Infancy: Physical
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
71 Terms
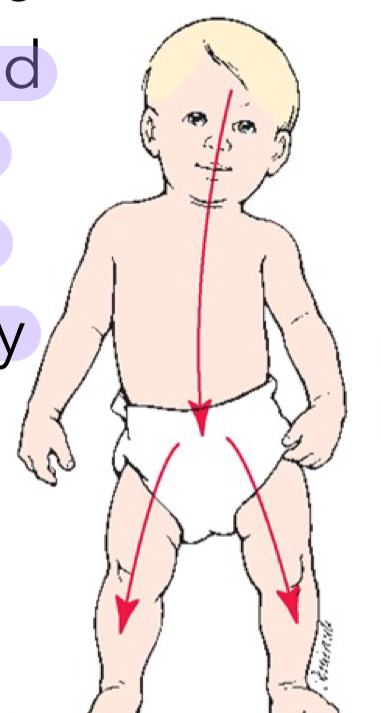
Cephalocaudal Development
Growth proceeds from the head downward
the head and upper regions of the body develop before the lower regions of the body
the brain development leads to development of other things
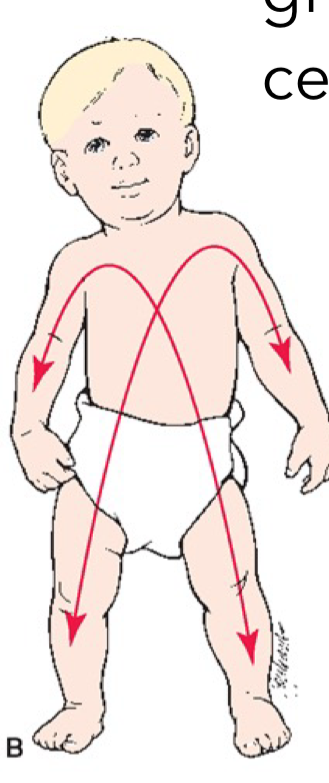
Proximodistal Development
Growth proceeds from the centre of the body outward
limbs catch up with head/torso
Synaptic Development
all brain structures are composed of two basic cell types: neurons and glial cells
millions of these cells are present at birth
synapses: connections between neurons, begin to form prenatally
two development processes: synaptogenesis, synaptic pruning
Neurons
nerve cells that store and transmit information from neuron to neuron
important for communication
responsible for what our bodies do
the first neurons form early in prenatal development, in the embryo’s neural tube thru neurogenesis (i.e the production of new neurons)
folic acid helps close the neural tube
Brain Development in Infancy
newborn babies are about 1/4 of the weight of an adult brain
the neural networks of axons and dendrites are simple (immature) wtih few synapses
responsible for breathing, communicating for help
major growth occurs during early infancy
at birth, the midbrain and medulla are most fully developed, they are connected to the spinal cord
the cortex develops in the final months prior to birth and continues to mature for many years after birth
our life experiences influence the physical structure of our brains
Synaptogenesis
the creation of synapses
occurs rapidly in the cortex during the first few years after birth
quadrupling the overall weight of the brain by age 4
occurs in spurts, instead of smooth and continuous
peaks in different brain regions at different ages
Synaptic Pruning
each synaptic growth spurt generates more connection between neurons than the individual actually needs
each burst of synaptogenesis is followed a period of pruning in which unnecessary pathways and connections are eliminated
Synaptogenesis/Pruning Cycle
continues thru the lifespan
with each cycle, the brain becomes more efficient
1-year olds have denser dendrites and synapses than an adult, but their network operates les efficiently than the adults
because infants have more unused synapses, they can bounce back from a host of insults to the brain (eg. malnutrition, head injury) more easily than adults
plasticity
Plasticity
the brain’s ability to change in response to experience
the period of greatest plasticity is also the period in which the child is most vulnerable to major deficits
Implications of Synaptic Development
changes in an infant’s behavior suggest they are engaging with the world in ways they did not before result from changes in the brain at the synapatic level
a child growing up in a rich or intellectually challenging environment will retain a more complex network of synapses than one growing up with fewer forms of stimulation
infant brains possess greater plasiticity
a young infant needs sufficient stimulation and order in their environment to maximize the early period of rapid growth and plasiticity
an inadequate diet or serious lack of stimulation in the early months may have subtle but long range effects on the child’s later cognitive progress
Myelination
process of neurons being coated in a fatty substance (myelin) to speed up neural communication and transmission of info
contributes to the numerous changes we see in children’s capacities
the sequence of myelinization follows both cephalocaudal and proximodistal patterns
eg. nerves serving muscle cells in the neck and shoulders are myelinized earlier than those serving the abdomen.
