week 37 - hernias and groin problems
0.0(0)
Studied by 2 peopleCard Sorting
1/47
There's no tags or description
Looks like no tags are added yet.
Last updated 4:05 PM on 7/8/26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
1
New cards
Most common cause of lumps in the groin =
Hernias, mainly inguinal but also femoral → both are caused by abdominal contents protruding through an abdominal wall defect
Other causes → enlarged lymph nodes (due to infection or malignancy), vascular abnormalities (eg. Saphena varia or a femoral artery aneurysm) and a psaos abscess (not very common nowadays, used to be a common complication of spinal tuberculosis but is now more often a result of infection tracking down from a perforation in the left colon)
Other causes → enlarged lymph nodes (due to infection or malignancy), vascular abnormalities (eg. Saphena varia or a femoral artery aneurysm) and a psaos abscess (not very common nowadays, used to be a common complication of spinal tuberculosis but is now more often a result of infection tracking down from a perforation in the left colon)
2
New cards
Inguinal hernias are much more common in… because…
Males because the testicles descend from the abdomen to the scrotum via the inguinal canal and this area remains vulnerable throughout life
Inguinal hernias in females are due to a problem in the uterine round ligament (amongst other problems i think)
Inguinal hernias in females are due to a problem in the uterine round ligament (amongst other problems i think)
3
New cards
Femoral hernias are more common in…
Females
The femoral canal is below the inguinal ligament and it is also a weak spot
The femoral canal is below the inguinal ligament and it is also a weak spot
4
New cards
Examining a lump in the groin
1. Patient must be examined both standing and lying
* standing → increases intra abdominal pressure → makes hernias more visible
* Ask the patient to cough while palpating the lump → the intra abdominal pressure is transmitted through the abdominal wall and an expansive ==__cough impulse__== is felt in a hernia (except if femoral)
* ==__Small hernias may reduce on laying down and a scrotal varicocele will empty__==
2. Examine the consistency and reducibility
* hernias are usually soft and squishy but the most reliable sign is if a lump reduces when the patient lies flat or can be reduced by gentle manipulation
