2.CW inhibit
1/126
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
127 Terms
What class of antibiotic is vancomycin?
Vancomycin is a:
Glycopeptide antibiotic
Cell wall inhibitor
Mainly active against:
→ Gram-positive bacteria
Mnemonic:
“VAN protects against Gram POSITIVE vans.”
What is the mechanism of action of vancomycin?
Vancomycin:
Binds to D-Ala-D-Ala
Blocks peptidoglycan elongation(stop polymerisation)
Prevents bacterial cell wall synthesis
Result:
→ Weak cell wall
→ Bacterial death
Mnemonic:
“VAN parks on D-Ala-D-Ala.”
What organisms does vancomycin cover?
Strong activity against:
MRSA
MRSE
Enterococci
Other Gram-positive bacteria
NO significant activity against:
Gram-negative bacteria
What does MRSA stand for?
Methicillin-Resistant Staphylococcus aureus
Vancomycin is a major treatment for MRSA.
What are the major clinical uses of vancomycin?
First-line treatment for:
Complicated skin infections
Bloodstream infections
Endocarditis
Bone & joint infections
MRSA meningitis
When is oral vancomycin used?
Used for:
Severe Clostridium difficile colitis
Relapse cases
Infection unresponsive to metronidazole
Important:
Oral vancomycin stays in GI tract
Poor systemic absorption
Mnemonic:
“PO VAN stays in the bowel.”
How is vancomycin administered?
IV Vancomycin:
Serious systemic infections
Slow infusion over 1–2 hours
Oral Vancomycin:
C. difficile colitis only
Why must vancomycin be infused slowly?
Rapid infusion can cause:
→ Red Man Syndrome
Symptoms:
Flushing
Red rash
Hypotension
Itching
Cause:
Histamine release
Prevention:
Infuse slowly (1–2 h)
Mnemonic:
“Fast VAN = RED MAN”
What are the important adverse effects of vancomycin?
Major adverse effects:
Red man syndrome
Nephrotoxicity
Ototoxicity
Thrombophlebitis
Risk increases when combined with:
Aminoglycosides
How is vancomycin eliminated?
Excreted unchanged by:
Kidneys (glomerular filtration)
Clinical implication:
→ Dose adjustment needed in renal impairment
What is the resistance mechanism against vancomycin?
Bacteria change:
D-Ala-D-Ala → D-Ala-D-Lac
This decreases vancomycin binding.
Example:
VRE (Vancomycin-resistant Enterococci)
What combination therapy involving vancomycin is important?
Vancomycin + gentamicin:
Alternative treatment for enterococcal endocarditis in severe penicillin allergy
Vancomycin + ceftriaxone/cefotaxime:
Resistant pneumococcal meningitis
Why is vancomycin use restricted(limited)?
To reduce emergence of:
VRE (Vancomycin-resistant Enterococci)
Used mainly for:
Serious resistant Gram-positive infections
High-yield vancomycin exam pearl?
Vancomycin:
Covers Gram-positive bacteria including MRSA
Binds D-Ala-D-Ala
Causes Red Man Syndrome if infused rapidly
Oral form treats C. difficile
Nephrotoxicity + ototoxicity are key toxicities
VAN parks on D-Ala-D-Ala, kills MRSA, turns patients RED if infused too FAST.”
What class of antibiotic is daptomycin?
Daptomycin is a:
Lipopeptide antibiotic
Cell membrane disruptor
Important:
→ NOT a cell wall inhibitor
What is the mechanism of action of daptomycin?
Daptomycin:
Inserts into bacterial cell membrane
Uses calcium-dependent binding
Causes membrane depolarization
Leakage of potassium ions occurs
Result:
→ Inhibits DNA, RNA & protein synthesis
→ Rapid bacterial death
Mnemonic:
“DAP = DePolarizes”
Is daptomycin bactericidal or bacteriostatic?
Daptomycin is:
Rapidly bactericidal
Concentration-dependent killer
What organisms does daptomycin cover?
Strong activity against resistant Gram-positive bacteria:
MRSA
VRE (Vancomycin-resistant Enterococci)
What are the major clinical uses of daptomycin?
Used for:
Complicated skin infections
MRSA bacteremia
Right-sided infective endocarditis(a rare but life-threatening inflammation of the heart’s inner lining and valves, usually caused by bacterial or fungal infections)
Why should daptomycin NEVER be used for pneumonia?
Because:
Pulmonary surfactant inactivates daptomycin
Result:
→ Ineffective in lungs
(Note: Linezolid has good lung penetration)
Mnemonic:
“DAP gets trapped by lung surfactant.”