most rapid during the first 2 years after birth, but continues at a slower pace throughout childhood and adolescence
Experience-Expectant Brain Development
dependent on basic environmental experiences, such as visual and auditory stimulation, in order to develop normally
eg. lights on vs off, carpet vs hard ground
Experience-Dependent Brain Development
brain development that occurs in response to specific learning experiences
eg. exposure to many languages, raised in farm vs city
Reflexes
involuntary and automatic response to stimuli to help them survive
newborns respond to certain stimuli thru reflexes
some reflexes last throughout life whereas others disappear
Reflexes: Adaptive and Primitive
adaptive reflexes: lifelong, voluntary, and purposeful responses that allow us to adjust to our environment (eg. blinking, yawning)
some disappear in infancy or childhood, but others protect us over the whole lifespan
weak or absent adaptive reflexes in newborns suggest that the brain is not functioning properly
primitive reflexes: involuntary, automatic movements present in newborns that aid survival
controlled by less sophisticated parts of the brain (the medulla and midbrain)
by 6-8 months, primitive reflexes begin to disappear, if such reflexes persist past this age, the baby may have some kind of neurological problem
Sleep and Wakefulness
newborns sleep ~80% of each day, as much in the daytime as at night
by eight weeks infants sleep less and may differentiate between day time and night time
crying is communication: they develop different cries (hunger, dirty diaper, etc.)
most infants stop crying when picked up, held and talking/sung to
essentially when in motion, b/c they are constantly in motion due to amniotic fluid
Sleep Patterns
infants’ sleep patterns change over the first few months as the neurological systems that synchronize their bodily function with the circadian rhythms outside the womb mature
the light/dark cycle of the world
