PT 471C
1/103
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
104 Terms
relative flexibility
increased mobility or frequency of movement in a joint adjacent to a body part with restricted mobility
- stiff muscle, joint capsule, tendon, bone, ligament
the body compensates for restrictions by ____
increasing motion elsewhere to maintain function
when a joint develops abnormal compensatory motion in response to an adjacent stiffness, what happens to the joint and its supporting structures
stabilizing muscles, tendons, ligaments around the joint become too flexible or lax, providing insufficient stiffness or resistance to motion
what is a common issue with relative inflexibility
shear force
stiff muscle
goes through full range of motion, but often creates movement compensation when countered by a less stiff muscle
less stiff muscle
- fewer sarcomeres in parallel
- relatively weaker: cannot overcome passive tension of antagonist
- decreased excitability of alpha motor neuron pool
relative flexibility due to muscle dominance
muscles can become overly dominant in action, leading to movement fault
- hamstrings > gluteus maximus for hip ext
- spinal extensor > gluteus maximus for return from L/S flexion
- lats > subscapularis for shoulder IR
secondary test
a correction of the movement to determine if a change occurs
- with symptoms, range of motion, etc
when a muscle is short, you should ____
lengthen the muscle
when a muscle is stiff, you should ____
create more stiffness in muscles that prevent compensation
pathokinesiologic source
tissue of pathoanatomical structure believed to cause symptoms
- ex: supraspinatus tendon
kinesiopathologic source
mechanical factor that causes tissue irritation
- ex: insufficient scapular upROT
MSI diagnosis
determined by motion, direction, or alignments that most consistently elicit symptoms, and when corrected, decrease symptoms
MSI diagnostic name is based on:
- the motion that is performed in a less than idea manner
- movement or postural alignment which the pt complains of pain and when corrected reduces their symptoms
- ex: flexion syndrome
directional susceptibility to movement (DSM)
- repeated motions and sustained posture alter tissue and movement patterns
- increase frequency of accessory and physiologic movements into a specific direction
- stress/microtrauma/tissue damage
- inflammation/pain
- DSM increases potential for tissue injury
physiologic/osteokinematic hypermobility
- greater motion than ideal range
- in relation to composite body area
accessory/arthrokinematic hypermobility
- greater translation of roll/glide/spin
- in relation to joint name
frequency of motion hypermobility
- movement more often at a specific joint/muscle than adjacent joints/muscles during a functional activity
- more motion than recommended for functional task
how to determine patient MSI diagnosis
primary test: unadjusted movement
secondary test: adjusted movement that improves mechanics and symptoms
fundamental principles of physical stress theory
1. changes in relative level of physical stress cause predictable response to all biological tissue
2. 5 responses to physical stress: atrophy, maintenance, incr stress tolerance, injury, death
3. inflammation renders tissue less tolerant to stress than prior to injury
4. tissues are affected by history of recent stresses
5. stress thresholds can be modulated based on: extrinsic/intrinsic factors, psychosocial factors
6. level of exposure to physical stress is defined by magnitude, time, and direction of stress application
normal sequence of lumbar flexion
- initial motion from posterior sway of pelvis as hips flex
- as hips flex, lumbar spine reverses lordosis
