Session 1 mesenteric Duplex
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
What arteries comprise the mesenteric arteries? / mesenteric arteries are made up of 3 main arteries, name them?
What are splanchnic arteries? - what do they supply?
What is another name for mesenteric ischemia?
What arteries comprise the mesenteric arteries?
→ Celiac, SMA, and IMA
What are splanchnic arteries?
→ Arteries supplying blood to the gut
What is another name for mesenteric ischemia?
→ Mesenteric angina
What causes mesenteric ischemia?
Why is mesenteric ischemia uncommon?
What test is required for definitive diagnosis of mesenteric ischemia?
What causes mesenteric ischemia?
→ Acute or chronic compromise of blood supply to the intestines from stenosis or occlusion
Why is mesenteric ischemia uncommon?
→ very uncommon due to Collateral pathways
What test is required for definitive diagnosis of mesenteric ischemia?
→ Arteriogram
What symptoms occur with chronic mesenteric ischemia? Name 4
What is “fear of food” syndrome?
How many arteries are usually involved to classify mesenteric ischemia clinically?
What symptoms occur with chronic mesenteric ischemia?
→ Abdominal cramps / pain after eating, diarrhea, bowel habit changes, weight loss, fear of food syndrome
What is “fear of food” syndrome?
→ Avoiding eating due to postprandial abdominal pain
How many arteries are usually involved to classify mesenteric ischemia clinically?
→ At least 2 arteries
What is the “two vessel rule”?
What degree of stenosis is usually present in chronic mesenteric ischemia?
What is the “two vessel rule”?
→ At least 2 mesenteric arteries involved for clinical diagnosis of ischemia
What degree of stenosis is usually present in chronic mesenteric ischemia?
→ Greater than 70% stenosis
What collateral pathway connects the celiac artery and SMA?
What artery is another collateral connection between the celiac artery and SMA?
What collateral pathway connects the celiac artery and SMA?
→ Pancreatico - duodenal complex
What artery is another collateral connection between the celiac artery and SMA?
→ Gastroduodenal artery
What collateral pathways connect the SMA and IMA? name 2
What is the purpose of collateral pathways in mesenteric circulation?
What collateral pathways connect the SMA and IMA?
→ Arc of Riolan and Marginal artery of Drummond
What is the purpose of collateral pathways in mesenteric circulation?
→ Maintain intestinal blood supply despite stenosis/occlusion
What commonly causes acute mesenteric ischemia?
Can acute mesenteric ischemia involve more than one artery?
Is acute mesenteric ischemia life threatening?
What commonly causes acute mesenteric ischemia?
→ Thrombosis from embolic occlusion
Can acute mesenteric ischemia involve more than one artery?
→ Yes
Is acute mesenteric ischemia life threatening?
→ Yes
A clot in an artery. This is more dangerous because arteries carry oxygen-rich blood to organs. If an artery is blocked, the tissue can become ischemic.
For your mesenteric slide, it is talking about arteries that supply the intestines, like the celiac, SMA, and IMA. The slide says acute mesenteric ischemia can happen from thrombosis caused by embolic occlusion, meaning something blocks an artery supplying the bowel.
What type of emergency is acute mesenteric ischemia?
What imaging studies diagnose acute mesenteric ischemia? name 3
Is acute mesenteric ischemia commonly diagnosed in ultrasound?
What type of emergency is acute mesenteric ischemia?
→ Life threatening, surgical emergency
What imaging studies diagnose acute mesenteric ischemia?
→ CT, MRA (Magnetic Resonance Angiography), or arteriogram
Is acute mesenteric ischemia commonly diagnosed in ultrasound?
→ No
What symptoms occur with acute mesenteric ischemia?
name 4
What symptoms occur with acute mesenteric ischemia?
→ Sudden onset of abdominal pain, fever, dehydration, acidosis
(Acidosis is a condition in which there is too much acid in the body fluids.)
