NSG 506 - Complex Care Nursing of the Older Adult [Exam 1] Questions with 100% accurate solutions+ rationales 2026
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
Geriatric Syndromes
-Term used to capture certain clinical conditions in older people that do not necessarily fit into discrete categories
-Often related to physiological changes of aging
-Atypical presentation
types of geriatric syndromes
-Frailty
-Delirium
-Falls/Dizziness/Syncope
-Sleep problems
-Urinary Incontinence
Age-Friendly Health System
Value is optimized for all — patients, families, caregivers, health care providers, and the overall system.
An Age-Friendly Health System is one in which every older adult's care is:
-Guided by an essential set of evidence-based practices ("4Ms" - What Matters, Medication, Mentation, Mobility);
-Causes no harms
-Is consistent with What Matters to the older adult and their family.
Why an age-friendly system?
-Avoid costs associated with poor quality care
-Deliver care in a more cost-effective manner
-Aligned with Rush's mission and vision
-The right thing to do
4Ms Framework
what matters, medication, mentation, mobility
What Matters
What is important to the patient
-Do not make assumptions, listen to the patient
-Helps align goals of care
-Ex: pain control vs lucidity, functional status, ability to interact with friends/family
-Often influenced by culture, religion, life experiences etc.
-Important to involve family/caregivers in discussions
-Assess their needs and ability to care for the patient
-Advocate for the patient's preferences and ensure the whole team understands
-Often involves care coordination
-This includes discussions around advanced directives
-More likely to discuss if feel part of the team
Mobility
-Goal: Ensure safety while maintaining functional status so they can "Do what matters"
-Assessing for mobility and functional status goals
-Assessing for and implementing interventions to reduce fall risk
-In acute care setting: Goal is to maintain or improve pre-admission functional status
-Ambulate, get into chair, ROM exercises etc.
-Increased mobility actually reduces fall risk
-If patient already a fall risk just need to ensure safety
-Acutely, limited mobility can lead to changes in mentation and decline in overall functional status
-Need to collaborate as a healthcare interdisciplinary team
Medications
Ensuring all medications are appropriate, have a purpose, and are being used correctly.
Medication use in older adults
1. Metabolic changes and decreased drug clearance associated with aging
2. Multiple prescriptions increases the possibility of "prescribing cascades".
A prescribing cascade develops when an adverse drug event is misinterpreted as a new medical condition and additional drug therapy is then prescribed
3. Use of multiple medications can lead to problems with medication adherence
4. Some medications put older adults at increased risk for adverse outcomes, Includes effects of mobility and mentation
prescribing cascade
Prescribing a new drug to treat the side effects of a previously prescribed drug; the symptoms of the first drug may be evaluated as part of the medical problem
together account for over 1/3 of emergency department visits for adverse drug reactions among older adults, because they are highly dangerous when they are used incorrectly or when side effects occur
-warfarin (bleeding with falls)
-insulin (hypoglycemia)
-digoxin (toxicity)
Polymedicine
-The use of an increasing number of drugs related to an increasing number of medical problems.
-More than one agent needed to treat a condition
-Comorbidities
-Health maintenance: vitamins, etc.
Polymedicine vs. Polypharmacy
polymedicine = good
polypharmacy = bad
Polypharmacy
•The inappropriate use of multiple drugs
•No indication
•Duplication of therapy
•Treating side-effects
•Includes OTC medications/supplements
•Increases risk for adverse reactions regardless of age
Roads to Polypharmacy
•Excessive prescribing: multiple comorbidities, treating side effects
•Multiple prescribers/dispensers and lack of coordinating provider
•Impairments in vision/dexterity
•Self-medication: OTC's, homeopathy, non-dietary herbal supplementation, "borrowing", reusing
Issues with Polypharmacy
•Increased monetary expenditures
•Increased incidence/severity of adverse effects
•Increased risk of drug interactions
•Difficulty with adherence
•Increased caregiver time
•Increased morbidity/mortality
•Decreased quality of life
Identify Potentially Inappropriate Medication Use
-Full medication reconciliation every admission, office visit, and care transition
-Identify any drug interactions
-Identify medications that pose high risk for adverse reactions
-Ensure formulation is still appropriate
-Identify any potential medications that are unnecessary and collaborate with team to get them deprescribed
Screening tools for medication use
-Beer's Criteria
-STOPP (screening tool of older people's prescriptions)
-START (screening tool to alert to right treatment) criteria, and the Medication Appropriateness Index
Beer's Criteria
-Consensus criteria for improving medication safety in the older adult population
-Intended for use in all ambulatory and institutional settings of care for populations aged 65 and older
-Goal is to improve care of older adults by reducing their exposure to potentially inappropriate medications
Medications that should not be routinely used or limited in use due to:
•Safety concerns - Adverse Drug Reactions, interactions
•Potential drug-disease interactions
•Higher dosing increases risk for ADRs
•Frequent dosing increases risk for ADRs
•Length of treatment increases risk for ADRs
Medication Education
-Ensure patient and caregivers understand purpose behind various medications
-Are able to access medications (cost etc.)
