Urinary and Male Reproductive Disorders
1/101
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
102 Terms
24-Hour Urine Specimen Start Protocol
Have patient void, discard first specimen, then collect all subsequent urine for 24 hours.
24-Hour Urine Specimen Missed Sample Action
Restart the entire 24-hour collection process from the beginning.
Ideal Time for Urinalysis Collection
Early morning, as it provides a more concentrated urine sample.
Significance of Glucose, Ketones, and Protein in Urine
Abnormal findings indicating potential diabetes mellitus, fat metabolism, infection, or cancer.
Key Nursing Action Prior to CT Scan with IV Contrast
Ask for iodine/shellfish allergies, establish IV access, and check for Metformin use.
Hydration Recommendation After Contrast Media Radiography
Increase fluid intake to flush contrast and prevent contrast-induced kidney injury.
Essential Pre-MRI Assessment
Screen the patient for metal implants, pacemakers, or any metallic objects.
Cystography vs. Voiding Cystourethrogram (VCUG)
Cystography detects bladder injury; VCUG uses x-rays during urination to detect ureteral reflux.
Nephrotoxicity Risk of Cystography Contrast
Not nephrotoxic, as contrast is instilled directly into bladder and doesn't enter bloodstream.
Post-Cystourethrogram Monitoring Window
Monitor for urinary tract infection signs for 72 hours after the procedure.
