Aortic Regurgitation (AR) and Aortic Insufficiency (AI)
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
68 Terms
What is AR?
The backflow of blood though the aortic valve in diastole. This may be due to abnormalities of the aorta or to abnormalities of the valve leaflets themselves.
What are the hemodynamics in early findings of AR?
Increased LV volume by regurgitant leak, increased SV (Starlings law)
LVVO
Hyperdynamic LV
What are the hemodynamics in late findings of AR?
LV decompenstates, thus decreasing the LV function (because LV gets tired of compensating for the extra volume of blood and begins to “fail”)
Left ventricular hypertrophy (LVH) and LV failure).
What is acute AR?
When AR happens suddenly.
What is chronic AR?
When AR happens slowly.
What are the causes of acute AR? (3)
Infective endocarditis
Aortic dissection
Blunt chest trauma
What is aortic dissection?
When the intima of the heart layers is torn away. This is usually long standing hypertension.
What are the causes of chronic AR? (6)
Rheumatic Fever
Congenital BAV (bicuspid aortic valve)
Calcific valve disease
Systemic inflammatory diseases
Aortic dilatation (causes leaftlets to pull further apart thus causing leaking)
Incomplete closure of AoV
What are the clinical findings of AR?
Minor symptoms for many years, then abruptly symptomatic in the 4th decade of life
Exertional or paroxysmal (spasms) dyspmea (SOB)
Chest pain (angina) - due to coronary insufficency
Dizziness (due to cerebral insufficiency)
Syncope (fainting due to decreased cardiac output)
What is the auscultation like when there is AR?
High-pitched, blowing decrecendo with diastole murmur on the LSB.
What are the two auscultation changes present with AR?
Austin Flint Murmur
Bisferiens pulse
What is Austin Flint Murmur?
Where there is mid-diastole rumble that is low pitched at the apex. This indicates severe AR.
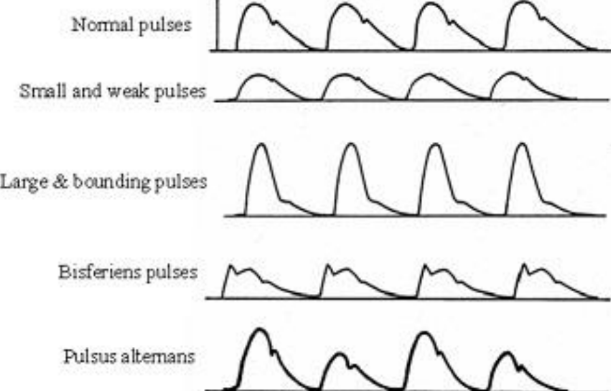
What is Bisferiens pulse?
Where there is a widely notched, double peaked, arterial pulse due to the rapid falling of the aortic pressure.
When there is Austin Flint Murmur, there is usually what?
Bisferiens pulse.
When there is Bisferiens pulse, there is often what?
Austin Flint Murmur.
Describe a pressure recording of the AoV with regurgitation in the catheterization lab?
A decrease in aortic end diastolic pressure and an increase in LVED pressure as the AR leaves the Ao and enters the LV during diastole. Severe acute AR will present with equalization of the diastolic pressures.