What important adverse effects are associated with daptomycin?
Major toxicities:
Myalgia(muscle pain)
Muscle weakness
Rhabdomyolysis
Elevated creatine kinase (CK)
What monitoring is important during daptomycin therapy?
Monitor:
Creatine kinase (CK) levels
Especially in:
Patients on statins
Muscle symptoms
What makes daptomycin unique compared with β-lactams and vancomycin?
Daptomycin:
Targets cell membrane
NOT cell wall
Mechanism:
→ Membrane depolarization
While β-lactams/vancomycin:
→ Inhibit cell wall synthesis
What is the high-yield exam point about daptomycin?
What is the high-yield exam point about daptomycin?
Back:
Key exam pearl:
Covers MRSA & VRE
Causes muscle toxicity
Check CK
NEVER use for pneumonia
Mnemonic:
“DAP DePolarizes muscles & can’t enter lungs.”
One-line summary of daptomycin?
Daptomycin is a lipopeptide antibiotic that kills resistant Gram-positive bacteria by depolarizing the bacterial membrane, but it cannot treat pneumonia because lung surfactant inactivates it.
What are the main polymyxin antibiotics?
Main polymyxins:
Polymyxin B
Colistin (Polymyxin E)
What class of antibiotics are polymyxins?
Polymyxins are:
Polypeptide antibiotics
Cell membrane disruptors
Important:
→ NOT cell wall inhibitors
What is the mechanism of action of polymyxins?
Polymyxins:
Bind to phospholipids of Gram-negative bacteria
Disrupt bacterial cell membrane integrity
Result:
→ Leakage of cell contents
→ Cell death
Mnemonic:
“POLYmyxin punches HOLES in membrane.”
Are polymyxins bactericidal or bacteriostatic?
Polymyxins are:
Concentration-dependent
Bactericidal
What bacteria are covered by polymyxins?
Strong activity against Gram-negative bacteria:
Pseudomonas aeruginosa
E. coli
Klebsiella pneumoniae
Acinetobacter species
Enterobacter species
Do polymyxins work against Gram-positive bacteria?
No
Polymyxins mainly target:
Gram-negative bacteria
Because they bind:
→ Lipopolysaccharide (LPS)
What are the major adverse effects of polymyxins?
Major toxicities:
Nephrotoxicity
Neurotoxicity
Examples of neurotoxicity:
Slurred speech
Muscle weakness
Paresthesia
Mnemonic:
“POLY = kidney + nerve toxicity.”
Why is therapeutic drug monitoring (TDM) important for polymyxins?
Because polymyxins have:
Narrow therapeutic index
Significant nephrotoxicity/neurotoxicity risk
TDM helps:
→ Reduce toxicity
When are polymyxins usually used clinically?
Used mainly for:
Severe multidrug-resistant Gram-negative infections
Especially when other antibiotics fail.
What is the membrane effect of polymyxins similar to?
Polymyxins act like:
Detergents
They disrupt membrane integrity causing leakage.
What is the high-yield exam pearl for polymyxins?
Polymyxins:
Target Gram-negative bacteria
Bind LPS
Destroy cell membrane
Cause nephrotoxicity & neurotoxicity
Mnemonic:
“POLY punches holes → kidneys & nerves suffer.”
What class of antibiotic is fosfomycin?
Fosfomycin is:
A bactericidal antibiotic
A cell wall synthesis inhibito
What is the mechanism of action of fosfomycin?
Fosfomycin:
Inhibits UDP-N-ag transferase (MurA)
This blocks:
→ The FIRST step of peptidoglycan synthesis
Result:
→ Inhibition of bacterial cell wall formation
Mnemonic:
“FOSFO = FIRST step OFF”
Is fosfomycin bactericidal or bacteriostatic?
Fosfomycin is:
Bactericidal
Kills bacteria by blocking cell wall synthesis early.
What infections is fosfomycin mainly used to treat?
Mainly used for:
Urinary tract infections (UTIs)
Especially caused by:
E. coli
Enterococcus faecalis
Why is fosfomycin effective for UTIs?
Because fosfomycin:
Is rapidly absorbed orally
Concentrates well in urine
Maintains high urinary levels for several days
What are the pharmacokinetic properties of fosfomycin?
Fosfomycin:
Rapid oral absorption
Well distributed to:
Kidneys
Bladder
Prostate
Excreted active in urine & feces
Often given as:
→ One-time dose for uncomplicated UTI
Does fosfomycin have cross-reactivity with β-lactams?
Unlikely
Because fosfomycin has:
Unique chemical structure
Useful in some β-lactam allergic patients.