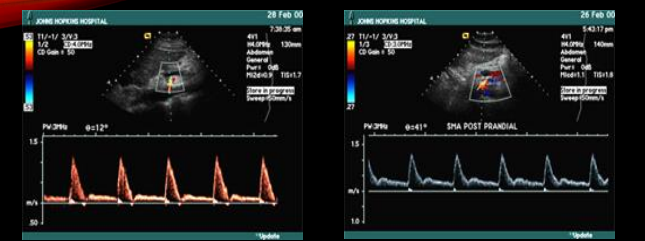
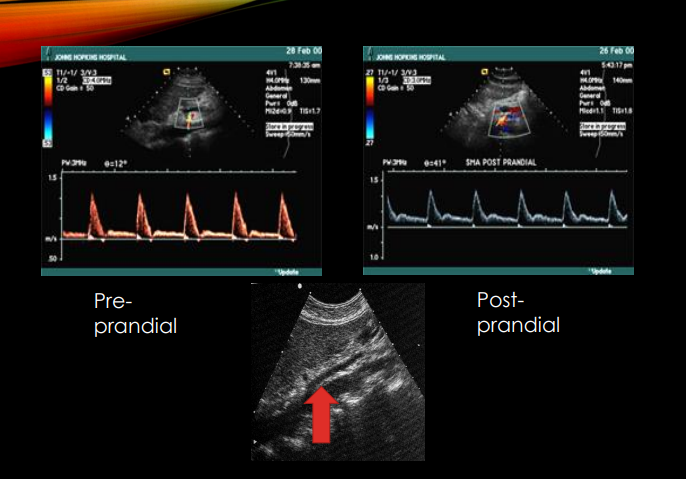
What flow pattern do the SMA and IMA have during fasting?
What flow pattern do the SMA and IMA have Post prandial (after eating)?
Why does mesenteric flow become ^ resistance postprandially?
what happens to the EDV ?
What flow pattern do the SMA and IMA have during fasting?
→ High resistance
What flow pattern do the SMA and IMA have after eating?
→ Low resistance
Why does mesenteric flow become low resistance postprandially?
→ Increased intestinal blood demand after eating
(blood goes to your intestines after eating to help digest and absorb your food. After eating = intestines are working harder = they need more blood flow.)
That is why your slide says the SMA and IMA are high resistance when fasting, but become low resistance after eating. Low resistance means the vessels open up more so more blood can flow to the intestines. Your slide also says after eating the EDV should at least double, meaning there is more forward blood flow during diastole after a meal
What preparation is required before a mesenteric duplex exam?
What may be given after the ^^^study?
Why is a postprandial meal sometimes given during mesenteric duplex?
What preparation is required before a mesenteric duplex exam?
→ Fasting
What may be given after the fasting study?
→ High calorie liquid meal
Why is a postprandial meal sometimes given during mesenteric duplex?
→ To evaluate postprandial flow changes
SONOGRAPHIC TECHNIQUE
What patient position & head is used for mesenteric duplex?
What transducer frequency is commonly used for mesenteric duplex?
What patient position is used for mesenteric duplex?
→ Supine with head elevated 10–30°
What transducer frequency is commonly used for mesenteric duplex?
→ 3.0–5.0 MHz
SONOGRAPHIC TECHNIQUE
Where is the transducer positioned during mesenteric duplex?
What vessels are evaluated before mesenteric arteries?
Why is an aortic Doppler waveform obtained? and what level do you place the doppler?
Where is the transducer positioned during mesenteric duplex?
→ Left of midline in longitudinal plane
What vessels are evaluated before mesenteric arteries?
→ Aorta and IVC
Why is an aortic Doppler waveform obtained?