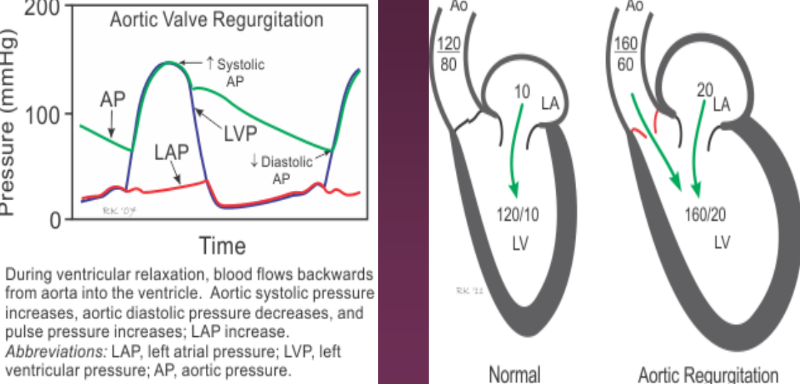
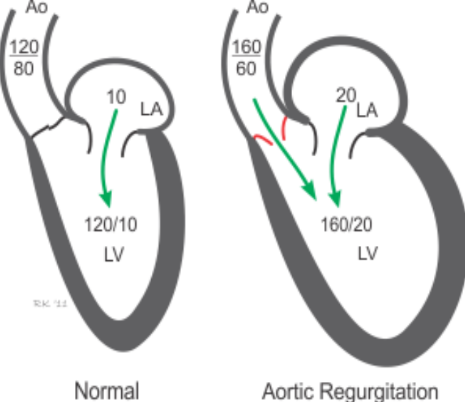
What happens with AR in terms of the LV?
LV fills from 2 sources in diastole, the Ao (normal) and the LA (abnormal). This causes LVED volume to increase which causes increased contraction (hyperdynamic), thus increasing LVVO. It also causes LVED pressure to increase.
AR causes an increase in stroke volume in the Ao, therefore increasing what pressure?
The systolic pressure of Ao (> 120 mmHg)
What happens to the diastolic pressure of Ao with AR?
It decreases due to the diastolic leak back into the LV (< 80 mmHg)
An increase in LVED pressure due to AR, causes what?
Blood to back up inot the LA and pulmonary veins,w which leads to an increase in the LA pressure, and possibly leading to pulmonary congestion (due to the pressure increase).
What are the treatments for AR?
Serial echocardiograms are performed to track changes in function, chamber size, and the degree of AR (to see if its getting worse)
Depending on the severity, an Ao V replacement or repair may be required. This is usually done before the LV gets compromised (tired for compensating for the extra load and failing after years of “extra” work)
What are the 2-D findings in an echo when there is AR?
Flail or prolapsing leaflets
AS
Incomplete closure of the Ao V
Dilated ascending AO
Bicuspid Ao V
Rheumatic heart disease
Diastolic fluttering of the AMVL/IVS (quivers) - due to the AR jet hitting one or the other.
Reverse doming of the AMVL in diastole (due to jet; associated with moderate to severe AR)
LVVO
LV failure
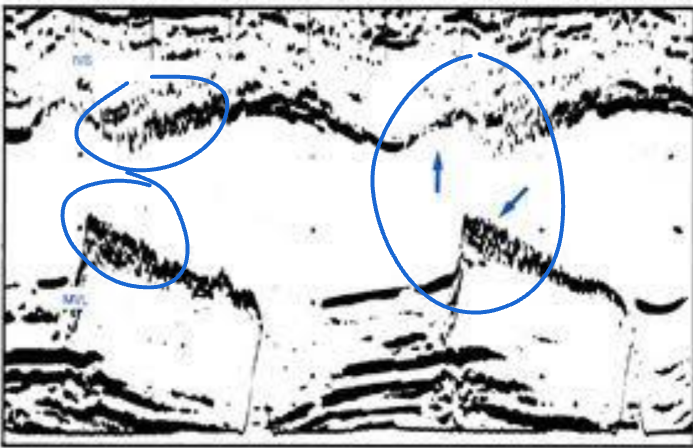
What are the M-Mode findings in an echo when there is AR?
Diastolic flutter AMVL/IVS (quivers) (if the AR jet hits them)
Premature closing of the MV (C pioint occurs before QRS complex)
Premature Ao V opening (beofre QRS) from an increase in LVED pressure due to severe AR
Diastolic flutter of Ao V.
Is systolic flutter of the Ao V valves normal?
Yes. But DIASTOLIC flutter is ABNORMAL! (Questioning AR)
What is the method of choice for dectecting AR?
Doppler (Colour, CW)
When is Doppler of the Ao Valve is done to look for AR, what view(s) is this done in?
