Chapter 6 Skeletal System Lecture Objectives
1/83
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
84 Terms
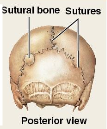
Sutural Bones
Flat, oddly shaped bones found between the flat bones of the skull. Their borders fit together like a jigsaw puzzle
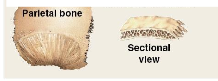
Flat Bones
Thin, parallel surfaces that provide protection and muscle attachment. Ex: Roof of skull (parietal bone), sternum, ribs, and scapula
Irregular Bones
Complex shapes with short, flat, notched, or ridged surfaces. Examples: Vertebrae and pelvis

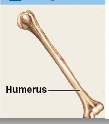
Long Bones
Long and slender. Examples: Humerus (arm), forearm, femur (thigh—largest/heaviest bone), leg, palms, soles, fingers, and toes
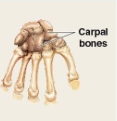
Short Bones
Boxlike appearance. Examples: Carpal bones (wrists) and tarsal bones (ankles).
Sesamoid Bones
Small, round, and flat; typically located near joints. Example: Patella (kneecaps—everyone has these).

Diaphysis
The extended, tubular shaft of the bone.
What is the anatomy of a long bone?
Epiphysis (the ends), diaphysis (shaft), medullary cavity, compact bone, and spongy bone
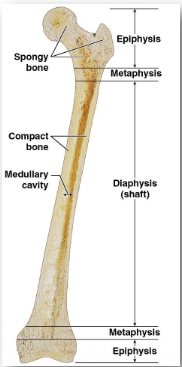
Epiphysis
The expanded area at each end of the bone
Metaphysis
The narrow zone where the diaphysis and epiphysis interconnect.
Medullary Cavity
The central space within the shaft surrounded by compact bone
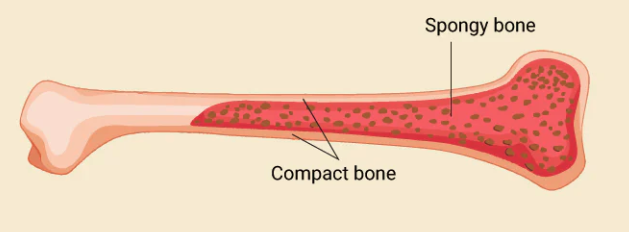
Compact Bone
dense, solid, and forms a sturdy protective outer layer
Spongy bone (trabecular bone)
forms an open, less dense network of struts and plates resembling a 3D garden lattice, and contains red bone marrow
Diploe
Flat bone-spongy bone; sandwich between compact bones
Two Main Components of Bone Matrix
Calcium Phosphate (2/3) and Collagen Fibers (1/3)
Calcium Phosphate (2/3 of bone weight)
Combines with other calcium salts to form hydroxyapatite crystals. It makes bones hard to withstand compression, but inflexible and brittle.
Collagen Fibers (1/3 bone weight)
Provides flexibility, strength, and toughness to withstand twisting and bending. (Without calcium phosphate, bones appear normal but are highly flexible).
Calcium phosphate + Calcium hydroxide + Calcium carbonate =
Hydroxyapatite crystals
Osteogenic Cells
Mesenchymal stem cells that divide to produce daughter cells that differentiate into osteoblasts. They are crucial for fracture repair and are found in the inner layers of the periosteum and endosteum.
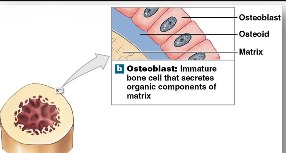
Osteoblasts
Immature bone cells that produce new bone matrix through osteogenesis/ossification by secreting proteins and depositing calcium salts.
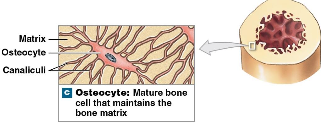
Osteocytes
Mature bone cells that cannot divide; only one occupies a single pocket called a lacuna. They feature narrow cytoplasmic extensions tracking through canalicutli for cell communication and nutrient access. They maintain matrix protein/mineral content and help repair damaged bone.
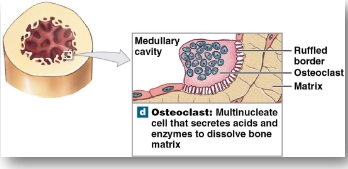
Osteoclasts
Large, multinucleated cells (50+ nuclei) that absorb and remove bone matrix via osteolysis by secreting acids and enzymes. They reside in Howship's lacunae and have a ruffled border to increase secretory surface area.
3 different types of lamellae that makes up compact bone
interstitial, circumferential, and concentric
Concentric Lamellae
Target-like nested layers of bone matrix arranged in concentric rings around a central canal
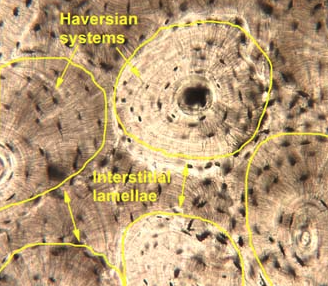
Interstitial Lamellae
Layers of bone matrix that fill in the angular spaces between adjacent osteons.
Circumferential Lamellae
Found winding around the outermost and innermost surfaces of the bone shaft, produced during appositional bone growth.
