HLTH2002: Introduction to Global Health - Sem2 (W1-W6)
1/103
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
104 Terms
What is the International Organisation of Migration definition of global heatlh?
‘Health problems, issues, and concerns that transcend national boundaries may be influenced by circumstances or experiences in other countries and are best addressed by cooperative actions and solutions’.
What is global heatlh?
Not just about ‘global’ health problems.
Not only a field of theory.
Global burden of disease snapshot.
Non-communicable diseases (NCDs) kill 41 million people each year, equivalent to 71% of all deaths globally.
Each year, more than 15 million people die from a NCD between the ages of 30 and 69 years; 85% of these ‘premature’ deaths occur in low- and middle-income countries.
When reviewed 77% of all NCD deaths are in low- and middle-income countries.
Cardiovascular diseases account for most NCD deaths, or 17.9 million people annually, followed by cancers (9.3 million), respiratory diseases (4.1 million), and diabetes (1.5 million).
These four groups of diseases account for over 80% of all premature NCD deaths.
Challenges in considering global health problems?
Health system comparisons?
Governance and regulation?
International relations?
Trade?
One health?
Life course models?
Disease and burden of disease?
Who are the players when it comes to global health?
Individual countries.
Organisations within the UN system relevant to health (ie. WHO).
Organisations outside the UN system relevant to health (ie. World Bank, GAVI).
Non-governmental organisations (NGOs) → Bill and Melinda Gates Foundation, International Red Cross, Medicins Sans Frontieres.
What does the sphere of health finance encompass?
Universal Health Coverage.
Trade.
International Health Agreements.
Provision of health goods and services (workforce, knowledge/skills, pharmaceuticals).
What does migration entail?
Voluntary and involuntary migration.
Burden shifts.
Regulatory practices in health systems.
What are some risks/concerns to consider in the arena of global health?
Burden shifts → communicable vs. non-communicable disease.
Internet and AI.
Bioterrorism.
Conflict → immediate, short, mid, and long term health consequences.
Post-conflict healthcare and service delivery.
Environmental concerns → pollution, toxins, and vectors.
Comment broadly on the evolution of global health and development.
Global understandings of health and development change.
Since 1978 there have been 6 key global development policy ‘events’ with implications for health:
1978 → WHO/Unicef Declaration on Primary Health Care.
1993 → World Bank WDR Investing in Health.
1996 → OECD International Development Goals.
2001 → UN Millennium Development Goals.
2005 → OECD Paris Principles of Aid Effectiveness.
2015 → UN Sustainable Development Goals.
Comment on the 1978 development of Primary Health Care.
Primary Health Care Alma Ata conference 1978, supported by WHO/Unicef.
Health defined in holistic terms, with community focus.
‘Governments have a responsibility for the health of their people…’
A philosophy → ‘essential health care based on practical, scientifically sound and socially acceptable methods… made universally accessible… through their full participation…’
A level of care → ‘first level of contact… bringing healthcare as close as possible’.
A set of 8 essential components.
What are the 8 essential components of PHC?
Education on health and prevention of disease.
Promotion of food supply and nutrition.
Adequate water supply and basic sanitation.
MHC care, including Family Planning.
Immunisation against major diseases.
Prevention/control of locally endemic diseases.
Appropriate treatment of common diseases and injuries.
Provision of essential drugs.
Comment on the notion of ‘health for all’, and the ‘failure’ of the PHC.
WHO 1997: ‘Health for all by the year 2000’ was intended as a goal for the 1978 PHC declaration.
In 1979, Julia Walsh and Kenneth Warren presented ‘selective primary health care’ as an ‘interim’ strategy for PHC implementation.
Selective PHC - ‘vertical’ programmes often with parallel systems to target specific diseases/issues.
Comprehensive PHC - ‘horizontal’ sectoral approach to health services, developed using the district as the primary organisation for services.
Still evident in Global Health initiatives such as Roll Back Malaria, GAVI, Global Fund.
What was significant about the 1993 World Development Report?
World Bank bought into international health with World Development Report 1993 - Investing in Health.
Examined the interplay between human health, health policy, and economic development.
Health redefined in economic terms.
DALYs used to determine cost-effective interventions.
Argues for state intervention/investment in health.
Focus shifted from Mother and Child to the economically productive adult.
