Biopsychology
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
Nervous System AO1 - Structure
Specialised network of cells, based on electrical and chemical signals. It collects, processes and reponds to info in the environment and coordinates the working off different cells and organs in the body.
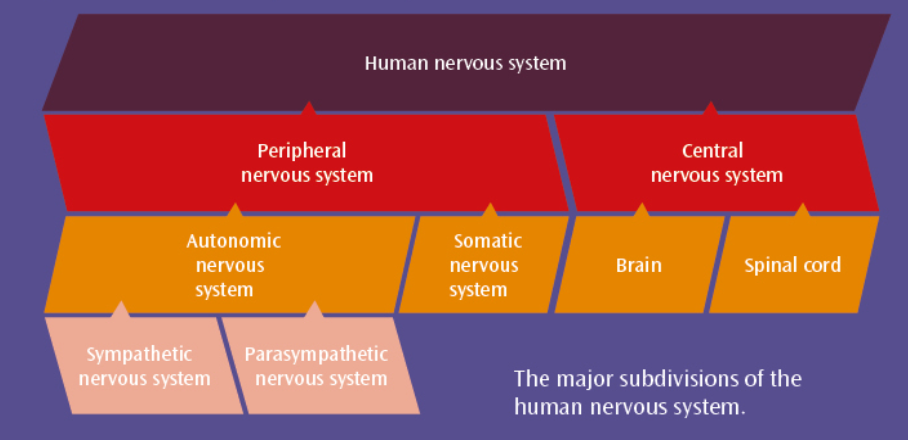
Nervous System AO1 - Definitions
CNS – Brain and Spinal cord. All complex commands and decisions.
PNS – Sends messages from CNS to muscles, glands.
SNS – Sends information from receptor cells in sense organs to CNS. Receives info from CNS that directs muscles to act.
ANS – Transmits info to and from internal organs involuntarily. 2 divisions (sympathetic/parasympathetic).
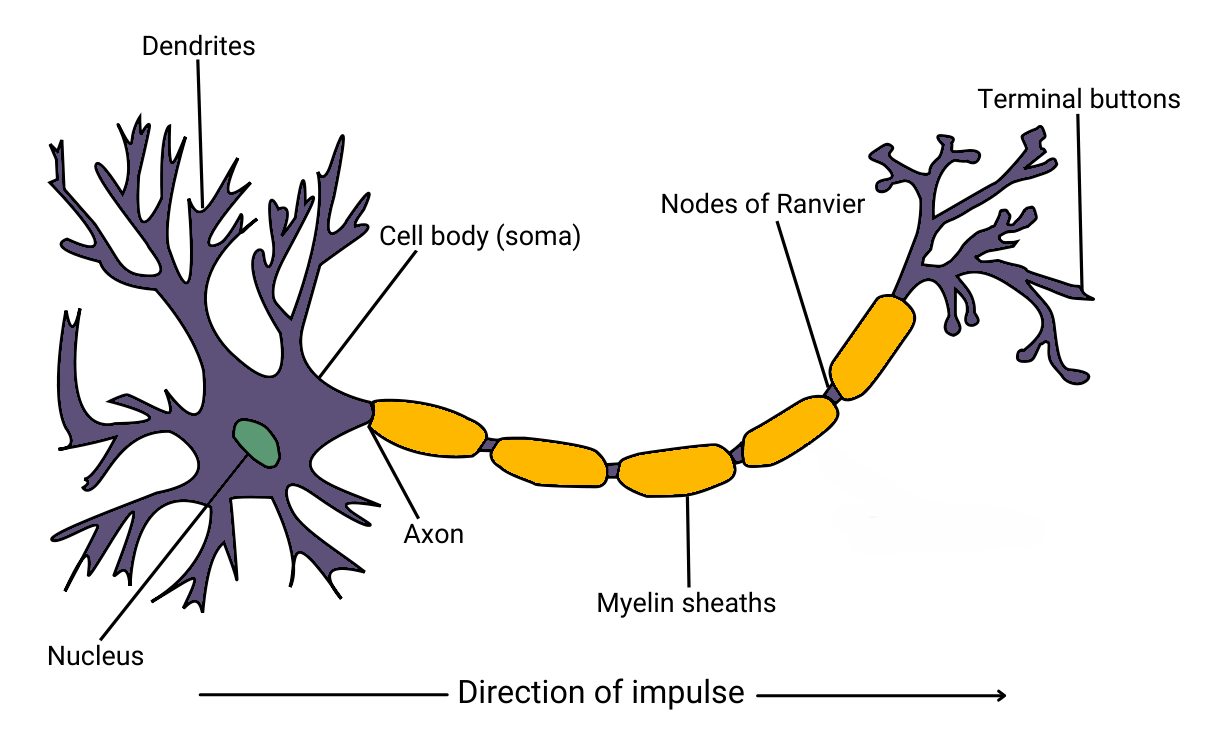
Nervous System AO1 - Neuron Structure
1) Cell Body: Includes nucleus, contains genetic material of cell.