Compact bone structure
basic functional unit at microscopic level is the osteon or Haversian system
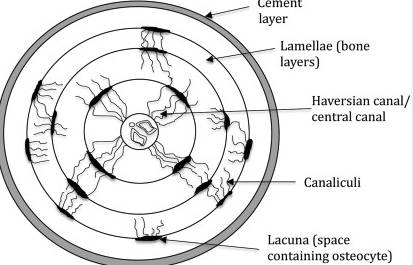
Central Canal (Haversian Canal)
Runs vertically down the center of an osteon parallel to the bone axis
Perforating Canal (Volkmann's Canal)
Horizontal canals extending perpendicularly to supply blood to osteons deeper in the bone.
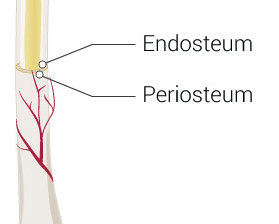
Periosteum (Outside)
Covers all superficial compact bone surfaces (except at joint cavities) and features an outer fibrous layer and inner cellular layer. Functions: Isolates bone, routes blood vessels/nerves, and aids bone growth/repair. Perforating fibers interweave with tendons to strengthen attachments.
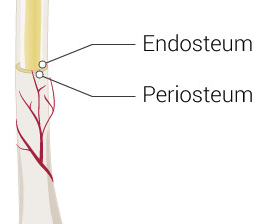
Endosteum (Inside)
An incomplete cellular layer lining the medullary cavity, covering trabeculae of spongy bone, and lining central canals. Functions: Active during bone growth, repair, and remodeling. Its incomplete nature exposes bone matrix for osteoblasts/osteoclasts to work
What are the 2 layers covering long bones?
Periosteum and Endosteum
What does endochondral ossification make?
Long bones and other non-dermal skeletal elements
What is Endochondral Ossification?
The process by which bone tissue is created from a preexisting framework of hyaline cartilage. It is responsible for the formation and growth of most bones.
Step 1 of Endochondral Ossification
Cartilage Calcifies; Chondrocytes in the center of the shaft enlarge, the matrix calcifies, and the cells die, leaving empty cavities
Step 2 of Endochondral Ossification
Blood vessels encircle the edges, and perichondrial cells switch to osteoblasts, forming a superficial bone collar around the shaft
Step 3 of Endochondral Ossification
Blood vessels penetrate the cartilage matrix, bringing fibroblasts that convert to osteoblasts to produce spongy bone at the primary ossification center in the diaphysis.
Step 4 of Endochondral Ossification
Medullary Cavity Forms; Remodeling carves out the central medullary cavity as the bone shaft grows and thickens.
Step 5 of Endochondral Ossification
Secondary Ossification Center (Epiphyses); Capillaries and osteoblasts migrate into the bone ends (epiphyses), creating spongy bone there.
Step 6 of Endochondral Ossification
Epiphyseal Closure; The epiphyseal cartilage (plate) separates the ends from the shaft for lengthwise growth. At puberty, sex hormones accelerate osteoblast activity until the cartilage disappears, leaving a permanent epiphyseal line.
Appositional growth (growth in width)
Early bone collar is formed during early stages of endochondral ossification, then it increases in diameter with bone growth at the outer surface.
Interstitial Growth (Growth in Length)
Epiphyseal cartilage (plate) separates the epiphysis and diaphysis. On the epiphyseal side, new cartilage is continuously produced, while on the diaphysis side, osteoblasts continuously invade and replace old cartilage with bone
Epiphyseal Closure
At puberty, rising sex hormone levels accelerate osteoblast activity faster than cartilage production. The epiphyseal cartilage gets narrower until it completely disappears, leaving behind a permanent epiphyseal line
Layers handled in appositional growth
Matrix is added to the outer surface, while osteoclasts simultaneously remove bone matrix from the inner surface lining the medullary cavity. This allows the medullary cavity to expand gradually as the bone gets thicker in diameter.
What bones are made in Intramembranous Ossification?
Dermal bones (e.g., flat bones of the skull, mandible, and clavicles).
Intramembranous Ossification
Begins when osteoblasts differentiate within mesenchymal/fibrous connective tissue (about 8th week of embryonic development)
What cells are involved in appositional growth?