Packages of basic care (essential curative, preventive, public health activities) calculated by bang-for-bucks.

Significant points of the 1996 OECD International Development Goals?
OECD Shaping the 21st Century - The Contribution of Development Cooperation.
Reduce by half the proportion of people living in extreme poverty between 1990 and 2015.
Enrol all children in primary school by 2015.
Make progress towards gender equality and empowering women by eliminating gender disparities in… education by 2005.
Reduce infant and child mortality rates by ⅔ [by] 2015.
Reduce maternal mortality ratios by ¾ [by] 2015.
Provide access for all who need reproductive health services by 2015.
Implement national strategies for sustainable development by 2005 so as to reverse the loss of environmental resources by 2015.
What are the four principles for partner-based cooperation?
Country priorities → interests and priorities of developing countries must be central.
Ownership → each country has to develop locally owned strategy, which should orient the programs and activities of donors.
Multi-stakeholder approach → planning and implementation must involve a multitude of stakeholders from the state, private sector, and civil society.
Local capacity → development processes have to strengthen and be based on local capacities.
1996 OECD International Development Goals vs. 2005 Paris Principles for Development Assistance 🙂

2001 UN Millennium Development Goals 🙂

Comment on the implementation of the MDGs.
The MDGs were not expected to have a significant impact;
Created opportunistically by a small group of technocrates, with support of Kofi Anan.
Never debated by the UN, nor formally endorsed.
Rejected by the USA until 2005.
But progressively MDGs gained credence in development:
World Bank used them to monitor loans, grants, and in Poverty Reduction Development Strategies.
Bilateral development agencies adopted them.
Many countries used them to report their development progress.
The MDGs shaped development priorities.
2015 MDG Final Report - outcomes of the 8 goals?
MDG1 - Eradicate Extreme Poverty and Hunger.
Extreme poverty declined from 47% of the population in the developing world in 1990 living on less than $1.25 a day, to 14% in 2015. Globally, extreme poverty fell by more than half.
MDG2 - Achieve Universal Primary Education.
The proportion of children not at school fell by nearly 50%. Primary school enrolment in developing countries rose from 83% to 91%.
MDG3 - Promote Gender Equality and Empower Women.
Equity in school nearly achieved - increases in employment and parliament - 90% - but only 1 in 5 females overall.
MDG4 - Reduce Child Mortality.
The global under-5 mortality rate has declined by more than half, dropping from 90 to 43 deaths per 1000 live births.
Measles vaccination rose from 73% to 84% worldwide.
MDG5 - Improve Maternal Health.
Maternal Mortality Rate has dropped by 45% worldwide; skilled birth attendance rose from 59% to 71%.
MDG6 - Combat HIV/AIDS, Malaria and Other Diseases.
New HIV infections dropped by 41%; 13.6 million are on ART compared to 800,000. 6.2 million malaria deaths have been averted; 900 million impregnated nets distributed.
MDG7 - Ensure Environmental Sustainability.
91% of world population have access to improved water; 147 countries have met the drinking water target.
MDG8 - Develop a Global Partnership for Development.
Official development assistance increased by 66%, reaching $135.2 billion.
But, despite many successes, the poorest and most vulnerable people are being left behind.
What were the outcomes of the WHR 2008 ‘PHC: Now More than Ever’?
Universal coverage reforms.
Service delivery reforms.
Public policy reforms.
Leadership reforms.
WHR 2010 Health Systems Financing - The Path to Universal Coverage

Comment on the process of consultation with regard to the SDGs.
UN consultative process initiated in 2012:
88 country consultations.
Regional consultations - most notably the African Common Position on the Post 2015 Development Agenda.
11 thematic consultations.
Web-based platform ‘World We Want’.
High Level Panel of Eminent Persons on the Post-2015 Development Agenda.
Open Working Group thematic groups from 2013.
2014: Zero Draft Open Working Group Proposal for Sustainable Development Goals
2015: The Sustainable Development Goals 🙂

What were the MDG+ targets in the health SDG?
MDG5 → SDG3.1 = by 2030 reduce global mortality ratio to less than 70 per 100,000 live births.
MDG4 → SDG3.2 = by 2030 end preventable deaths of newborns and children under 5 years of age.