* Most inguinal hernias are at least partly reducible
* but long standing hernias gradually become irreducible because of adhesions within the sac = ==__incarcerated hernias__== = chronically irreducible
* Femoral hernias are nearly always irreducible and have no cough impulse since the femoral canal is so narrow
* A strangulated inguinal hernia is irreducible, tender and often red but strangulated femoral hernias are usually very small and unimpressive but they have serious consequences
* Strangulated hernias (especially femoral) sometimes present with abdominal pain or signs of obstruction but without localised pain in the groin
* enlarged inguinal lymph nodes vary in consistency number and size depending on the pathological cause, NOT reducible
* a saphena varix is very soft and disappears completelt on palpation or if the patient lies down → refills when pressure is released or if the patient stands
the leg on that side almost always has varicose veins
* femoral artery aneurysms are firm but pulsatile
3. find the relationship of the lump to the inguinal ligament
* the inguinal ligament is not visible but it stretches between 2 palpable bony prominences = the anterior superior iliac spine laterally and the pubic tubercle medially (lies 2-3 cm above the groin crease, best found by palpating along the upper border of the pubic symphysis outwards from the midline)
* inguinal hernias always originate ==__above__== the inguinal ligament while femoral hernias, saphena varices and femoral artery aneurysms always arise ==__below__== it
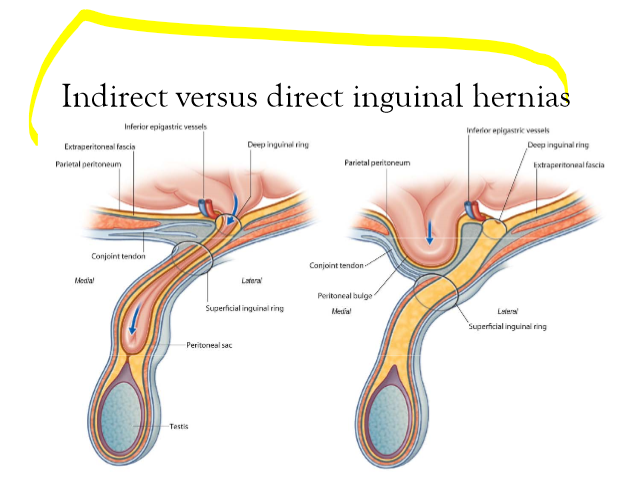
4. distinguish between direct and indirect inguinal hernias
* indirect = where the hernial sac lies within the spermatic cord, leaving the abdomen via the deep (==__internal__==) inguinal ring to pass along the inguinal canal. exiting through the superficial (==__external__==) ring
* if the hernia can be completely reduced, finger pressure over the deep ring will prevent it reappearing on coughing
* direct = leaves the abdomen through a weakness or split in the ==__transversalis fascia (the posterior wall of the inguinal canal)__== → emerges directly through the superficial ring
* cannot be controlled by digital pressure over the deep ring
* however, this test is difficult and often unreliable but, the patients age is perhaps the most useful indicator of the likely type of inguinal hernia → indirect hernias most frequent <50 y/o and direct hernias more common after that age