What are the adverse effects of fosfomycin?
Common side effects:
Diarrhoea
Nausea
Headache
Vaginitis
What is the high-yield exam pearl for fosfomycin?
Fosfomycin:
Blocks the FIRST step of cell wall synthesis
Used mainly for UTIs
Given as single oral dose
Concentrates in urine
Mnemonic:
“FOSFO stops the FIRST wall brick.”
What type of antibiotic is cycloserine?
Cycloserine is:
A cell wall synthesis inhibitor
An anti-tuberculosis (anti-TB) drug
Mainly used for:
Drug-resistant tuberculosis
What is the mechanism of action of cycloserine?
Cycloserine:
Inhibits alanine racemase
Inhibits D-Ala-D-Ala formation
Result:
→ Prevents peptidoglycan synthesis
→ Weak bacterial cell wall
Mnemonic:
“CYCLO stops the D-Ala cycle.”
What bacteria is cycloserine mainly used against?
Used mainly for:
Multidrug-resistant (MDR) tuberculosis
Extensively drug-resistant (XDR) tuberculosis
Especially when:
→ First-line TB drugs fail
What are the pharmacokinetic properties of cycloserine?
Cycloserine:
Water soluble
Unstable at acidic pH
Widely distributed into tissues
Mainly excreted unchanged in urine
What is the most important toxicity of cycloserine?
Major toxicity:
→ CNS toxicity
Examples:
Headache
Tremors
Acute psychosis
Convulsions (seizures)
Mnemonic:
“CYCLO = CNS goes in circles.”
Why should cycloserine be used cautiously in epilepsy patients?
Because cycloserine can:
Cause seizures
Produce serious CNS toxicity
High risk in:
Epileptic patients
Psychiatric illness
What part of the cell wall pathway does cycloserine affect?
What part of the cell wall pathway does cycloserine affect?
Is cycloserine bactericidal or bacteriostatic?
Cycloserine is generally:
Bacteriostatic against TB
But may be bactericidal at high concentrations.
What is the high-yield exam pearl for cycloserine?
Cycloserine:
Treats MDR/XDR TB
Blocks D-Ala formation
Causes major CNS toxicity
Mnemonic:
“CYCLO affects the brain while stopping D-Ala chain.”
What type of antibiotic is bacitracin?
Bacitracin is:
A polypeptide antibiotic
A cell wall synthesis inhibitor
What is the mechanism of action of bacitracin?
Interferes with the dephosphorylation of C55- isoprenyl pyrophosphate
Result:
→ Inhibits bacterial cell wall synthesis
What bacteria does bacitracin mainly cover?
Mainly active against:
Gram-positive bacteria
What is unique about bacitracin resistance?
Bacitracin has:
No cross-resistance with other antimicrobial drugs
Why is bacitracin NOT used systemically?
Because bacitracin is:
→ Highly nephrotoxic
Can cause severe kidney damage if given systemically.
Mnemonic:
“BACI breaks kidneys.”
How is bacitracin usually used clinically?
Used TOPICALLY for:
Skin infections
Wounds
Surface lesions
Mucous membranes
Why is topical bacitracin useful?
Because it suppresses:
Mixed bacterial flora
on skin and wounds.
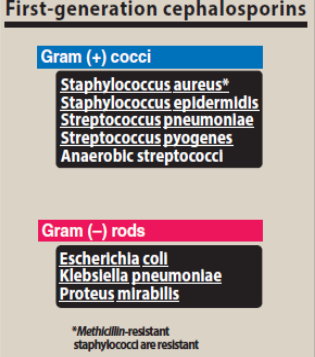
Cephalosporins
1st-generation
cefazolin, Cephalexin
penicillin Gsubstitutes.
• Resistant to the staphylococcal penicillinase (including MSSA)
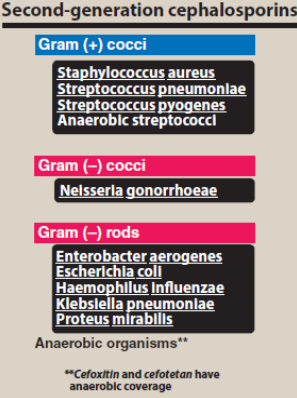
Cephalosporins
2nd-generation
(Cefuroxime, cefotetan, cefoxitin)
Cefotetan and cefoxitin are the only cephalosporins against gram-negative anaerobic bacteria
Cephalosporins
3rd-generation
Cefotaxime, ceftriaxone, ceftazidime
Cephalosporins
4th-generation
Cefepime
Must be administered parenterally.