MDG6 → SDG3.3 = by 2030 end the epidemics of AIDS, tuberculosis, malaria, and NTDs and combat hepatitis, water-borne diseases, and other communicable diseases.
MDG5b → SDG3.7 = by 2030, ensure universal access to sexual and reproductive health services… and integration… into national strategies and programs.
What were the ‘new’ health targets in health SDG?
SDG3.4 → by 2030, reduce ⅓ premature mortality from NCDs through prevention and treatment and promote mental health and well-being.
SDG3.5 → strengthen the prevention and treatment of substance abuse, including narcotic drug abuse and harmful use of alcohol.
SDG3.6 → by 2020, halve the number of global deaths and injuries from road traffic accidents.
SDG3.9 → by 2030 substantially reduce the number of deaths and illnesses from hazardous chemicals, and air, water, and oil pollution and contamination.
What were the four Means of Implementation in the health SDG?
SDG3a → strengthen the implementation of the WHO Framework Convention on Tobacco Control in all countries as appropriate.
SDG3b → support the research and development of vaccines and medicines… provide access to affordable essential medicines and vaccines, in accordance with the Doha Declaration on the TRIPS Agreement and Public Health.
SDG3c → substantially increase health financing and the recruitment, development, training, and retention of the health workforce in developing countries.
SDG3d → strengthen the capacity of all countries for early warning, risk reduction, and management of national and global health risks.
October 2018, international delegates celebrate Primary Health care in Astana, Kazakhstan, 40 years after Alma Ata. What was the quote given?
‘The new declaration has renewed political commitment to primary healthcare from governments, NGOs, professional organisations, academia, and global health and development organisations. It will be used to inform the UN General Assembly high-level meeting on Universal Health Coverage in 2019’.
The 1978 Alma Ata Charter for Primary Health Care emphasised the importance of…
…community-based healthcare that is affordable and accessible.
Comment on the early PHC landscape in Australia.
1972 introduced Medibank in Australia (Whitlam).
Fraser Government tried to dismantle it, but electorate was not supportive of this change.
Subsequent government restored Medibank - now called Medicare.
What was the 1980s shift to the social model of health?
Framework in which improvements in health and well-being are achieved by addressing the social and environmental determinants of health in tandem with biological and medical factors.
Inequalities and premature mortality continue to rise despite focus on society.
Give the main points of the WHO Ottawa charter for health promotion 1986.
Landmark Conference in Canada: shifted public health paradigm towards health promotion.
Five key action areas:
Build healthy public policy.
Creative supportive environment.
Strengthen community action.
Develop personal skills.
Reorient health services.
Comment on the 1900s-2000s emergence of new public health.
Focus on physical infrastructure, but also on social support, social capital, behaviour, and lifestyle.
Legislation and policy crucial for improving public health.
Intersectoral action is essential and medicine is only one of several contributing professions.
Community participation encouraged.
Focus on disease prevention, health promotion, and positive definition of health.
Equity is an explicit aim.
What were the 2018 public health domains?
Disease prevention.
Disease control.
Health protection.
Environmental health management.
Health promotion.
Comment on the three levels of disease prevention.
Primary: preventing ill health before it occurs and promoting wellness (skin cancer prevention, dental visits, prevent social isolation among elderly).
Secondary: detection of early signs of disease to stop progressions, or shorten duration (cancer screening, diabetes screening, diet modification).
Tertiary: reducing severity and impact of ill health (rehabilitation, support groups, eye and foot care for people with diabetes).
Comment on the National Preventative Health Strategy Australia.
Vision: Australia to be the healthiest country by 2020.
Aims:
Prevent premature illness and deaths between now and 2020.
Minimise impending overload of the health and hospital systems.
Increase the productivity of Australia’s workforce.
Avoid the health and social costs that would otherwise be incurred if we did nothing.
Elements of health protection?
Environmental health hazards.
Safe drinking water.
Sanitation.
Food contamination.
Indoor air pollution.
Inadequate solid waste disposal.
Occupational injury.
Natural disasters (flood, drought, bushfire, earthquakes).
Disease vectors (insects and rodents).
Government involvement/roles in health protection?
Federal Government → development of national policy (food import policy, national strategies, quarantine services).
State Government → enforcement of legislation (public health act, food acts, environmental protection acts).