- when lumbar motion completes, last of motion comes from hip flexion
abnormal lumbar flexion ROM
- greater than 25-30 degrees lumbar flexion
- less than 80 degrees of hip flexion
- more than 50% of L/S flex motion before initiation of hip flexion
return from lumbar flexion normal sequence
- initial motion from hip ext
- equal portions of hip ext and L/S ext throughout motion
abnormal return from lumbar flexion
- initiation of motion with L/S ext before hip ext
- exaggerated forward sway
- overuse of L/S paraspinals and underuse of glutes can increase facet pressure
lumbar sidebend ROM normal sequence
- more thoracic than lumbar motion
- smooth curve
abnormal lumbar sidebend ROM
- hinge points
- straight lumbar spine
- secondary test: block w/ your hand and see if symptoms or motion improves
- positive sign for ipsilateral rotation if hinge point, stabilize above iliac crest
single leg stance common errors
- pelvic drop
- trunk lean
- pelvic lateral shift
- pelvic IR
lumbar rotation normal ROM
- 13 degrees to ea side
- majority of motion comes from thoracic
seated hip flexion normal movement
able to flex hip to 120 degrees without lumbar compensation and with neutral femur
abnormal seated hip flexion
- anterior/posterior pelvic tilt: flex/ext syndrome
- pelvic rotation
- trunk sidebend and/or rotation
- femur ER/IR
- stabilize pelvis to see if Sx change
subcostal angle
- normal: 90 degrees
- > 100: short rectus + internal oblique, long external oblique
- < 75: short external obliques
paraspinal asymmetry
when one side of lumbar area is 1/2 inch larger, considered positive for lumbar rotation
supine hip ER normal movement
- no pelvic or lumbar ROT within first 50% of movement
- start with one knee extended
- go to hooklying if too difficult
- test for rotation in pelvis: stabilize to see if Sx improve
lumbar movement dysfunction classifications
- lumbar flexion
- lumbar extension
- lumbar flexion rotation
- lumbar extension rotation
- lumbar rotation
treatment of lumbar movement dysfunction (Maluf 2000)
- correct lumbar movement dysfunction by limiting direction specific motion or alignment that elicits painful symptoms
- address impairments in muscle force and joint flexibility
MSI exercise principles
- perform modified versions of movement tests
- goal to modify movement by decreasing preferred movements of the limb or trunk
- emphasize correct performance over number of reps
- avoid reproduction of Sx
lumbar extension/rotation syndrome sources of Sx
- facet dysfunction
- spinal stenosis
- spondylolisthesis
- spinal instability
- DDD
- L/S OA
L/S ext/rotation syndrome relative flexibility and stiffness impairments
lumbar spine is excessively flexible into extension and ROT
possible stiff/short:
- hip flexors/rectus femoris: anterior tilt
- hip abductors: lateral pelvic tilt
- TFL: pelvic rotation
- latissimus dorsi: anterior tilt, extension
not stiff enough:
- abdominals: posterior pelvic tilt
- lateral abdominal/obliques: lateral tilt, pelvic rotation
- gluteal muscles: posterior tilt, return from flexion
L/S ext/rotation muscle recruitment patterns
- dominance of L/S extensors without counterbalance of abdominals for posterior pelvic tilt
- return from standing: L/S extensor dominance over hip ext
- dominance of hip flexors over abdominals for leaning forward, sitting up
- eliminating hip flexor muscle activity may reduce Sx
L/S extension syndrome flexibility/stiffness impairments
L/S more flexible into extension
short/stiff:
- hip flexors: anterior tilt
- lats: anterior tilt, lumbar extension
not stiff enough:
- gluteals: return from flexion
- external obliques/abdominals: posterior tilt
L/S rotation syndrome tissue sources
- pain with lumbar rotation and sidebend