Effective against aerobic gram-negative organisms, such as Enterobacter species, E. coli, K. pneumoniae, P. mirabilis, P. aeruginos
Cephalosporins
Advanced generation
Ceftaroline
Administered IV as a prodrug
Against MRSA and treat complicated skin and skin structure infections and community-acquired pneumonia
coverage include P. aeruginosa, extendedspectrum β-lactamase (ESBL)-producing Enterobacteriaceae, and Acinetobacter baumannii.
Therapeutic advantage if each cephalosporins
Ceftriaxone(3rd)
longest half life
effective against Neisserisa gonorrhoeae
excreted via bile maybe be used for renal insufficiency
why resistance to penicillin =resistant to cephalosporins
cephalosporins susceptible to extended-spectrum β-lactamases (ESBLs) by E. coli and K. pneumoniae
Cephalosporins has a good or poor oral absorption?
poor (need IV or IM)
Distribution of cephalosporins
Distribute very well
Ceftriaxone, cefotaxime (3 rd gen)] are effective to treat neonatal and childhood meningitis caused by H. influenzae.
Cefazolin (1 st gen)- single prophylaxis dose prior to surgery including orthopedic surgery
Cephalosporins
Elimination
Tubular secretion(doses adjustment is needed for renal impaired patients)
Only ceftriaxone (3 rd gen)is excreted through the bile (can be employed in patients with renal insufficiency)
Cephalosporins
Adverse effects
anaphylaxis, fever, skin rashes, nephritis, granulocytopenia, and hemolytic anemia
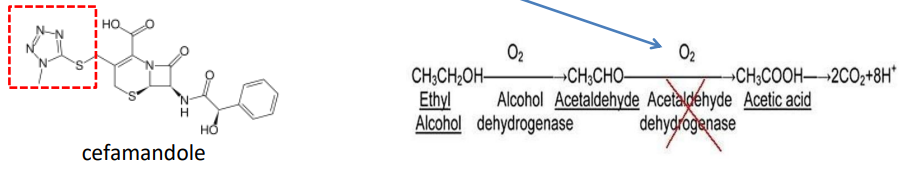
Cephalosporins that contain a methylthiotetrazole group (cefamandole, cefmetazole, cefotetan, cefoperazone) cause hypoprothrombinemia (inhibits vitamin K epoxide reductase) and inhibition of aldehyde dehydrogenase like disulfiram .
5th generation cephalosporin-Ceftobiprole
IV injection(prodrug)
Indication: Community and hospital acquired pneumonia
Excreted via the kidney
Common side effects: Nausea, vomiting, dysgeusia(impairment of your sense of taste.)
5th generation cephalosporin-Ceftobiprole
Coverage:
Gram +ve: Staphylococci (MRSA), Vancomycin RA
Gram –ve: Similar to ceftriaxone and ceftazidime (not active against ESBL and carbapenemases strains)
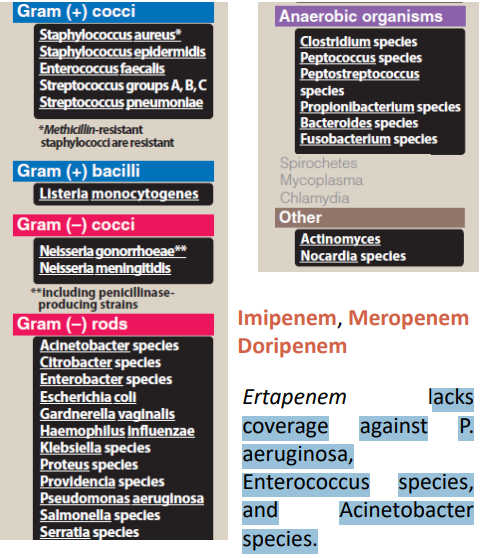
Carbapenems(Imipenem, Meropenem, Doripenem, Ertapenem)
Can treat ESBL-producing bacteria (E.g.: E. coli and K. pneumoniae).
Lacks coverage against P. aeruginosa, Enterococcus species, and Acinetobacter species.
Imipenem resists hydrolysis by most β lactamases
but not the metallo-βlactamases
Why is cilastatin only combined with imipenem?
Cilastatin prevent imipenem from broken down by Inhibiting dehydropeptidase
Which carbapenem penetrates CSF well and is useful in meningitis?
Meropenem
but Imipenem/cilastatin can also penetrate well into body tissues and fluids Including CSF
How are carbapenems eliminated?
Mainly by:
Glomerular filtration (renal excretion)
Clinical significance:
Dose adjustment needed in renal impairment
What are the common adverse effects of carbapenems?
