Looks like no one added any tags here yet for you.
identify different arthropod vectors
Hematophagous arthropods
Mosquitos (aedes aegypti, anopheles), flea, black fly, sand fly, kissing bug
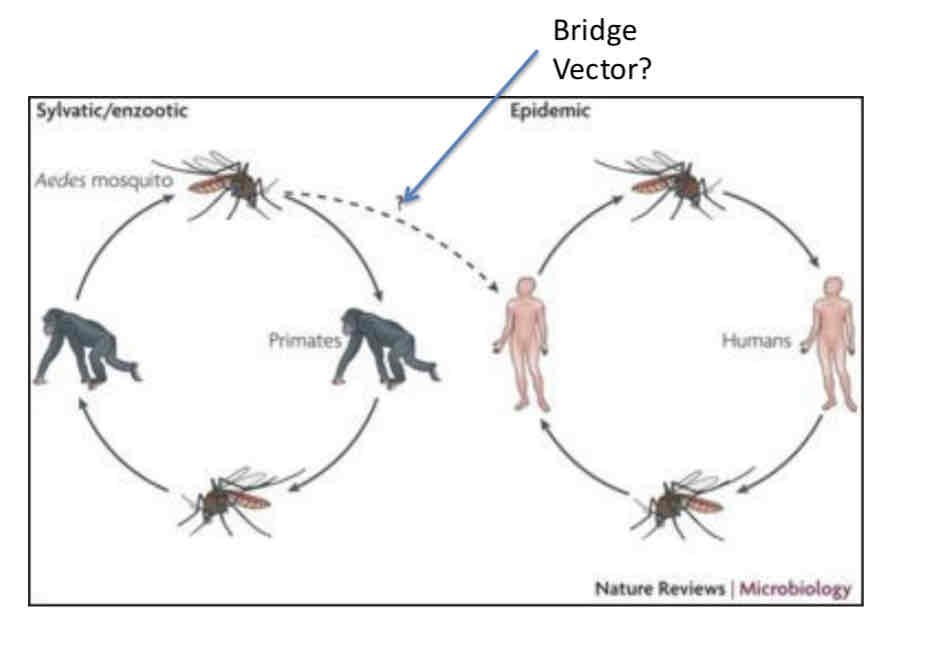
Explain simple and complex transmission cycles
Identify types of questions that are important in arthropod transmission
What factors contribute to outbreak?
Population levels, location, breeding habits of vectors?
How and where do humans interact with vector?
How do environmental factors affect human, vector, and reservoir behavior?
Describe the main virus families transmitted by mosquitoes
Flaviviruses, alphaviruses - icosahedral, positive sense, enveloped
bunyaviruses - plieomorphic, negative sense, envelope
Explain the basics of mosquito behavior and anatomy and how it aids in transmission
Anatomy
1. Proboscis: Mosquitoes use their proboscis to pierce the skin and feed on blood. During this, they can inject the dengue virus into the bloodstream.
2. Salivary Glands: The virus can be present in the mosquito’s saliva, which is transferred during feeding.
Behavior
1. Feeding: Female mosquitoes require blood for egg development. If they feed on an infected person, they can carry and transmit the virus to others.
2. Active During Day: Aedes mosquitoes are most active in the early morning and late afternoon, increasing human contact and transmission chances.
3. Attraction to Humans: They are attracted to human scent and carbon dioxide, making humans their preferred hosts.
4. Multiple Feedings: Mosquitoes can bite multiple people over their lifespan, spreading the virus to various individuals.
Transmission
After feeding on an infected person, the virus incubates in the mosquito for up to two weeks, allowing it to spread to other humans during subsequent blood meals.
Explain the pathway of infection in mosquitoes
Virus taken up in blood meal
Enters midgut
Infects midgut and breeches barrier
Transmits through hemocoel to salivary glands
Infects salivary glands and grows to high titers
Explain the pattern of infection used in mosquitoes and why that is beneficial
1. Acute – high level replication with rapid (days) resolution
2. Chronic/persistent – constant replication either at low level, or high level with immune evasion
3. Latent – high level replication followed by almost complete quiescence. Can reactivate
Identify the major pathways involved in mosquito immunity
RNAi (primary antiviral defense), Toll, Imd, Jak-STAT
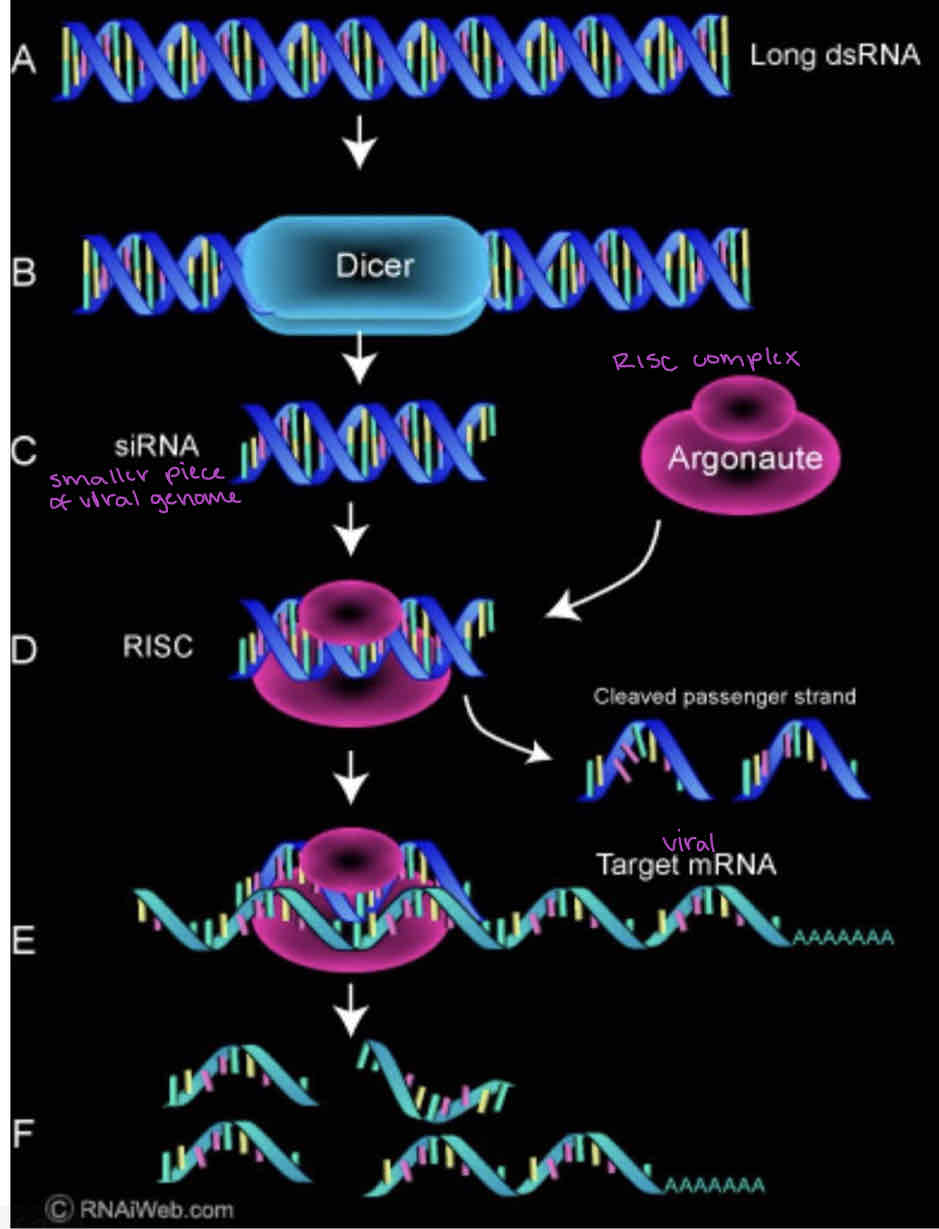
Explain how RNAi works to prevent viral infection
Dicer recognizes dsRNA and cuts it into small pieces (good trigger because dsRNA only comes from viruses)
One strand of the pieces is loaded into the RNA-induced silencing complex (RISC) (degrades and removes complementary piece)
Base pairing of the RNA strand to another RNA strand targets it for degradation by the Argonaute associated RNase activity
Explain how yellow fever spread to the Americas
Yellow fever is long endemic in central Africa, disease in native Africans is relatively mild. Due to the activities of slave traders yellow fever was imported to the Americas.