2) Dendrites: Branch like structures protruding from cell body. Carry nerve impulses from neighbouring neurons towards cell body.
3) Axon: Carries impulse away from cell body down length of neuron
4) Myelin Sheath: Fat layer that protects Axon
5) Nodes of Ranvier: Segments myelin sheath to speed impulse transmission across axon
6) Terminal Buttons: End of axon, connects to next neuron.
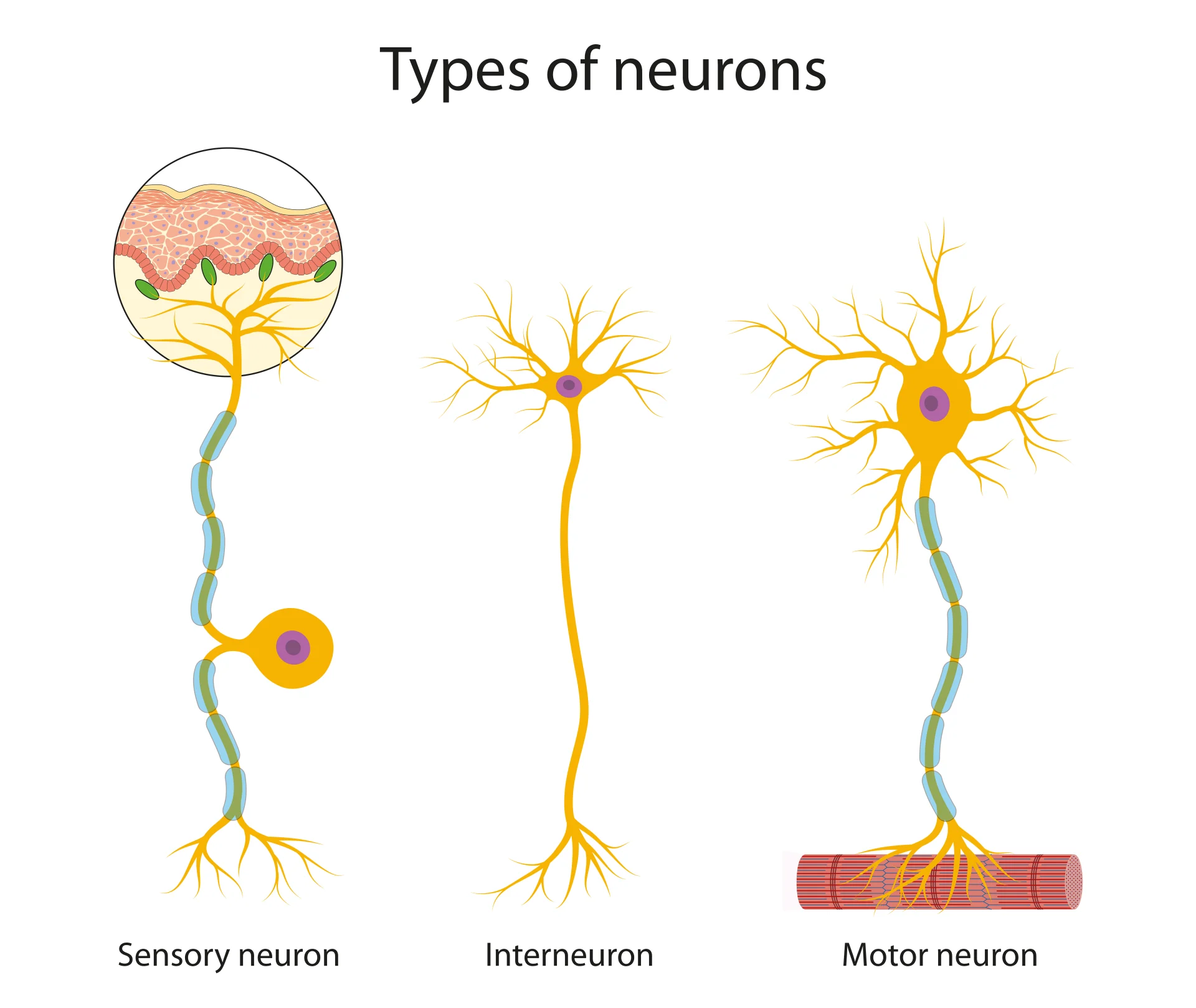
Nervous System AO1 - Types of Neuron
1) Sensory: Carry signals from receptors to spinal cord, LONG Dendrites, SHORT Axons
2) Relay: Connect sensory neuron to other relay/motor neurons. SHORT Dendrites, SHORT Axons.
3) Motor: Carry signals from CNS to effectors, SHORT Dendrites, LONG Axons
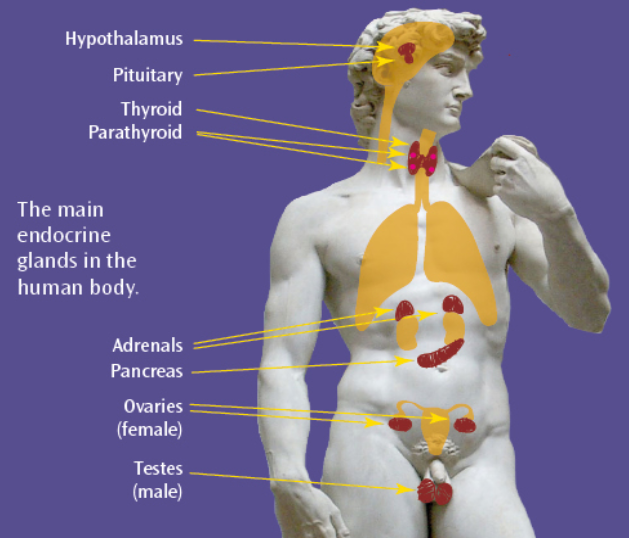
Endocrine System AO1 - Structure
Glands instructed to release hormones into bloodstream, carried towards target organs. Works alongside nervous system to control vital bodily functions. Causes slower, gradual, longer effects.
Endocrine System AO1 - Definitions
Gland – Organ that synthesises substances e.g. hormones.
Hormone – Biochemical substance that circulates through bloodstream affecting target organs. Strong and large quantity produced quickly, quickly dissipates.
Fight/Flight – Stress response, triggers adrenal glands to release adrenaline. Gives readiness to fight/flee an aggressor.
Adrenaline – Hormone released by adrenal glands, part of immediate stress response system. Strongly affects cardiovascular system’s cells (stimulates heart rate, contract blood vessels, dilate air passages).
Fight/Flight Response - AO1
Combinations of endocrine/ANS. Body recieves stressor, Adrenal medulla releases adrenaline into blood (acute sympathetic response)
Sympathetic state: + heart rate, + breathing rate, dilated pupils, - digestion, - salivation, contracts rectum.
Stressor passes = parasympathetic system returns body to resting state.
Parasympathetic state: - heart rate, -breathing rate, constricted pupils, + digestion, + salivation, relaxes rectum.
Synaptic Transmission AO1
Signals transmitted chemically between synapses. Neurotransmitters released from vesicles in presynaptic neuron terminal.