Pre-Procedure Positioning for Kidney Biopsy
Prone position with a pillow placed under the patient's abdomen.
Post-Kidney Biopsy Laboratory Monitoring
Monitor hemoglobin and hematocrit levels to detect internal bleeding.
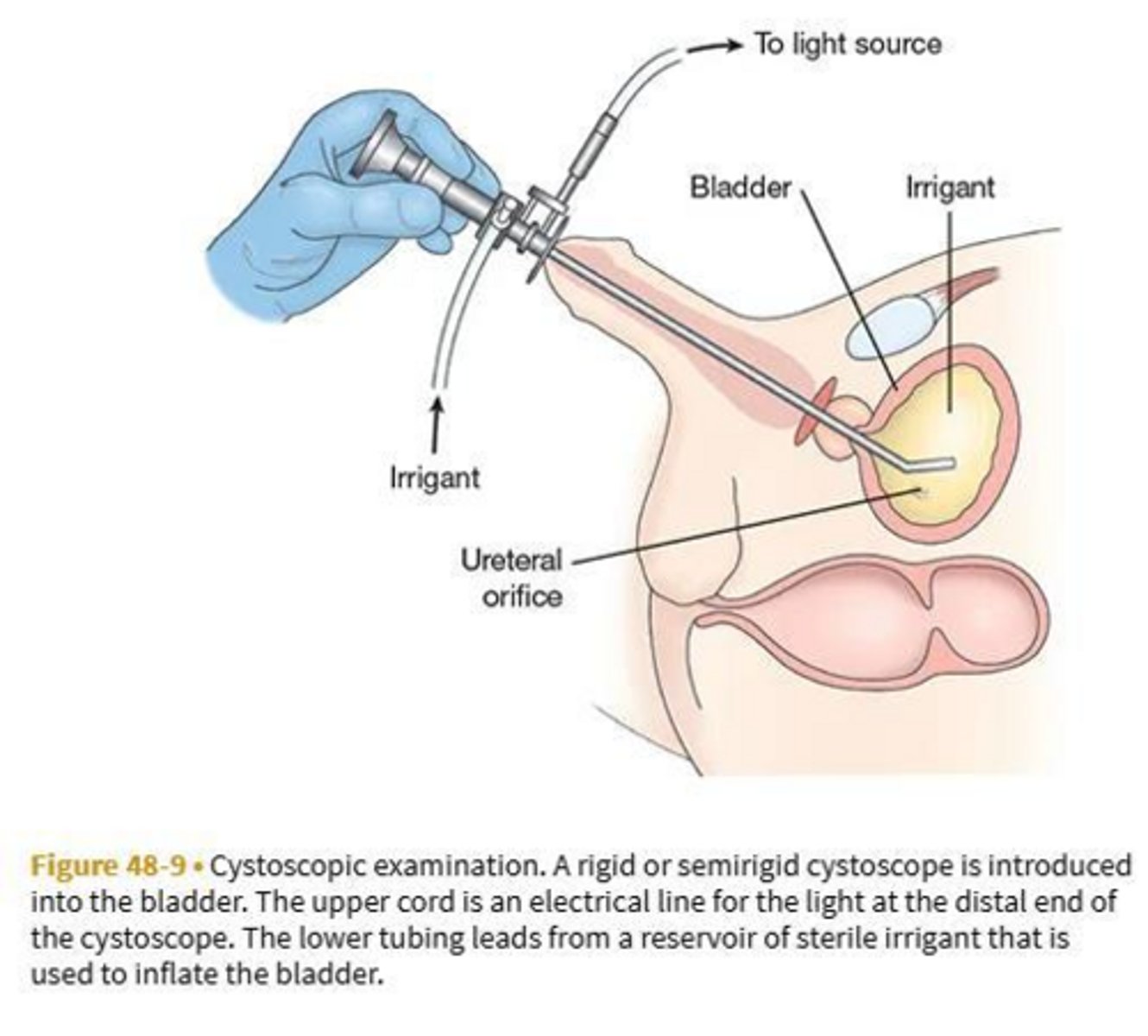
Nurse Action for Decreased Urine Output Post-Cystoscopy
Irrigate the urinary catheter if blood clots are present or output is absent.
Target Symptoms to Report 72 Hours Post-Cystoscopy
Urinary retention, gross hematuria, severe abdominal pain, fever, chills, or dysuria.
Retrograde Pyelogram Purpose
Identifies obstruction or structural disorders of ureters and the renal pelvis.
Cystogram vs. Urethrogram Diagnostic Focus
Cystogram identifies bladder fistulas/diverticula/tumors; urethrogram identifies urethral structural details.
Renal Scan Function
Assesses renal blood flow and estimates glomerular filtration rate (GFR) via radioisotopes.
Captopril Risk During Renal Scan
Increases risk of orthostatic hypotension; monitor vitals and encourage fluids post-scan.
Excretory Urography Metformin Protocol
Withhold Metformin 24 hours before and 48 hours after contrast administration.
Expected vs. Reportable Urine Post-Excretory Urography
Pink-tinged urine is expected; frank hematuria or blood clots must be reported.
Definition of CAUTI
Urinary tract infection developed 2 or more days after catheter insertion.
Lower vs. Upper UTI Classifications