by 8 weeks of age, the total amount of sleep per day has dropped and signs of day/night sleep rhythms become evident
babies of this age begin to sleep thru two or three 2-hour cycles in sequences without coming to full wakefulness
thus are often said to “sleep thru the night”
by 6 months, babies still sleep over 14 hours per day, but sleep is more regular and predictable (clear nighttime sleep patterns and predictable nap times)
cultural beliefs play an important role in parent’s responses to infants’ sleep patterns (eg. choosing to intervene with crying during the night or not)
Crying Patterns
infants have different cries for pain, anger and hunger
Basic cry: often signals hunger, has a rhythmical pattern (cry, silence, breath, repeat) with a whistling sound accompanying the in-breath
Anger cry: louder and more intense
Pain cry: very abrupt onset (other 2 cries begin with whimpering/moaning)
crying increases in frequency over the first 6 weeks and then tapers off
Colic
15-20% of infants develop colic
pattern involving intense bouts of crying totaling 3 or more hours a day, for no apparent reason such as hunger or a wet diaper
to be diagnosed w/ colic, an infant must have manifested symptoms for at least 3 weeks
psychologists or physicians don’t know why colic begins or why it stops without any intervension
Wakefulness Patterns
on average, neonates are awake and alert for 2-3 hours each day
this time is unevenly distributed over a 24 hour period
over the first 6 months, advances in neurological development enable infants to remain awake and alert for longer periods of time, as their patterns of sleeping, crying and eating become more regular
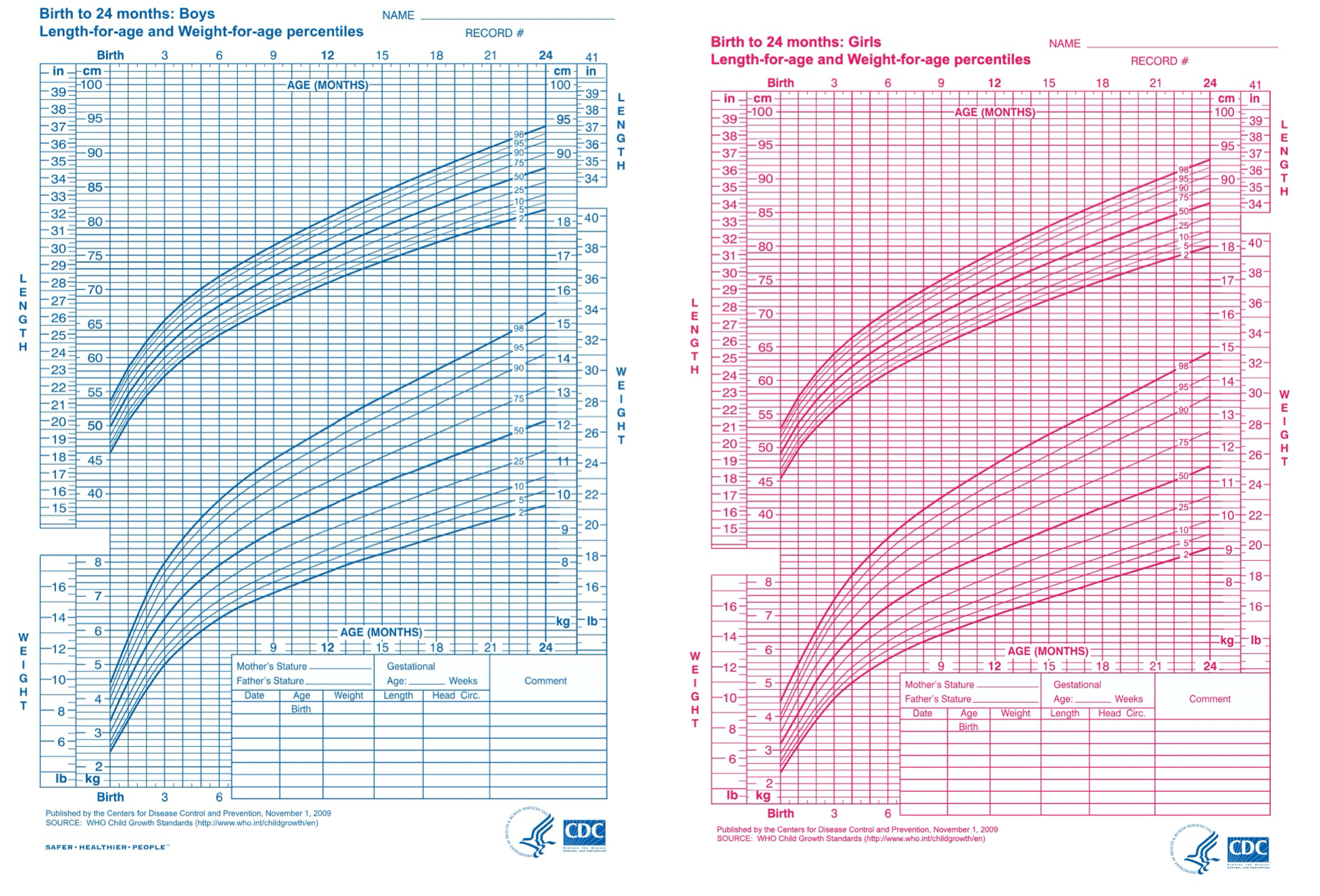
Growth Norms
Expectations for typical gains and variations in height and weight based on chronological age, biological sex and potentially whether breastfed or formula fed
is infant growing faster/slower in comparison to age norms?
