Special Populations
1/180
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
181 Terms
Abnormal
anything that deviates from the norm
tall or short
could be a talent
whether deviating negatively or excelling
people are not abnormal
it’s not that it’s a bad word in nature
but there is a lot of stigma
but we don’t want to call people abnormal
there’s a lot of differences across people
the purpose of studying
not to put apart the differences
but rather to describe or identify patterns that are seen as atypical that are causing distress to the individual and provide resources
psychopathology
the scientific study of mental disorders
doesn’t mean the same thing as abnormal — abnormal being more broad
psychopathology — important to consider it within the psychological triad
emotion
behaviour
cognition
when looking at a child we have to consider that emotion and cognition are private and internal
if the child is young it’s even more difficult to observe the internal things
behaviour is the only thing we can objectively observe
directly observable
when we consider behaviour
have to consider that not all behaviour that is abnormal is necessarily indicative of a mental health problem
atypical behaviour should reflect deviations in underlying processes
self-harm
bed-rotting
lethargy
shaking and pacing
anxiety
avoiding eating
depression
We also need to consider age and developmental level
Developmental norms
typical rates of growth, sequences of growth and forms of physical skills, language, cognition, emotion, and social behaviour
generally a pattern of behaviours that are typical
a pattern of growth that we typically see
generally there are average ages we associate with these mile stones
must consider
behaviour frequency
behaviour intensity
duration of behaviour
situational context
ex: if someone is screaming in a situation, we might think it’s abnormal if we don’t think about the situation they’re in, but it can be normal if they are in pain, roller coaster etc
Normal Distribution or bell curve
usually when looking at behaviour or cog or emo people fall into an average — a bell curve
think about how many people are represented under the curve
bigger area is more people
small area less people
most people fall into the middle/average
ex: IQ
most people fall on average middle of bell curve (100)
consider variability or deviations
look at anyone who falls under 1 standard deviation of the mean it ends of 68% of people
basically most people are falling around average
2 standard deviations
95% of people fall around average
we only really care about the bottom 2.5% in this context
because it could be distressing, dysfunction
deviations cause either: distress or dysfunction
not all normal distributions will behave the same way
ex: sleeping hours
focus on both top and bottom here
bottom because not enough sleep
top because too much could be an indicative of other issues
Deviations interfere with adaptation
adaptation: fitting into the circumstances of your life
3 main things that make up circumstances of you life
school, work or both occupational or academic
connect socially
being able to communicate
taking care of yourself
cleaning up after yourself
bills
cleaning home
things you need to do
we need to be able to do all these things with minimal distress
adaptation will look different for everyone
everyone’s life circumstances look different
the degree to which we adapt will look different for everyone
ex: two girls
first is in a society in which everything she wears is made with buttons
she needs to learn how to do buttons to adapt
another girl where everything she wears is made with zippers
she needs to know how to use zippers to adapt
she wouldn’t need to know how to use buttons so it wouldn’t be a maladaptation
adaptation
fitting into the circumstances of your life
abnormality isn’t all or nothing
there’s a spectrum
normal
able to do all of the things you need to do in your everyday life
and able to do these things with little to no stress at all
abnormal
a lot of issues with distress
middle area
experience a little dysfunction and or distress and not be considered abnormal
think about people dealing with mental health struggles that don’t meet criteria for a disorder
mental disorder:
syndrome of clinically significant behavioural cognitive or emotional disturbances that reflect dysfunction in underlying mental processes, and that is associated with distress or disability in important areas of functioning
doesn’t have to be all three at once
has to be clinically significant
are we concerned about this person
should be diagnosed by an expert
Difference between mental illness and mental health
just because you have no mental illness does not mean you have good mental health and vice versa
ex: maybe you have schizophrenia that is a mental disorder, but maybe they are on top of treatment
they feel great even
that would be good mental health despite have a mental illness
intersecting spectrums of mental illness and mental health
neurodivergent
non-medical term used to describe people whose brains function differently than the ‘typical’ population
Neurodiversity
things like ADHD autism, fetal alcohol
people arguing it’s not a disorder just a natural divergent from typical function
evidence that suggests that people who have neurodivergent things they have some strengths too
people argue if proper accommodations or society was different they would function just fine
people starting to call for change of language
call it things like neurodiversity instead of disorder
Cultural Relativism Theory
there are no universal standards or rules by which we can judge behaviour cognitions and emotions to be atypical or abnormal
these can only be considered atypical when compared to relevant cultural norms
Shyness - Canada and US
shyness considered quite concerning
worry about psychosocial adjustment, social skills
Shyness - China
collectivist cultures see it as a sign of maturity, self-control, and obedience
tend to emerge with more adaptive outcomes
have positive peer relationships, social competence, positive psychosocial adjustment