Explain how yellow fever impacted historical events such as the Louisiana Purchase and the Spanish American War
Louisiana purchase - Napoleon sends large force to crush uprising in Haiti. 27,000 French troops die of yellow fever. Due to massive losses in Haitian uprising, loss of capital from Haiti and increased need for resources, Napoleon sells Louisiana territory to US
Spanish American war - outbreak delayed military campaigns and exposed weaknesses in sanitation and medical preparedness. This experience led to improved disease control measures and spurred research into mosquito-borne illnesses, culminating in Dr. Walter Reed's discovery that mosquitoes transmitted yellow fever, which influenced later public health efforts.
explain how the mechanism of yellow fever transmission was discovered
Commission members self inoculated using mosquitoes that had bitten infected individuals.
No symptoms occurred
Used mosquitoes that had bitten an infected patient 12 days before.
Success! They became sick and died! Transmission from human to human by Aedes aegypti
identify the vector of flavivirus infection (Genus species)
Aedes aegypti
explain the factors that make a pathogen eradicable
1. Limited host range, preferably only humans or a defined vector
2. Mechanism of transmission intervention (vaccine)
3. Has been eliminated in a smaller geographic area
4. Significant public health burden
5. Makes financial sense to the countries involved
explain why yellow fever is not a good candidate for eradication
sylvatic cycle cycle involving mosquitoes, animal reservoirs (non-human primates), and widespread mosquito populations in diverse environments.
vaccine is effective but difficult to distribute in remote areas
virus's ability to persist in various settings adds to the challenge.
describe the vaccine design and efficacy for yellow fever
a live attenuated virus vaccine
highly effective, with over 90% efficacy in preventing yellow fever after a single dose. Protection begins within 10 days after vaccination and lasts for at least 10 years, often for life
explain the advantages and disadvantages of using DTT as a control method for yellow fever
Advantages: Effectiveness, Long-lasting, Low Cost
Disadvantages: Environmental Impact, Resistance, Health Concerns, Public and Regulatory Backlash
explain the advantages and disadvantages of using SIT and RIDL to control flaviviruses
Sterile Insect Technique (SIT) involves releasing sterilized male mosquitoes to mate with wild females, leading to no offspring and reducing mosquito populations over time.
Advantages:
1. targets mosquitoes without harming other species, making it environmentally friendly.
2. provides long-term mosquito population control without chemical use.
3.does not lead to resistance in mosquito populations.
Disadvantages:
1. can be expensive and logistically challenging.
2. most effective for certain mosquito species, limiting its use for controlling flaviviruses across all vector species.
3. requires large-scale releases to be effective, which may be difficult in areas with high mosquito densities or limited resources.
explain the state of yellow fever now and what factors allow the problem to persist
Urban yellow fever completely eliminated from Americas
The loss of vector control programs as a result of the ban on DDT use has led to a re-emergence of yellow fever, particularly in sub-Saharan Africa.
In addition to the loss of vector control in Africa there have been systemic failures to immunize at risk populations, mainly due to delivery of the vaccine. Political instability and warfare prevent vaccine delivery due to physical access and lack of funds
describe how Wolbachia infected Aedes is used to control flaviviruses
Wolbachia is a Gram negatvie bacterium.
Causes cytoplasmic incompatibility meaning embryos resulting from uninfected females mating with infected males die.
Infection causes decreased life span, and reduces virus replication hence reduces transmission of virus
Use Wolbachia as means to prevent Dengue transmission by introducing infected mosquitoes into natural populations.
identify the regions of the world most at risk for yellow fever infection
90% of cases occur in Africa, also some in South America
describe the factors contributing to the re-emergence of yellow fever in sub-Saharan Africa and South America
loss of vector control programs as a result of the ban on DDT
Yellow fever in South America has been a result of intrusion on the sylvatic cycle. No confirmed urban transmission, although some outbreaks suggest this is happening.
systemic failures to immunize at risk populations, mainly due to delivery of the vaccine. Political instability and warfare prevent vaccine delivery due to physical access and lack of funds
describe the hierarchical relationship between Flaviviridae family, Flavivirus genus, and species.