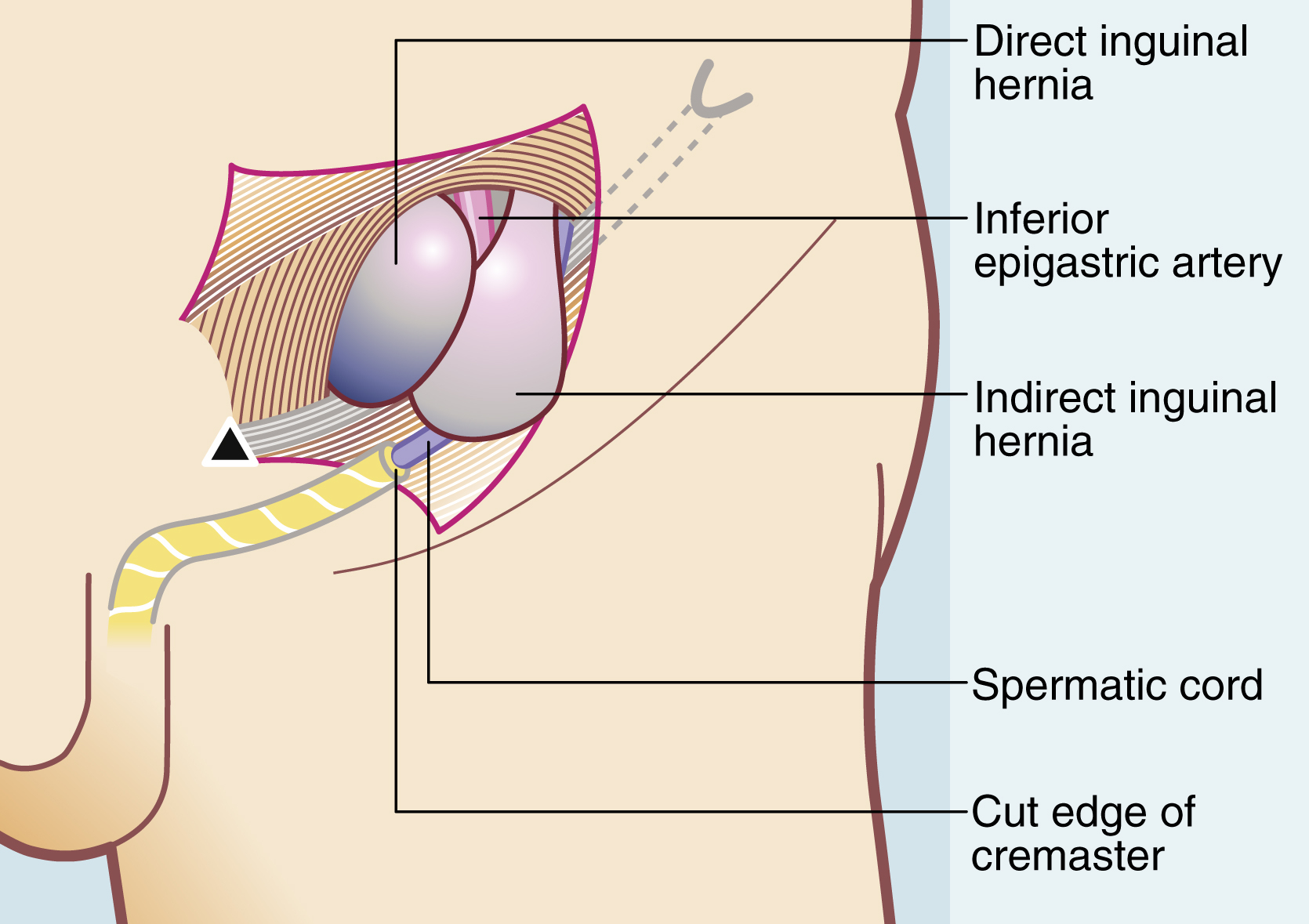
* ==__*at operation, its relationship to the inferior epigastric artery defines whether an inguinal hernia is direct or indirect*__==
5. differentiate between inguinal and femoral hernias
* difficult but the key is the position of the hernia in relation to the inguinal ligament = point 3
* an inguinal hernia, emerging from the superficial ring, has its origin above the inguinal ligament, often descending over or medial to the pubic tubercle
* a femoral hernia originates below the inguinal ligament and lies lateral to the pubic tubercle
5
New cards
indirect vs direct inguinal hernias
6
New cards
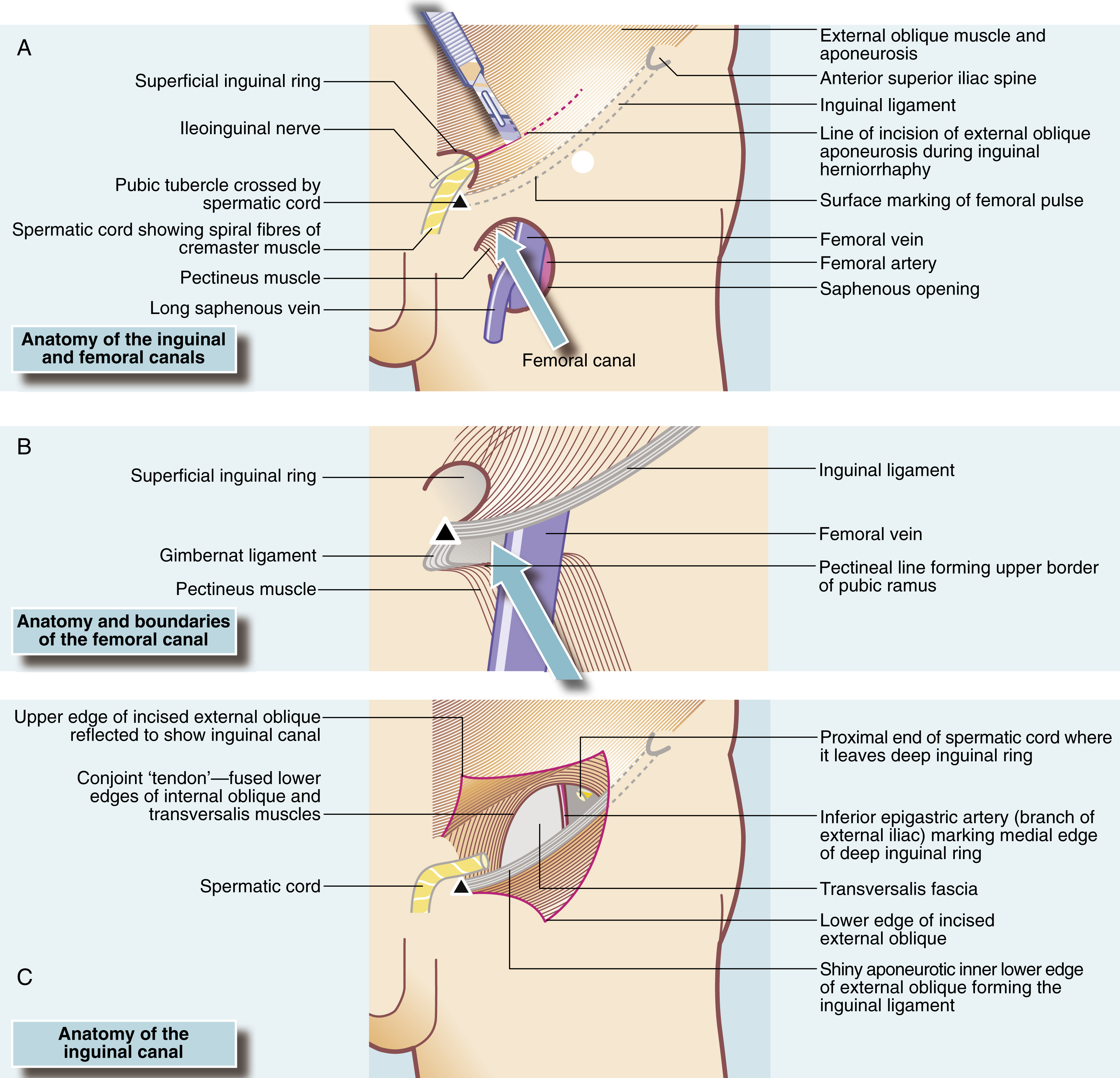
structure of the inguinal and femoral canals
7
New cards
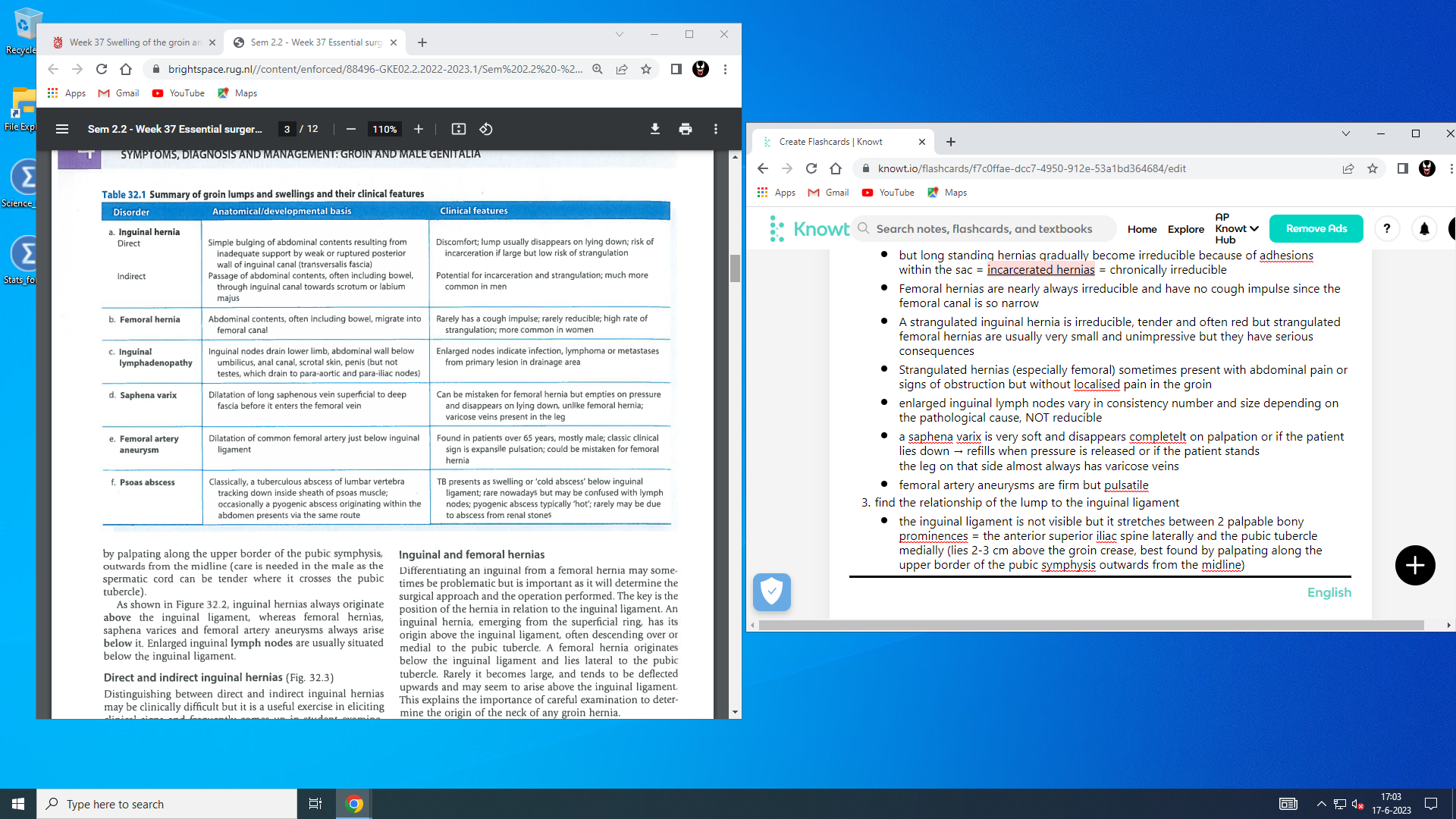
summary of groin lumps and swellings + clinical features
8
New cards
inguinal hernia
* one of the most common conditions seen in general surgical clinics, account for around 7% of surgical outpatient consultations and about 12% of operating theatre time
* inguinal hernias in males are by far the most common type of groin hernia
more common in males (8:1 male to female) due to abdominal wall deficiency caused by testicular descent
* femoral hernias are rare in males (compromise 2.5% of groin hernias) but even in females, inguinal hernias are more common (2:1 inguinal to femoral)
* occur at any age
* have a developmental origin in children and are common in premature infants
* in males, hernias appear most often <5 y/o or after middle age, a smaller peak occurs in the late teens and early 20s
in young men it is probably due to a congenital predisposition exacerbated by work or sport
* most inguinal hernias should be repaired early to reduce the long term risk of strangulation and emergency operation
watchful waiting is ok in easily reducible painless direct hernias in elderly men or those with substantial comorbidity
* = the herniated abdominal contents are contained within a sac of peritoneum
* in indirect hernias, the peritoneal sac may represent a ==__patent or reopened processus vaginalis__== and may extend as far as the ==__tunica vaginalis__== and surround the testis
* direct hernias tend to bulge forwards and rarely enter the scrotum
→ usually found in older patients with deficient muscles and weak transversalis fascia