- DDD
- spondylolisthesis
- OA
- spinal instability
- facet dysfunction
L/S extension syndrome muscle recruitment
- hip flexors dominant over abdominals
- L/S paraspinals dominant over hip extensors
L/S rotation syndrome flexibility/stiffness impairments
L/S more flexible into rotation and side bend
short/stiff:
- L/S paraspinals: lateral flexion/SB
- hip abductors: lateral flexion, lateral pelvic tilt
- TFL: pelvic rotation
not stiff enough:
- lateral abominals/obliques: cannot control rotation
- transverse abdominis
L/S flexion/rotation syndrome tissue sources
- herniated disc
- DDD
- OA
- spinal instability
limited hip motion in L/S flex/rot syndrome
- usually not due to hamstring stiffness/shortness
- limited hip motion result of influence of hamstrings to exert control over weight of the trunk
corrected forward bend for L/S flexion syndrome
place hands on elevated table and bend forward by flexing hips
L/S flex/ROT syndrome flexibility/stiffness impairments
L/S more flexible into flexion and rotation
short/stiff:
- hamstrings
- glutes
- rectus abdominis: more support than back ext
- TFL: pelvic ROT
not stiff enough:
- L/S paraspinals
- obliques: cannot control rotation
L/S flex/rot syndrome muscle recruitment patterns
- rectus abdominis dominant over back extensors for providing trunk support
- abdominals have poor control of lumbopelvic rotation: obliques
L/S flexion syndrome tissue sources
- herniated disc
- lumbar strain
- DDD
femoral anterior glide syndrome
- inadequate posterior glide of femur during hip flexion due to taut posterior capsule, stretched anterior capsule
- altered PICR of hip flexion
- causes iliopsoas tendonitis
- femur impinges on anterior tissue of joint capsule
- development associated with hip extension activities stretching the anterior joint capsule
femoral anterior glide syndrome relative flexibility/stiffness impairments
short/stiff:
- TFL
- hamstrings (medial)
- hip ER: prevent posterior glide of femur
not stiff enough:
- iliopsoas: prevent anterior capsule from getting pinched
- glute max/medius
femoral anterior glide syndrome muscle recruitment pattern
- TFL dominant over iliopsoas and posterior glute medius
- hamstrings dominant over glute max
- medial hamstrings > lateral hamstrings causing hip IR with knee ext
hip adduction syndrome
- with or w/o IR, w/ IR most common
- women > men
- piriformis syndrome
- ITB syndrome
- result of insufficient performance of hip abductors
hip adduction + IR syndrome flexibility/stiffness impairments
short/stiff:
- hip adductors
- TFL: dominant as hip abd
not stiff enough:
- glute med/max
- hip ER
hip add + IR syndrome muscle recruitment pattern
- hip add dominant over hip abd
- TFL + sartorius may be used to abd
hip extension with knee extension
- insufficient gluteus maximus or quads
- contraction of hamstrings to help quads with extension
- pain at ischial tuberosity - HS origin
- likely hamstring strain
hip lateral rotation syndrome
- insufficient participation of hip ER
- shortened piriformis with sciatica
- dominance of hip ER mm over IR
- short/stiff hamstrings, quads, hip ER mm
femoral accessory mobility motion hypermobility
- rotation and excessive accessory motion of anterior/superior glide occur during hip flex/ext
- hypermobility
- potential labral tear
- excessive compression of hip by rectus femoris and hamstring stretching in hip flexion/extension
femoral accessory motion hypermobility flexibility/stiffness impairments
- rectus femoris and hamstrings stiff/short
- iliopsoas, hip rotators, gluteus medius not stiff enough
femoral accessory motion hypermobility muscle recruitment
- hamstrings dominant as hip extensors
- TFL + rectus femoris dominant hip flexors
