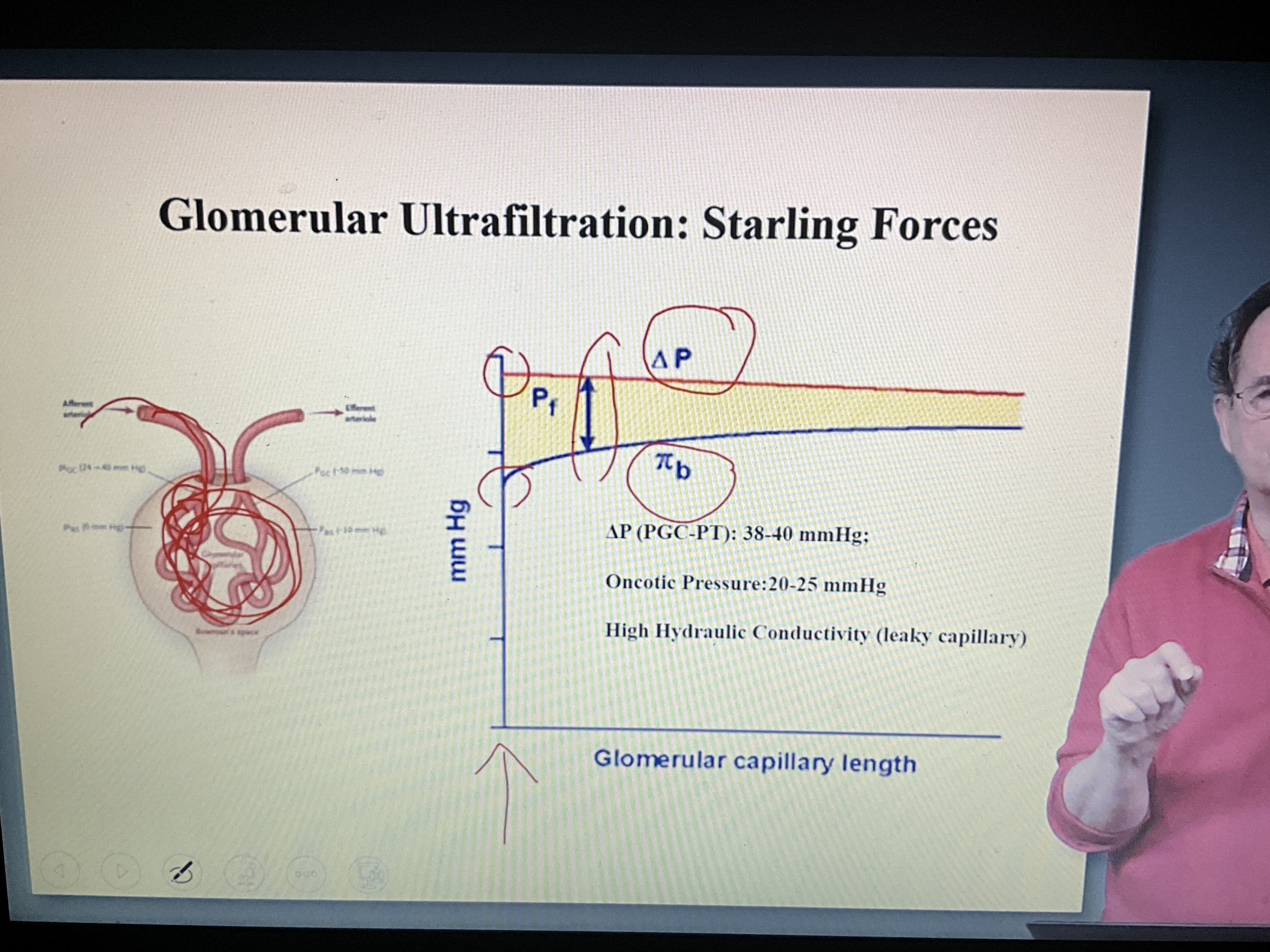
Hydrostatic Pressure Gradient
difference between hydrostatic pressure between capillary and bowmans space
drives ultrafiltration
Oncotic pressure
serves to hold water in capiilaries
water retention
Glomerular filtration rate
Calculated as Permeability X Ultrafiltration pressure
filter 150-180 litres per day which is 100-125 ml/min
What are the determinants of glomerular filtration rate (GFR)
Plasma flow
required for filtration
as it increases, GFR increases but there is a limitation on plasma flow so it will plateau
Hydrostatic pressure
must exceed oncotic pressure for filtration (20 mmHg)
positive relationship after 20 mmhg
Oncotic pressure
negative relationship
ultrafiltration coefficnet
positive relationship
but there is a limitation where it wont increase GFR anymore
what is the most important determinant of GFR
renal blood flow (plasma flow)
this is determined by blood pressure and renal vascular resistance
autoregulation of renal blood flow
blood flow is relatively constant (70-150 mmHg)
efferent circulation can change resistance based on blood pressure (myogenic reflex)
will dilate if BP drops and constrict if it increases
Tubulo-glomerular feedback
when there is too much sodium in tubule, adenosine is released which activates receptors and causes vasoconstriction to reduce GFR
Angiotensin II
hormone that increases the resistance in the efferent arteriole
this decreases renal blood flow but increases GFR because of the hydrostatic pressure buildup
Convection
movement of small solutes with bulk flow of water
Freely filtered
filtered with the water
includes sodium, potassium, chloride, glucose, bicarbonate, urea and creatine