→ may occur suddenly after physical strain (==__in this case, the transversalis fascia has split__==)
* direct = broad neck, indirect = narrow neck (due to being confined by the borders of the deep ring → also makes them more liable to strangulate)
* indirect and direct hernias can occur together on the same side = pantaloon hernia
* a hernia may consist merely of peritoneum and associated extraperitoneal fat, but if larger, the sac usually contains omentum or small bowel, or less commonly large bowel or appendix
may be diseased (eg. carcinoma, inflamed appendix etc)
* sometimes, a retroperitoneal viscus ‘slides’ down the posterior abdominal wall and herniates directly (occasionally indirectly) into the inguinal canal, dragging its overlying peritoneum with it
→ visceral contents of a **sliding hernia** lie behind and outside the peritoneal sac
→ most commonly occurs in the left groin involving the descending and sigmoid colon or in larger direct hernias, may involve the bladder
==__**doesnt make sense**__==
* spigelian hernia??????????????:
*Rarely, herniation occurs through a fascial defect in the linea semilunaris at the lateral border of rectus abdominis. The hernial sac comes to lie interstitially, that is, between the layers of internal and external oblique or transversus abdominis. This is a* ***Spigelian hernia*** *. It has some clinical characteristics of an inguinal hernia, but the bulge lies higher than an inguinal hernia and may be difficult to palpate, because it is covered by one or more layers of the abdominal wall*
\
* typically develop slowly but are exacerbated by any condition which persistently raised intra abdominal pressure (eg. obesity. constipation, straining at mictruition or chronic coughing etc)
* in infants, a period of severe coughing or crying may precipitate an acute indirect hernia, which may become irreducible
* lifetime risk of inguinal hernia is high (>1 in 4 men; >1 in 30 women)
* men account for around 90% of all inguinal hernia repairs
* *inguinal hernias have a bimodal distribution, with peaks aged 1 year (indirect) and in those aged 70 to 80 years (direct)*
* women with affected first degree relatives are at much higher risk of developing an inguinal hernia
* incarcerated = chronically irreducible hernia that is not strangulated (always assume a hernia is strangulated until proven otherwise)