hip flexion arthrokinematics
- spin
- anterior roll, posterior glide
hip extension arthrokinematics
- spin
- posterior roll, anterior glide
hip IR arthrokinematics
anterior roll, posterior glide
hip ER arthrokinematics
posterior roll, anterior glide
external oblique actions
- posterior pelvic tilt bilaterally
- contralateral trunk rotation w/ CL internal oblique
- ipsilateral pelvis rotation w/ CL internal oblique
- ipsilateral side bend
iliopsoas muscle actions
- hip flexion
- anterior pelvic tilt
- upper lumbar extension
- lower lumbar flexion
- ER and ABD
erector spinae actions
- spinal extension
- anterior pelvic tilt
- pelvis lateral tilt
latissimus dorsi action on spine
- pelvis anterior tilt
- L/S extension as compensatory motion when short, or if abdominals not stiff enough to counterbalance
QL muscle action
- ipsilateral side bend
- lateral pelvic tilt
TFL actions
- hip flex, IR, abd
- can cause pelvic rotation if short/stiff, also resulting in lumbar rotation
gluteus maximus actions
- hip ext + ER
- upper half abd
- lower half add
spurt muscle
- origin away from joint
- insertion close to joint center
- ex: piriformis, glutes, iliacus, psoas
shunt muscle
- origin near the joint
- insertion away from joint
- causes shear/compression force if not countered by local muscles
- ex: hamstrings, TFL, sartorius
the hip greater trochanter will move ____ when hamstrings are dominant muscle for hip extension
anteriorly
- will maintain its position or move posteriorly if glutes and piriformis are prime movers
Van Dillen article hip ROM + LBP
- is hip PROM different in people with or w/o LBP for people who participate in rotation related sports
- group with LBP had less total hip ROT than group w/o LBP
- LBP group displayed more asymmetry of total hip ROT between right and left
- directional demands of sport may be important factor to address or consider in interventions
Lewis article hip forces
Increases in anterior hip forces due to muscle can be attributed to:
- decreased force contribution of glutes in hip ext
- decreased force contribution of iliopsoas during hip flex
- increasing hip extension angle
compensations:
- semimembranosus, TFL, sartorius activation increases with decreased glute activation
- TFL and sartorius activate to offset ER and add torques
- TFL, sartorius, and add longus dominate hip flex instead of iliopsoas
femoral lateral glide syndrome
- laxity of hip abductors cause femoral head to glide laterally to the point of subluxation
- popping hip with hip add/IR
- excessive hip add, IR with movements
- short/stiff TFL, weak glute med/external rotators
tibiofemoral rotation w/ valgus syndrome
excessive IR and add of femur compared to tibia
- may impact ITB, tibiofemoral J, patellofemoral J
- PFPS and ITB syndrome
- resting femur IR or tibia ER
- posterior pelvic tilt indicates weak glutes
- potential XS pronation of feet
tibiofemoral rotation w/ valgus flexibility/stiffness impairments
short/stiff:
- TFL: femur IR or tibia ER
- tibia ER
not stiff:
- hip ER:
- hip abd
- tibia IR
tibiofemoral rotation w/ varus syndrome
varus thrust in gait
- medial compartment tibiofemoral J at risk
- large knee adduction moment arm, increase force thru medial J compartment
- toe out gait may potentially relieve Sx
- femoral IR + knee hyperext
- potential supinated/flat foot
TFRVar flexibility/stiffness impairments
stiff/short:
- TFL: femoral IR
not stiff:
- hip ER
- hip abd
tibiofemoral hypomobility syndrome
limitation of knee motion due to degenerative changes or immobilization
- may be due to arthrokinematics or mm extensibility
tibiofemoral hypomobility stiffness impairments
short/stiff:
- hip flexors
- hamstrings
- ankle PF