Local Government → infrastructure and policy (waste management services, licensing and auditing of food premises, enforcement of environmental protection legislation, health promotion programs, planning and development).
What was Ilona Kickbush’s commentary on health governance?
Global Health Governance: ‘those institutions and processes of governance which are related to an explicit health mandate, such as the World Health Organisation’.
Global Governance for Health: ‘those institutions and processes of global governance which have a direct and indirect health impact, such as the World Trade Organisation - many of these are related to the social determinants of health’.
The transition from International Health to Global Health recognises this differentiation between the ‘old architecture’ - Global Health Governance - WHO, Unicef and the other health multilaterals, and Global Governance for Health - agencies such as the World Bank, WTO etc. that have a direct or indirect impact on health.
Comment on the creation of WHO - in the shadows of WW2.
1946 International Conference on Health:
51 UN members, 13 non-members.
Approved World Health Organisation constitution.
1948 first World Health Assembly.
World Health Organisation incorporated PAHO (Washington), and new regional offices:
Europe (Copenhagen).
Eastern Mediterranean (Cairo).
Africa (Brazzavile).
South East Asia (New Delhi).
Western Pacific (Manila).
Comment on the WHO as the UN’s most ‘democratic’ agency.
World Health Assembly ‘most democratic UN process’.
One vote for each of 191 member countries.
WHO Executive: 32 countries.
Decentralised structure: regional offices autonomous.
Budgetary funds from country subscriptions.
Extra-budgetary funds from bilateral aid/philanthropy/donors - ¾ of the budget, ear-marked by donors:
Bilateral aid increasingly directed through multilateral agencies - but this varies.
Private sector/philanthropy significant contributors.
Donors effectively dictate WHO direction.
Comment on Dr Tedros’ claims for WHO as the director general.
First African Director General.
Endorsed by Bill and Hillary Clinton, George Bush, Barak Obama, etc.
Not a ‘real’ doctor, but Chair Global Fund, RBM.
Proven Health System reformer - massive increase in health centers, extension officers, doctors, but,
‘Dr Tedros uniquely stands out among the 9 WHO DGs for his high-level position in a repressive government’.
‘As health minister, the government failed to honestly and openly report several cholera outbreaks’.
First year in leadership:
He has confirmed and acted on his four policy priorities:
Universal Health Coverage (UHC) and PHC.
Global health emergencies.
Health for women, children, adolescents.
Health impact of climate change.
Ebola emergency response.
But Chan’s WHO reform processes have lapsed:
Tedros has increased women in leadership, but has added two layers to the WHO hierarchy.
Some political faux-pas: Mugabe as Goodwill Ambassador; Rwandan President Kagame (Chair African Union) as WHO Opening Day speaker.
Give a background on Halfdan Mahler - the WHO DG from 1973-1988.
Eradication programmes failing.
Shift towards development.
Increasing emphasis on health systems, district health.
Primary Health Care declaration.
Increasing controversy:
Code on Infant Formula (118:1).
Essential drugs (US objects).
Global alcohol report withdrawn.
Conflict over nuclear war.
Division on South Africa, Middle East.
Give a background on Hiroshi Nakajima - the WHO DG from 1988-1998.
Technological, managerial, disease-oriented approach.
Rapprochement with Big Pharma.
Cronyism, corruption, loss of policy focus, poor communication.
Did launch Global Polio Eradication, DOTS; Integrated Management of Childhood Illness Initiative.
Conflict with Jonathan Mann, head of WHO’s Global Program on AIDS, lost confidence and lead to creation of UNAIDS (1996).
Give a background on Gro Harlem Brundtland - the WHO DG from 1998 -2003.
‘Moral voice… technical leader’.
Creating One WHO, not 2, not 7.
Sweeping reform, renewed agenda:
Reducing burden of disease.
Reducing risks to health.
Sustainable health systems.
An ‘enabling’ policy framework.
New campaigns/partners: Roll Back Malaria, Framework Convention on Tobacco Control, GAVI, Global Fund.
Commission on Macroeconomics and Health, but WHR 2000: Health System Performance.
Give a background on Margaret Chan - the WHO DG from 2007 -2017.

Comment on the UN Children’s Emergency Fund.
United Nations’ Children’s Emergency Fund (Unicef), established by UN in 1946.