less likely to exhibit social gaze
less likely to speak or smile
more concern spreading in China recently
study in 2014 reported childrens shyness associated with peer dislike
another study showing parents not liking
could be globalization
need to consider heterogeneity
Kong et al. 2023
anxious shyness: fear or anxiety in social situations
regulated shyness: self-conscious avoidance of public attention and social restraint in behaviour
preoccupied with ourselves and how we come across to people
can be looked as a good think in moderation
Canada vs China
which children are more likely to experience social anxiety as a result of these shyness's
anxious shyness
social anxiety arose in both Canada and China
mean age of around 4 years old
regulated shyness
social anxiety arose in Canadian children
not in Chinese children
appears to be a good shyness
appears to go along with what is valued and expected in that culture
can see that shyness can be adaptive in china
Eye Contact
nonverbal communication that can impact social behaviour
western cultures
expected
signals honesty and attention
some Latin, Asian, and African cultures
can seen as not positive
rude confrontational and aggressive
not as common
Externalizing Problems
examples include aggression, rule breaking, other conduct problems
North America
more patience around rule breaking and aggression
more accepting and typical in young children
as a result we have lower expectations for young children
Thailand
do not accept these behaviours
teachers report many more conduct problems
when actually comparing
American actually presenting more problems but Thailand reporting more
cultural expectations different
The Changing Nature of Culture
western societies
look at eating disorders
used to be that they were only in western societies and at lower rates
because they focused more on a slim figure
now that globalization happens
the standards are present everywhere
now see the prevalence rates similar all around the world
Opposing Cultural Relativism
should cultural norms always be able to dictate what is normal and abnormal
Thomas Szasz (1961,2011) → societies label groups as abnormal to justify controlling or silencing them
ex: WW2 the Nazis viewed Jews as abnormal
ex: Soviet Union labelling people as mentally ill and arresting those who are not
however, culture can influence
the way in which symptoms are expressed
ex: some Asian and Latin cultures experience more bodily symptoms while white individuals experience more cognitive symptoms
ex: some people in some cultures go through rituals
ex: think about symptoms of psychosis
common symptoms is feeling that you are on top of the world and having superpowers
what those powers look like might be based on your religious background
people’s willingness to admit to certain behaviour, thoughts, and feelings
Hattian or indigenous people less likely to admit to anger
depending on culture anger is either valued or suppressed
treatments deemed acceptable or helpful
Scientific Method
observation/question
research topic
hypothesis
test
analyze
report
start again
psychology is different in how we analyze
operationalizing constructs
psychological constructs are intangible aspects of one’s psychology, which can’t be measured directly
behaviour is the only directly observable measure
but even that has underlying cognitions
victimization, shyness, well-being
when it comes to measuring not possible directly
researchers rely on operationalization, or translation of the construct concrete, measurable terms
making sure the thing were interested in is defined in a very specific way
and in a very measurable way
operationalization
important in our own research
need a consistent definition
Systematic Observation
watching children and recording what they say or do
naturalistic observation
behaviour observed in real-life situation
not too far out of their routine
Naturalistic Observation
time sampling
event sampling
time sampling
when we are assessing whether a behaviour occurred or not in a specific time frame
did the behaviour occur within the epoch
good at sequentially understanding children’s behaviour
this ex we have 5 second epoch’s
is the child smiling within the first 5 sec yes or no
are they active yes or no
really important to have a video of the behaviour
maybe we are interested in multiple children
able to validly observe the behaviour
need to consider the operational definition of each behaviour
what is a smile
what is active
doesn’t need to binary either
could say intensity
depends on the experiment and the goal
event sampling
how many times did the child engage in the behaviour the whole time
like the big chunk of time
count how many times they engaged in the behaviour of interest
not the intensity
how many times they smiled in the 20 minutes
usually for longer periods of time
and also interested in less behaviours
interested in fewer things than time sampling
challenge
knowing when a behaviour begins and when it starts
Systemic Observations
watching and recording what they say or do
naturalistic observations: behaviours observed in real life-life situation
might not always engaged in desired behaviour
structured observation: researcher creates setting likely to elicit behaviour of interest
can also use either time sampling or event sampling
Structured Observation
ex: is a child likely to help an adult in need
adult purposely drops something
observing whether they help or not
we could be interested in
what strategy they used to help
using words
actually picking it up
positive affect
do they care
how long does it take to start helping
ex: child did a lab and warmed up then experimenter leaves then a stranger leaves and they start talking to the child,
called the stranger approach
the stranger uses a script and waits a certain amount of time between each line
slowly approaches the child
interested in
are they going to respond fearfully
what is an indictor of fear
facial expression
what they say
the degree to which they are close or far
body language
runs away?