Cross gap, converts back into electrical impulses at postsynaptic receptor sites on dendrites.
Can cause inhibition (negative charge, less likely to fire e.g. serotonin) and excitation (positive charge, more likely to fire e.g. adrenaline)
Fires depending on summation (overall charge).
Localisation AO1 (1)
H - Functions are distributed across the whole brain
L - Specific areas of the brain control different functions.
Cerebral Cortex - Outer Layer of each hemisphere
Motor Cortex (frontal lobe) - Voluntary motor control
Somatosensory Cortex (parietal lobe) - Sensory info from skin, spatial awareness
Visual Cortex (occipital lobe) - Colour, shape, movement
Auditory cortex (temporal lobe) - Speech analysis, volume, tempo, pitch
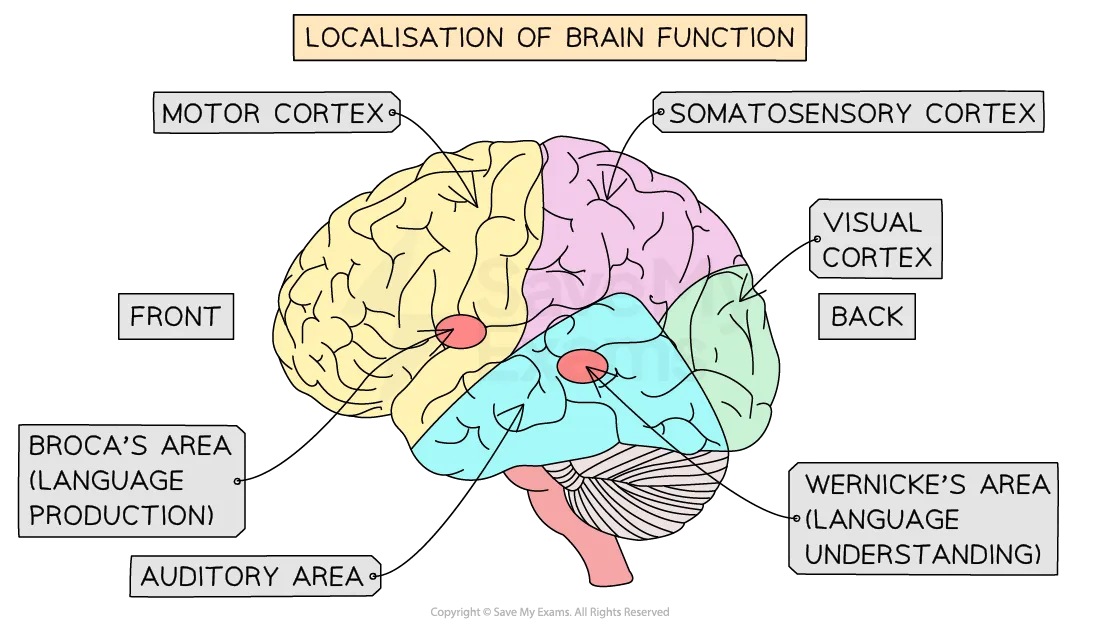
Localisation AO1 (2)
Broca’s area (left frontal lobe) - Language production & understanding. Damage = Broca’s aphasia = slow inarticulate speech.
Patient Tan: Could understand language, unable to produce words.
Wernicke’s area (left temporal lobe) - Language comprehension.
Damage = Wernicke’s aphasia = Fluent meaningless speech
Localisation AO3 – Evidence from neurosurgery (STR)
Damage to specific areas linked to mental disorders.
Neurosurgery last resort method e.g. Cingulotomy isolates cingulate gyrus, implc OCD
Dougherty et al (2002): 32 week follow-up on 44 patients; 30% success, 14% partial.
Localisation AO3 – Evidence from brain scans (STR)
Petersen et al (1998): PET to demonstrate WA active during listening task, BA active during reading task.
Buckner and Petersen (1996) PET, Episodic/Semantic memory in opposite sides of prefrontal cortex.