* difficult to reduce or intermittently causing pain inguinal hernias are at a particular risk of strangulation
→ obstruction of venous return then leads to swelling and later to arterial obstruction
→ if strangulation is not relieved by manual or operative reduction → infarction
* ==__***some hernias become intermittently irreducible, often with local pain and tenderness or even symptoms of bowel obstruction (vomiting, colicky abdominal pain, distension and absolute constipation)***__==
* inguinal hernias in males are by far the most common type of groin hernia
more common in males (8:1 male to female) due to abdominal wall deficiency caused by testicular descent
* femoral hernias are rare in males (compromise 2.5% of groin hernias) but even in females, inguinal hernias are more common (2:1 inguinal to femoral)
* occur at any age
* have a developmental origin in children and are common in premature infants
* in males, hernias appear most often <5 y/o or after middle age, a smaller peak occurs in the late teens and early 20s
in young men it is probably due to a congenital predisposition exacerbated by work or sport
* most inguinal hernias should be repaired early to reduce the long term risk of strangulation and emergency operation
watchful waiting is ok in easily reducible painless direct hernias in elderly men or those with substantial comorbidity
* = the herniated abdominal contents are contained within a sac of peritoneum
* in indirect hernias, the peritoneal sac may represent a ==__patent or reopened processus vaginalis__== and may extend as far as the ==__tunica vaginalis__== and surround the testis
* direct hernias tend to bulge forwards and rarely enter the scrotum
→ usually found in older patients with deficient muscles and weak transversalis fascia
→ may occur suddenly after physical strain (==__in this case, the transversalis fascia has split__==)
* direct = broad neck, indirect = narrow neck (due to being confined by the borders of the deep ring → also makes them more liable to strangulate)
* indirect and direct hernias can occur together on the same side = pantaloon hernia
* a hernia may consist merely of peritoneum and associated extraperitoneal fat, but if larger, the sac usually contains omentum or small bowel, or less commonly large bowel or appendix
may be diseased (eg. carcinoma, inflamed appendix etc)