→ Baseline comparison with mesenteric artery PSV (pulsed doppler waveform at level of mesenteric arteries)
Tell me the protocol sequence for Mesenteric Duplex should be 8 steps
Aorta Grey Scale:
• Long of Proximal, mid and distal and AP measurement
• Trans of Proximal, mid and distal and Width Measurement
• Aortal Color and Spectral Doppler at Mid and Adjacent to celiac / SMA
Celiac artery, Inspiration & Expiration
SMA, Proximal, mid and distal
IMA, Proximal
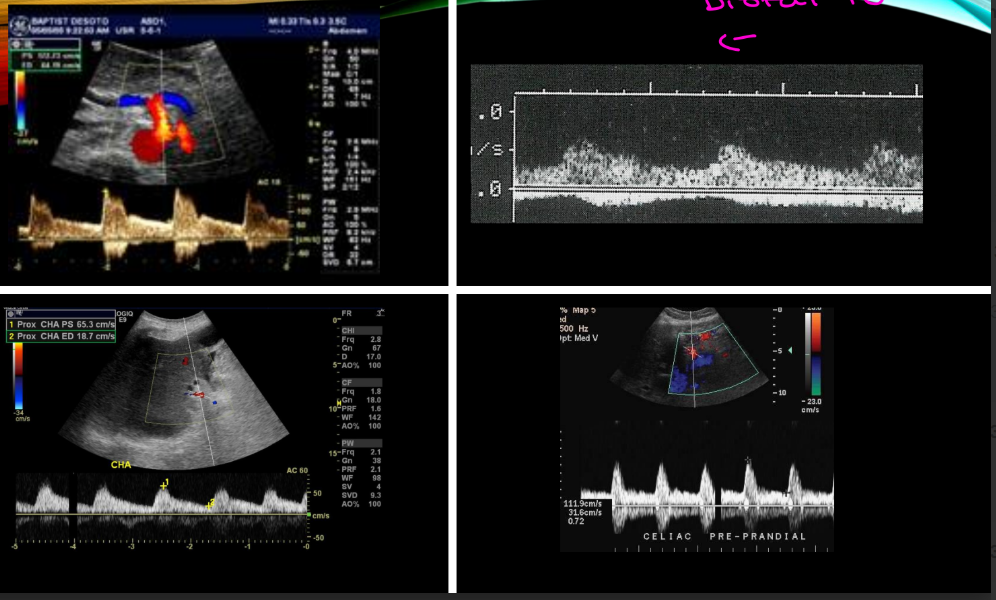
Common hepatic artery, Determine flow direction (should be antegrade)
skip
skip
skip
SONOGRAPHIC TECHNIQUE
What type of meal is used during postprandial mesenteric studies?
What should be documented after the patient drinks the meal?
What pt factors should be documented after the meal?
What type of meal is used during postprandial mesenteric studies?
→ High calorie liquid meal
What should be documented after the patient drinks the meal?
→ document Amount of liquid ingested and completion time of the drink
What pt factors should be documented after the meal?
→ Document onset of symptoms (document lack of symptoms)
When should the repeat study be performed after eating?
What else can postprandial mesenteric duplex evaluate?
When should the repeat study be performed after eating?
→ 20–30 minutes after meal
What else can postprandial mesenteric duplex evaluate?
→ Mesenteric bypass graft function
TECHNICAL TIPS
What gray-scale parameters should be optimized in mesenteric duplex? name 5
What pathology should gray scale evaluate?
What gray-scale parameters should be optimized in mesenteric duplex?
→ Depth, frequency, advanced imaging techniques, focal zone, dynamic range
What pathology should gray scale evaluate?
→ Atherosclerotic plaque
TECHNICAL TIPS
What lumen feature should be evaluated on gray scale?
What color Doppler settings should be optimized?
Why is color Doppler useful in mesenteric duplex?
What lumen feature should be evaluated on gray scale?
→ Residual lumen
What color Doppler settings should be optimized?
→ Gain, PRF, and wall filter
Why is color Doppler useful in mesenteric duplex?
→ Quick screening for flow abnormalities and aliasing
Residual lumen means the remaining open space inside a blood vessel where blood can still flow.