Scientific evidence for localisation.
Localisation AO3 – Animal Studies (LIM)
Lashley (1950) – Removes 10-50% cortex of rats that were learning maze route. No area proved more important than another. Learning seemed to req the whole cortex.
Suggests holistic function of the brain.
Localisation AO3 – Language (LIM)
Language might not just be in BA & WA.
Dick and Tremblay (2016): 2% modern researchers agree with just BA WA.
High clarity fMRI scans -> Langauge more holistically distributed, in subcortical reigons e.g. thalamus.
Contra localisation theory.
Lateralisation AO1
2 Halves of the brain = functionally different, distinct.
LH controls right, RH controls left.
RH specialised for perception: Visuospatial, Artistic, Facial Recog, Emotion
LH specialised for language: symbolic/logical linguistic expression, mathematical ability.
Joined by Corpus Callosum, thick bundle of nerve fibres allowing communication. If severed, independent function.
Lateralisation AO3 – Connected brains (STR)
Research shows LH RH process info differently.
Fink et al (1996) – PET scans for visual processing task. RH more dominant globally (whole forest). LH more dominant for finer details (trees).
Lateralisation part of both connected and split brain.
Lateralisation AO3 – One Brain (LIM)
Idea of LH analyser, RH synthesiser maybe incorrect.
Nielsen et al (2013) – Analysis of >1000 scans age 7-29. Certain hemispheres for certain tasks, but no evidence of dominant side.
Notion of Left/Right brained = wrong.
Split Brain AO1 (1)
Corpus Callosotomy severs connection, last resort for epilepsy (excessively firing brain cells contained to one side).
Sperry (1968) - Quasi experiment, 11 patients vs 11 intact non-epileptic ptcps.
Lab experiment, highy standardised, specialist equipment.
Subject - 1 eye blinded, gae at fixation point, middle of screen. Slides projected onto either side for 1/10sec (eye movement not spread to both H) → only 1 VF (H) recieves info.
Split Brain AO1 (2)
1) Vision: Object in LVF (RH) not described, drawn with left hand. Object in RVF (LH) described.
2) Touch: Object in left hand (RH) recognised, even though nothing seen.
Object in right hand (LH) not recognised, even though seen and descibed.
3) Composite Words: Word on left and right.
Could identify left word by touch but not seen (LVF, RH), could see right word (RVF, LH).
4) Matching Faces: Pictures shown in LVF (RH) were matched. Ignored and not matched in RVF (LH)
5) Emotion: Nude pin-up shown in LVF (RH). Saw nothing, but giggled and blushed.
Split Brain AO3 – Research Support (STR)
Gazzaniga showed split brain > connected brain on some tasks. E.g. faster at finding odd one out in array of similar objects.
Kingstone et al (1995): LH better cog strategies ‘watered down’ by inferior RH.
Supports Sperry’s distinct Left/Right brain.
Split Brain AO3 – Generalisation (LIM)
Sperry causal relationships hard to establish.
Control group were neurotypical, did not have epilepsy. Major confounding variable (differences may be epilepsy, not split brain).
Unique features of ptcps cog abilities may be epilepsy > split brain.
Plasticity AO1 (1)
Neural Plasticity - Brain’s tendency to change, adapt (functionally, physically). Result of experience, new learning. Synaptic connections form and prune.
Rapid growth in no. synaptic connections. Peaks at 2-3 years (2x adult brain).
Unused connections deleted as we age, frequently used connections strenghtned.
Brain in continual state of change (early years = growth, adulthood = refinement).
Plasticity AO1 (2)
Hippocampus - Small comp of brain, in each H, deep in temporal lobe, central to spatial memory.
Maguire (2000) - Investigate role of Hippocampus in spatial memory.
Quasi, measuring Hippocampi volume (right, left, anterior, posterior).
Opportunity sample, 16 male, healthy (medical, neurological, psychological) taxi drivers.
Matched pairs by health, mean age, gender, handedness in structural MRI database.
fMRI: count voxels (VBM) of grey matter. Counter blind to ptcp. Sig difference in left & right (posterior) hippocampi density.