* sometimes, a retroperitoneal viscus ‘slides’ down the posterior abdominal wall and herniates directly (occasionally indirectly) into the inguinal canal, dragging its overlying peritoneum with it
→ visceral contents of a **sliding hernia** lie behind and outside the peritoneal sac
→ most commonly occurs in the left groin involving the descending and sigmoid colon or in larger direct hernias, may involve the bladder
==__**doesnt make sense**__==
* spigelian hernia??????????????:
*Rarely, herniation occurs through a fascial defect in the linea semilunaris at the lateral border of rectus abdominis. The hernial sac comes to lie interstitially, that is, between the layers of internal and external oblique or transversus abdominis. This is a* ***Spigelian hernia*** *. It has some clinical characteristics of an inguinal hernia, but the bulge lies higher than an inguinal hernia and may be difficult to palpate, because it is covered by one or more layers of the abdominal wall*
\
* typically develop slowly but are exacerbated by any condition which persistently raised intra abdominal pressure (eg. obesity. constipation, straining at mictruition or chronic coughing etc)
* in infants, a period of severe coughing or crying may precipitate an acute indirect hernia, which may become irreducible
* lifetime risk of inguinal hernia is high (>1 in 4 men; >1 in 30 women)
* men account for around 90% of all inguinal hernia repairs
* *inguinal hernias have a bimodal distribution, with peaks aged 1 year (indirect) and in those aged 70 to 80 years (direct)*
* women with affected first degree relatives are at much higher risk of developing an inguinal hernia
* incarcerated = chronically irreducible hernia that is not strangulated (always assume a hernia is strangulated until proven otherwise)
* difficult to reduce or intermittently causing pain inguinal hernias are at a particular risk of strangulation
→ obstruction of venous return then leads to swelling and later to arterial obstruction
→ if strangulation is not relieved by manual or operative reduction → infarction
* ==__***some hernias become intermittently irreducible, often with local pain and tenderness or even symptoms of bowel obstruction (vomiting, colicky abdominal pain, distension and absolute constipation)***__==
9
New cards
when is an inguinal hernia particularly at risk of strangulation
when it is difficult to reduce or it intermittently causes pain