Parasternal LAX (even though perpendicular)
Parasternal SAX (even though perpendicular)
Apical 5 and 3 views are best for CW Doppler
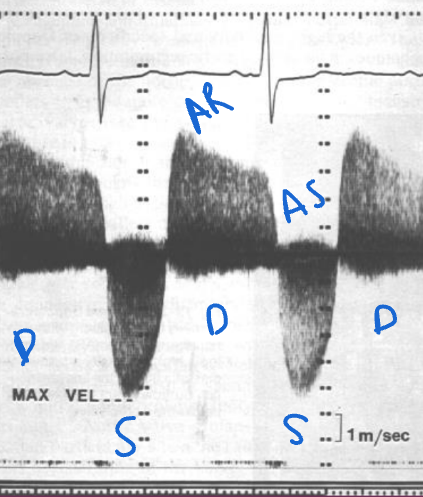
What does A Doppler of AR look like?
Leaking in diastole. There is also stenosis here! Shown in systole with a velocity higher than 1 m/s. (@ 5 m/s)
Pulsed wave Doppler of an AR is done in what views?
A5 and A3
Where is the sample volume placed when PW Doppler-ing for AR?
In the LVOT.
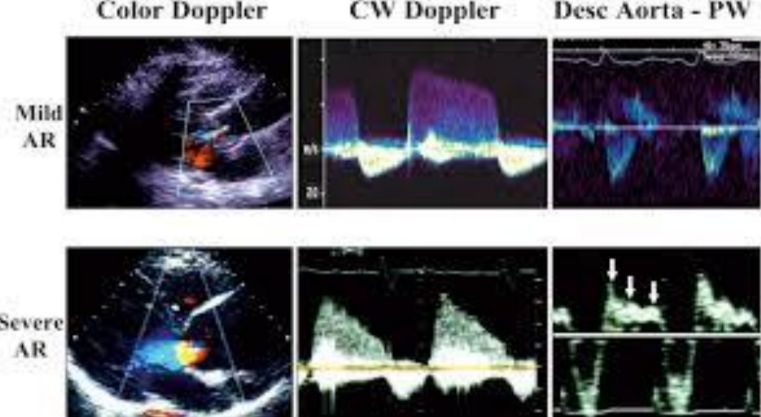
What is looked at when CW Doppler is placed on the Ao Valve in A5 or A3 for AR?
The severity of it.
Mild would see a jet beneath the AOV
Moderate would see a jet at the tips of the MVL
Moderate/Severe would see a jet to the papillary muscles
Severe would see a jet beyond the papillary muscles.
(This colour mapping technique has been replaced by colour Doppler but is still good to learn).
Colour flow Doppler is the easiest method to see any valve’s….
regurgitant jet (if present).
Regurgitant flow through the AOV will appear in what phase?
Diastole (when the AOV is supposed to be closed).
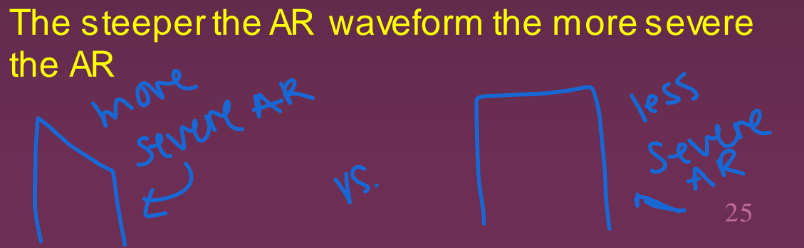
A more severe AR will have more of a slope on Doppler or more of a box shape in diastole?
Slope.