Behavioural coding
operational definition: what exactly does the behaviour look like?
definitions will be outlined in a coding scheme: a document that contains all the rules for coding a set of behaviour for a given task or set up
ex: includes
is a child really showing shyness if they’re saying they’re scared of something else
if they do something weird or funny do we still code?
used so multiple people look at them and they all agree or come up with the same conclusions
not easy
everyone comes with biases
everyone has different perceptions
fidgeting arms:
children told they are going to give a public speech with no preparation
0 = arms remain at sides
1 = arms hinge at the elbows, upper arms remain at side
2 = upper arms move away from sides
3 = arms life above shoulders
fidgeting is not coded if child’s arms are moving for the purpose of expression
Systematic Observation Limitations
observer influence (Hawthorne Effect): participant changes their behaviour because they are being observed
younger children are easier to avoid this
habituation: allows participant to get used to researcher’s presence
Observer bias: expectations influence decisions
may notice behaviours that support the hypothesis and discount those that do not
may interpret behaviour in such a way that they support the hypothesis
Inter-Rater Reliability
are behaviours coded in a consistent way across independent coders?
making sure people aren’t working together to come up with the same outcome
making sure two or more researchers can come up with the same outcome separately
compare ratings for 15-30% of the sample
we need to make sure were in agreement for a smaller part of the sample before we do the rest separately
percent agreement
to what degree did we agree
if we agree 50%, 70% etc our inter-rater reliability is __
depends on how many kids we are looking at though
intraclass correlation
used when codes have variability
used to assess inter-rater reliability when looking at things like time,
we wouldn’t agree exactly but we are correlated
Kappa statistic
best way
actual agreement as a proportion of the potential agreement following correction for chance agreement
the degree to which we could agree after we account for change agreement
ranges from -1 (less agreement than can be expected by change) to +1( perfect agreement)
researchers generally aim for a Kappa of 0.7 or higher
need stats programs
need what we are doing
need data from rater 1 and 2
What does a smile look like?
genuine Smile
lips turned up
balls of cheek prominent
squinty eyes
Controlled smile
might not have raised cheeks
might not have squinting eyes
but lips still turned up
Operationalization
provides a good definition
but will still be disagreement
everyone has personal bias
agree to the extent we can get reliable statistics
The Birthday speech
instructed to give a speech about their most recent birthday in front of a camera
this task commonly used to assess
anxiety
shyness
any other uncomfortable behaviour
first video
swinging side to side
arms at sides hands in pockets
could this be anxious or regulative
could be a squirmy kid and this is his baseline
could be excitement
stuttering
could be anxious
could be baseline
redness in cheeks
he was facing the person he was speaking to
a little bit of confidence
attention to the conversation
smiling
excitement?
Behavioural Coding - activity
operational definition
what exactly does the behaviour look like
activity
pick two behaviours
what is it and what is it an indicator of
one time sampling and one event sampling
create operational definition for each
event = stuttering
operational definition - any hesitation during speaking and use of filler words
looking at number of occurrences throughout total event
indicator of anxiety, excitement, nerves, could be baseline
time = swaying
operational definition - shifting weight from one side to the other
looking at the time spent swaying within the 30 sec epoch
indicator of anxiety, excitement, nerves, could be baseline
Questionnaire Reports
what makes them special
insight on what the person thinks and feels
can get complicated when dealing with young children
so should we be asking young children about their mental health symptoms?