-Ensure taking appropriately
-Are aware of side effects and what to watch for
-Have the tools to take medications at home safely: Ex: BP cuff for HTN meds
-Understand why medications being removed if deprescribing
-Know how to ask questions/advocate when a new medication is suggested by healthcare provider
Mentation
-Assessing for, identifying, managing and treating: Depression, Delirium, and Dementia
-Important to know the patient's baseline so can determine any/the degree of alteration
-Family/caregivers vital role
Mental status assessment involves
-level of consciousness
-orientation (confusion assessment)
Level of Consciousness
AVPU
•A - Alert
•V - Verbal
•P - Pain
•U - Unconscious
Ex: Dementia does not affect level of consciousness
Orientation
•Person, Place, Time,
•Can also include situation
•Ex: Dementia affects orientation
•Usually predictable order - Time, Place, Person
•Important to note what patient oriented to if not fully oriented and what their baseline is
The 3 D's
delirium, dementia, depression
Depression
-Incidence increases with age and chronic illness
-Depression on top of dementia can make dementia worse
-treat depression can improve symptoms of dementia
-can stem from a caregiver's own depression and a change in the relationship between the two people
-Ensuring older adults are able to do What Matters can assist in preventing depression
Diagnostic criterion for depression:
Symptoms of depressed mood and diminished pleasure (anhedonia) + four or more additional depression symptom
Assessment for depression
Geriatric Depression Scale
-15 item yes/no questionnaire
-Important to involve caregivers in discussion
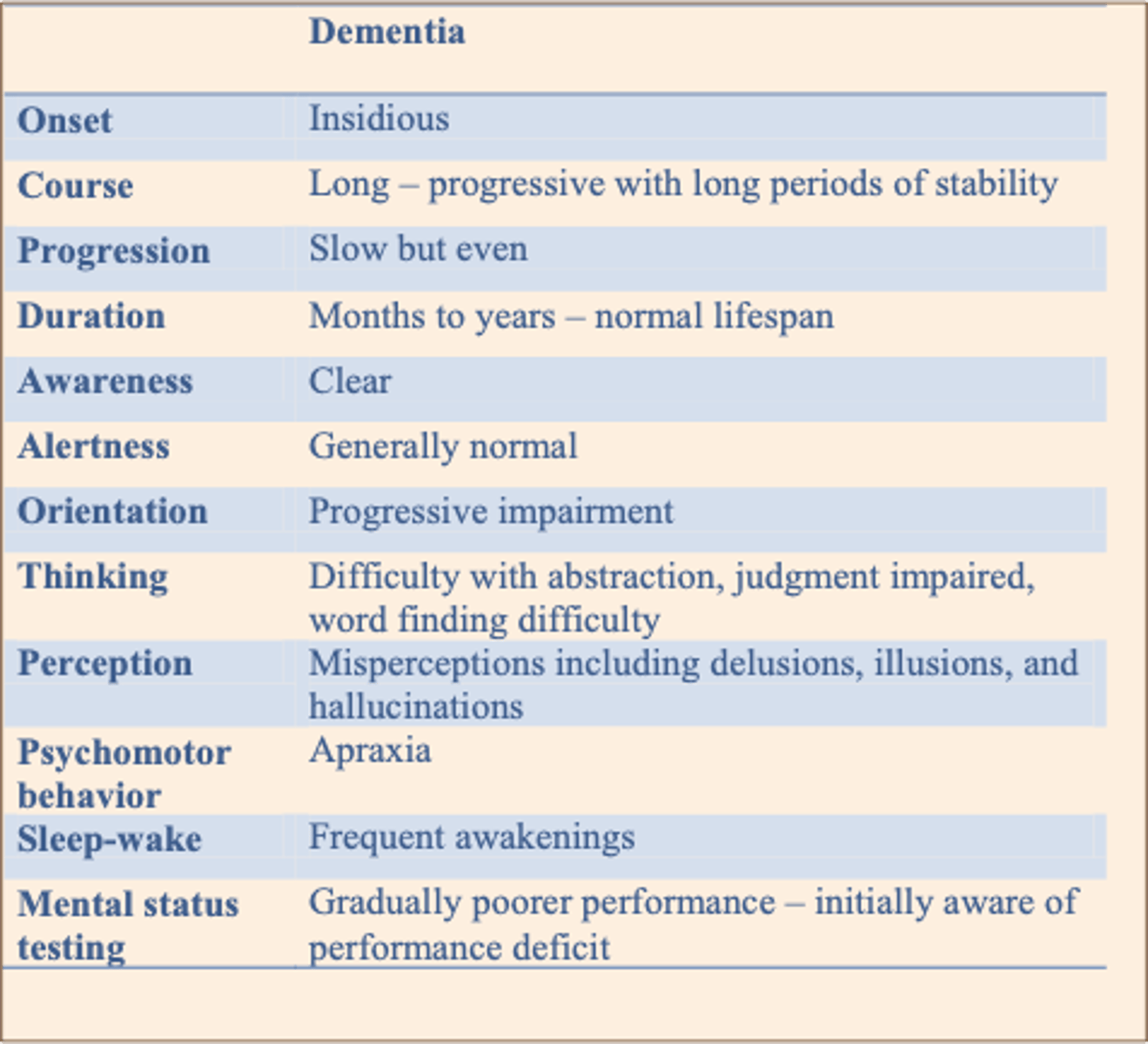
Dementia
The etiologies for dementia include
•Alzheimer's disease
•Vascular dementia
•Parkinson's dementia
•Lewy body dementia
•Frontotemporal dementia
Goals of care must always be directed towards providing/ increasing quality of life
Dementia Features/Symptoms
Nursing Management of the Patient with Dementia
Behavioral symptoms
-Remember, all behavior is meaningful, but communication is not necessarily clear.
-First, assess for physical problems that may be a trigger for behavioral symptoms.
-Wandering, screaming, and aggression (Risk for violence/Risk for injury): Occurs in over 50% of dementia patients
-Ensure appropriate goals and expectations
-Priority is SAFETY
-Rule out other causes of inappropriate behavior: pain (UTI, fracture), medications side effects or interactions