not stiff:
- glute max
- hip ER
- gastroc
- quads
knee extension syndrome
knee pain associated w/ quad dominance or stiffness resulting in excessive pull on patella
- patella superior glide/patella alta
- patellar tendinopathy, quad strain
- osgood schlatters
knee extension syndrome secondary tests
- inferior glide of patella during movement
- allow tibia to advance forward over foot
knee extension syndrome stiffness impairments
short/stiff:
- quads: pull patella superiorly
not stiff:
- patellar tendon:
- glutes
- hamstrings: imbalance puts more demand on quads
knee hyperextension syndrome
knee pain associated with impaired knee extensor mechanism
- dominance of hamstrings, poor performance of glutes and quads
- pain with prolonged standing, rapid knee ext activities
- PFPS
- fat pad syndrome/Hoffa
knee hyperext syndrome stiffness impairments
short/stiff:
- gastroc
- hamstrings
not stiff:
- glutes
- quads: strong w/ MMT, not poor functional use
patella lateral glide syndrome
impaired patellar relationship in femoral groove
- imbalance between VMO and vastus lateralis
- movie goer syndrome: pain w/ prolonged knee flexion w/ sitting
- secondary diagnosis w/ tibiofemoral ROT or hyperext
- PFPS
- patellar lateral tilt or glide
patella lateral glide stiffness impairments
short/stiff:
- TFL
not stiff:
- VMO: impossible to measure
- glute med
- hip ER
pronation syndrome stiffness impairments
short/stiff:
- gastroc/soleus leading to impaired ankle DF
- FHL limiting 1st MTP ext
not stiff:
- ankle PF: poor recruitment leads to pronation post MSt
- hip ER: IR of femur can lead to pronation
- foot intrinsics: cannot maintain arch during WB activity
- limited talocrural DF
supination syndrome
rigid foot with little ability to absorb shock
- absence of pronation in initial stance phase
- whip to medial side of foot in push off
- limited talocrural DF and MTP motion
- pain in late stance due to eccentric loading at achilles tendon
- pain at fibular mm during WB activities as mm works to eccentrically control supination
what muscles pronate the foot
none
- gravity is pronator, most of muscles of the foot act as supinators and eccentrically control pronation
fibularis longus closed chain action
pulls 1st MTP down to the ground
windlass effect
from MSt to TSt full body weight transfers to MTP heads
- MTP extends, plantar tissues tighten, arch elevates
- navicular moves dorsally, causing PF of first ray
- with 1st MTP passive ext there should be arch elevation
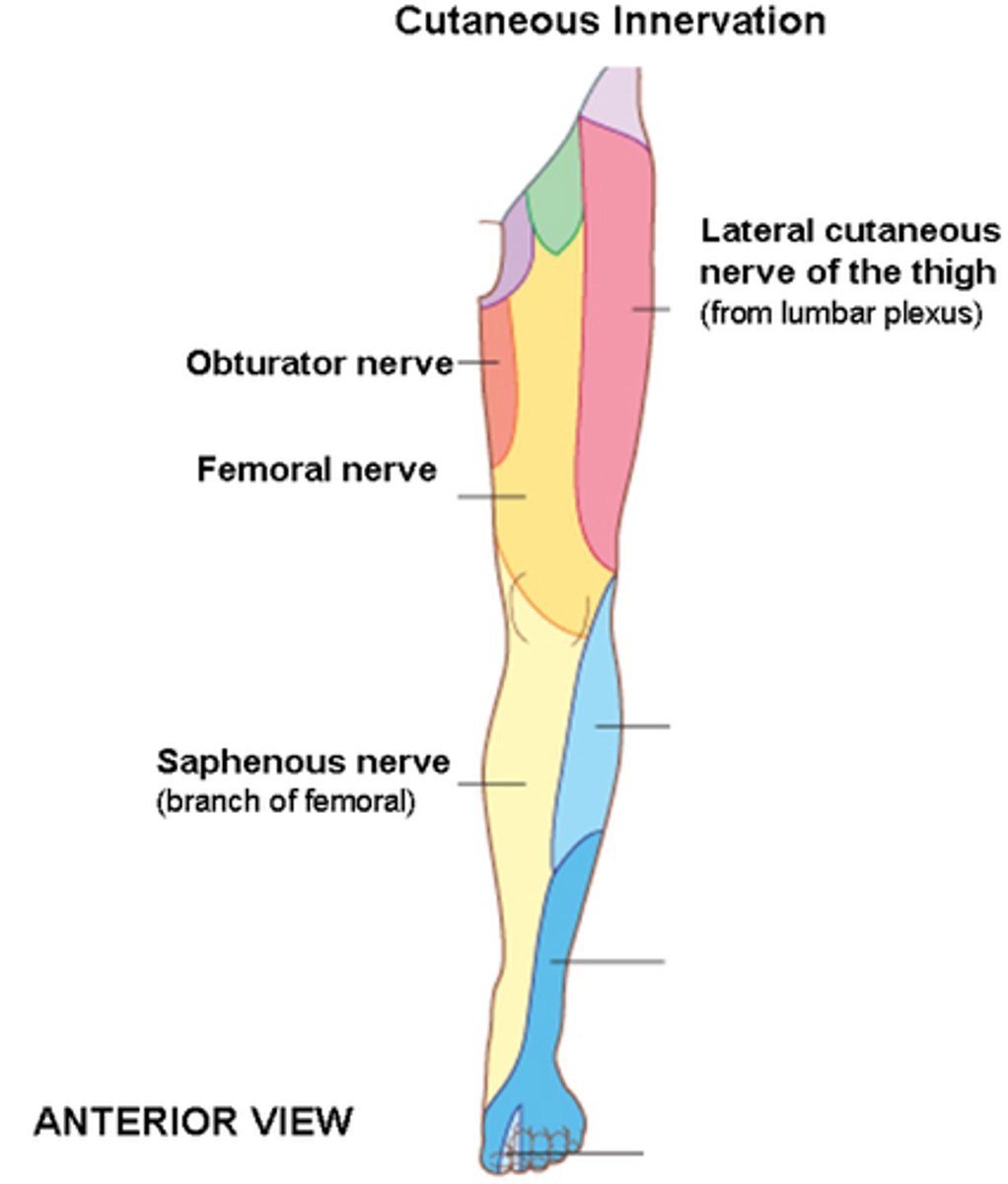
lower extremity cutaneous map
rearfoot varus
calcaneal inversion in subtalar neutral
- uncompensated: lateral heel contact, limited eversion and pronation in gait
- compensated: bring medial side of foot to the ground, stressing posterior tibialis as it tries to control pronation
- associated with genu valgum
forefoot varus
medial side of forefoot higher than lateral
- most common intrinsic cause of mechanical pain/dysfunction in the foot
- compensated: increase force laterally at 4/5th met heads
- uncompensated: excessive pronation of subtalar J to help medial foot hit the ground, keeps pronation throughout stance phase
effect of compensated forefoot varus
- foot mm fire out of sync, midtarsal joints hypermobile
- abnormal stress on peroneus longus and forefoot
- dorsiflexed, hypermobile first ray
- first ray cannot contribute to propulsion, 2nd and 3rd met heads get excessive loading
compensated forefoot valgus
- excessive and rapid supination of subtalar joint
- abnormal supination cannot adapt to uneven surfaces, increasing risk of inversion sprains
- poor shock absorption at IC and necessary tibia IR for knee flexion compromised, leading to other problems