Flaviviridae (Family) > Flavivirus (Genus) > Dengue virus, Zika virus, West Nile virus, etc. (Species)
give examples of the major members of Flavivirus
Yellow fever, dengue, west Nile, encephalitis
compare and contrast the different host, diseases, and vectors associated with Flavivirus
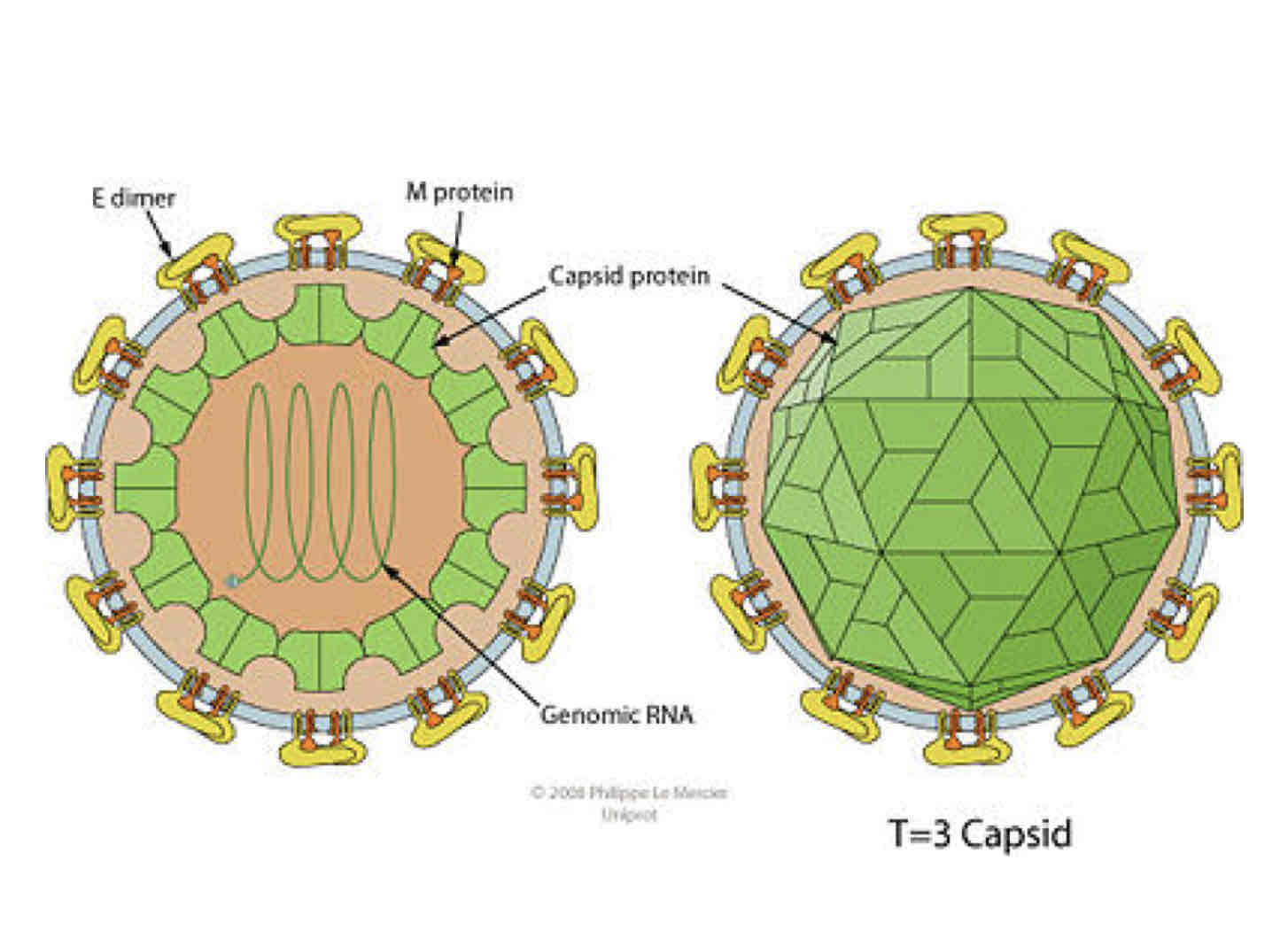
describe the structure of the Flavivirus virion
Enveloped and spherical, icosahedral geometry with T=3 symmetry
describe the viral and host proteins involved in flavivirus attachment
E protein binds to cellular receptor. No individual receptor identified, but can use integrins (connect cells together) and lectins that bind sugars.
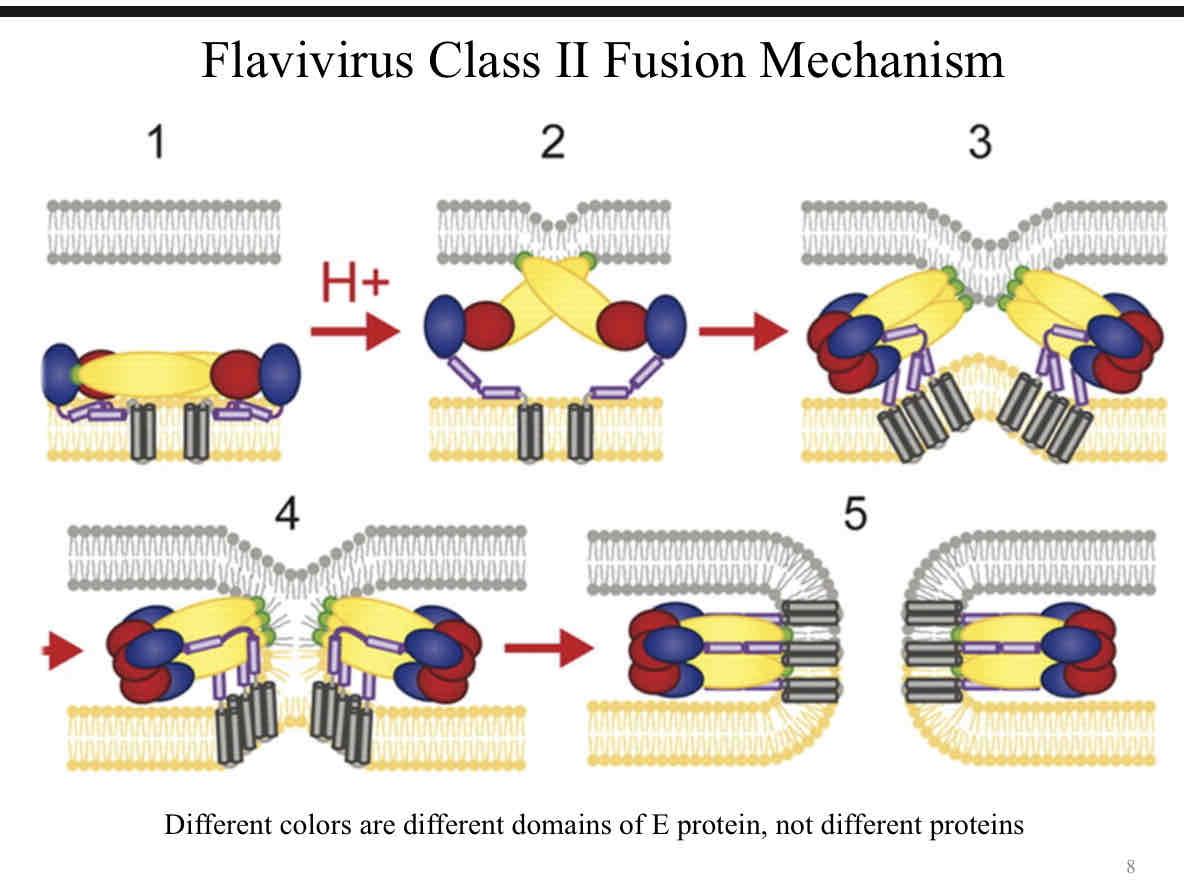
describe the class II fusion mechanism used for entry (flavivirus)
The E protein on the viral envelope binds to host cell receptors.