trouble is there’s a drop in percentile in comparison to the growth curve
growth curves are specific to the individual
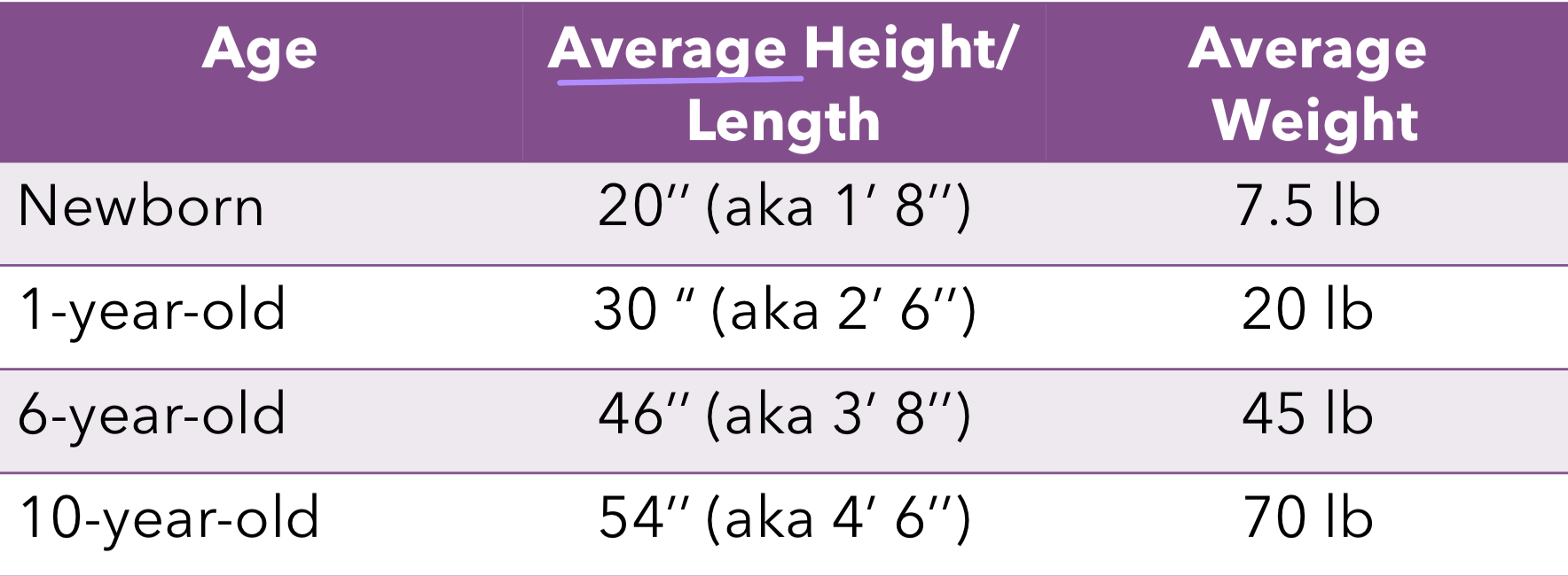
Growth during Infancy and Toddlerhood
“average” applies to full gestation only
the most amount of growth in life for weight and height occurs in the first 2 years
by 2, toddlers are half as tall as they will be as adults
it’s ok to sometimes lose weight b/c the babies need to learn how to eat and digest food
also possible if the mom was given IV fluids during birth
despite gender differences in physical development rate, the sequence of motor skill development is the same for all children, even those with physical or mental disabilities
Head Circumference
often indicates brain growth
there are 4 plates that are not fused
allows for compression during birth
lead to soft spots and dents can indicate dehydration
Genes and Hormones
genes influence the rate of growth by stipulating the amount of hormones to be released
hormones are chemicals produced and secreted into the bloodstream to affect and influence physiological functions
Developmental Milestones
almost universal, age-related events (physical, cognitive, socio-emotional) that mark major developmental changes
Growth Motor Development
development of the ability to control large movements of the body
eg. sitting, standing, crawling
once babies can walk, their entire visual field changes which influences cognitive and socio-emotional development, and how they interact with the world
Fine Motor Development
tiny manipulations of fingers/hands
voluntarily reaching is important for cognitive development
infants’ attention moves away from the motor skill, to the object, as well as the events that occur before and after acquiring the object
Dynamic Systems
Motor skills result from ongoing interactions among physical, cognitive and socioemotional influences and environmental supports…
in which previously mastered skills are combined to provide more complex and effective ways of exploring and controlling the environment
environmental supports: what are they exposed to? caregiver response?