the problem is they don’t have the best insight into their own thoughts and feelings
they may not have the best awareness about themselves
that can be a big issue
another big issue is language
some questionnaires may have big language
Collecting Information from infants
of course differ to parents for information
school teachers
older siblings
basically any caregivers
often do ask the kid to even if we don’t expect good things
Self Reports for young children
Hearter self esteem scale
assessing children’s self esteem
first break it down into 2 options
on left side a girl who does puzzles well on the right side one who doesn’t
which one is most like you
then they have to make a forced choice
the gender depends on who is being asked
once made the forced choice break it down further
Likert Scale
select the circle that is most like them
4 being really good at puzzles
the bigger the circle the better at puzzles
basically 2 forced choices
we would start asking real questionnaires at 8
start to notice children begin to have more insight on their thoughts and feelings
The Child Behaviour Checklist (CBCL)
long and comprehensive checklist
not used for diagnostic
used for research
helpful because
provides information on narrow and broad stuff
CBCL Scales
narrow-band scales makeup broadband
broadband — an umbrella for some of the more narrow-band scales
Internalizing Behavior (aka negative emotional or behavioral patterns directed inward) — broad-band scale
narrow-band scales:
Anxious/Depressed Behavior
Withdrawn Behavior
Somatic Complaints
Externalizing Behavior (aka outward directed, disruptive behaviors) — broad-band scale
narrow-band scale
Rule Breaking
Aggression
Other broad-band scales
Social Problems
Thought Problems
Attention Problems
How to score an CBCL
looking at the questions in the CBCL and how they turn out
horizontal dotted lines being a cut off t=70
helps us determine a borderline range
T-score: value that describes how far a data point is from the population mean
T-scores of 70 or higher indicate clinical range functioning
anything above that 70 t-score they are clinical range
T-scores between 65 and 70 are considered ‘borderline’
middle of both dotted lines
T-scores below 65 indicate normal range functioning
below both dotted lines
Reversal Design
also referred to as an ABA design
A — baseline
are they actually engaging in positive behaviours? (class example)
if after day 4 we introduce an intervention will they change
B—treatment
better than baseline
we want to make sure that the treatment is actually the thing impacting the behaviour
consider the ethics of removing that treatment
then remove it and see if behaviours go back to baseline
does the participant worsen when treatment is not being provided?
limited to interventions:
without lasting change (e.g., drugs)
can’t use this design if the intervention leads to lasting change
don’t want to use it on learned coping skills
where there is behavioural change
psychotherapy, coping skills, talk therapy not good candidates for this design
Multiple Baseline Design
can account for more than one behaviour
can account for the same behaviour in different settings
looking at one behaviour (tantrums) or looking at throwing behaviour
can also use multiple particpants
can see how different time points can impact the intervention
ex: looking at behaviours in school
look at first day
then look at 2 weeks
then intervention on the first day with a different child
then 2 weeks with different child
reactivity and behavioural inhibition
high reactivity in a situation where a person is experiencing something new is a good indicator they are highly behaviourally inhibited
behavioural inhibition is reactivity to new stimulus
Quadrelli et al. (2015) Do infants respond to ostracism?
nfants responses to being ostracized
84 13-month-old infants
baseline phase
both conditions experienced the same thing
baby playing pass the ball to the two experimenters
Inclusion Condition
No exclusion
continued that game of pass
Ostracism Condition
Excluded from ball- passing game during experimental phase
no longer passes to the baby
Quadrelli et al. (2015) Do infants respond to ostracism? Results