Common:
Nausea
Vomiting
Diarrhoea
Less common:
Eosinophilia-abnormally high count of eosinophils (a type of white blood cell) in the blood
Neutropenia-a condition characterized by a lower-than-normal level of neutrophils,
Which carbapenem is most associated with seizures?
Imipenem
Especially:
High doses
Renal impairment
Meropenem has lower seizure risk.
What is the main monobactam antibiotic?
Aztreonam
Route:
IV
IM
What is unique about the β-lactam ring in monobactams?
The β-lactam ring is:
NOT fused to another ring
This distinguishes monobactams from:
Penicillins
Cephalosporins
Carbapenems
What bacteria does aztreonam mainly cover?
Strong activity against:
Gram-negative bacteria
Especially:
Enterobacteriaceae
Pseudomonas aeruginosa
What organisms are NOT covered by aztreonam?
Aztreonam lacks activity against:
Gram-positive bacteria
Anaerobes
Mnemonic:
“Aztreonam = NEGATIVE only”
How does aztreonam work?
Mechanism of action:
Binds to PBPs
Inhibits bacterial cell wall synthesis
Prevents peptidoglycan cross-linking
Result:
→ Bacterial death (bactericidal)
Is aztreonam resistant to β-lactamases?
Yes
Aztreonam is resistant to:
Most β-lactamases
BUT:
Can be destroyed by ESBLs
(Extended-spectrum β-lactamases)
What important pharmacokinetic property does aztreonam have?
Aztreonam can accumulate in:
Renal failure patients
Therefore:
Dose adjustment is needed in renal impairment
What are the adverse effects of aztreonam?
Generally nontoxic
Possible side effects:
Phlebitis
Skin rash
Abnormal liver function tests
Why is aztreonam useful in β-lactam allergic patients?
Because it has:
Little cross-reactivity with other β-lactams
Can be used in patients allergic to:
Penicillins
Cephalosporins
Carbapenems
High-yield summary of aztreonam?
Aztreonam is a monobactam active mainly against gram-negative bacteria including Pseudomonas, resistant to many β-lactamases, and useful in β-lactam-allergic patients.
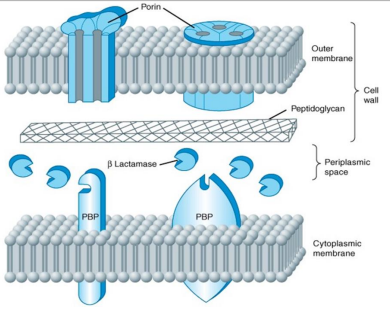
Gram (+ve) Physical properties
peptidoglycan layer is much thicker in grampositive than in gram-negative
Penicillin-binding proteins (PBPs) are membrane proteins that cross-link peptidoglycan.
TRUE/FALSE
True
Cell wall inhibitors work on actively proliferating microorganisms (no effect on bacteria that are not growing and dividing)
True/false
True
Characteristic of Penicillin?
widely effective and least toxic
Note: Penicillins
Penicillins are only effective against rapidly growing organisms that synthesize a peptidoglycan cell wall
(inactive against mycobacteria, protozoa, fungi, and viruses).
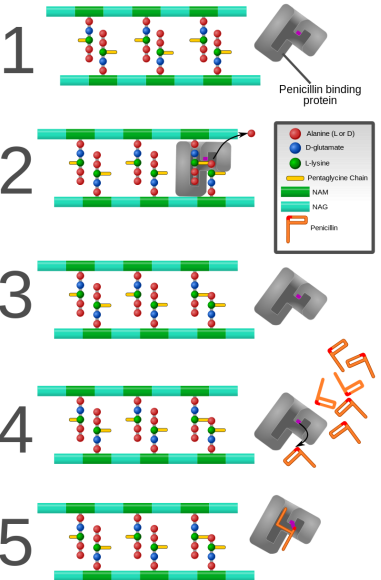
MOA of penicillin(2)
1.Inhibit PBP
2.Production of autolysins
MOA of penicillin for inhibit PBP?detailed
1. Bacterial cell wall consists of strands of repeating (NAG) and (NAM) subunits. The NAM subunits have short peptide chains (used in cross-linking).
2. The penicillin binding protein (PBP) forms a crosslink
3. The PBP dissociates from the wall once the cross-link has been formed.
4. Penicillin is added to the system. It enters the active site of the PBP and reacts with the serine group.
5. The beta-lactam ring of penicillin covalently linked to the PBP and permanently blocks the active site.
Thus blocking cross linking of peptidoglycan