Dynamic Systems Theory
the inborn timetable for motor skills development interacts with other aspects for physical development
the notion that several factors interact to influence development
all movement requires coordination of our senses and cognitive abilities to plan and predict actions (learn cause and effect)
motor development reflects goal-oriented behavior
differences in caregiver interactions and caregiver environments affect children’s motor skills
infants attain the same motor tasks at about the same age, yet differ in how they approach the tasks (eg. types of crawling styles)
individual differences can be accounted for by the dynamic systems perspective
Motor Development: Experience
experience influences motor development
opportunities to practice motor skills is important for young children who have disorders that impair motor functioning
eg. babies placed on their backs in cribs learned to walk later than babies in less restrictive settings
Motor Development: Culture
traditional cultural practices intentionally and coincidentally promote motor development
eg. African mothers who vigorously massage their babies muscles to mimic motor actions like walking)
Bone Development
wrist development is critical to the development of fine motor skills
at birth, the wrist contains a single mass of cartilage which develops into 9 separate bones over several years
ossification: process of bone hardening
begin in the last weeks of prenatal development and continue thru puberty
bones in different parts of the body harden in a sequence that follows the typical proximodistal and cepalocaudal patterns
motor development depends to a large extent on ossification
Muscle Development
a newborns’s muscle contain a high proportion of fat
by age 1, the water content of an infant’s muscles is equal to that of an adult’s, and the ratio of fat to muscle tissue has begun to decline
changes in muscle composition lead to increases in strength that enable 1-year olds to walk, run, jump, climb
Lungs and Heart
lungs grow rapidly and become more efficient during the first 2 weeks
improvements in lung efficiency, together with the increasing strength of heart muscles, give a 2-year old greater stamina than a new born
consequently, by the end of infancy, children are capable of engaging in long periods of sustained motor activity without rest (exhausting their parents)
Infant Health: Breastmilk
breastmilk provides newborns and infants with everything they need for the first 6 months of life
breastmilk is tailored to infants and has the right amount of fat, sugar, water and protein needed for the baby’s growth and development (no ned to alter the size of serving)
contains bioactive components (e.g. immunizing agents that protect from infections)
breastmilk is substantially superior nutritionally to formula feeding
Benefits of Breastfeeding
Growth: breast milk contributes to more rapid weight and size gain
Health: breastfed infants are less likely to suffer from problems, such as diarrhea, ear infection
Preterm babies: their intestinal tracts are not as mature as those of full-term infants, and they require special formulas that contain amino acids and fats that full-term babies can manufacture on their own
physicians recommend feeding preterm babies expressed breast milk that has been fortified with fats, proteins, vitamins and minerals their bodies need
Alternatives to Breastfeeding
sometimes is impossible, like if drugs are present in the breast milk whether from substance abuse or medications. These drugs would negatively impact infant development
doctors recommend avoiding breastfeeding here
these babies are fed high-quality infant formula, prepared according to the manufacturer’s instructions and properly sterilized
Infant Health: Nutrition
up until 4-6 months, babies only breast milk or formula accompanied by appropriate supplements
doctors may recommend supplemental formula
pediatricians usually recommend withholding solid foods until a baby is at least 6 months old
parents should introduce a baby to no more than one new food each week, allowing them to identify food allergies
infants do not necessarily like new flavors and textures and therefore foods need to be introduced numerous times
Infant Health: Appetite
appetite is lower compared to infancy
meals may take longer, and self-feeding can mean eating less
appetites continue to decrease ages 2-6
some go thru picky eating ~ age 3
Malnutrition
can seriously impair a baby’s brain because the nervous system is the most rapidly developing body system during the first 2 years of life
although malnutrition is common is developing countries, it is also found in some of the wealthiest countires
in Canada, 1 in 8 households was food insecure
each type of malnutrition has unique effects on development
Macronutrient Malnutrition
results from a diet that contains too few calories