results
inclusion group doesn’t change much across the variable changes
exclusion group
active engagement
no change in inclusion group
because there is no asterisks
asterisks on ostracized group
statistically signifigant change
because they are essentially trying to get more involved in the game
maybe a show of infants not being good at self regulation
visual attention
similar to active engagement
anything that denotes reactivity?
we are capturing the state representation
regulatory outcomes
Two main hypothesis about temperament - Spectrum
can be low or high
basically most people fall around average
it’s not that temperament is a spectrum it’s more about how mental health fits in the spectrum
saying that at the very high or lows depending on the temperament we are talking about that determines mental illness
Two main hypothesis about temperament - Risk Factors
think shyness
social anxiety is more likely to happen when high in shyness and low in sociability
a bunch of temperaments acting as risk factors
Irritability
low threshold for experiencing agitation, frustration, anger in response to a blocked goal or reward
usually characterized by negative mood and dysregulation
more irritable a child is the more likely to be diagnosed with any DSM disorder
Diathesis Stress Model
account for vulnerability (bio or psych) as well as additional stress
considering both at once when considering who will develop a disability or disorder
Predispositions in combination with additional stress can lead to the emergence of a disorder
looking at different start lines
some have ones really far away — they don’t have a lot of vulnerabilities
some are closer to finish line — lots of vulnerability
stress will move you closer on the finish line
Based on the diathesis stress model, plot what you might expect to see in:
an individual with high resilience
an individual with high vulnerability
experiencing negative outcomes with exposure to negative experience in environment
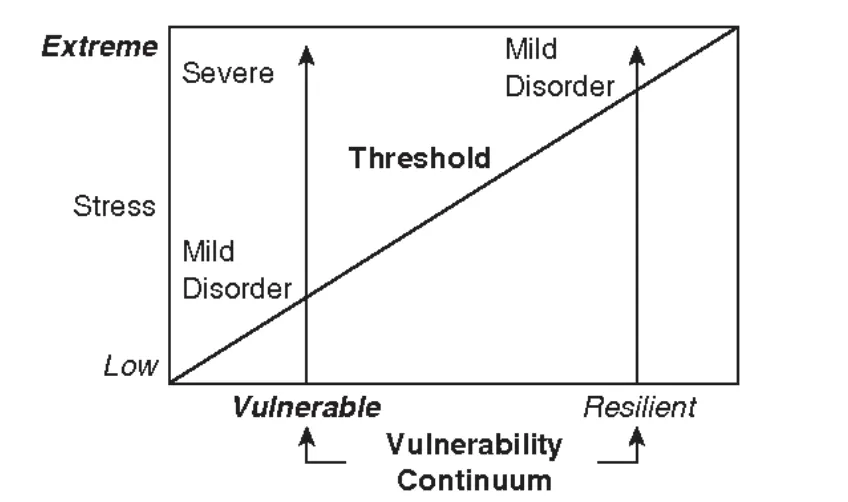
Model for vulnerability and resilience - Diathesis Stress
x-axis: vulnerability continuum
y-axis: how extreme the stress is
in this iteration of the model
how severe is this disorder going to be
if a person is very vulnerable—they need relatively little stress to meet criteria for disorder
however when that vulnerable person meets more stress the severity of symptoms gets worse
on other end, someone who is very resilient
needs a lot more stress in order to experience any symptoms
might meet criteria if they get enough stress
because they are highly resilient person their symptoms won’t be that severe as vulnerable persons
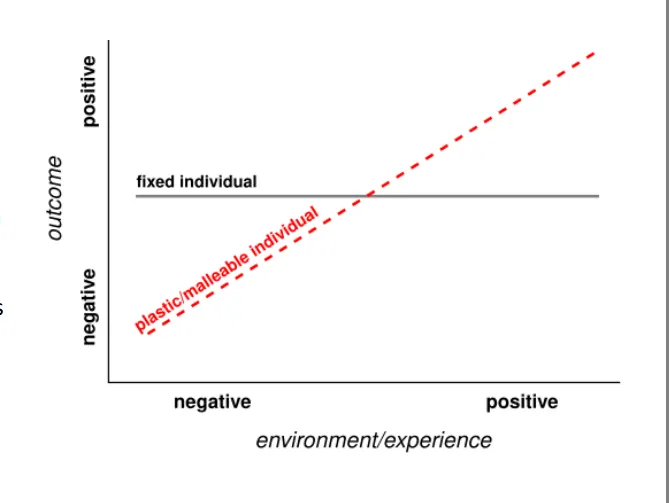
Differential Susceptibility
Some children can flourish in developmentally appropriate and encouraging environment
before looking at that vulnerable person as someone who is relatively stable across environments— in this model we look at how some children based on certain traits they have will be malleable
some children with negative environments will have negative outcomes
some children with positive outcomes will flourish and have extremely positive outcomes
a fixed individual will experience same outcomes regardless of the environment they are in
Differential susceptibility vs diathesis stress model
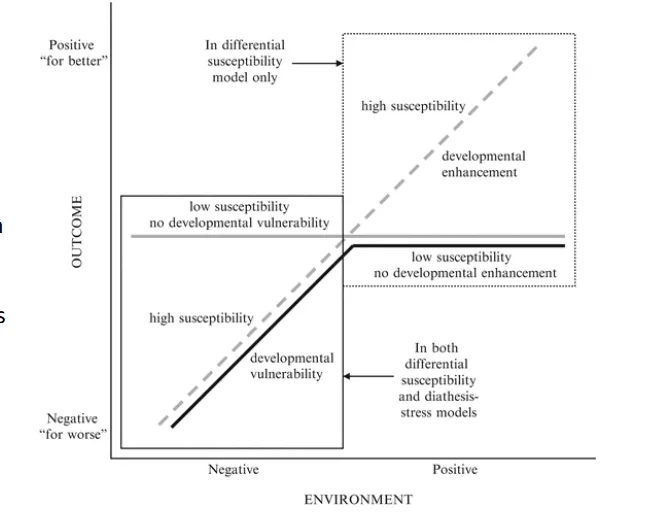
Differential susceptibility model
Surgency model
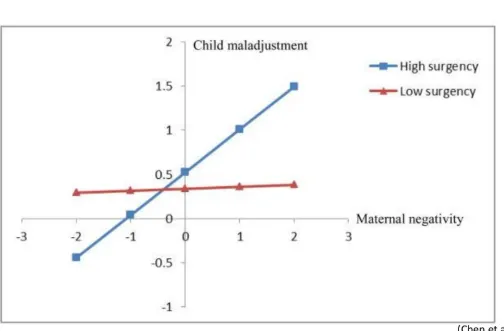
looking at surgency
the degree to which a child is more likely to experience positive emotions due to relatively small things in their environment
only looking at one thing in the environment
the out come is one particular outcome
so what kind of child will be relatively fixed
low surgency
high surgency - high bio sensitivity/malleability
common anecdote
in general we can think of these two types of children based on the kind of flower they are
fixed child
considered a dandelion
be able to grow in any environment
but is it particularly flourishing—no
malleable
orchid
flourishes in the proper environment
won’t flourish in bad environments
Interactionist model
have to consider if it’s an interaction at all?