Lower includes cystitis, prostatitis, urethritis; Upper includes pyelonephritis and renal abscess.
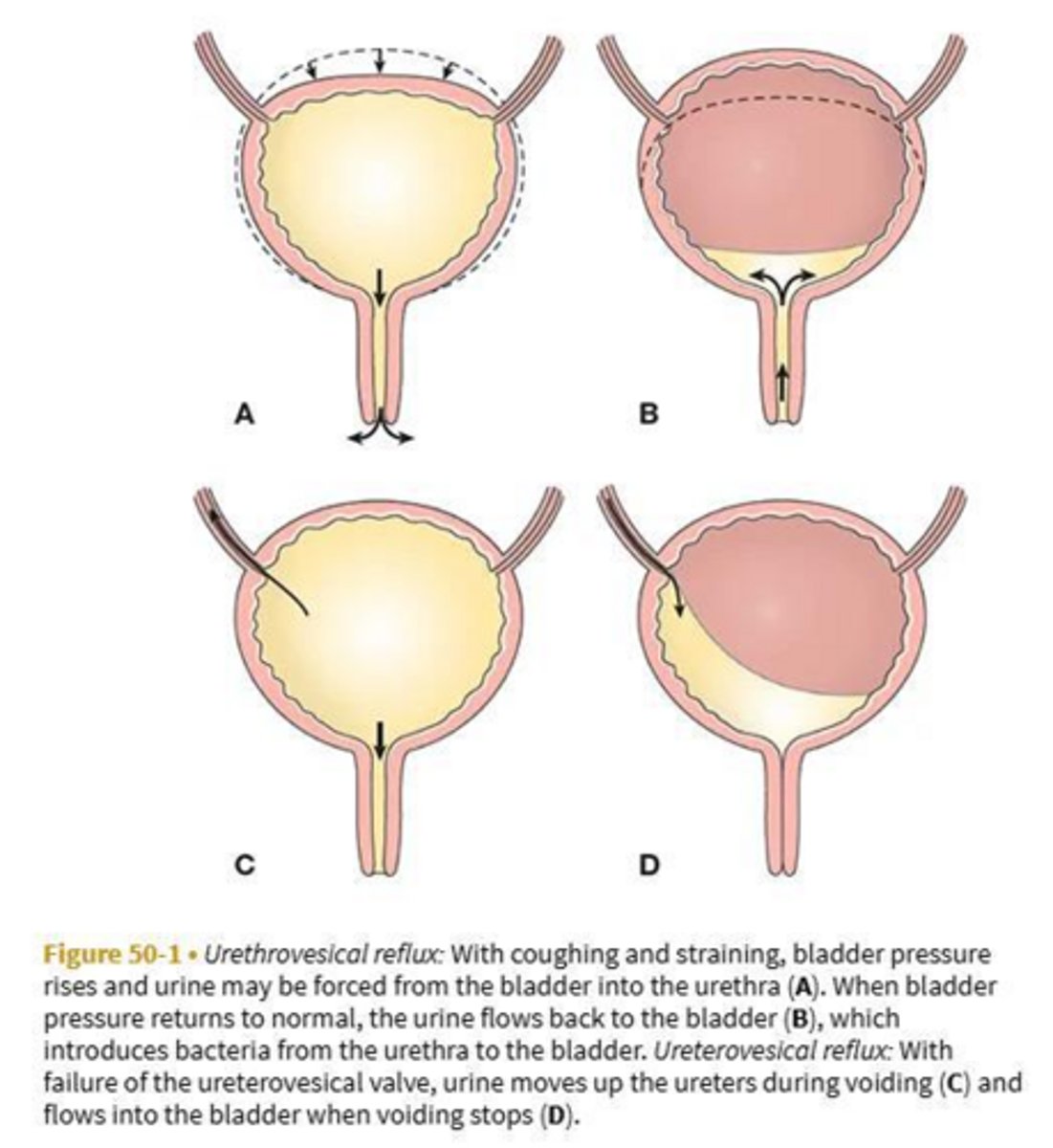
Urethrovesical Reflux Mechanism
Backflow of urine from the urethra into the bladder.
Ureterovesical Reflux Mechanism
Backflow of urine from the bladder into one or both ureters.
Three Routes of Bacterial Invasion in UTIs
Transurethral (ascending), bloodstream (hematogenous), and direct extension via intestinal fistula.
Primary Clinical Presentation of Geriatric Urosepsis
Hypotension, tachycardia, tachypnea, fever, and acute delirium or confusion.
Uncomplicated vs. Complicated UTI
Uncomplicated is simple localized burning/frequency; complicated coexists with systemic illness or anatomical issues.
Key Urinalysis Markers for Active UTI
Positive leukocyte esterase, positive nitrites, sediment, and elevated WBCs/RBCs.
Transrectal Ultrasonography (TRUS) Indication
Evaluates prostate and bladder conditions specifically in male patients.
Dietary Irritants to Avoid in Active UTI
Coffee, tea, citrus, spices, cola, and alcohol.
Perineal Hygiene Education for Females
Wipe the perineal area strictly from front to back after elimination.
Clothing Modifications to Prevent UTIs
Avoid pantyhose with slacks, tight clothing, and synthetic underwear.
Long-Term Complications of Unresolved UTIs
Gram-negative urosepsis, acute kidney injury, and chronic kidney disease.