makes the concentration equal in both capillary and bowmans space
bigger molecules like albumin cannot move across the membrane (perm-selectivity) which protects against their loss
movement of macromolecules from kidney capilalries to bowmans space
determined by weight and protein charge
15 kDa is the cutoff for free-filtration
albumin is rarely excreted - very little is lost per day
What is the significance of glomerular filtration rate
measures kidney function
kidney disease affect GFR
How to we measure GFR
we essentially use a molecule we know is freely-filtered then we can measure the amount filtered in a specific unit of time by looking at concentration in urine
Inulin is used in laboratory because it wont be reabsorbed in the tubules so 100% of the amount excreted in the amount filtered
however it must be given intravenously in a lab
Creatinine is used in medical practice to measure GFR
end product of energy metabolism in muscle cells
relatively constant depending on muscle mass and there is very limited excretion
How do we measure creatinine clearence
Urine flow rate (v/min) X Ratio of [urine creatinine] to [plasma creatinine]
Relationship between GFR and Pcreat
inversely proportional
how do we assess perm-selectivity
measure total protein or albumin in urine over 24 hours
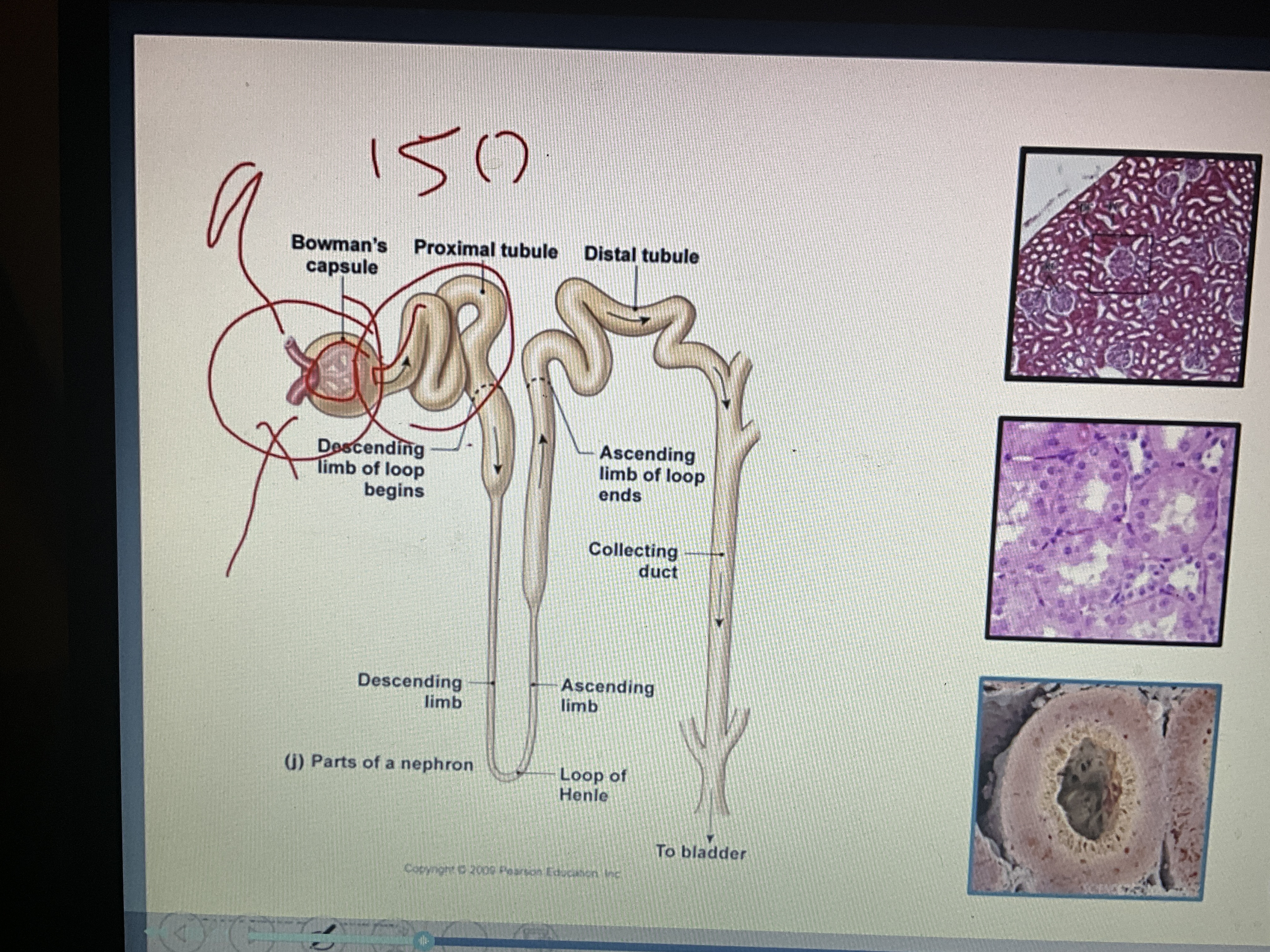
Anatomy of Nephron
bowmans capsule
proximal tubule
loop of henle
distal tubule
collecting duct
goes to bladder
normal urine volume
0.5-2 L/day
depends on how much you drink
99% of filtered water is reabsorbed
how much sodium do you filter, excrete and reabsorb each day
filter 22,500 mmol
excrete 150 mmol
99% reabsorbed