you need to look at whether the things looking at are crossing paths
if they are different slopes on the graph then they are not interacting
can be longitudinal or may not be
typically over time we look more at transactional model
interacting over time
Transactional model
basically like crossing over each other over time
interacting over time
Kappa Statistic Model
accounts for correcting for chance
acceptable 0.6
0.7 better
anything below bad
Falconer Formula
helps us to estimate heritability based specifically on twin studies
assuming they are raised together
multiplying 2(rmz - rdz)
correlation of mz-correlation of dz
Correlation or mediation
to see if is a mediation we’d have to look at:
IV sugar intake DV misbehaviour
if we account for three variabes together and we saw the p value reduce itself to a .1 after being 0.01
therefore initially statistically signifigant and now it’s not
means that arousal mediates the intake of sugar and misbehaviour
basicually if pvalue was signifigant then reduced to not being signifigant that is a mediating variable
it better explains that relationship
Twin study monozygotic as similar as dizygotic twins
outcome = gene + environment
outcome = genetics + shared environment + unshared environment
if monozygotic were almost as similar as dizygotic then genetics aren’t playing a big role
unshared environment having a bigger role
the twins were raised together so shared environment has an equal role
big impact of the unshared environment — twins looking similar
What is a Psychological Assessment?
Formal evaluation of individual’s functioning in one or more areas
standardized way to figure out whats going on
figure out if there’s a psychological diagnosis
how can we go forward in supporting them
some areas we might look at in an assessment
Learning
Emotions
Behaviour
Conducted by:
Clinical psychologists
the main people
especially when thinking about a comprehensive one
often involves standardized testing
especially when mental health is concerned
Psychological consultants with specific training (supervised)
when talking about a psych assessment and what the steps are
referral
when someone brings themselves forward about wanting to get looked at
intake
sitting down and talking about background information
first point of contact
information gathering/testing
more hands on work with the client and peers of client
might test for things like intelligence, anxiety, attention etc.
report
put the information in a formalized report
talk about what you learned about this person and what you will do now
feedback meeting
talking about the results of that report
meeting with client to talk about it
formulation
everything is a very back and forth process with everything
it’s a working concept about what is going on with this clien
Referral
Setting (schoolboard, private clinic, etc.)
it can go through a lot of public methods
but waitlists very long
it can go through private
but money
can be community — family clinics
hospital
basically any professional in their lives
otherwise a parent
Referee
the one to bring the assessment forward
because kids aren’t the ones referring themselves there might be a lot of motivation issues
Referral question
vary
like a research question
Learning?
Attention?
Emotions? Behaviour?
Specific query (e.g., ASD? Gifted?)
Intake
Consent; confidentiality
age based laws in Canada that determine that the kid you are working with is giving consent or if their parents are giving consent
Interview
sometimes pretty short
getting information
Top Hat: What types of questions / areas would we want to ask about during an intake interview?
presenting concern
what is the concern first of all
why now?
when did they come up?
different settings?
how long?
learning
what area of learning reading or writing?
specific difficulties
what exactly are they struggling with when it comes to the reading, writing or math
common mistakes?
who noticed and when?
feelings and attitude about learning especially?
developmental history
labour/delivery? any complications, health concerns
injuries or hospitalization, medication, vision and hearing
milestones
major life events
family death, big moves or transitions, COVID-19, trauma
other
family life? emotions? behaviour
friendships and bullying
prior assessments
strengths
what are they good at?
Testing
Can look different
Behavioural Observation
your direct observations about how the child is throughout the assessment
Ability vs. Skill
ability — things we can do that are static
skills — can improve over time
Typical battery
Cognitive Functioning (verbal, non-verbal, visual spatial), Processing Speed Memory, Visual-Motor Integration, Phonological Processing, Oral Language, Achievement/Academic Functioning
if there's concerns with mental health we might do questionnaires asking about:
Emotions/Mood
Behaviour
Attention
Executive Functioning
Adaptive Functioning
Report
Varies
Like a lab report
Percentile ranks
how you compare with other children's results
every measure you use is normed to their age range
Recommendations (school, home, attention, etc.)
based on everything we learned what would be helpful to support this child
Percentile Ranks Client’s performance in relation to peers of the same age
easy way to explain a child’s scores in relatoin to other’s
Formulation
basically putting together the story
Interpreting data with context!