The virus is endocytosed into an acidic endosome.
The drop in pH triggers a conformational change in the E protein, exposing the fusion peptide.
The fusion peptide inserts into the host cell membrane, and the viral and host membranes fuse.
This fusion releases the viral genome into the host cell, where it can begin replication.
explain how the genome organization allows for immediate translation of a polypeptide
The genome has a 5' cap, which is recognized by the host’s ribosomes, allowing for translation of the viral RNA immediately after the virus enters the cell.
The genome contains a single ORF that is translated into a polyprotein which is processed by proteases into individual functional proteins.
explain the difference between the initial polypeptide and the mature viral proteins
Initial Polypeptide: a single, long chain that includes the structural (e.g., capsid, envelope) and non-structural proteins (e.g., polymerase, protease) in a precursor form.
Mature Viral Proteins: polyprotein is cleaved into individual, functional proteins that are necessary for viral assembly, replication, and release, such as the capsid protein, envelope protein, and NS (non-structural) proteins.
explain the problem between translation and replication that arises from being a positive sense genome. explain how flavivirus use the circularization motif to resolve this problem.
The problem: the same RNA is used both for translation (5 → 3) into proteins and for replication (3 →5) into new genomes. Since translation occurs as soon as the RNA enters the cell, it can compete with the need for replication
solution: using a circularization motif in their RNA. This involves the 5' and 3' untranslated regions interacting to form a circular structure. For replication, proteins bind to terminal and prevent translation
identify the viral protein responsible for replication
RNA-dependent RNA polymerase (NS5)
describe the steps and location of viral assembly and budding
1. The C (capsid) protein associates with the genomic RNA, forming the nucleocapsid. The prM (precursor membrane) and E (envelope) proteins are inserted into the ER membrane, where they undergo processing.
2. The nucleocapsid (C protein + viral RNA) interacts with the prM-E protein complex in the ER membrane, forming the immature virion.
3. The immature virion is transported from the ER to the Golgi apparatus in vesicles where the virus matures as the prM is cleaved to M by furin, and the virion acquires its final, infectious form.
5. The newly formed virions are transported to the cell surface in vesicles and are released from the cell via exocytosis.
explain the difference between viral glycoprotein modifications in the mosquito vector and the human host.
complex sugars added in vertebrates, high mannose in mosquitoes.
Humans: Modifications favor interaction with human receptors for infection.
Mosquitoes: Modifications support replication in the mosquito midgut and salivary glands.
describe the role of prM in viral infection and the importance of the cleavage of pr
The prM acts as a precursor to the M (membrane) protein. prM prevents premature fusion of the viral membrane with the host cell membrane during assembly, ensuring the virus remains in an immature, non-infectious form.
- Facilitates Viral Assembly: prM assists in the correct folding and assembly of the virus in the ER and Golgi.
importance of prM Cleavage (furin):
- Cleavage activates the virus, allowing the E protein to undergo structural changes necessary for the virus to become infectious.
describe the basic symptoms associated with yellow fever
1. Fever, chills, back pain, nausea, anorexia, mild gingival hemorrhaging, nose bleeds
2. Short remission (6-24 hours)
3. Symptoms recur with frequent vomiting (black), jaundice
4. Increased hemorrhaging
5. Death in 20-50% of cases 7-10 days following onset of symptoms
Recovery: Prolonged convalescence (months), with severe fatigue.
Explain steps involved in the initial flavivirus infection and how it spreads, paying close attention to the type of cells involved.
1. The mosquito injects the virus into the skin and, in some cases, directly into the bloodstream.
2. The virus infects Langerhans cells (immune cells in the skin.) It does this by binding to a receptor called DC-SIGN on these cells facilitated by high mannose glycans on the virus’s glycoproteins
3. The infected Langerhans cells travel to nearby lymph nodes, where they encounter macrophages. These macrophages are highly susceptible to infection by the virus.
4. From the lymph nodes, the virus enters the bloodstream, spreading throughout the body to infect various tissues where it can be picked up by other mosquitos and spread
Explain the steps involved in yellow fever pathogenesis, paying close attention to the type of cells involved and how it is resolved.
1. The virus infects Kupffer cells, which then spread the infection to nearby hepatocytes (liver cells).
2. The infected cells release cytokines, signaling for help from immune cells, including eosinophils.
3. Eosinophils, typically involved in responses to parasites or allergies, respond to the cytokine signals. Their activity can inadvertently damage liver tissue, leading to liver degradation.
4. This liver damage can cause jaundice (yellowing of the skin and eyes), a key symptom of severe yellow fever.
Describe the yellow fever vaccine design, paying close attention to the type of vaccine format used.
live attenuated virus vaccine
highly effective, with over 90% efficacy in preventing yellow fever after a single dose. Protection begins within 10 days after vaccination and lasts for at least 10 years, often for life
Explain the differences between classic dengue fever and dengue hemorrhagic fever and shock syndrome, both in terms of symptoms, lethality, and cause.
Classic Dengue Fever
self limiting infection
- Symptoms: fever, headache, nausea and vomiting, joint and muscle pain, weakness, prostration
- Lethality: Generally mild and rarely fatal
- Cause: Caused by infection with any one of the four dengue virus serotypes. A primary (first-time) infection usually leads to classic dengue fever.