Positive correlation between prev and experience driving.
Plasticity AO3 – Age (STR)
Generally reduces with age, but Plasticity may be lifelong.
Bezzola et al (2012): 40 hrs golf training ptcps age 40-60. fMRI observed increased motor cortex activity compared to control.
Suggests more efficient neural representation after training; plasticity continues throughout lifespan.
Plasticity AO3 – Behavioural Consequences (LIM)
Brain adaptation to prolonged drug use = poorer cog functioning in later life, inc. risk of dementia (Medina et al 2007).
60-80% amputees develop PLS -> can be unpleasant, painful. Ramachandran and Hirstein (1998): due to cortical reorganisation in somatosensory cortex.
Brain’s ability to adapt not always beneficial.
Functional Recovery AO1
Imp example of neural plasticity, some compensation of areas damaged due to trauma (stroke).
Spontaneious Recovery - Happens quickly after trauma, then slows after weeks/months. May require rehabilitative therapy.
Brain can rewire and reorganise, forms new synaptic connections close to damaged areas. Unused secondary neural pathways ‘unmasked’ - enables function to continue.
Strucutral Changes:
1) Axon sprouting - new nerve endings grow, connect with undamaged areas.
2) Reformation of blood vessels - Supports 1)
3) Recruitment of homologous areas on opposite hemisphere to do specific task (almost impossible for langauge).
Functional recovery AO3 – Real World Application (STR)
Contributed to neurorehabilitation. Understanding axonal growth is possible = new therapies.
E.g. constraint-induced movement therapy for stoke patients (repeatedly practise using affected body part, while unaffected mirror body part is restrained.
Helps medical profs know when intervention need to be made.
Functional recovery AO3 – Cognitive Reserve (LIM)
Level of education may = recovery rate.
Schneider et al (2014): More time people those with brain injury spent in education (cog reserve) had greater chance of DFR. >16 years = 40%, <12 years = 10%.
Other factors than plasticity (cog reserve) important in functional recovery.
Ways of Studying the Brain AO1 - fMRI
Functional Magnetic Resonance Imaging.
Detects brain activity as a result of blood flow. Brain activity (stimuli) req. more oxygenation (haemodynamic response). Produces precise activation maps.
Ways of Studying the Brain AO3 - fMRI
STR - No radiation (risk free), very high spatial resolution to 1mm (accurate, specific).
LIM - Less economical (expensive), poor temporal resolution (5 second lag). Does not represent true moment-moment activity.
Ways of Studying the Brain AO1 - EEG
Electroencephalogram.
Measures electrical activity in the brain via electrodes on a skull cap. Scan records brainwave patters from 1000s of neurons firing. Provides overall account of brain activity.
Ways of Studying the Brain AO3 - EEG
STR - Useful in studying real examples of brain activity e.g. sleep patterns and epilepsy. High temporal resolution to 1ms.
LIM - Low spatial resolution, only general conclusions shown. Not useful for pinpointing exact source of neural activity. Can’t distinguish between adjacent locations.
Ways of Studying the Brain AO1 - ERP
Event Related Potential.
EEG with isolated stimuli to show relevant responses.
Ways of Studying the Brain AO3 - ERP
STR - Same as EEG
LIM - Lack of standardisation in ERP methodology = difficult to confirm findings. Very difficult to obtain pure data, sensitivity of electrodes to extraneuous material.
Ways of Studying the Brain AO1 - Post Mortem
Brain analysis after death, likely those with rare disorders / cog deficits throughout life. Can be compared alongside neurotypical brain.
Ways of Studying the Brain AO3 - Post Mortem
STR - Vital in early psychology e.g. Broca, Wernicke before any neuroimaging tech existed. Also useful in modern day e.g. HM. Real world impact.
LIM - Difficult to establish causation, damage found may not be for abnormal behaviour. Ethical issues, ptcps may be unable to consent before death.