Sometimes: Diagnosis
Feedback
Depends on consent
Emotions
Clear and accessible
language you use matters
Client/caregiver choice re. sharing
Classification - Hi top
when we think about personality we think about 5 big personality traits that encompasses personality
everyone falls somewhere on the spectrum
5 orthogonal or spectrums you can fall on
The DSM (& other categorical approaches)
problem with DSM is we need to have a cut off line
first of all there is heterogeneity within one disorder
Heterogeneity within one disorder
if someone has anxiety their experience can be vastly different from another individual who has anxiety
Comorbidity across disorders
the overlap quite oten
like depression and anxiety
at the very top General Factor of Psychopathology (p-factor) (adults)
explaining all psychopathology within that one factor
not the best way
but there is evidence supporting it
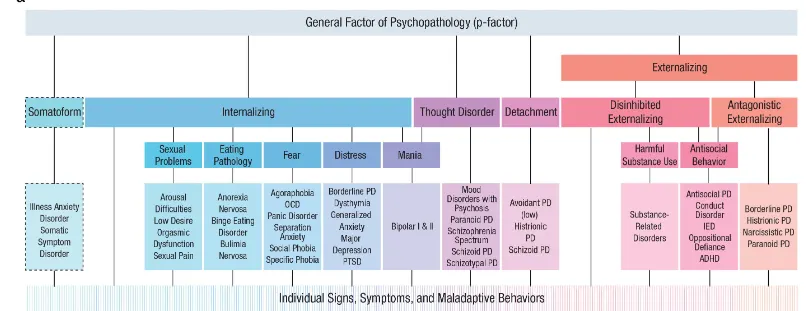
next level down secondary scale - externalizing (adults)
only secondary scale
only covers two spectrums
disinhibited and antagonistic spectrums
3rd level down - 6 different spectra (adults)
find strongest evidence for validity and reliability
Internalizing: excessive negative emotions
Disinhibition: excitement seeking, impulsivity, substance problems
typically issues with substance abuse
Antagonism: aggression, callousness, grandiosity
Thought disorder: delusions, hallucinations, paranoia
Detachment: low social drive, social withdrawal
Somatoform: unexplained medical symptoms and associated worry and reassurance-seeking
Youth version of the graph
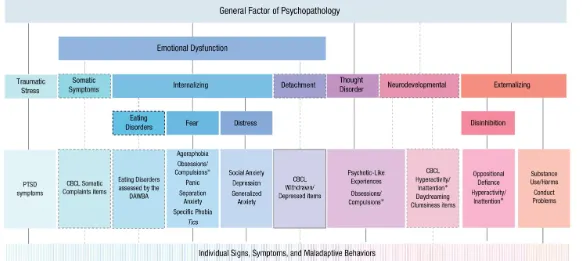
changes in graph for youth version
disinhibition is no longer a main spectra it’s below externalizing
externalizing becomes one of the main spectra
neurodevelopmental - more about inattention, obsessions impulsions, etc. is a new main spectra
traumatic stress
considers ages 11-17
Correlational design
correlational studyL looks specifically at the relations between the variables as they exist naturally in the world
what most of mental health research consists of
looing at how things naturally exist in the world
how does mental health impact academic success
how does living with depression effect social relations
correlational coefficient r
direction and strength of a relation between two variables
a line moving upwards is positive correlation
positive correlation will always be a positive r
as one variable increases so does the other
a line going down negative correlation
a negative correlation will always be negative r
if one increases the other will decrease
a straight sideways no correlation
but pay attention to the r and whether the p-value is below 0.05
Correlational vs. experimental design
we can’t always no which variable is driving the other variable
multidirectional
we don’t know the driving variable
correlation not equal to causation
we also don’t know if there’s a third variable
confounding factors
Experimental Research
two types
randomized: participants assigned to different groups using random assignment
when we randomly assign individuals to a group we hope that the groups will represent the larger sample from which we are drawing
quasi-experimental: subjects not randomly assigned
looking at differences between genders is an example
quite common in mental health research because a lot of the time were interested in healthy controls in comparison to mental health issues
allows for causal conclusions
we are assuming the only difference between two groups is what we chose to look at
involves: an independent variable (a cause that is tested) and a dependent variable (an effect that is tested)
testing differences between groups with statistical tests to determine if the difference is larger than would be expected by chance
Experimental Design
example: whether children are likely to share with a friend or stranger
assign to condition
friends condition
no friends condition
create standardized setting
lab and procedure
everything should be the same regardless of the group they’re in other than the assign condition
manipulate the independent variable
play with friend
play with non-friend
measure dependent variable
amount of time before child shares toy
compare results
which group had the longer time
children share toys sooner with friends than non-friends
Case Study
when we are looking at one or few participants
intervention or experimental manipulation with a single participant
not an experiment cause no control or treatment group
can be used when participants are unique or present with unique issues
like schizophrenia
or when intervention is unique and expensive
ex: maybe we have a new robotic walking aid and it is really expensive we want to see if it’s worth making more
could run a case study with a child who has mobility issues and look at if that aid is working for them
designs for studying age related change
cross sectional
longitudinal
accelerated longitudinal
Cross sectional design
testing children of different ages at one particular point of development
ex:
interested in infants 10yo 20yo
we would have three different groups all tested in the same year
we can then directly compare how they are performing on different tasks
however issues