Think of the artery like a straw:
Normal lumen = the full open hole of the straw
Plaque/stenosis = something building up and narrowing the hole
Residual lumen = the small opening that is still left for blood to pass through
So on your mesenteric duplex slide, when it says to look for atherosclerotic plaque and the residual lumen, it means:
Look at how much plaque is inside the artery and how much open space is still available for blood flow.
Simple card version:
Residual lumen = the leftover open channel inside a narrowed vessel where blood can still flow.
What sample volume size is recommended for mesenteric Doppler?
Why is 60 degree angle correction difficult in mesenteric duplex? especially in which artery?
Are lower Doppler angles acceptable?
What sample volume size is recommended for mesenteric Doppler?
→ Larger sample volume
Why is angle correction difficult in mesenteric duplex?
→ Challenging abdominal insonation, especially celiac artery
Are lower Doppler angles acceptable?
→ Yes
TECHNICAL TIPS
Why is reproducibility important in mesenteric duplex?
What is the Doppler rule of thumb in mesenteric duplex?
Why is reproducibility important in mesenteric duplex?
→ Important for comparison in follow-up studies
What is the Doppler rule of thumb in mesenteric duplex?
→ Angle <60° and/or parallel to flow
PITFALLS
Why is Doppler insonation difficult in mesenteric duplex?
What syndrome causes increased celiac velocities on expiration?
Why do celiac velocities increase during expiration ^?
What maneuvers should be performed when evaluating possible ^that syndrome?
Why is Doppler insonation difficult in mesenteric duplex?
→ Challenging abdominal imaging
What syndrome causes increased celiac velocities on expiration?
→ Median arcuate ligament syndrome (MALS)
Why do celiac velocities increase during expiration in MALS?
→ Compression of celiac artery by median arcuate ligament
What maneuvers should be performed when evaluating possible MALS?
→ Breathing and patient maneuvers
What resistance pattern is normal in SMA/IMA during fasting?
What resistance pattern is normal after eating?
What should happen to EDV after eating?
What resistance pattern is normal in SMA/IMA during fasting?
→ High resistance
What resistance pattern is normal after eating?
→ Low resistance
What should happen to EDV after eating?
→ EDV should at least double
(meaning there is more forward blood flow during diastole after a meal.)
INTERPRETATION NORMAL
What normal velocity range is seen in mesenteric arteries?
(Velocities: depending on the vessel, velocity rages from)
What is the normal mesenteric-aortic ratio?
What flow pattern is considered normal in mesenteric arteries?
What normal velocity range is seen in mesenteric arteries?
→ 90–140 cm/sec
What is the normal mesenteric-aortic ratio?
→ 1.0
What flow pattern is considered normal in mesenteric arteries?
→ Laminar flow
INTERPRETATION ABNORMAL
What gray-scale adjustments help visualize mesenteric disease? list 5
What does color Doppler assess in abnormal mesenteric studies?
What color Doppler artifact commonly suggests stenosis?
What gray-scale adjustments help visualize mesenteric disease?
→ Depth, frequency, dynamic range, focal zone, TGC/gain
What does color Doppler assess in abnormal mesenteric studies?
→ Flow disturbances
What color Doppler artifact commonly suggests stenosis?
→ Aliasing
INTERPRETATION ABNORMAL
Why is pulsed Doppler essential in mesenteric duplex?
What Doppler finding suggests stenosis?
What Doppler finding suggests focal stenosis?
Why is pulsed Doppler essential in mesenteric duplex?
→ Identification and characterization of stenosis
What Doppler finding suggests stenosis?
→ Elevated velocities
What Doppler finding suggests focal stenosis?
→ Focal increase in velocity
What Doppler parameter may increase in tighter stenosis?
What turbulent finding may occur distal to stenosis?
What Doppler parameter may increase in tighter stenosis?
→ narrower stenosis can have Elevated EDV
What turbulent finding may occur distal to stenosis?
→ Post-stenotic turbulence
INTERPRETATION ABNORMAL
What are the “4 D’s” in mesenteric duplex?