Na-K-ATPase
maintains sodium-potassium gradient
located on basolateral membrane of cells
Sodium Hydrogen Exchanger (NHE)
Na into cell and hydrogen out
allows for sodium reabsorption by allowing it to go into the proximal tubule cell then be pumped into interstital fluid by ATP-ase
Epithelial Sodium Channel (ENaC)
allows sodium to move in and out of cell for reabsorption and excretion
proximal tubule cell
always low sodium to maintain gradient and be able to pump sodium into interstitial fluid to allow sodium to be reabsorbed
Proximal tubule
located immediately after bowmans capsule in nephron
site of most reabsorption of water and solutes
2/3 of all reabsorption
uses sodium-hydrogen exchanger (NHE3)
bicarbonate reabsorbtion
glucose, AA, and phosphate cotransporters only found here
very leaky
Thick Ascending Limb of Henle (the part that goes back up)
20-30% sodium reabsorbtion
NKCC2 kumenal transport protein
inhibited by furosemide by displacing one of the chlorides
impermeable to water
fluid that leaves is hypotonic
Distial Tubule
located after loop of Henle in nephron
reabsorbs 5 to 10% of filterred sodium and water
uses NCC transporter
inhibted by thiazides
less potent than furosemide
important in urinary dilution
Collecting duct of nephron
last step before bladder
reabsorbed 1-3% of sodium
uses ENaC transporter
more aldosterone-receptors
Vasopressin receptors increase water reabsorption
facilitates potassium secretion
low capacity for transport but can generate large concentration gradient
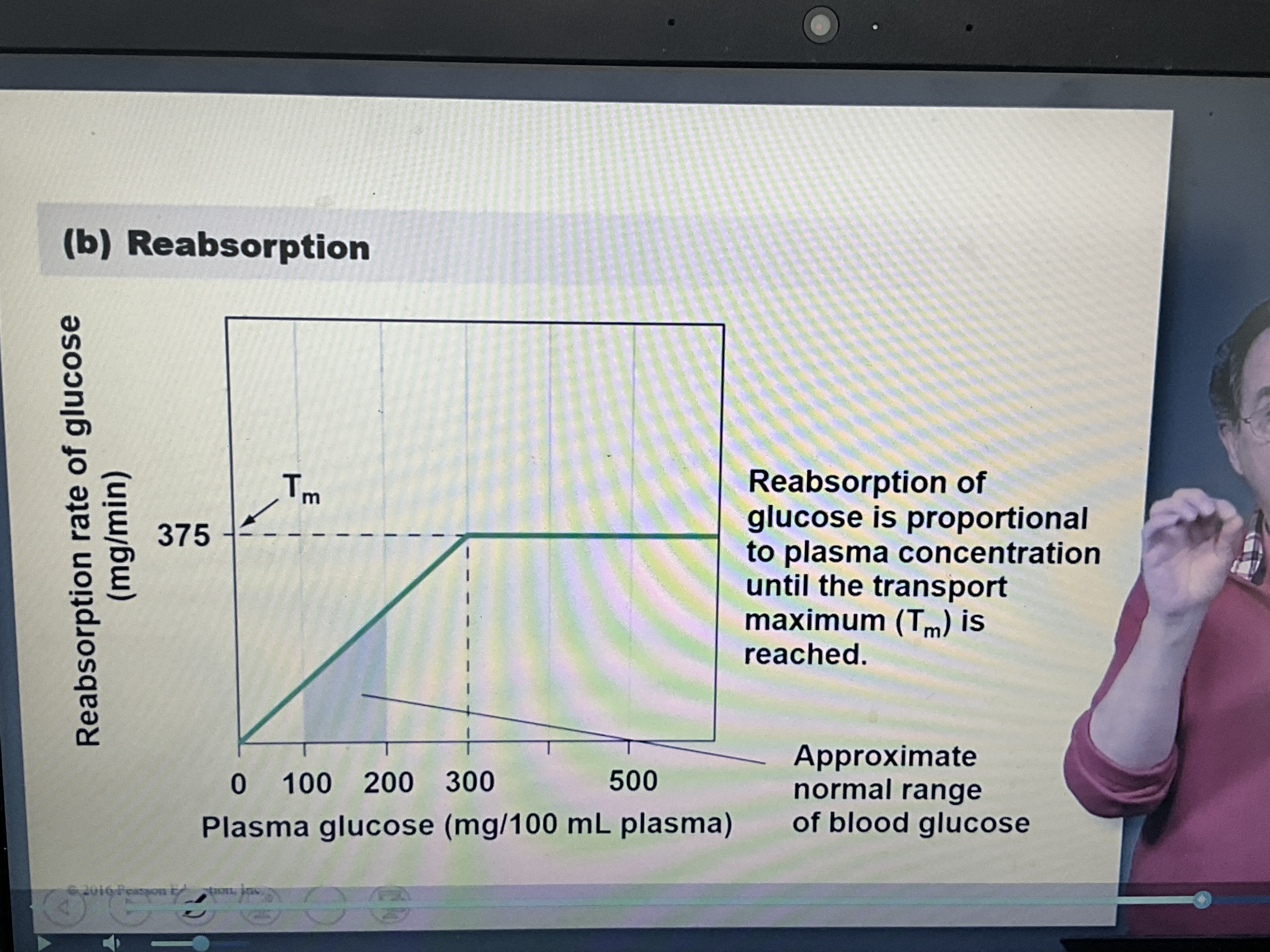
Relationship between reabsorption rate of glucose and Plasma glucose
positive relationship until you reach maximum, then it plateaus
