Lecture 8 B: Head and Neck: non-monoisocentric/non-half beam
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
True or False: In a non-monoisocentric setup. The jaws are typically NOT asymmetrical jaws.
True
A non-monoisocentric AP SC field will have some way of blocking the superior edge of the field that you would normally just close down with an asymmetrical jaw.
What would we use to create a half-beam for the AP SC?
A cerrobend block
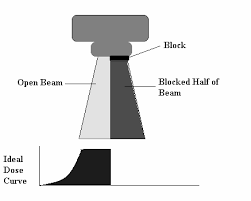
True or False: Because we don’t have asymmetrical jaws, you will ballpark the AP SC with an open field
True
how does a non-monoisocentric setup look?

Steps for Setting up a Non-Monoisocentric Setup.

Steps: Consult Dr
Steps: Meet, Greet, Eval
Steps: Position
Get Patient on table: Swing legs, center on table, lay them back.
Assure patient is straight using sagittal laser: line between feet, legs, center of pelvis, xiphoid process, SSN, chin, nose, glabella.
Create tongue blades, bite blocks, or mouth devices
Create Mask
How do you create the mask?
Apply shoulder retractors
Assure that chin is extended (up) and straight
Assure that laser follows along the same lines
Apply mask. Two therapists may be required to properly make long mask.

Step: Ballpark AP SC
Set CR sup/inf: at thyroid notch
Set field length: just inferior to SSN
Set field width: to include the lateral aspect of both clavicles
Set ant/post: just Posterior to the angle of the mandible OR Set 100 SSD at your AP SC CR
Step: Fluoro AP SC
Step: Call Dr
Step: Notate
What do you notate?
Everything INCLUDING table vertical
Step: Mark AP SC CR
Mark AP SC CR
Mark inferior border
Put wire along superior border

Why do we put a wire along the superior border?
It will determine the couch angle for the laterals

After doing all the marks on AP SC, what step is next?
set supraclav dose point
Where is the Supraclav dose point?
3 cm superior & 3 cm lateral to SSN
What steps do we take after setting dose point?
step: Verify SSD is at 100
Step: Film AP SC
Step: Have film approved by Dr
Step: Mark rest of relevant field borders
Step: Rotate to lateral
Step: Ballpark lateral
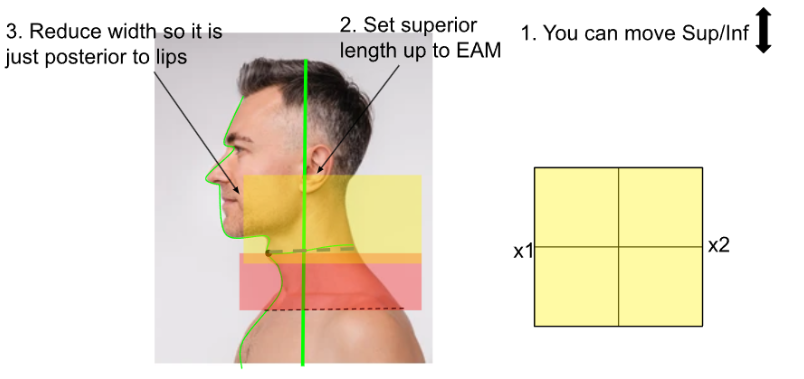
Set length: by moving patient sup/inf & changing f.s.
Superior border: at EAM
Inferior border: flashing across wire
Note: CR won’t be in the same place since you are moving the patient in/out
Reduce width: posterior to lips
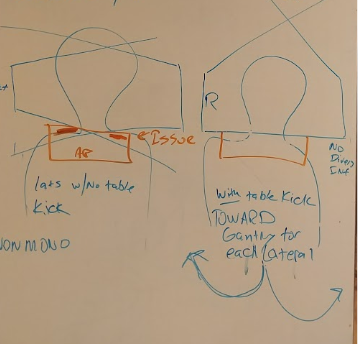
Rotate table