Osteoblasts (inner layer of periosteum) add bone to the outside, while osteoclasts remove bone from the inside.
Overall process of intramembranous ossification
Begins when embryonic mesenchymal cells differentiate into osteoblasts to secrete a matrix that calcifies into small bone struts called spicules. As these spicules grow and trap surrounding blood vessels, they remodel into a "sandwich" structure made of internal spongy bone protected by outer layers of compact bone
What is bone remodeling?
Continuous recycling and renewal of organic/mineral matrix elements. It does not happen equally everywhere; young adults recycle about 1/5 of the skeleton per year (the head of the femur is replaced 2–3 times/year, while the shaft is largely unchanged)
Does our entire skeleton go through this throughout the year? Why is it dangerous with radioactive compounds?
Any exposure to it with high biochemical resemblance to calcium can be deposited through bone remodeling activities as well.
Calcitriol
Produced in kidneys; increases calcium and phosphate ion absorption by the intestines
Growth Hormone
Produced in pituitary gland; Stimulates osteoblast activity and synthesis of bone matrix
Thyroxine
Produced in Thyroid Gland Follicle Cells; Works with growth hormone to stimulate osteoblast activity and matrix synthesis
Sex Hormones- Estrogen/Testosterone (Ovaries/Testes)
Stimulate osteoblast activity and matrix synthesis; estrogen closes epiphyseal plates earlier.
Parathyroid Hormone
Produced in PTH (Parathyroid Glands); Stimulates osteoclast activity to elevate blood calcium levels
Calcitonin
Produced in Thyroid Gland C Cells; Inhibits osteoclast activity to lower blood calcium levels (primarily in pregnant/nursing women)
What happens when blood calcium ion concentration is too high (above 11 mg/dL)?
Thyroid gland C cells release Calcitonin; 1) Bone: Osteoclast activity decreases, slowing calcium release. 2) Intestines: Calcium absorption decreases. 3) Kidneys: Kidneys excrete calcium ions. 4) Urine: Increased calcium loss in urine
What happens when blood calcium ion concentration is too low (below 8.5 mg/dL)?
Parathyroid glands release PTH; 1) Bone: Osteoclasts stimulated to release calcium. 2) Intestines: Intestinal calcium absorption increases. 3) Kidneys: Kidneys absorb/conserve calcium ions. 4) Urine: Decreased calcium loss in urine.
What are the consequences if blood calcium remains too high (+30%)?
Neurons and muscle cells become completely unresponsive
What are the consequences if blood calcium remains too low (-35%)?
Neurons become overly excited, causing muscle convulsions
What are the consequences if blood calcium remains extremely low (-50%)?
Results in death
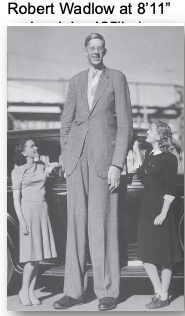
Gigantism
Overproduction of growth hormone before puberty; results in extreme height
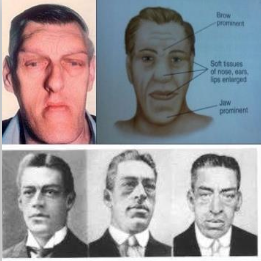
Acromegaly
Growth hormone levels rise abnormally after epiphyseal closure; bones grow thicker instead of longer, especially in the face, jaw, and hands.
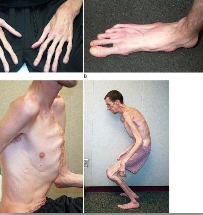
Marfan Syndrome
Excessive cartilage formation at epiphyseal plates; leads to an abnormally tall height and long, slender limbs.
Why do women after menopause (~30 & 40yrs old) often result in osteoporosis?
Sex hormones maintain bone deposition; a sharp decline in estrogen accelerates bone mass loss (~8% per decade) because osteoblast activity drops while osteoclasts continue uninhibited.
Why is osteoporosis after menopause dangerous?
Compromises normal skeletal function. Mass is lost heavily in the vertebrae, epiphyses, and jaws, making limbs so fragile that hip fractures can occur from simply trying to stand up.
Compression Fracture
Vertebrae collapse under extreme stress (associated with osteoporosis)