Renal Threshold
This is the threshold of plasma glucose concentration in which the body can no longer reabsorb the amount lost and we start to have a net loss of glucose in urine
normally we are under the threshold, we don’t want to start loosing glucose because its valuable
Sodium-glucose cotransporters
avoid the loss of glucose in urine (600 cals/day)
where are receptors that regulate sodium levels located
vascular compartment
Water gained and lost in the body
Gained
2.2 L/day from food and drink
0.3 L/day from metabolism
Lost
0.9 L/day from skin and lungs (sweat and water vapour in breath)
1.5 L/day in urine
0.1 L/day in feces
2.5 L/day in and out
where are sensors for water balance located?
inside cells in the intracellular fluid - the volume inside cells tells us water need
(grape vs raisin)
what two nuclei in the hypothalamus play a role in water balance and what do they do
Suprasotic nucleus (SON)
Paraventricular nucleus (PVN)
they signal to posterieur pituitary for release of hormones and send signals to areas of hypothalamus that regulate thirst
Hypothalamic Osmoreceptors
cells in anterior hypothalamus
stretch-inhibited cation channels
the cells that regulate water balance
when the cells shrink which causes the channels to open and depolarize cell (causing action potential)
leads to increased AVP (arginine vasopressin) release and thirst
Vasopressin (AVP, ADH)
main hormone responsible for water balance
increases when high osmolality is sensed, which indicates not enough water present to dilute solutes
decreases when there is low osmolarity, indicating the cells have enough water
directly related to level of thirst as well