Dengue Hemorrhagic Fever (DHF) and Dengue Shock Syndrome (DSS)
- Symptoms: Fever, increased hemo-concentration, low platelet count. Spontaneous hemorrhaging (nose bleeds, also gastrointestinal and intracerebral bleeding)
- Lethality: 1-10%
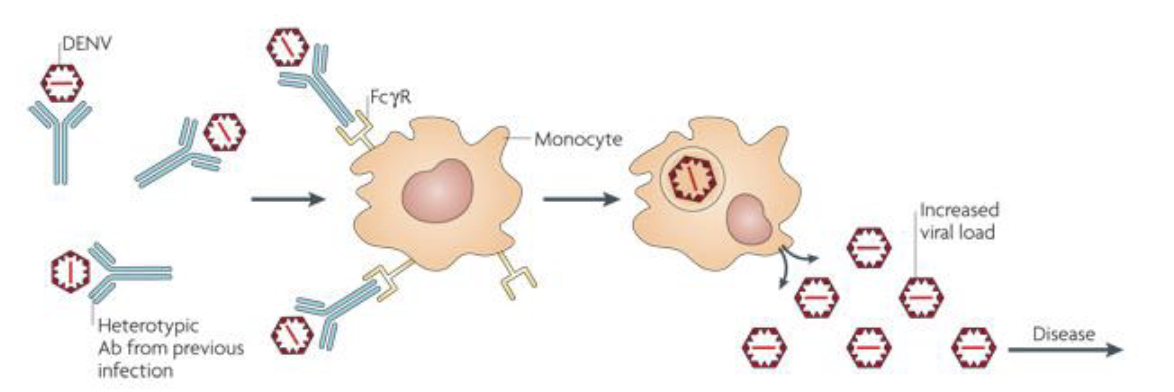
- Cause: Often occurs in people with secondary infections with a different serotype of dengue virus. This second infection can trigger antibody-dependent enhancement (ADE), where pre-existing antibodies from the first infection enhance viral entry into immune cells, leading to an exaggerated immune response, plasma leakage, and shock.
define the difference between neutralizing vs non-neutralizing antibody.
- Neutralizing Antibodies: directly prevent the virus from infecting cells by binding to viral surface proteins in a way that blocks the virus from attaching to or entering host cells.
- Non-Neutralizing Antibodies: bind to the virus but don’t prevent the virus from entering host cells. they may signal immune cells to destroy the virus or infected cells. In some cases, such as in antibody-dependent enhancement (ADE), non-neutralizing antibodies can inadvertently help the virus infect immune cells, potentially worsening the infection.
Explain the role of ADE in dengue virus infection and how it impacts pathogenesis and vaccine design.
Antibodies from a previous infection with one dengue serotype can partially bind to a different serotype, but they don’t fully neutralize it increases its ability to infect cells
These partially bound antibodies form DEN-Ab complexes allow it to attach to Fc receptors on macrophages (immune cells), helping the virus enter these cells.
Increased Infection: Once inside the macrophages, the virus replicates faster, increasing the viral load in the body.
Vascular permeability is increased due to inappropriate cytokine release
Explain why we have seen an emergence of DHF.
Human population growth increasing contact with vector
Urbanization with poor infrastructure favoring vector breeding
Air travel allows movement of viremic humans an dissemination of multiple serotypes
Hyperendemic areas with increased chance of serial infection
problems with vaccine development (4 serotypes)
Explain the different vaccine design strategies used for dengue virus, focusing on the different vaccine formats and the challenges for each.
1. Subunit vaccines using E glycoprotein from different serotypes. Do not stimulate robust response
2. Attenuated virus vaccine. Passage of Dengue viruses in non-human tissue culture cells causing attenuation in humans. Concerns about incomplete immune response and issues with production
3. Recombinant noninfectious subviral particles. Expression of just the surface glycoproteins in cells can lead to production of virus like particles that do not contain genetic material and are therefore noninfectious. Will produce antibodies but not a
complete immune response.
4. DNA vaccines. DNA only driving production of E protein. Licensed for use in animals against West Nile. Problems are number of doses needed for sero-conversion and for the need to express 4 different Dengue E proteins
5. Recombinant chimeric viruses. Introduction of major antigens from Dengue into an attenuated virus backbone such as the yellow fever vaccine virus. Dengvaxia only licensed vaccine (a lot of restrictions on use), have to carefully balance response to all
4 serotypes of Dengue
Describe the mechanism of transmission of malaria and how it was discovered
Caused by parasites of the genus Plasmodium.
Plasmodium spp. causing human malaria are thought to have been co-evolved with humans. Plasmodium falciparum is a more recent human pathogen being introduced between 10,000 and 50,000 years ago
Charles Laveran, a French physician first observed parasites in red blood cells of patients suffering from malaria in the late 19th century
Sir Ronald Ross demonstrated that mosquitoes were the vector using birds
Describe the clinical symptoms of malaria
headache, fever, shivering, arthralgia, vomiting, hemolytic anemia, jaundice, hemoglobinuria, retinal damage, and convulsions
Depending on the species of parasite the fever will be replaced by sudden coldness and rigor reverting back to fever and sweating
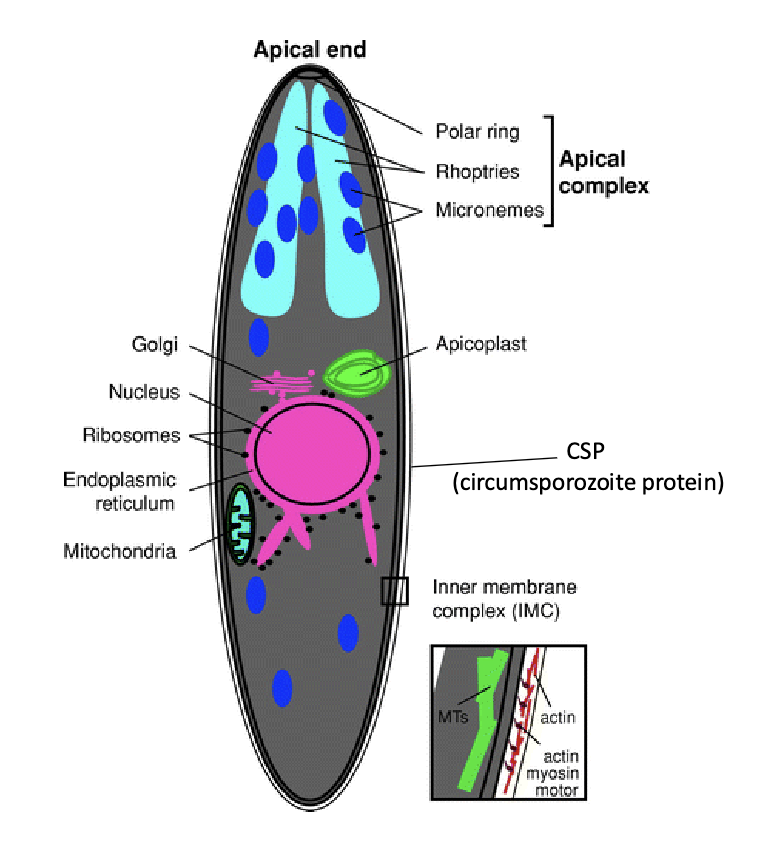
Define apicomplexian (and explain what it has to do with Plasmodium)
Obligate parasites evolved from free living photosynthetic ancestor
Apical Complex: This unique structure at one end of the cell which release enzymes and proteins essential for penetrating host cells.