-Sensory – ensure they have hearing aids, dentures, glasses etc.
-Provide reorientation and assurances of safety
-Ensure staff introduce themselves when entering room
-Write date on white board, have pictures of loved ones etc.
Delirium
-Most frequent complication of hospitalized Older Adults
•Affects up to 50% of hospitalized older adults
•A state of acute mental confusion
•Under-recognized disorder & underdiagnosed!
•Often reversible
•May be life-threatening
-Use CAM scale
4 Features of Delirium that distinguish it from other cognitive impairment
-Status altered from baseline (acute onset or fluctuating)
-Inattention
-Disorganized thinking
-Altered level of consciousness
Delirium most at risk:
-older adults with dementia
-advanced age
-comorbid physical issues
-Immobility
-sleep deprivation
-Dehydration
-Pain
-sensory impairment
Risk factors for delirium
-Medication(s) (Try This: Beers Criteria)
-Fecal impaction
-Urinary retention
-Infection (urine, lungs, skin)
-Hypoxia
-Dehydration
-Hypo/hyperglycemia
-Pain (See Try This: Assessing Pain)
-Immobility
-Sensory impairment
Three main presentations delirium:
•Hyperactive (most recognized)
•Hypoactive (under recognized)
•Mixed (highest risk for morbidity/mortality)
hyperactive delirium
•↑ psychomotor activity (agitation, mood labiality, refusal to cooperate, disruptive behaviors, combativeness)
hypoactive delirium
•↓ psychomotor activity (sluggish, lethargic, withdrawn, apathy)
mixed delirium
-fluctuating course
-highest risk for morbidity/mortality
Delirium management main components
-Identification and treatment of etiology of delirium
-Environmental modification
-Control of symptoms
Pharmacologic treatment
Delirium management pharmacologic treatment
Haldol most studied (Starting dose 0.5mg; max 3-5mg/24 hr. (start low, go slow)
Haldol for delirium
-Sedates, treats hallucinations, paranoia, delusions, less hypotensive & anticholinergic
Nonpharmacological treatment of delirium
-Speak slowly and keep instructions simple.
-Do not argue about things they see, hear, or believe that are not accurate—instead, reassure them that they are safe.
-Avoid restraints - will cause more problems than help
-Encourage familiar faces for reassurance e.g. family members
-Meet basic needs: Fluids, nutrition, toileting
-Low stimulation - avoid/decrease excessive noise
-Ensure adequate sleep
-Provide orientation (calendar, clock)
-Correct sensory impairment e.g. glasses, hearing aids
-May take days, weeks, months to clear