Mandate not limited to health: nutrition, breast-feeding, education, rights of the child.
36 member board, reports to UNESCO.
Structure more decentralised - HQ over 6 centres, 6 regional offices, country offices.
Decision making delegated to country representative - much more responsive organisation.
Funded by voluntary contributions - not subscriptions - but popular with bilateral donors.
Influence of donors significant.
Comment on Unicef and PHC.
Closely collaborated with WHO on PHC declaration at Alma Ata in 1978.
1938 State of the World’s Children report signaled shift to GOBI:
Growth monitoring for nutrition.
Oral rehydration for diarrhoeal disease.
Breast feeding.
Immunisation.
In 1948, expanded agenda to GOBI-FFF.
FFF = family planning, female education, and food supplementation.
Comment on Unicef beyond PHC.
Recognised falling child health status in 1980s.
Evaluation of International Monetary Fund structural adjustment lead to engagement with IMF/WB.
‘Adjustment with a human face’: mediating local impact of adjustment on children; interventions to reduce impact of changes, prioritise children, vulnerable.
Macroeconomic experience with WB/IMF lead to interest in efficient use of drugs.
Bamako Conference on essential drugs in PHC failed to consult WHO-strained relationships.
Issues of equity and access, greater emphasis on drugs.
Implications for essential drugs, privatization.
Comment on Unicef ‘taking its own road’.
Country programming has enabled flexibility and strong local alliances.
Millennium Development Goals have promoted Unicef’s agendas in child health, women’s health, and education.
MDG gains secured - and extended - in the SDGs.
Infant and child health, immunisation, gender quality, education, child rights.
Strategic exploitation of media exposure - strong public presence, direct appeal to public.
Successful use of bilateral agencies, philanthropy, major donors.
Give a background on the World Bank.
Created with International Monetary Foundation at Bretton Woods, 1944 - prior to end WW2.
Bretton Woods institutions consisted of:
International Bank for Reconstruction and Development (IBRD).
International Finance Corporation (IFC).
Multilateral Investment Guarantee Agency (MIGA).
No clear mandate for health.
Prior to early 1980s health not a priority: health focus legitimased through economics.
Since 1980s major funding agency for population and health issues.
Voting power within WB relates to funding - US dominates and PResident always US appointment.
Most UN countries are members - but dominated by richest economies.
90% funds borrowed on world capital markets - accountable to major contributors.
Policies neo-liberal - focus on economic growth.
Investment in health incremental in 1980s, arising from structural adjustment policies.
‘Adjustment with human face’.
Primary points of the World Development Report 1993: Investing in Health?
In 1993 - in absence of WHO leadership, World Bank fills policy vacuum in health.
Redefined health in economic terms.
Adapted DALY for use in policy.
Shifted focus to economic adult.
Allowed comparisons of health issues between and within countries.
Compared interventions for cost-efficiency using DALYs avoided.
Comment on the World Bank’s poverty reduction strategies.
Developed the Poverty Reduction Strategy Paper (PRSP) - now a pre-requisite for WB development loans, but also for country pro-poor planning.
Focus on poverty reduction, using a whole of government approach.
Integration of MDG metrics into reporting obligations as development indicators.
First wave of PRSPs were imitative - cut and paste - driven by World Bank consultants.
More recently, greater government ownership, more effective strategy, greater integration into policy.
Health policies reconfigured in terms of poverty.
Comment on the World Bank’s directions.
Criticism for history of secrecy, lack of legal and political accountability, US dominance.
In health, history of tensions with WHO.
Emphasis on market forces for change, neoliberal policy framing.
Strong support for privatization.
Redefining health in economic terms and structural adjustment questionable.
Macroeconomic interventions have had equivocal outcomes - often negative.
Despite mandate, policies tend to result in wealth transfers from South to North.
Comment on the ‘new’ players in health in this millenium.
World Trade Organisation - important because of the significant contribution of pharmaceuticals and the protections of patents, with TRIPS agreements negotiating flexibilities for public goods.
Philanthropy increasingly important - esp. Gates.
Criticisms levelled by various stakeholders: South-South aid undervalued, BRICS, Arab aid.
Private sector increasingly integral to global initiatives in partnerships with public institutions.
Global Governance for Health is a dynamic matrix - particularly since 2001.