Connection to Plasmodium
Plasmodium is a genus within the Apicomplexa phylum. Its apical complex is vital for the parasite’s ability to invade red blood cells and liver cells in the human host, as well as mosquito gut cells during transmission.
List the five major Plasmodium spp. associated with malaria in humans.
P. falciparum, P. vivax, P. ovale, P. malariae, P. knowlesi
Explain the origin of Plasmodium falciparum
Has been thought that P. falciparum diverged from P. reichenowi
as a consequence of human-chimpanzee speciation.
Now good evidence from mitochondrial DNA sequencing that it came from a cross-species transmission event from gorillas
List the three Anopheles spp. associated with the most transmission.
An. gambiae, An. stevensi, An. punctulatus
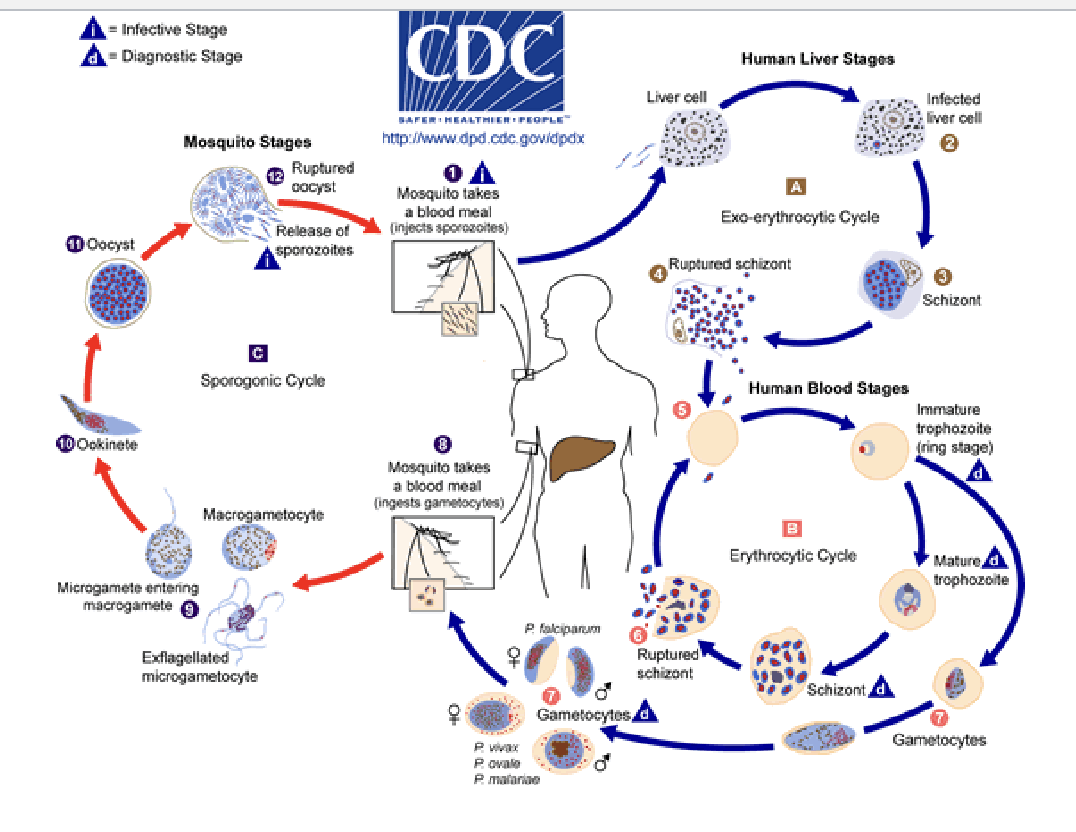
Explain the general Plasmodium life cycle and how it relates to transmission (next lecture will have much more detail).
Mosquito Stage (Sporogony):
When an infected Anopheles mosquito bites a human, it injects sporozoites into the bloodstream.
Human Liver Stage (Exoerythrocytic Cycle):
Sporozoites travel to the liver, infecting liver cells and developing into schizonts, which contain thousands of merozoites.
Schizonts eventually rupture, releasing merozoites into the bloodstream.
Human Blood Stage (Erythrocytic Cycle):
Merozoites infect red blood cells, where they multiply and develop through ring, trophozoite, and schizont stages, producing more merozoites.
Infected cells burst, releasing merozoites to infect new red blood cells, causing malaria symptoms.
Mosquito Transmission (Gametocyte Formation):
Some merozoites develop into gametocytes (sexual forms) that circulate in the bloodstream.
When another mosquito bites an infected person, it ingests gametocytes, which then mature in the mosquito, forming new sporozoites that migrate to the mosquito’s salivary glands, ready to infect a new host.
Explain the current economic and societal concerns facing malaria
linked with poverty; however, it is not symptomatic but causative
high death rates, lower life expectancy, reduction in work force, impairment of cognitive abilities in children
High impact on health expenditure
Estimated loss of $12 billion per year to African Nations (minimally)
Problems can be compounded by substandard or counterfeit drugs (1/3 of all)
Historically has been hard to get buy-in from non-malaria nations to assist with funding research, prevention and treatment
Describe the Plasmodium falciparum genome.
Genome: 14 chromosomes, 23 MB
Haploid except at zygote stage in mosquito
Low proportion of spliced mRNAs
60% of genes have no assigned function or ortholog
Low number of metabolic and amino acid synthesis genes
(host cell dependence)
High proportion of genes involved in immune evasion
Draw a flow chart of the developmental cycle of Plasmodium within both the human and mosquito host.
Describe the initial plasmodium infection within humans, paying to close attention to the developmental form and the importance of the apical complex in movement and invasion.
Developmental Form: Sporozoite
Sporozoite: This is the infective form of Plasmodium that enters humans. It is adapted to quickly reach and invade liver cells, where it will develop further.
Role of the Apical Complex
Structure and Function: Infection of the hepatocyte is a result of secretion of proteins from the apical complex into the cell that leads to the formation of a protective parasitophorous vacuole. allow sporozoites to penetrate host cell membranes.
Motility: The apical complex enables sporozoites to move through the bloodstream, reach the liver, and traverse several liver cells until they find one suitable for infection.
Define the sporozoite
A sporozoite is the infectious stage of Plasmodium that is transmitted from mosquitoes to humans. When an infected mosquito bites a person, it injects sporozoites into the bloodstream. These sporozoites travel to the liver, where they invade liver cells and multiply, eventually developing into merozoites.
CSP on sporozoites is key for malaria infection and immune evasion. Though CSP can stimulate immune memory over repeated exposures, the parasite’s ability to change CSP structure helps it evade the immune system
Describe the steps involved in P. falciparum infection of the liver, focusing on the progression of development.