What are the “4 D’s” in mesenteric duplex?
→ Distal Disease Determines Diastole
(Distal Disease Determines Diastole = what happens downstream controls the diastolic flow. If downstream resistance is high, EDV is low. If downstream resistance is low, EDV increases.)
Normal post-prandial EDV increase:
Happens after eating
Flow becomes low resistance
Should be more generalized/expected response
No focal narrowing or turbulence
Abnormal elevated EDV from stenosis:
Happens at the narrowed area
Usually comes with high PSV
Focal velocity increase
Color aliasing
Post-stenotic turbulence
Plaque or narrowed residual lumen may be seen
Simple note:
EDV doubling after eating is normal. EDV elevated with a focal high-velocity jet/turbulence at a narrowed area is abnormal stenosis.
What does “Distal Disease Determines Diastole” mean?
What does “Distal Disease Determines Diastole” mean?
→ Distal disease affects diastolic flow patterns
INTERPRETATION ABNORMAL
What is another name for celiac compression syndrome?
What is another name for celiac compression syndrome?
→ Median arcuate ligament syndrome (MALS)
What patient population commonly develops MALS?
When are MALS symptoms usually worse? during when?
Why do symptoms worsen during ^in MALS?
What patient population commonly develops MALS?
→ Young women
When are MALS symptoms usually worse?
→ Expiration
Why do symptoms worsen during expiration in MALS?
→ Median arcuate ligament compresses the celiac artery
Sonographic technique includes evaluation during What breathing maneuvers are used during MALS evaluation?
What body position may normalize the waveform in MALS?
What appearance does the celiac artery origin have in MALS?
What breathing maneuvers are used during MALS evaluation?
→ Inspiration and expiration imaging
What body position may normalize the waveform in MALS?
→ Upright position
What appearance does the celiac artery origin have in MALS?
→ Hook-like appearance on 2D imaging
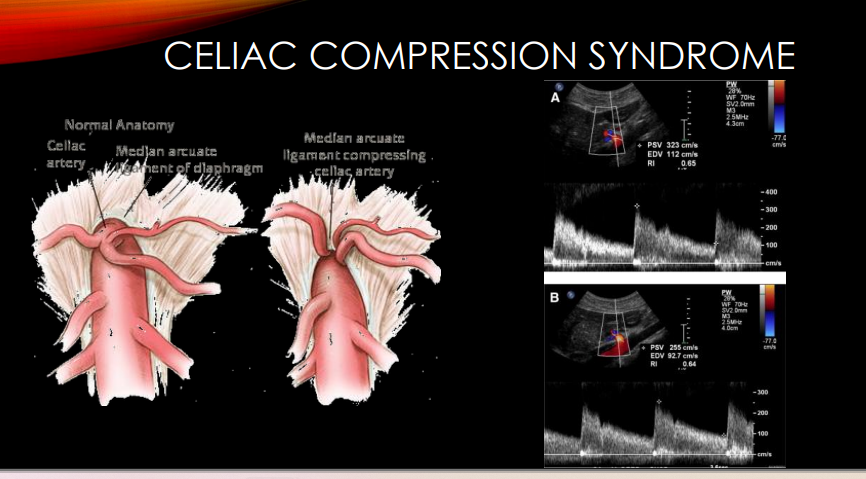
which one is pre - prandial & Post - prandial

A young women mimics signs and symptoms usally exacerbated with expiration, and has a “hook” like appearance on 2D whats is the pt diagnosis and explain what this picture tells you?
celiac compression syndrome / Median arcuate ligament syndrome
A shows during expiration the PSV is 323 cm/s
normal range for mesenteric artery is 90-140 cm/s, and this shows highly elvated velocity compare to image B which is inspiration and shows the PSV 255 cm/s
this pt has sudden onset of abdominal pain, fever , dehydration, acidosis diagnosed by MRA whats there diagnosis? due to what?