world’s leading cause of death among children under age 5
Marasmus
when the calorie deficit is severe, marasmus (a disease) results
infants weigh less than 60% of what they should at their age, and many suffer permanent neurological damage from the disease
suffer from parasitic infections that lead to chronic diarrhea
makes it difficult to treat marasmus by simply increasing an infant’s intake of calories
a program of dietary supplementation with formula combined with intravenous feedings and treatment for parasites can reverse marasmus
Kwashiokor
some infants’ diets contain almost enough calories, but not enough proteins
also seen in children who are chronically ill because of their bodies’ inability to use the protein from the foods they eat
can lead to variety of health problems as well as permanent brain damage
Micronutrient Malnutrition
a deficiency of certain vitamins and/or minerals
eg. infants who are still getting most of their calories from milk after the age of 12 months frequently develop iron-deficiency anemia
common among low-income families, but also children of all economic levels
Infant Health Care
routine appointments:
check ins
screening: pre-assessment before a real assessment is needed
referrals: meet with specializations
immunization: protects against a variety of disease
is most effective when it beings the first month of life and continues through childhood and adolescence
even adults need occasional “booster shots” to maintain immunity
the more people a baby is exposed to, the more often they’re likely to be sick
Adjusted Age
allows premature babies to catch up on development
assess development by backtracking
eg. a baby that is 5 weeks early is assessed by backtracking 5 weeks
Respiratory/Ear Infections
the average baby has 7 respiratory illnesses in the first year of life
babies in daycare centers have 2x as many infections
the timing of respiratory illnesses can lead to ear infections
those who have chronic ear infections are more likely to have learning disabilities, attention disorders and language deficits during school years
because ear infections temporarily impair hearing, they may compromise brain development areas essential for language learning during the first 2 years of life
Hearing Development
capacity to hear develops prenatally
hearing is the most well-developed sense at birth as newborns are able to hear about as well as adults
through listening, the process of learning language begins at birth
able to determine location of sounds, by turning their head roughly in the right direction
limited in hearing high-pitched sounds, as it needs to be louder in order to be heard
Sensation and Perceptual Development
Sensation: occurs when our senses detect a stimulus
Perception: the sense our brain makes of the stimulus and our awareness of it
actively paying attention to stimuli
Vision Development
the least developed of all senses at birth, but improves rapidly
since we don’t need to see anything in utero
the way infants explore visual stimuli changes with age
outer perimeter vs centre of objects
can pick up on contrasts of color and distance
preference to see human faces
adults are naturally driven to capture infants’ attention (eg. going closer to their face, dancing)
newborns are pretty nearsighted and can focus well at about 8-10 inches, the distance between a parent’s face and baby’s eyes when feeding
Vision Development: Visual Tracking
the ability to follow an object’s movement with the eyes
limited at first, but improves quickly
because newborns can’t move independently yet, a lot of their experiences with objects are with things that move toward or away from them
if the baby wants to successfully recognize objects, they have to be able to keep their eyes on the objects as the move
Vision Development: Depth Perception
the ability to perceive the distance of objects from each other and from ourselves
we must learn about depth thru experience, which is why toddlers are accident prone (eg. crawling off the bed)
Visual Acuity
aka 20/20 vision: you can see and identify something 20 feet away that the average person can also see at 20 feet
the higher the second number, the poorer the person’ s visual acuity
at birth, the infant’s acuity is in the range of 20/200 - 20/400, but improves rapidly during the first year as a result of synaptogenesis, pruning and myelination
most babies reach 20/20 vision by 6 months
it’s difficult to test an infant’s true visual acuity because children can’t be tested with conventional eye exams until they are old enough to respond verbally to the examiner
Depth Perception: Binocular and Monocular Cues
Binocular: involve both eyes, each of which receives a slightly different visual image of an object; the closer the object is, the more different the two views are
Monocular: requires input from only one eye
Kinetic Cues