Pathophysiology of Acute Pyelonephritis
Active bacterial infection causing interstitial inflammation, tubular necrosis, and temporary renal impairment.
Pathophysiology of Chronic Pyelonephritis
Repeated infections causing progressive inflammation, post-inflammatory fibrosis, and permanent renal scarring.
Classic Clinical Signs of Pyelonephritis
Chills, fever, flank pain, and costovertebral angle (CVA) tenderness.
Serum Lab Elevations in Pyelonephritis
Elevated serum creatinine, BUN, C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR).
Recommended Fluid Intake for Pyelonephritis
Increase oral fluid intake to 3 to 4 liters per day unless contraindicated.
Pyelolithotomy Definition
Surgical removal of a large kidney stone blocking urine flow from the pelvis.
Ureteroplasty Purpose
Repair or revision of the ureter, often involving reimplantation to preserve function.
Chronic Kidney Disease Sign in Pyelonephritis
Hypertension combined with persistently elevated BUN, creatinine, and electrolyte imbalances.
Primary Trigger for Glomerulonephritis
An immunologic reaction following an infection, particularly skin or upper respiratory streptococcal infections.
Glomerulonephritis Urine Characteristics
Reddish-brown, smoky, or cola-colored urine due to hematuria.
Fluid Volume Excess Signs in Glomerulonephritis
Edema (hands/face/eyes), crackles in lungs, S3 heart sound, dyspnea, and weight gain.
Gold Standard Diagnostic for Glomerulonephritis
Kidney biopsy to confirm diagnosis, determine prognosis, and guide treatment.
Electrolyte Imbalances in Glomerulonephritis
Hyperkalemia, hyperphosphatemia, and hypocalcemia.
Stress Management in Glomerulonephritis
Teach relaxation exercises to decrease systemic stress and help lower blood pressure.
Stress Urinary Incontinence Cause
Intact urethra but pelvic floor weakness; triggered by coughing, sneezing, or laughing.
Urge Urinary Incontinence Mechanism
Strong, unstoppable urge to void caused by neurologic dysfunction inhibiting bladder contraction.