ACUTE MESENTERIC ISCHEMIA, Due to thrombosis caused by embolic occlusion (stenosis or occlusion of the mesenteric arteries SMA, IMA, Celiac A)
may involve one or more arteries, is life-threatening/surgical emergency, and is usually diagnosed by CT, MRA, or arteriogram, not usually in the ultrasound department.
Acidosis
This means the body is becoming too acidic because bowel tissue is not getting enough oxygen
What you may see on images/Doppler
Since acute mesenteric ischemia is from an occlusion/blockage, you may expect:
Absent flow in the affected mesenteric artery if completely occluded.
Very abnormal flow if partially blocked.
Thrombus/embolus blocking the lumen if visible.
No normal color filling in the blocked segment.
Severe focal narrowing/occlusion instead of just mild elevated velocities.
But remember: your slide says acute cases are not normally seen in the ultrasound department and are usually diagnosed by CT, MRA, or arteriogram. So on an exam, they may give you the symptoms + emergency wording more than just an ultrasound image.
How to tell acute vs chronic
Acute mesenteric ischemia:
Sudden abdominal pain, emergency, embolic/thrombotic occlusion, one or more arteries involved.
Chronic mesenteric ischemia:
Pain after eating, weight loss, fear of food, usually at least 2 arteries involved, severe stenosis >70%.
Simple exam clue:
Acute = sudden severe belly pain + embolic occlusion + surgical emergency.
Yes — chronic mesenteric ischemia can be evaluated with ultrasound/duplex.
For chronic mesenteric ischemia, ultrasound looks for signs of stenosis/narrowing in the mesenteric arteries, especially the:
Celiac artery, SMA, and IMA — these are the mesenteric/splanchnic arteries that supply the gut.
On duplex, you would expect possible findings like:
Elevated velocities
Focal increase in velocity
Color aliasing
Post-stenotic turbulence
Possible plaque/narrowed lumen
Your PowerPoint says pulsed Doppler is essential for identifying and characterizing stenosis, and abnormal findings include elevated velocities, focal velocity increase, elevated EDV in tighter stenosis, and post-stenotic turbulence.
Acute mesenteric ischemia, the main symptoms , whats the cause
Diagnosed by CT, MRA, or arteriogram; not normally seen in the ultrasound
department
Due to thrombosis caused by embolic occlusion
• One or more arteries involved
• Life threatening, surgical emergency
Symptoms
• Sudden onset of abdominal pain
• Fever
• Dehydration
• Acidosis
Chronic mesenteric ischemia, main symptoms and cause
Severe compromise, >70% stenosis
“Two vessel rule” for clinical diagnosis
Abdominal cramps / pain after eating, Diarrhea, change in bowel habit, Weight loss, “Fear of food” syndrome
•Arteriogram required for definitive diagnosis
•Acute or chronic compromise of blood supply to small and large intestine
caused by stenosis or occlusion, •Very uncommon due to collateral pathways
Simple exam way to remember
Normal after eating: SMA/IMA should become low resistance and EDV increases.
Chronic disease: stenosis causes elevated velocities/turbulence, and the gut may not get enough flow after eating.
Acute disease: sudden embolic/thrombotic occlusion, possible absent flow or high-resistance/water-hammer proximal to blockage.
In acute mesenteric ischemia, it is more sudden and usually due to embolus/thrombus causing occlusion. Your slide says it is life-threatening and usually diagnosed by CT, MRA, or arteriogram, not normally in the ultrasound department.
If an artery is occluded, the waveform can look very different depending on where you sample:
Proximal to occlusion: may show a high-resistance “water-hammer” type waveform because blood hits a blockage and cannot continue forward normally.
At the occlusion: little to no color or spectral flow.
Distal to occlusion: reduced flow, absent flow, or collateral-dependent flow.
Celiac compression syndrome, causes, main clues
Young woman, celiac velocity worse on expiration, improves with inspiration/upright, hook like apparence on 2D, may have similar signs and sumptoms of mesenertic ischemia
External compression by median arcuate ligament