1. When an infected mosquito bites a human, it releases sporozoites into the bloodstream.
2. Sporozoites travel through the bloodstream to the liver, where they use kupffer cells to infect hepatocytes
3. Sporozoites invade hepatocytes by forming the parasitophorous vacuole, which shelters them from the host immune system. Here, they replicate.
4. Inside hepatocytes, sporozoites transform into liver-stage schizonts. Over several days, each schizont produces thousands of new merozoites.
5. Once fully developed, the schizonts rupture, releasing merozoites into the bloodstream.
Describe the role of the parasitophorous vacuole and schizont in development.
After the sporozoite invades a liver cell, the PV forms around it, creating a protected environment for the parasite to grow undetected by the immune system.
Within the PV, the parasite matures into a schizont, undergoing rapid replication to produce thousands of merozoites. When the schizont ruptures, these merozoites are released into the bloodstream, starting the blood stage of malaria.
Define the merozoite.
A merozoite is one of the stages in the life cycle of the malaria parasite, Plasmodium. Merozoites are formed during the asexual reproduction phase of the parasite's life cycle, which occurs in the human host.
1. sporozoites enter the human bloodstream, travel to the liver and infect liver cells. Inside these cells, they undergo a phase of replication, producing a large number of merozoites.
2. the merozoites are released into the bloodstream, where they begin infecting red blood cells.
3. Within red blood cells, merozoites multiply, causing the cells to eventually burst.
4. These newly released merozoites go on to infect additional red blood cells, repeating the cycle. Some of the merozoites also develop into sexual forms (gametocytes) that can be taken up by a mosquito, continuing the cycle back in the mosquito host.
Describe the steps involved in P. falciparum infection of the red blood cell, focusing on the progression of development.
Merozoite Invasion: Free merozoites enter RBCs by attaching to and penetrating the cell membrane.
The merozoite interacts with the erythrocyte through the PfEBA proteins on its surface.
It binds at the apical end forming a junction with the cell through which proteins are secreted that cause invasion and formation of the parasitophorous vacuole
Trophozoite Stage: The merozoite develops into a trophozoite that secretes proteins into the host cell.
P. falciparum erythrocyte membrane protein 1 (PfEMP1) is made by the parasite and secreted into the cell where it becomes part of “knobs” on cell surface.
PfEMP1 binds to endothelial cells in blood vessels
Schizont Stage: The trophozoite divides to form a schizont, which producing multiple new merozoites.
RBC Rupture: The schizont eventually bursts, releasing the new merozoites into the bloodstream to infect additional RBCs.
Define the trophozoite.
A trophozoite is the active, growing stage of the Plasmodium parasite inside a red blood cell. After the parasite enters the red blood cell, it becomes a trophozoite, where it eats the cell's hemoglobin to grow and develop
Define the gametocyte.
A gametocyte is the sexual form of the Plasmodium parasite that circulates in the human bloodstream. When a mosquito bites an infected person, it ingests these gametocytes, which then mature into male and female gametes inside the mosquito. These gametes fuse to form a zygote, starting the sexual cycle of the parasite in the mosquito, ultimately leading to the formation of sporozoites that can be transmitted to humans.
Describe the role of PfEMP1 in infection and pathogenesis.
PfEMP1 is a protein on the surface of infected red blood cells (erythrocyte) that helps Plasmodium falciparum stick to the endothelial lining of the blood vessel. It enables antigenic variation, allowing the parasite to hide from immune detection, and adherence to blood vessel walls, leading to sequestration of infected RBCs in organs, which contributes to complications like cerebral malaria and organ damage.
describe the infection of a mosquito
Fertilization and Ookinete Formation:
After the mosquito takes a blood meal, the male and female gametocytes mature into gametes (male and female sex cells). These gametes fertilize each other, forming a zygote (ookenete)
The ookinete undergoes meiosis, producing haploid nuclei.
Migration and Oocyst Formation:
The ookinete moves through the mosquito's gut wall and lodges in the basal layer of the gut, where it forms an oocyst.
The oocyst is covered with proteins from the mosquito, protecting it from the mosquito's immune system.
Sporozoite Development:
Inside the oocyst, nuclear division happens rapidly, and centers form that eventually develop into thousands of sporozoites.
This process takes up to 14 days.
Sporozoite Release:
Sporozoites exit the oocyst, swim through the hemolymph and can attach to the
basal lamina of the salivary glands which they then breach achieving infection
Define the ookinete.
The ookinete is the motile, diploid zygote stage of the Plasmodium parasite that forms after the fertilization of male and female gametes within the mosquito’s gut. It is capable of moving through the mosquito’s midgut epithelium to reach the basal lamina, where it forms an oocyst.
Define the oocyst.
In the mosquito, Plasmodium gametocytes fuse to form a zygote, which develops into an oocyst on the midgut wall. Inside the oocyst, sporozoites replicate and mature. When the oocyst ruptures, sporozoites are released into the mosquito’s hemolymph and migrate to the salivary glands, ready to infect a new human host during a bite.
Explain the difficulties inherent in the Plasmodium life cycle that make it difficult for us to mount an immune response.
1. Antigenic Variation: Plasmodium constantly changes the proteins expressed on the surface of infected red blood cells (such as pFEMP1) and sporozoites, through processes like var gene switching.
2. Liver Stage Secrecy: The parasite spends a significant portion of its life cycle in the liver, where it is largely hidden from the immune system. sporozoites are shielded from immune surveillance, preventing an early immune response.
3. Red Blood Cell Stage: Once the parasite infects red blood cells, it is again protected from the immune system because red blood cells lack major histocompatibility complex (MHC) molecules, which are typically used to present antigens to immune cells.
4. Immune Suppression and Evasion: Plasmodium can manipulate the host's immune system, suppressing immune responses and inducing tolerance. Infected individuals may develop partial immunity over time, but it is often incomplete due to the parasite’s ability to evade immune recognition.
5. Complex Life Cycle: The parasite’s ability to transition between different host environments (mosquito and human) and cell types (liver, red blood cells) complicates immune recognition. The immune system must respond to multiple stages of the parasite's life cycle, each with different antigens.
Explain the immune response to the sporozoite
1. Innate Immunity:
- Natural Killer (NK) Cells can recognize and kill sporozoites before they enter liver cells.
- Macrophages and Dendritic Cells help capture and process sporozoites, activate adaptive immunity.
2. Adaptive Immunity:
- Antibodies against sporozoite surface proteins can neutralize sporozoites, preventing them from entering liver cells.
- CD8+ T cells target and kill liver cells infected by sporozoites, limiting parasite development
Explain the immune response to the merozoite
1. Innate Immunity:
- Phagocytosis: Macrophages and dendritic cells recognize and engulf merozoites, limiting their spread.