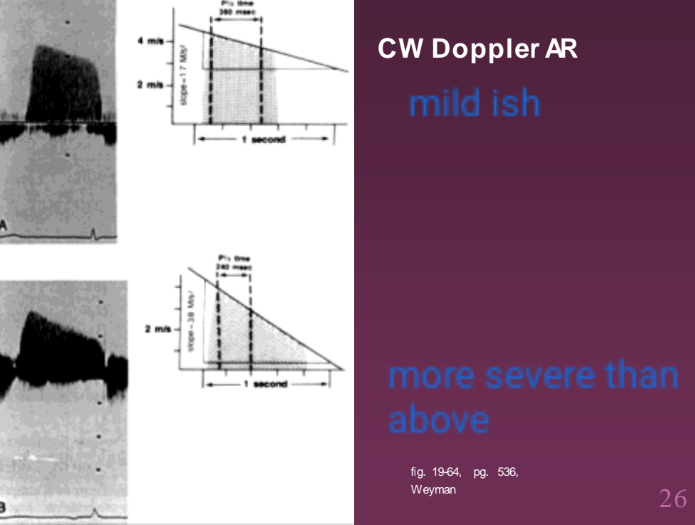
AR has a similar Doppler waveform measurement method utilized for MS. What is this?
Pressure Half Time.
The steeper the AR waveform, the more ______ the AR. (seen in diastole)
severe
What does a CW Doppler look like of AR in diastole?
A milder AR will create a more _______ AR waveform with CW Doppler.
Flatter. (This is because the pressure difference gradually decreases as the AR slowly moves back through the closed AOV into the LV in diastole)
Severe AR waveform in diastole using CW Doppler has more of a steeper slope. Why?
Since it is severe, this means there is more of an opening when the AOV is closed for AR. This allows more blood to rush back into the LV during diastole. This causes the aortic pressure to drop faster, thus increasing the LV pressure faster.
When coducting pressure half-time on AR, what view is this accomplished in?
A5 or A3.
How do you do a pressure half-time measurement for AR?
Select the AOV pressure Half-Time measurement package. Then measure the deceleration slope of the AR. Once measured, the machine will automatically calculate the Pressure Half-Time.