10
New cards
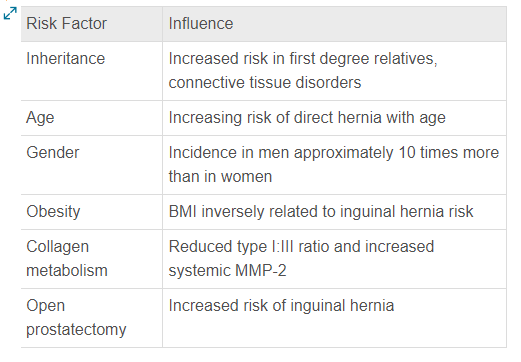
risk factors for developing inguinal hernias
11
New cards
a strangulated hernia first becomes… (+ following/future signs)
irreducible and then tender and later red
signs → symptoms and signs of bowel obstruction develop (due to the strangulation) over the next few hours, followed by peritonitis, if the bowel perforates
rigler sign???
signs → symptoms and signs of bowel obstruction develop (due to the strangulation) over the next few hours, followed by peritonitis, if the bowel perforates
rigler sign???
12
New cards
SLIDING HERNIAS?????
13
New cards
where are the internal oblique and transversus abdominis muscles deficient (only in hernias or generally???)
above the medial half of the inguinal ligament
14
New cards
direct vs indirect inguinal hernia
15
New cards
what does the spermatic cord pass through
the deep ring
16
New cards
how is the deep inguinal ring bounded\*\*\*
bounded by the inguinal ligament below, conjoint musculature above and laterally, and the inferior epigastric artery medially
17
New cards
management of inguinal hernias
* should ideally be repaired by herniorrhaphy or mesh patching in adults
* small reducible direct hernias in older men can safely be left alone
* direct hernias can be managed with an open McVay repair (approximation of the transversalis aponeurotic arch and internal oblique aponeurosis to the anterior ileopubic tract and shelving edge of the inguinal ligament), a Bassini approach, or with mesh
* some hernias become intermittently irreducible, often with local pain and tenderness or even symptoms of bowel obstruction (vomiting, colicky abdominal pain, distension and absolute constipation)
→ warning signs → indicate early operation
→ __more severe and prolonged symptoms of this nature precipitate emergency admission to hospital, in which case strangulation must be assumed and operation performed urgently, preferably within 4 hours to maximise the chance of saving ischaemic bowel__
* in any patient with an obstructed or strangulated hernia → first resuscitate (more patients die of fluid and electrolyte problems than of delaying an operation by a few hours)
\
1. inguinal herniorrhaphy and herniotomy:
* herniotomy → patent processus vaginalis is ligated and excised
→ done in infants, formal repair of the abdominal wall defect in unnecessary (why???)