cohort effect
ex: if we test in 2020 and we have babies born in 2020 those babies will have a very different developmental journey then those who were born 10 or 20 years before then
it is possible those things could have effected the baby
consider we can’t assess continuity in the same individual
making big assumptions when assessing babies to 10yos etc
they are different people with different cultures, families, experiences
can’t make a ton of grand conclusions if they are not actually the same people
Longitudinal Design
studying the same individuals observed or tested repeatedly at different points in their lives
ex:
first tested in 2020 then again in 2030 and again in 2040
issues
we do have to wait 20 whole years for kids to grow up
very expensive
attrition
when participants or participant families become uninterested in the research
basically drop out of study
sometimes there is systematic reasons for dropping out of a study
practice effects
depends on the study if its like 10 years between tests your good
but if it’s under 5 years then ya there will be
practice effect: improvement over time might be attributed to practice with a particular test
selective attrition: those who drop out of the study may be significantly different from participants who remain
Cohort effects: developmental change may be particular to specific generation of people
Accelerated Longitudinal Design
sequences of samples that are studied longitudinally
can account for practice and cohort effects while maintaining continuity
ex:
babies born in 2020 —> follow up 10 years later
10 year old's tested in 2020—> follow up 10 years later
able to get same time points than we did before but getting it more quickly and account for practice and cohort effects
basically look at the 2 groups and see if they are similar to eachother in response when at same age
look at 10 year olds at 2020 and 2030 see if they give similar responses
account for attrition
there is a high chance of high attrition if it is a long test
we can add in kids of that same age to keep our sample the right size
and helps with practice effects as well
Temperament
Core emotional, cognitive, and behavioral characteristics around which later personality traits develop
characteristics you will have almost immediately
can look at them in fetuses before they are even born
some can regulate by sucking on thumb
others are more reactive
seeing individual differences very early on
biologically-based behavioral styles that are stable across situations
we don’t really use this term once you are older because by then you have environmental influences
very evident from infancy
stability
we do see that temperament is generally stable over time
the impact gets smaller as we grow up
a broad definition
temperament is individual differences in emotional reactivity and self-regulation
Reactivity
excitability, responsivity, and arousability of behavioural and physiological systems
threshold for some sort of response
to what degree are you going to feel sad while you watch a sad movie
look at it as a thermometer
everyone has a different size of thermometer
we all need a different level of stimulation to get a reaction
Self-regulation
neural and behavioural processes functioning to modulate our underlying reactivity
the degree to which we can bring our reactivity back down
speed to which we can do it too
can be conscious but mostly unconscious
Co-regulation of Emotion
parents help teach children how to regulate their emotions
we get physical comfort and touch from parents
early on, touch and comfort is effective
think rocking, touching, stroking
when close to our parents and our parents have calm physiology we see that this helps us synch up infant with parents physiology
not just with infants
basically at any age if you are stressed it is helpful to have physical comfort
later, parents will use distraction as a method of co-regulation
specifically they are going to try to distract the child away from the thing that is distressing
example: child receives disappointing prize
parent shifts child’s attention to accompanying stickers (just something else)
reframe prize → uses sock to make hand puppet
provide comforting support and understanding
Co-regulation of Emotion Western societies
active problem-focused regulatory strategies
talk to child about emotions
try to solve the problem causing distress
directly focusing on emotions
Co-regulation of Emotion Asian Societies
endurance of emotion to maintain social harmony
being able to stick through negative emotion without engaging in too much behavioural response
it is important we do need to be able to sit and feel uncomfortable
but especially important in collective societies
Reactivity and Regulation
generally, behavioral reactivity and regulation can be used as a measure/proxy for emotional reactivity and regulation
and likely underlying physiological systems
how do we knowo how quickly a child reacts emotionally?
we look at facial expressions
behaviors
how do we know that a child is regulating their emotions?
see how quick they calm themselves down
we do have to consider age though
Emotion regulation - Infant
fussing, looking away
self-soothing
even before born
alert parents around them with crying