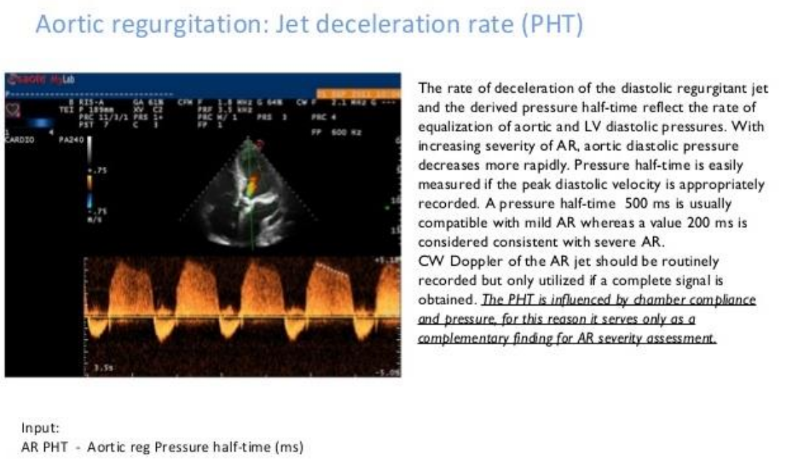
List the Pressure Half-Time severity scale for AR. (3)
Mild @ > 500m/s
Moderate @ 350-500 m/s
Severe @ < 200 m/s
What are four other methods used to estimate the severity of AR? (Besides pressure half-time)
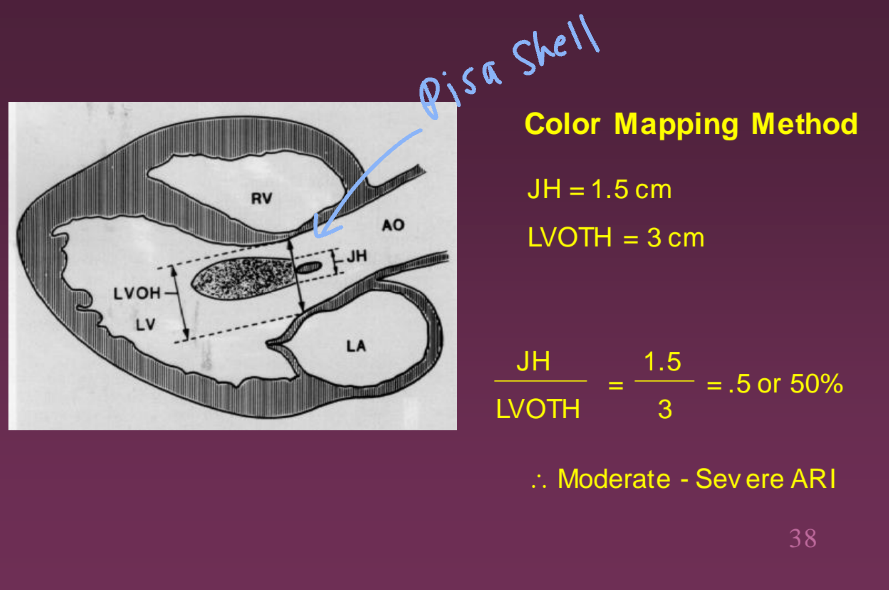
AR jet/LVOT area
AR jet height/LVOT height
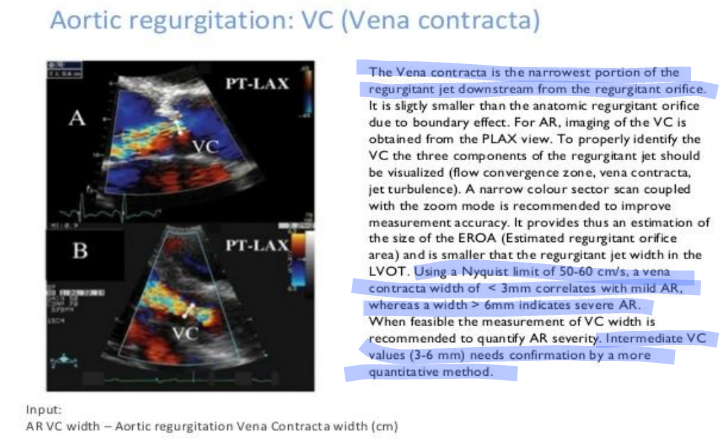
AR Vena Contracta
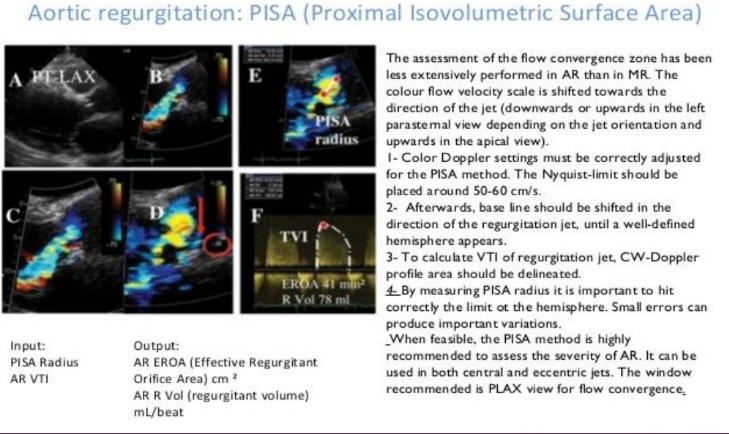
AR PISA
When using jet height/LVOT height, what are the different grades used to identify the severity of AR?
Mild @ < 25%
Moderate @ 25-46%
Moderate-Severe @ 47-64%
Severe @ 65%
(Tends to be more “eyeballed" than actually calculated)
Example of how AR jet height and LVOT height is used to grade severity of AR.
Jet area/LVOT area for AR is graded how? Also, what view is this done in?
Mild @ <4%
Moderate @ 4-24%
Moderate-Severe @ 25-59%
Severe @ > 60%
Done in the parasternal SAX view by using planimetry with the machines calculation package.
Below is a picture of how Vena Contracta would be used in needed for AR.
Below is a picture of how PISA would be used if needed for AR.
