Water and Salt
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
69 Terms
Normal serum sodium range
135-145 mmol/L
Hyponatraemia
Low serum sodium
What is the most common electrolyte abnormality?
Hyponatraemia (20-30% od hospital admissions)
What can cause hyponatraemia?
Sodium loss
Water gain
Why are women made up of less water than men (55% compared to 60%)?
Women have more adipose tissue.
What are the separate fluid compartments in the body called?
Intracellular (30 L)
Interstitial (9 L)
Vascular (3 L)
What does movement of water in the body respond to?
Tonicity (a measure of the effective osmotic pressure gradient)
In which compartments is sodium found?
Extracellular and vascular compartments
Euvolaemic / Normovolaemic
A normal volume of blood
Hypovolaemic
Blood volume is depleted
Hypervolaemic
Blood volume is too high.
What are the different types of hyponatraemia?
Normovolaemic hyponatraemia
Hypovolaemic hyponatraemia
Hypervolaemic hyponatraemia
What happens to sodium levels if we lose water?
Sodium becomes concentrated - hypernatraemia.
What happens to sodium levels if we gain water?
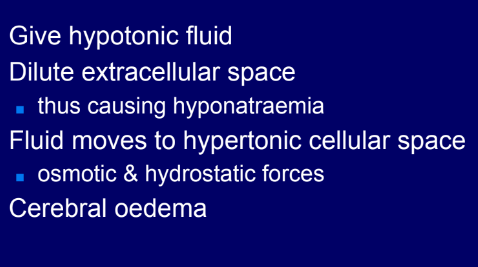
Sodium becomes diluted - hyponatraemia.
What happens to water in the body when we lose salt?
Water is also lost - hypovolaemia.
What happens to water in the body when we gain salt?
Water is gained - hypervolaemia
What diseases can cause fluid loss?
Haemorrhage
Vomiting
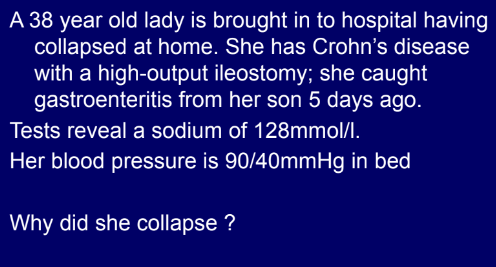
Diarrhoea
Burns
Diuretic states
Sequestration
What are the iatrogenic causes of fluid loss?
Diuretics
Stomas / fistulas
Gastric aspiration
Surgical drains
What diseases can cause fluid gain (salty)?
Heart failure
Liver failure
Renal failure
What diseases can cause fluid gain (more water than salt)?
Hypothyroidism
Psychogenic
ADH excess
What are the iatrogenic causes of fluid gain?
IV fluids (saltiness variable)
Supplemental nutrition (usually salty)
What can cause pure water loss hypernatraemia?
Fever (sweating too much)
Hyperventilation
Diabetes insipidus
Why might some patients have a reduced water intake?
Iatrogenic
Psychosocial - elderly, infants, apathetic etc.
Stroke, coma, confusion etc.
What causes pure Na+ gain hypernatraemia?
This is rare.
Iatrogenic:
Concentrated feeds
Emetics
Hypersecretion of ADH can cause what?
SIADH
Hyponatraemia
Failure of ADH causes what?
Diabetes insipidus
Hypernatraemia
How does excessive ADH secretion cause hyponatraemia?
No suppressed by reduced tonicity
Free water reabsorption is excessive
Sodium is diluted and hyponatraemia results
Does a person with SIADH have a normal blood volume?
Yes.
What causes diabetes insipidus?
ADH is either not produced in sufficient amounts, or non-functional.
What might cause non/reduced synthesis of ADH?
Pituitary tumour
Head injury
Meningitis
Genetic
Idiopathic
When investigating a patient on a renal ward, what should you inspect in the environment?
Charts
Drug kardex
Drains and drips
Psychiatric disease?
Chest disease?
Neurological disease?
Volume state: hyper/normo/hypovolaemic
What recent events should ask a renal patient when taking a history?
Surgery
Trauma
Diagnoses
Diarrhoea
Chest diseases
Drugs
Drips
What questions should you ask a renal patient when taking a past medical history?
Polyuria
Polydipsia
Hypovolaemiae
What non-specific investigations should be considered for a renal patient?
Other electrolytes
FBC
Infection screen
Chest X-ray
Serum cortisol
CT brain
How should a patient be given water?
Orally - cannot give a patient water through a drip unless it is in a 5% dextrose solution (typical concentration).