- Complement Activation: The complement system can bind to merozoites, marking them for destruction.
2. Adaptive Immunity:
- Antibodies: Antibodies, particularly those targeting merozoite surface proteins like AMA-1 and MSP-1, block the merozoites from invading red blood cells.
- T Cell Response: Cytotoxic T lymphocytes (CTLs) can help eliminate infected cells and contribute to immune memory.
Explain how nitric oxide is beneficial in fighting Plasmodium
1. It is toxic to Plasmodium parasites, particularly at the red blood cell stage, where it can interfere with their metabolism and survival.
2. NO is produced by immune cells (e.g., macrophages and dendritic cells) as part of the immune response to infection. It enhances the activation of other immune cells like T cells
3. NO also limits the growth and development of sporozoites within liver cells, helping prevent the spread of the parasite to the bloodstream.
4. Vascular Defense: NO helps modulate blood vessel dilation and immune cell recruitment, aiding in the inflammatory response and helping to control infection spread.
Explain the vaccine design of RTS,S
RTS,S is a recombinant protein-based vaccine
Vaccine Design:
- RTS,S is a chimeric protein that combines parts of CSP, which is found on the surface of the sporozoite, with a portion of the hepatitis B surface antigen (HBsAg).
- stimulates an immune response against the sporozoite stage of Plasmodium falciparum, helping the body recognize and attack the parasite before it can establish an infection in the liver.
Efficacy:
- RTS,S provides moderate protection against malaria, particularly in young children, reducing the incidence of malaria by around 30-50% in various studies.
- The vaccine also offers partial protection against severe malaria and hospitalizations. effectiveness can vary based on factors like age and transmission intensity in different regions.
What problems does the plasmodium life cycle present for antigen recognition?
1. Intracellular – very little time outside the host cell
- Sporozoite, minutes before finding liver cells
- Merozoite, minutes before re-entering RBCs
2. RBCs don’t express MHC
- contained within vesicle, proteins released but not presented
3. High reproductive rate so high variation in population
- high reproduction always increases variation
- sexual stage which increases variation/recombination
4. Deliberate variation in proteins
- specific mechanisms to cause variation in surface proteins, 60 variants of the PfEMP1 protein encoding gene, transcriptional switching
Explain the role of var gene in pfEMP1 expression and immune evasion and response
The var gene controls the expression of pFEMP1, with only one variant active at a time. This antigenic variation helps the parasite evade the immune system by constantly switching pFEMP1 variants, preventing effective immune responses.
Explain the role of pFEMP1 in pathogenesis
- Vascular Adhesion: pFEMP1 binds to receptors on endothelial cells, allowing infected RBCs to stick to blood vessel walls and evade the immune system
- Blockages and Inflammation: This adhesion can cause clusters that block blood flow, especially in critical organs like the brain (cerebral malaria) and placenta, leading to severe symptoms.
- Immune Evasion: P. falciparum changes pFEMP1 variants frequently, helping it evade immune detection and prolong infection.
Explain how Plasmodium induces short term effector cells and its effect on protective immunity
T-helper cells differentiate into short-lived “effector” cells and long-lived memory cells
Effector cells help the immediate response, but die through apoptosis following the response
Memory cells remain partially activated in lymph tissue awaiting reinfection
The differentiation is dependent on cytokine activation
Plasmodium encodes a cytokine ortholog that favors short-lived effector cells
Therefore while sterilizing immunity may occur the lack of memory T-helper cells prevents effective establishment of protective immunity
Explain the challenges associated with RTS,S
Series of 4 injections in children under 5
Modest efficacy – prevents ~30% of severe cases of malaria after 4 injections
Cost – Sold just above cost of production, but 100 million annual dosages needed to cover children in all high burden countries
underfunded anti malaria programs
Identify major regions that are endemic with malaria
Africa, south america, south asia
Explain how vector distribution effects transmission
areas with vectors that affect humans are where malaria is endemic
Define vectorial capacity
daily rate at which future inoculations arise from a currently infective case
Identify vector with highest vectorial capacity
An. gambiae has by far the highest vectorial capacity i.e. is most “infectious”
Explain EIR, the factors that define it and how it relates to transmissibility
This is a measure of transmission intensity in a given area. Has a relationship to vectorial capacity
What factors will it depend on?
1. Density of mosquito population
2. Proportion of female mosquitoes with infected salivary glands
3. Number of infected mosquitoes feeding on a person in a unit of time
Relates to:
1) The number of contacts between infected individual
and uninfected.
2) Proportion of contacts that are susceptible?
3) Probability of transmission per susceptible contact?
Describe the vector control current efforts to reduce EIR
Indoor residual spraying (IRS) – highly effective
Organophosphates, Carbamates, Pyrethroids, Organochlorines (DDT)
Insecticide treated nets – An. gambiae is a night-time feeder
Sleeping under nets significantly reduces malaria risk (~50%)
All chemicals have some degree of negative health effect.
However this has to be balanced against the consequences of high malaria transmission.
Explain the mechanisms of insecticide resistance
1. Target site changes – pyrethroids target sodium channels on insect neurons
Binding of the insecticide keeps the channel open and
results in continuous neuron firing resulting in
paralysis and death
Single amino acid changes in the channel prevent
insecticide function
2. Metabolic resistance – increase in activity of detoxifying enzymes
Cytochrome P450s (111 of these enzymes in An gambiae)
Changes in the expression levels of one or more of these
capable of metabolizing the insecticide allows resistance
Explain in general the difference between therapeutic, prophylaxis, and intermittent preventative approaches to treatment
Therapeutic – treatment of confirmed infections
Prophylaxis – prevention of infection for travelers from non-endemic regions to endemic regions
Intermittent preventative – for certain groups in endemic regions, frequently infants and pregnant women
Explain the mechanism of action (if known) behind the current major anti malaria drugs (chloroquine, doxycycline and artemisinin) and the mechanisms of resistance
Chloroquine – acts against blood schizonts and gametocytes
Doxycycline – disrupts parasite translation in erythrocyte stage
not recommended to use on own due to delayed response
Artemisinin – mechanism unknown, but effective against all forms of multi drug resistant P. falciparum
define symptoms of dengue fever
Dengue Fever Symptoms:
Mild to Severe:
1. Headache, fever, eye pain, upper back pain, sometimes rash
2. Followed by muscle, joint and bone pain, anorexia, vomiting, weakness and prostration
3. May be hemorrhaging (mild and infrequent)
4. Not lethal, but debilitating
Dengue hemorrhagic fever or dengue shock syndrome; includes severe bleeding, organ damage, and potentially fatal shock.