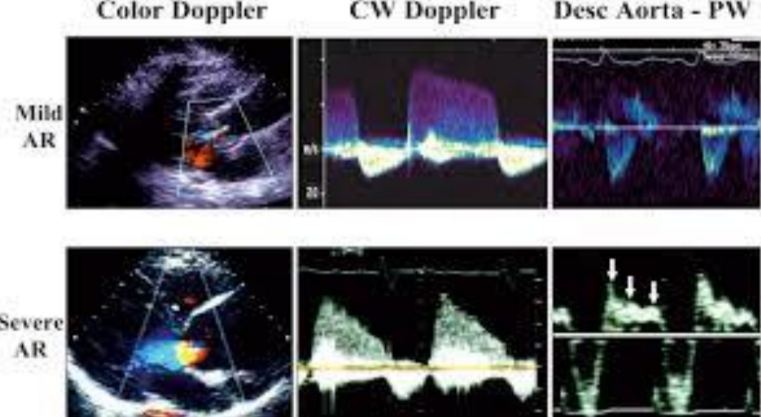
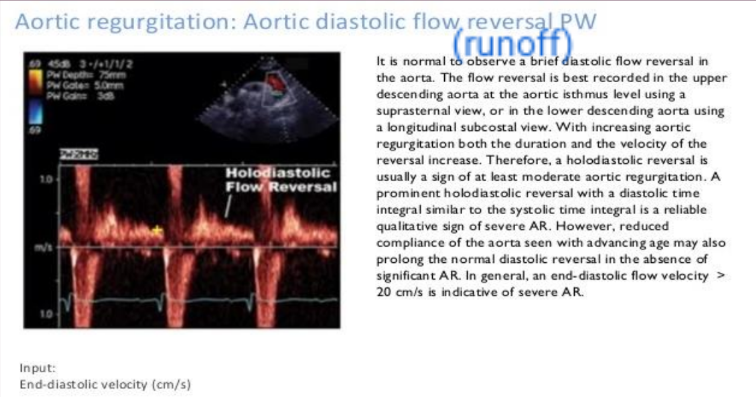
The suprasternal notch view can be used to do what with AR?
Determining its severity by assessing the descending AO and the Abdominal AO to see how far back the leaking is coming from. Absences of reversed blood flow means it is probably less severe AR. Presence of reversed blood flow means that it is more severe.
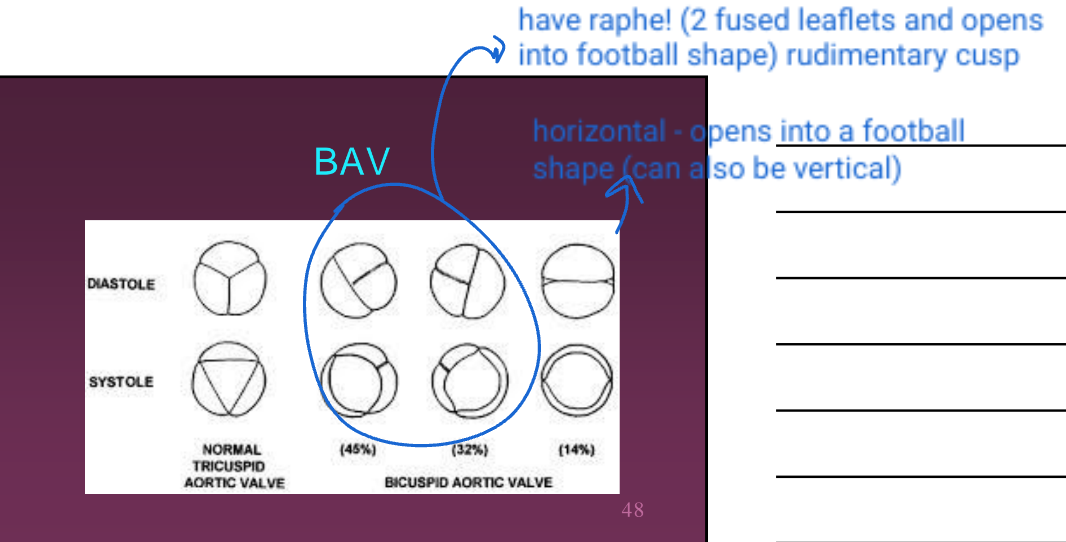
What is a bicuspid AO V?