What are the symptoms of dehydration / volume depletion?
Thirst
Dizziness
Dysphagia
Weakness
Confusion / aggression
Coma
What are the clinical signs of volume depletion / dehydration?
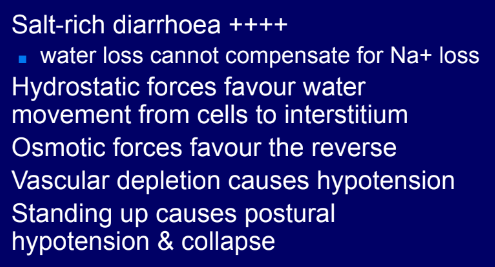
Postural hypotension
Tachycardia
Absence of JVP at 45 degrees
Reduced skin turgor / dry mucosae
Supine hypotension
Oliguria
Organ failure
Why do burns victims lose more water?
The skin cannot prevent water evaporating.
What happens to the volume of the blood when there is pure water gain?
It remains normal / there is mild hypervolaemia.
What happens to the volume of the blood when there is Na+ and water gain?
Interstitial oedema / hypervolaemia.
What happens to the volume of the blood when there is Na+ and water loss?
Hypovolaemia
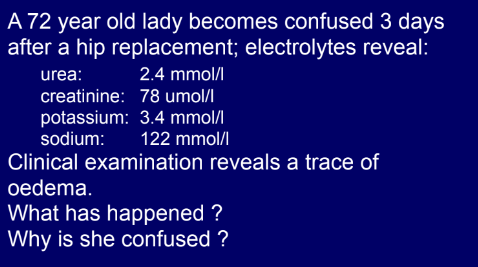
Hypovolaemic hyponatraemia
Any case in which salt and water loss occur, but water loss is insufficient to concentrate the sodium.
Why does heart failure lead to hypervolaemic hyponatraemia?
Reduced effective circulating volume
Reduced organ perfusion
Physiological correcting mechanisms kick in:
RAAS - sodium retention
ADH - water retention
Hyponatraemia results from dilution
Fluid overload worsens LV function, creating a worsening cycle
When there is abnormalities in [Na+], what is usually the cause: water or Na+ movement?
Water
What are some other names for SIADH?
AVP and SIAD
SIADH aetiology
Excessive secretion of ADH, which can be caused by:
Pituitary hypersecretion
Meningitis
Encephalitis
Head injury
Stroke
Ectopic secretion
Malignancy (eg. bladder, prostate…)
Pulmonary (eg. TB)
Drugs (many)
SIADH causes…
Excessive water resorption and therefore normovolaemic hyponatraemia.
Diabetes insipidus causes…
Excessive renal water loss, and therefore hypovolaemic hypernatraemia.
What causes diabetes insipidus?
A condition caused by failure of the ADH mechanism:
Cranial / central causes - non / reduced synthesis
Pituitary tumour
Head injury
Meningitis
Genetic
Idiopathic
Nephrogenic causes - reduced tubular response
Inherited
Drugs (eg. lithium)
Metabolic (hyperkalaemia, hypercalcaemia)
What are the clinical signs of volume excess / overhydration?
Hypertension
Tachycardia
Raised JVP at 45 degrees
Gallop rhythm
Oedema
Organ failure
Is SIADH common?
No
Is diabetes insipidus common?
No.
Central pontine myelinolysis
Damage to the myelin sheath covering the pons - related to rapid correction of Na+.
What is the recommended rate of Na+ correction?
4-10 mmol/L/day if asymptomatic
8-12 mmol/L/day if symptomatic
What specific investigations are there for water and salt balance?
Plasma osmolality
Urine osmolality
Urine (and other) sodium concentration
What is a normal plasma osmolality?
280-300
What plasma osmolality indicates diabetes insipidus?
>300
What plasma osmolality indicates SIADH?
<280
What urine osmolality indicates diabetes insipidus?
<300
What urine osmolality indicates SIADH?
>300
When a patient has hyponatraemia, how is this managed?
Usually with restriction of water intake.
When a patient has hypernatraemia, how is this managed?
Giving the patient water (typically orally).
Aside from restricting / giving water, how else are conditions affecting water and salt balance managed?
Treat the primary cause
Stop / change any drugs that are causing it (remember to look at drips and feeds too)
Allow time
What are some specific treatments for cranial / central diabetes insipidus?
Synthetic ADH - desmopressin.
What are some specific treatments for nephrogenic diabetes insipidus?
Supraphysiological ADH
Diuretics (paradoxically)
NSAIDs