What is osteopenia?
Bones become thinner and waker as normal part of aging process, and inadequate ossification
Osteoclast-activating factor
Cancers of bone marrow, breast can release this chemical factor, and increase both number and activity of osteoclasts→severe osteoporosis
Nondisplaced/Displaced
Position of bone ends
Complete/Incomplete
Completeness of break
Linear/Transverse
Orientation of break to bone’s long axis
Open/Closed
Broken penetrate skin or not
Spiral fracture
produced by twisting stresses that spread along length of bone

Comminuted Fracture
shattering of affected area into many bony fragments

Epiphyseal Fracture
occur where bone matrix is undergoing calcification; unless carefully treated, fractures between epiphysis and epiphyseal cartilage can permanently stop growth

Greenstick Fracture
Only one side of the shaft breaks while the other bends; common in children.

Colles Fracture
A break in the distal portion of the radius, typically from cushioning a fall.

Pott's Fracture
Ankle fracture affecting both the distal tibia (medial malleolus) and distal fibula (lateral malleolus)

What is the process of fracture repair?
Fracture hematoma formation, callus formation, spongy bone formation, and compact bone formation
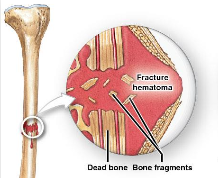
Fracture Hematoma Formation
Blood vessels break, leading to extensive bleeding and a clot (hematoma)
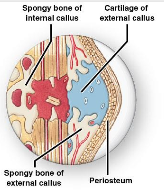
Callus Formation
An internal callus of spongy bone binds the inner edges, and an external callus of cartilage and bone stabilizes the outer edges.
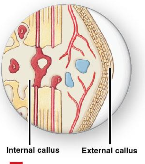
Spongy Bone Formation
Osteoblasts replace the central cartilage of the calluses with spongy bone, and dead bone fragments are reabsorbed.

Compact Bone Formation
Remodeling over time forms compact bone. The bone is often slightly thicker/stronger at the repair site than normal.