Who are the new global players in health?
Globalisation has substantially changed Global Governance for Health, primarily through the creation of Public-Private Partnerships.
2000 Global Alliance for Vaccines and Immunisation (GAVI).
2001 Global Fund to fight AIDS, TB, malaria.
2001 Bill and Melinda Gates Foundation.
Other philanthropists.
Warren Buffett.
George Soros.
Comment on GAVI.
Secretariat in Geneva, Switzerland.
Aim - to increase access to immunisation in poor countries by bringin together country and donor governments, WHO, UNICEF, WB, vaccine industry in both industrialised and developing countries, research and technical agencies, civil society, BMGF, and other private philanthropists.
Optimise access to currently underused vaccines.
Strengthen health and immunisation systems.
Make innovation immunisation technology available.
Consistent performance, limited focus, link to MDG4 and SDG4.2 (infant mortality).
Comment on the challenges of GAVI.
Health System Strengthening (HSS) initiatives.
Continue specific work on immunisation.
Engage health systems as a whole.
Resolution;
Primacy of immunisation (non-negotiable).
Limit HSS to immunisation systems.
Paris Principles - ensure country-driven approach, aligned with national planning and budgetary cycles, utilising MoH structures and processes for the coordination and support of health systems.
Health workforce, supply, distribution and maintenance systems for primary healthcare at district level and below.
Maintaining funding base (2000-2020) from diverse sources.
‘Graduating’ low income countries.
Comment on the Global Fund.
Public-private partnership, secretariat in Geneva, Switzerland.
Proposed at G8 Okinawa, 2000.
Massive Attack on Diseases of Poverty (MAD-OP) - malaria, Tb, unsafe pregnancy, AIDS, diarrhoea, ARI, measles, neglected tropical diseases, effective and responsive healthcare.
Focus initially on HIV: strong lobby for malaria, Tb.
International financing organisation: world’s largest financier of anti-AIDS, Tb, malaria programs.
Comment on the challenges of the Global Fund.
Much larger than GAVI, focus wider.
Poorly managed engagement with HSS.
Community Control Mechanisms broaden engagement away from government monopolies on funding, but create internal disputes.
Challenges with corruption: Uganda, Zimbabwe, Phillippines, Ukraine.
Failure of Round 11 halted new distributions to 2014.
Essential services maintained.
Replenishments since then difficult despite reform.
Challenges to expand to Global Fund for All.
Bill and Melinda Gates Foundation and criticisms from some stakeholders 🙂


Comment on global migratory patterns and trends.
Estimate of 281 million international migrants (3.6% of the world’s population) and significantly more internal migrants - people moving within their country of birth.
Migrant workers are estimated to account for 150.3 million of the 244 million international migrants.
The vast majority of people int he world continue to live in the country in which they were born, more people are migrating to other countries, especially those within their region.
Why do some definitions of ‘international migrant’ differ?
Various definitions that can stem from legal, policy, demographic, and other contexts.
While UN Statistical Commission prescribes a specific definition based on foreign-born, some analysts deploy other definitions for analytical purposes.
The 2023 World Development Report (WDR), chose to use a more limited definition by excluding from the UN DESA International Migrant Stock data migrants who had become citizens of the country to which they had migrated.
WDR provides perspective of migrants that encompasses all policy categories (including refugees), while overlaying a citizenship policy boundary even though acceptance by States of dual citizenship has increased significantly in recent years.
Comment on the relationship between work and migration.
Work is the major reason people migrate internationally.
Migrant workers constitute large majority of world’s international migrants, with most living in HICs. Global displacement at record high, with number of Internationally displaced at around 71.2 million, and the number of refugees and asylum seekers at 40.7 million.
Bidirectional relationship between migration and health remains poorly understood, and action on migration and health remains limited.
Comment on the concept of labour migration.
Key driver of global economic growth.
Migrants fill critical labour and skills shortages.
Sustain essential industries.
Contribute to development through remittances and knowledge exchange.
Yet:
Contributions of labour migration depend on how effectively it is governed.
Well-designed pathways can facilitate safe and orderly labour mobility.
Gaps in governance may lead to skills mismatches, underemployment and vulnerabilities for migrant workers.
India Case Study 🙂
After China, India has the largest diaspora with over 22 million people living outside India.