When there are only two leaflets of the aortic valve (there should be three).

Is a bicuspid valve congenital?
Yes.
What are the issues with a bicuspid valve?
It can cause AR and AS in the 3rd or 4th decade of life.
What is the most common congenital abnormality in an adult?
Bicuspid Aortic Valve.
When someone has a bicuspid aortic valve, how might it appear?
Raphe or a fold may appear in one of the leaflets.
What is a raphe bicuspid aortic valve?
A rudimentary cusp (under developed hence why two are fused together). It gives the impression of three leaflets when closed, but when open, instead of the Ao V opening to a triangle, it opens to a football shape.
Bicuspid aortic valves occur in what percentage of the population?
2%
Is it possible for a Ao V to be quadricuspid (4 leaflets) or unicuspid?
Yes, but it is MUCH more rare than a bicuspid aortic valve.
Does a bicuspid aortic valve need to be fixed at birth or can it stay until it becomes a problem?
Until it becomes a problem.
Examples of bicuspid aortic valve.
When someone has bicuspid aortic valve, are there symptoms?
Usually not in children and young adults. There will be some systolic murmur. Later in life, the valve tends to thicken and calcify thus leading to problems.
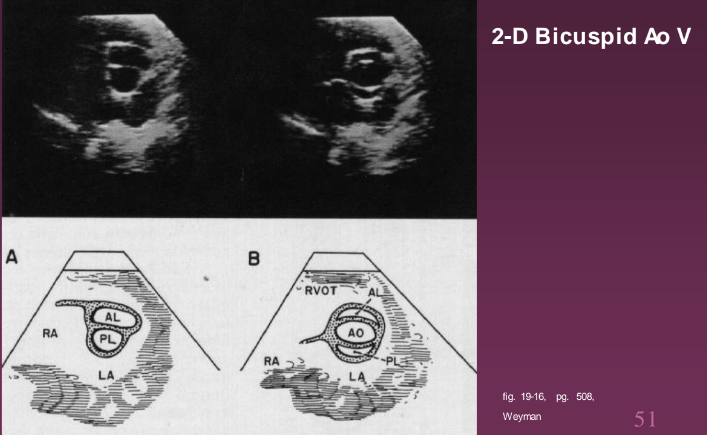
What are the 2-D findings when there is a bicuspid aortic valve?
Best view is in the parasternal SAX, with careful TX position. Cineloop the SAX to view how the aortic valve opens. Systolic doming in LAX and eccentric closure in LAX.
What are the M-Mode findings when there is bicuspid aortic valve?
May see eccentric closure line (not in the middle of aorta) in diastole.
What is aortic valve prolapse (AVP)?
The downward displacement of one or more aortic valve leaflets below a line joining the points of attachment of the aortic valve leaflets.
What view is best evaluated for aortic valve prolapse?
Parasternal LAX.
How do the leaflets appear with AVP?
Appear thick and redundant.
AVP when used with Doppler, what can be expected along with AVP?
AR.
AVP is often associated with what?
Bicuspid aortic valve
Aortic root dilatation
Infective endocarditis
Severe MR
If there is prolapse in one valve, it is important to check the other valves for what?
Prolapse.
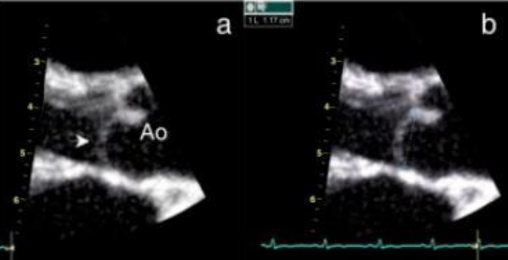
What’s going on in this picture?
AVP of the non coronary leaflet. It is possibly also showing a bicuspid valve because the closure of the AO V is not in the middle of the aortic root.