Circadian Rhythms AO1 - Sleep/Wake Cycle
Biological rhythms (distinct patterns of changes in body activity that conform to cyclical time periods) lasting 24 hours, governed by internal biological clocks (EdPs) and external factors (ExZ).
Sleep Wake cycle:
EdP → SCN, provides info from the eye about light.
ExZ → Light, can reset SCN.
Light detected by SCN inhibits production of melatonin in the pineal gland, leads to alertness.
Lack of light stimulates pineal gland to produce melatonin, leading to drowsiness.
Circadian Rhythms AO1 - Siffre’s cave study
2 set periods spent inside a cave, (2 months 1962, 6 months 1972). Deprived of exposure to natural light and sound, access to food and drink. Both cases = biological rhythms settles to 25 hours.
Circadian Rhythms AO1 - Other Research
Aschoff and Wever (1976) : ptcps spent 4 weeks in ww2 bunker, all bar one displayed 24-25 hour cycle. Suggests natural sleep cycle = slightly longer than 24 hours, entrained by ExZ.
Folkard et al (1985) : 12 ptcps in a cave for 3 weeks with set time to sleep and wake. Researcher gradually sped up clock to 22 hour cycle, 11 ptcps had difficulty adjusting. Suggests strong free-running circadian rhythm, difficult to change with ExZ.
Circadian Rhythms AO3 – Economic Application (STR)
Research shows adverse consequences of desynchronisation.
Boivin et al (1996): Night shift workers experience period of reduced concentration (circadian trough) at 6am = mistakes and accidents more likely.
Knutsson (2003): Shift workers 3x likely to develop heart disease than those on typical schedules.
Sleep wake cycle may have real world economic implications in managing worker productivity.
Circadian Rhythms AO3 – Real World Application (STR)
Research used to improve medical treatments. Circ rhythms coordinate various processes e.g. heart rate, digestion, hormone levels. Rise and fall during the day = led to chronotheraputics (medical treatment administered corresponding to biological rhythms.
Bonten et al (2015): Aspirin reduces platelet activity, most effective if taken at night = reduce likelihood of heart attack in morning (most common).
Circ rhythm research can help increase effectiveness of drug treatments.
Circadian Rhythms AO3 – Individual Differences (LIM)
Czeisler et al (1999): Individual Differences in sleep/wake cycles varying from ages 13-65.
Duffy et al (2001): Some people have preferences (Larks vs Owls).
No definitive circadian rhythms for all. Research can only demonstrate averages = mostly useless.
Circadian Rhythms AO3 – Research Flaws (LIM)
Methodological problems studies e.g. access to artificial light (research altered ptcps CR to 22/28 hours using artificial light.
Generalisations difficult to make from Siffre, Aschoff and Wever, as small sample size.
Siffre (1999): His sleep/wake cycle slowed as he aged.
Less internal validity, no meaningful generalisations drawn.
Infradian Rhythms AO1 - Overview
Biological rhythms with less than one cycle in 24 hours.
Menstrual cycle: Governed by monthly changes of hormone levels 24-35 (28) days.
SAD: Depressive disorder, seasonal pattern of onset, due to more darkness in the winter leads to more melatonin secretion than usual.
Infradian Rhythms AO1 - Menstrual Synchrony
Menstrual cycle is endogenour systen influenced by exogenous factors.
Stern and McClintock (1998) : 29 ptcps, irregular cycles. Samples of pheromones gathered from cotton pad in 9 womens armpits. Then rubbed on the other 20’s upper lip. 68% found cycles synced to odour donors.
Infradian Rhythms (synchrony) AO3 – Evolutionary Basis (STR)
Menstrual synchrony (Stern and McClintock) explained by natural selection. May have been advantageous for women to menstruate/pregnant together. Allows children who lost mothers to have breast milk, improving chances of survival.
Suggests synchrony is adaptive.
Infradian Rhythms (synchrony) AO3 – Methodological Shortcomings (LIM)
Many factors other than pheromones can alter menstrual cycle e.g. stress, diet, exercise = confounding variables. Synchronisation may be up to chance, shown by other studies unable to replicate results (Trevathan et al 1993).