Initially to Europe (UK).
Trinidad and Tobago, Guyana, South Africa, Mauritius, Fiji, Suriname, Kenya, Uganda.
1970s UAE, Saudi Arabia, Kuwait, Bahrain.
Australia, US, UK.
Emigration of skilled and professional class.
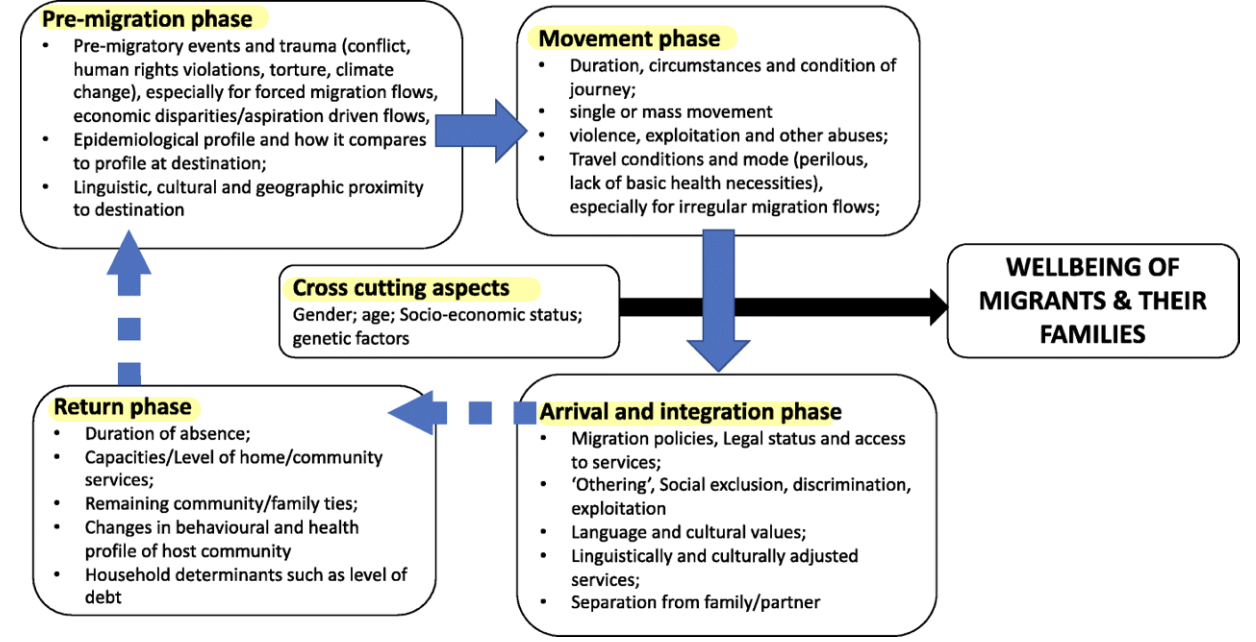
Comment on the implications of population movement.
Shifting populations affect health in complex ways:
Movement of people from one geographical space to another.
Production and management of risk, illness, health, and access to health services.
Chronic and infectious diseases.
Work-related health risks.
Psychosocial wellbeing.
Maternal and child health.
Comment on the process of crossing medical systems in relation to migration.
Migrants move not only across geographical borders (transnational migration), but also across, between, and among medical systems.
Significant changes in risks to health and therapeutic options accompany migration, but the vary in relation to features of migrant populations such as gender, ethnicity, class, and legal status.
Why is immigrant health important?
If one accepts the premise that health should be a basic human right (WHO, 2003), principles of distributive justice underscore the ethical unacceptability of neglecting… immigrant health concerns (Beauchamp and Childress, 2006).
Comment on the notion of diversity with regard to migrants.
Immigrant populations are diverse.
Educated elites.
Migrants seeking work in more affluent societies.
Refugees, asylum seekers.
Women, men, children.
Comment on the SDGs with regard to migration.
SDGs identify migration as both a catalyst and a driver for sustainable development.
While UHC aims at ensuring ‘everyone’ can access affordable health systems without increasing the risk of financial ruin or impoverishment, the formulation of UHC remains unclear regarding non-nationals/non-citizens.
Voluntary or involuntary migration 🙂