Functional Urinary Incontinence Definition
Involuntary urine loss due to physical or cognitive impairments preventing timely toileting.
Iatrogenic Urinary Incontinence Cause
Extrinsic medical factors, such as medications like alpha-adrenergics for hypertension.
Overflow Urinary Incontinence Mechanism
Continual leakage of urine from an overdistended, poorly contracting bladder.
Bladder Irritants to Avoid for Incontinence
Alcohol, carbonation, caffeine, and artificial sweeteners.
Pharmacologic Management for Urge Incontinence
Anticholinergics and amitriptyline to inhibit bladder contractions.
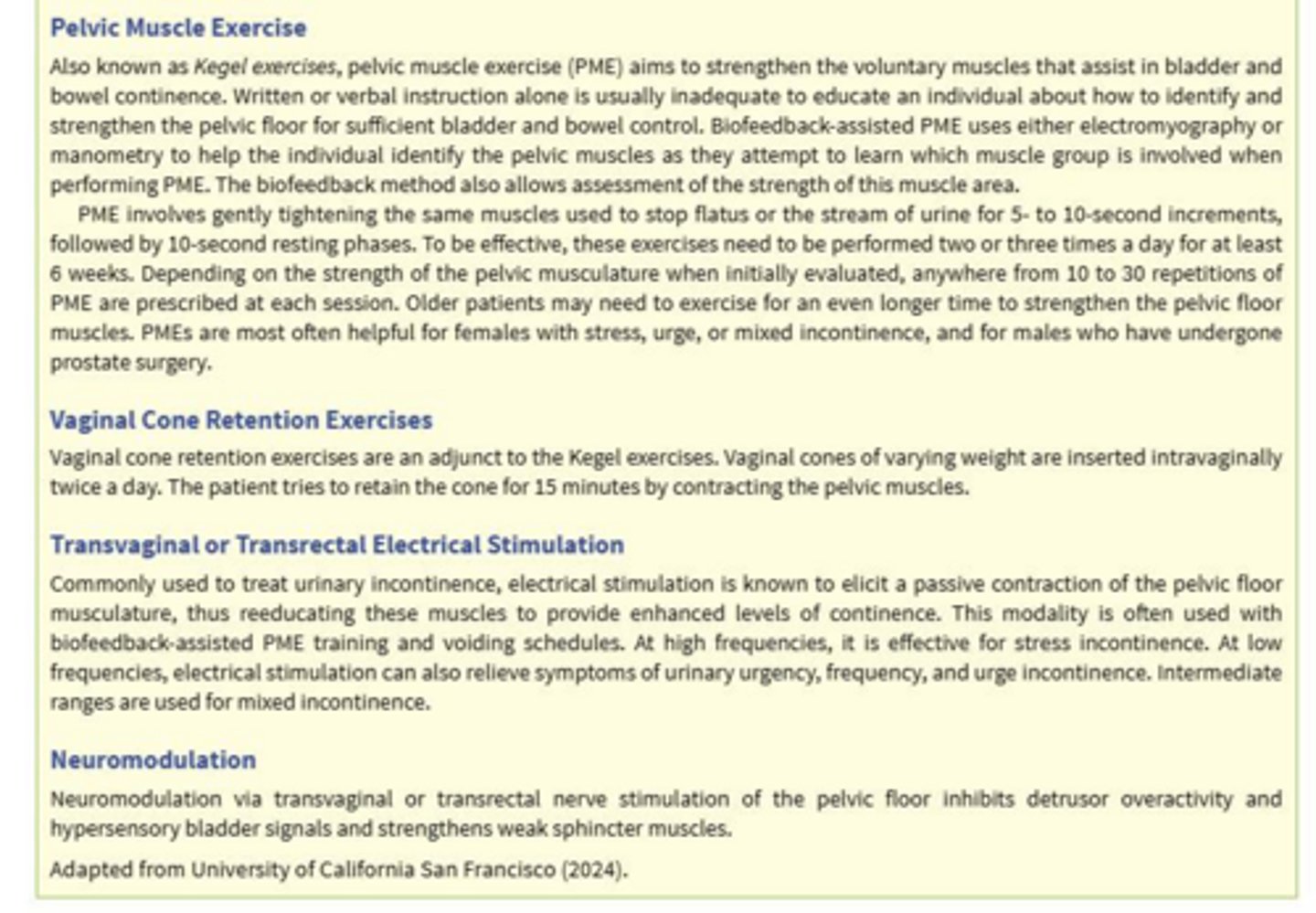
Vaginal Cone Therapy Protocol
Insert twice daily; contract pelvic muscles to retain cone for 15 minutes.
Normal Aging Postvoid Residual (PVR)
Adults 60 and older may normally have 50 to 100 mL remaining.
Anesthetic Effect on Bladder Retention
Suppresses urge to void and reduces bladder muscle innervation postoperatively.
Maximum Normal PVR in Middle-Aged Adults
No more than 50 mL of residual urine.
Non-Invasive Nursing Measures to Promote Urination
Running water, warm perineal compresses, hot drinks, or stroking inner thighs.
Suprapubic Catheter Indications
Urethral route impassable due to injuries, strictures, prostatic obstruction, or pelvic fractures.
Permanent Suprapubic Catheter Use Case
Spinal cord injury causing neurogenic bladder or bladder areflexia.
Urolithiasis vs. Nephrolithiasis
Urolithiasis is stones in the urinary tract; nephrolithiasis is stones in the kidney.
Renal Colic Pain Pathway
Intense flank pain radiating to the lower abdomen, scrotum, testes, or vulva.
Stone in Renal Pelvis Manifestations
Hematuria, pyuria, and an intense deep ache in the costovertebral area.
Stone in Ureter Manifestations
Acute, excruciating, colicky, wave-like pain radiating to the thigh and pelvic area.
Stone in Bladder Neck Complication
Acute urinary retention and severe localized irritation.