come from either your own motion or the motion of some object
infants use kinetic cues first, then binocular, then monocular
Color Vision
the eye cells necessary for perceiving red, green and blue are present by 1 month, and perhaps present at birth
infants’ ability to sense color, even in the earliest weeks of life is almost identical to that of adults
Smell and Taste Devlopment
smell and taste are well developed at birth
within a day of birth, newborns can detect and recognize their mother’s odour (postpartum smell that helps the infant determine who mom is)
infants show an innate preference for certain tastes
eg. sugary, and breastmilk is naturally sweet
Touch
the mouth is the first part of the body to show sensitivity to touch prenatally and remains one of the most sensitive areas to touch after birth
eg. rooting reflex when cheek/mouth is touched
babies are sensitive to touches on mouth, face, hands, soles of feet, and abdomen
Intermodal Perception
our interactions with the environment combine information from various sensory systems
Intermodal perception: the process of combining information from more than one sensory system
Infant Mortality
death within the first year after birth; almost 2/3 of these infant deaths occur in the first month of life and are directly linked to either congenital anomalies or low birth weight
Sudden Infant Death Syndrome (SIDS)
an apparently healthy infant dies suddenly and unexpectedly
risk factors: season, apnea, prenatal smoking, delayed myelination
deaths attributable to SIDS vary widely across ethnic groups
some groups are more likely to suffer from congenital abnormalities and low birth weight
SIDS: Season
much more in the winter, when babies may be suffering from viral infections that cause breathing difficulties
SIDS: Apnea
apnea: brief periods when breathing suddenly stops
babies with a history of apnea are at an increased risk of dying from SIDS
episodes of apnea may be noticed by medical personnel in the newborn nursery, or a nonbreathing baby may be discovered by parents in time to be resuscitated
physicians recommend usually recommend using electronic breathing monitors that will sound an alarm if the baby stops breathing again while asseep
SIDS: Prenatal Smoking
smoking by the mother during pregnancy or by anyone in the home after the child’s birth
babies exposed to smoke are 4x likely to die of SIDS
SIDS: Delayed Myelination
babies are at a higher risk of SIDS when their myelination progresses at a slower rate than others
babies’ sleep patterns reflect these neurological differences and also predict SIDS risk
infants who show increasingly lengthy sleep periods during the early months are at lower risk of SIDS than those whose sleep periods do not get much longer as they get older
autopsies of babies who have died from SIDS have revealed that their brains often show signs of delayed myelination and deficiencies in the neurotransmitter serotonin
SIDS: Prevention
most frequent among babies who sleep on their stomachs or sides, especially on a soft or fluffy mattress, pillow or comofrter
healthy infants are to be positioned on their backs to sleep
Preference Technique
babies are shown 2 pictures and researcher keeps track of how long the baby looks at each one
if many infants shown the same pair of pictures consistently look longer at one picture than the other, this tells us that babies seem some difference b/w the 2, and about what kinds of objects/pictures that capture their attention
Habituation
habituation: getting used to a stimulus
dishabituation: responding to a somewhat familiar stimulus as if it were new
Researchers first present the baby with a stimuli over and over until they habituate
Then the researchers present another stimuli that is slightly different from the original and watch to see whether the baby shows renewed interest
if the baby shows renewed interest, you know they perceive the new stimuli as different from the original
Discriminating b/w Similar Speech Sounds
as early as 1 month, babies can discriminate between similar speech sounds like pa and ba
they can also rapidly learn to discriminate between words and nonwords in artificial languages
Perception of language-specific speech sounds
each language uses only a subset of all possible speech sounds
up to about 6 months of age, babies can accurately discriminate all sound contrasts that appear in any language, including sounds they do not head in the language spoken to them
by age 1, the ability to discriminate nonheard consonant constrasts begin to fate
Recognition of Voices
newborn can tell the mother’s voice from another female, but not the father’s voice from another male voice
they prefer the mother’s voice
premature infants are less likely to recognize their mother’s voice than are full-term babies
in utero, learning appears to be responsible for newborns’ preference for the maternal voice