You rotate the table, feet (away from/towards) the gantry until:
Towards
until inferior border matches wire with no divergence- double check this on flouro
Steps: Fluoro lateral
Steps: Call Dr
Adjust field length (long):
changing f.s length with symmetrical jaws & moving in/out
Adjust depth if needed (vert)
What must you do if you adjust the field length?
Compensate by moving the table sup/ inf as well.
FYI:
Remember: your jaws are not asymmetrical. If what you are ballparking doesn’t match radiographically, you’ll have to change your field size. Both Y1 and Y2 will shrink down or open up. So you will have to move the table in/out to make sure your superior border is at the EAM and inferior border is flashing across the wire.
Steps: Notate
What do you notate?
Everything Including table vert & Table Angle
Note: you will have 2 table verticals. 1 for the APSC and another for the lats
Steps after notating:
Step: Mark Lateral CRs
Step: Set Cervical Dose Point
Where is the Cervical Dose point located?
½ way between sup and inf border
1-2 cm ant to post border.
Steps after setting up Cervical Dose point.
Step: Read Lateral CR SSD
Note: It will be in the middle of the patient’s head instead of the neck
Step: Film
Step: Have film approved by DR
Step: Mark rest of relevant field marks on patient
Step: Rotate to opposing lateral
What must you do when you rotate towards the opposing lateral?
Mirror table angle/kick
Repeat steps: ballpark → mark rest of relevant field borders on patient
Skip Cervical Dose Point step
True or False: If you already filmed your AP SC, you are pretty much done
TrueW
What step is next?
Check SSDs @ each dose point
Take separation at each dose point (no mask)
Remaining steps:
Step: photos
Step: Educate
What is the tiny box with crosshatching on the bottom right?
A safety block
Where does the doctor draw the safety block? Why?
On either lateral or AP SC
To protect the spinal cord from divergence/ hot spot
Even with a safety block in place, you might still have a:
Junction Shift
FYI: aka feathering
What is the purpose of the junction shift?
Move the junction/matchline every couple of weeks to reduce hot spots
What moves in a Junction shift? What remains the same?
Match line will be moved to a different location
The overall sup/inf aspect of the treatment volume remains the same
i.e. the inferior SC border and superior lateral border remain the same. Those borders cannot move
Junction shift steps
Lateral field will have a decrease in field size by 1 cm
AP SC field will have an increase in field size by 1 cm
CR & match line for each field will be moved by 0.5 cm in the same direction
This will equal to an overall match line shift of 1 cm, maintaining the original Sup/Inf border

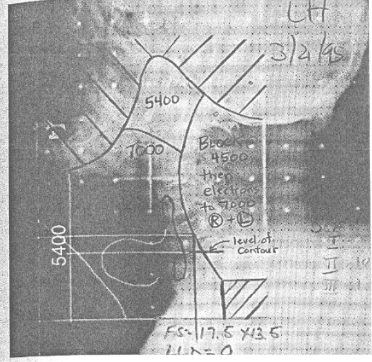
An Electron Boost is needed for:
Posterior Cervical Nodes

Add a cord block after ____cGy
4500
True or False: After you add a cord block, you still need to treat the cervical nodes to a higher dose.
TrueW
How do you treat the cervical nodes after adding the cord block at 4500cGy?
With an electron field
What size and shape is the electron field?
Same size and shape as the cord block
What are the field borders for the block & electron boost?
Anterior: Abuts to the new posterior photon field
Posterior: Where it used to be
Superior: Where it used to be
Inferior: Abuts to the SC matchline

Simulation for the cord block and electron boost is done on
A. Simulator
B. Treatment Machine
C. Neither, Drawn on radiographs
B. treatment machine
When you are simulating on the tx machine:
Draw the cord block.
These constraints are simulated for an electron field.
What other things might you need to do?
May need to tx at an extended SSD (in order to have shoulder-tray clearance)
May need to pour the block as far posterior & inferior as possible in the template to allow for more clearance