Key Nursing Action for Passed Calculi
Strain all urine, retrieve the stone, and send it to the lab.
Target Urine Output for Stone Prevention
Exceed 2 liters of urine output per day.
Nutritional Therapy for Calcium Stones
Restrict dietary calcium; utilize thiazide diuretics if hyperparathyroidism is present.
Low-Purine Diet Avoidance List
Shellfish, anchovies, asparagus, mushrooms, and organ meats.
Nutritional Therapy for Cystine Stones
Implement a low-protein diet.
Dietary Restrictions for Oxalate Stones
Avoid spinach, Swiss chard, chocolate, peanuts, and pecans.
Chemolysis Definition
Chemical instillation used to directly dissolve urinary calculi.
Extracorporeal Shock Wave Lithotripsy (ESWL)
Non-invasive shock waves break stones into sand-like particles for passage.
Hydronephrosis Complication of Stones
Calculus completely blocks the urinary tract, causing backflow and kidney distention.
Classic Triad of Urethral Trauma
Blood visible at the meatus, inability to void, and a distended bladder.
Leading Risk Factor for Bladder Cancer
Tobacco smoking significantly increases risk.
Primary Clinical Manifestation of Bladder Cancer
Visible, painless hematuria.
Intravesical BCG Therapy Protocol
Instilled for 1 year; uses Mycobacterium bovis to produce a local immune response.
Radical Cystectomy Scope in Men
Removal of the bladder, prostate gland, and seminal vesicles.
Radical Cystectomy Scope in Women
Removal of bladder, lower ureters, uterus, fallopian tubes, ovaries, and anterior vagina.
Cutaneous vs. Continent Urinary Diversion
Cutaneous drains continuously; continent uses an internal reservoir accessed via catheter.
Immediate Postoperative Urinary Diversion Monitoring
Monitor and document urine volume hourly.
Top Three Postoperative Complications of Stomas
Stoma ischemia/necrosis, stoma retraction/separation, and peritonitis.
Digital Rectal Exam (DRE) Screening Guidelines
Annually for men over 50; over 45 for high-risk (African American, family history).
Normal Prostate-Specific Antigen (PSA) Level
Safe range is 0 to 2.5 ng/mL.
Highly Suspicious PSA Level for Cancer
10 ng/mL and above indicates a 50% chance of prostate cancer.
Early Prostate Cancer Antigen (EPCA-2) Significance
Value of 30 ng/mL or greater is highly suggestive of prostate cancer.
Transrectal Ultrasound (TRUS) Pre-Procedure Requirement
Administration of an enema prior to the procedure.
Sildenafil (Viagra) Absolute Contraindication
Concurrent use of organic nitrates (nitroglycerin) due to severe hypotension risk.
Priapism Definition and Risk
Persistent, painful, abnormal erection lasting over 4 hours; medical emergency.
Acute vs. Chronic Bacterial Prostatitis Symptoms
Acute has sudden fever, dysuria, and perineal pain; chronic is typically asymptomatic.
Alpha-Adrenergic Blockers for BPH Action
Relax smooth muscle of the bladder neck and prostate to improve urine flow.
5-Alpha-Reductase Inhibitors for BPH Action
Prevent conversion of testosterone, gradually shrinking the prostate gland tissue.
Transurethral Resection of the Prostate (TURP)
Surgical removal of prostate tissue using a resectoscope inserted through the urethra.
Transurethral Resection (TUR) Syndrome Signs
Hyponatremia and hypervolemia due to absorption of bladder irrigation solution.
CBI True Urine Output Calculation Formula
Total fluid output minus total sterile irrigant infused equals true urine output.
CBI Calculation Example (3L hung, 2L left, 1.6L output)
1600 mL (total output) - 1000 mL (infused) = 600 mL true urine.
Post-Prostatectomy Activity Restrictions
Avoid straining, heavy lifting, and long car trips for 6 to 8 weeks.
Testicular Torsion Definition
Rotation of the testicle twisting the spermatic cord, rapidly reducing blood flow.