Menstrual Synchrony studies = flawed.
Ultradian Rhythms AO1 -
Biological rhythms with more than one cycle in 24 hours.
Sleep cycle, monitored by EEG alternated between REM and NREM sleep. 5 stages that repeats itself every 90 minutes.
Stages 1 & 2: Light sleep, easily woken. Alpha Waves (higher frequency, short amplitude). NREM
Stages 3 & 4: Deep sleep (SWS), difficult to wake. Delta waves (lower frequency, greater amplitude). NREM
Stage 5: REM sleep. Body paralysed but EEG reading suggests person is awake. Hard to wake, dreaming period.
Ultradian Rhythms AO3 – Practical Application (STR)
Improved understanding of age-related changes in sleep. SWS reduces with age; growth hormone mostly produced in SWS (reduced in older people).
Cauter et al (2000): Sleep deficit may explain issues in old ag e.g. reduced alertness. Can increase SWS to resolve this partially with relaxation/medication.
Practical value of ultradian rhythm knowledge.
Ultradian Rhythms AO3 – Individual Differences (STR)
Sig. variation between people.
Tucker et al (2007): Large differences between ptcps in duration of each stage (particularly SWS). Suggests they are likely to be biologically determined.
Difficult to define ‘normal sleep’ meaningfully.
Endogenous Pacemakers AO1 - SCN and Animal Studies
SCN = tiny bundle of nerve cells in hypothalmus in each hemisphere. Its influence demonstrated in animal studies:
DeCoursey et al (2000) - Destroyed SCN connection in brains of 30 chipmunks, returned to natural habitat, observed for 80 days. Sig. proportion killed by predators as they were awake when they should’ve been asleep.
Ralph et al (1990) - Bred mutant hamsters with 20 hour sleep/wake cycle. SCN cells from foetal tissue transplanted to brains of normal hamsters, defaulted to 20 hours.
Endogenous Pacemakers AO3 - Research Support (STR)
SCN of vital importance in circadian rhythms.
Atan et al: Blind individuals without light perception means SCN cannot function, experience circadian desynchrony, assc with sleep/wake disorders.
Demonstrates importance of this EdP, adds scientific credibility. Understanding allows for biological therapy for dysfunction e.g. melatonin supplements.
Endogenous Pacemakers AO3 - Body Clocks beyond SCN (LIM)
SCN research obscures other body clocks.
Numerous circadian rhythms in organs and cells. Periphral oscillators found in organs incl. lungs, pancreas, skin. Influenced by actions of SCN, but can act independently.
Damiola et al: Chaning feeding pattersn in mice alters circadian rhythms in liver cells up to 12h, leaves rhythm of SCN unaffected.
Imbalanced understanding of circ rhythms, suggests other complex influences of EdP on body.
Exogenous Zeitgebers AO1 - Overview
ExZ are external factors that entrain biological rhythms.
Light is a ExZ directly influencing sleep/wake cycle though SCN, also indirectly influencing hormone sec, blood circ.
Campbell and Murphy (1998) - 15 ptcps woken at various times, light pad shone on back of knees, deviating sleep/wake cycle by up to 3 hours.
Observed in babies, newborn initial sleep cycle random until ~6W begin entrainment, ~16 weeks fully entrained.
Exogenous Zeitgebers AO3 - Practical Application (STR)
Understanding how affected by ExZ = can entrain them for own benifit.
Burgess et al: Exposure to bright light prior to east-west flight decreased time needed to readjust to local time. Opposite for west-east flught (no light exposure) also has same effect.
Economic implication, improve productivity of workers who must travel internationally, more efficient.
Exogenous Zeitgebers AO3 - Environmental Observations (LIM)
ExZ do not have same effect in all environments.
Accounts of people who live in places with dark summer (e.g. Greenland Inuits, others in arctic circle) suggest similar sleep-patterns year round despite spending 6 months in darkness. Conflicts against expectation of sleeping earlier + waking later in darkness, due to lack of natural light (melatonin inhibition).
EdP override environmental changes in light, not as important in circ rhythms.