* hernoirrhaphy → herniotomy + mesh implant to repair and reinforce the defect (rather than pulling together muscle and fascial layers together under tension) = lichtenstein type of inguinal hernia repair
→ mesh rarely causes infections
* adv:
* postoperative pain is less
* recurrence rate is low
* relatively cheap
* disadv:
* early complications → scrotal haematoma and wound infection
* late complications → recurrence (recur in 2-25% of cases over a lifetime), chronic groin pain (due to inadvertent trapping of the ilioinguinal or another nerve in the repair) and testicular atrophy (due to inadvertent damage to the testicular artery, usually with diathermy, or overtightening of the deep ring)
2. laparoscopic inguinal hernia repair:
* → through a transperitoneal or retroperitoneal route
* the standard operation for hernia repair in many centers
* less postoperative pain and a slightly quicker return to normal activities, but has a slightly higher risk of major complications and recurrences compared to open techniques for primary hernia repair
* strongly recommended as the technique of choice in ==__women__==, as it allows coverage of the whole myopectineal orifice, thus allowing repair of inguinal and femoral hernias simultaneously
* particularly recommended for repair of recurrent hernias
\
* *During the first postoperative week, patients should avoid activities likely to strain the repair, such as heavy lifting or driving a car. Over the next 2 or 3 weeks, they should gradually return to normal activity, including usual sexual activity. Time to return to work depends on the physical nature of the job and whether activities cause pain, but usually varies from 2 to 4 weeks*
* mesh repairs are proven to reduce recurrence rates compared to nonmesh, although the optimal mesh design remains unknown
there are absorb-able and non absorb-able types
* try to avoid the use of trusses
* small reducible direct hernias in older men can safely be left alone
* direct hernias can be managed with an open McVay repair (approximation of the transversalis aponeurotic arch and internal oblique aponeurosis to the anterior ileopubic tract and shelving edge of the inguinal ligament), a Bassini approach, or with mesh
* some hernias become intermittently irreducible, often with local pain and tenderness or even symptoms of bowel obstruction (vomiting, colicky abdominal pain, distension and absolute constipation)
→ warning signs → indicate early operation
→ __more severe and prolonged symptoms of this nature precipitate emergency admission to hospital, in which case strangulation must be assumed and operation performed urgently, preferably within 4 hours to maximise the chance of saving ischaemic bowel__
* in any patient with an obstructed or strangulated hernia → first resuscitate (more patients die of fluid and electrolyte problems than of delaying an operation by a few hours)
\
1. inguinal herniorrhaphy and herniotomy:
* herniotomy → patent processus vaginalis is ligated and excised
→ done in infants, formal repair of the abdominal wall defect in unnecessary (why???)
* hernoirrhaphy → herniotomy + mesh implant to repair and reinforce the defect (rather than pulling together muscle and fascial layers together under tension) = lichtenstein type of inguinal hernia repair
→ mesh rarely causes infections
* adv:
* postoperative pain is less
* recurrence rate is low
* relatively cheap
* disadv:
* early complications → scrotal haematoma and wound infection
* late complications → recurrence (recur in 2-25% of cases over a lifetime), chronic groin pain (due to inadvertent trapping of the ilioinguinal or another nerve in the repair) and testicular atrophy (due to inadvertent damage to the testicular artery, usually with diathermy, or overtightening of the deep ring)
2. laparoscopic inguinal hernia repair:
* → through a transperitoneal or retroperitoneal route
* the standard operation for hernia repair in many centers
* less postoperative pain and a slightly quicker return to normal activities, but has a slightly higher risk of major complications and recurrences compared to open techniques for primary hernia repair
* strongly recommended as the technique of choice in ==__women__==, as it allows coverage of the whole myopectineal orifice, thus allowing repair of inguinal and femoral hernias simultaneously
* particularly recommended for repair of recurrent hernias
\
* *During the first postoperative week, patients should avoid activities likely to strain the repair, such as heavy lifting or driving a car. Over the next 2 or 3 weeks, they should gradually return to normal activity, including usual sexual activity. Time to return to work depends on the physical nature of the job and whether activities cause pain, but usually varies from 2 to 4 weeks*
* mesh repairs are proven to reduce recurrence rates compared to nonmesh, although the optimal mesh design remains unknown
there are absorb-able and non absorb-able types
* try to avoid the use of trusses
18
New cards
wheelbarrow hernias\*\*\*
*Very large ‘wheelbarrow’ hernias are invariably of long standing and are found mainly in elderly men. They only present when size becomes a handicap, if bowel strangulates within the hernia or if the anatomical distortion interferes with micturition. Bowel adhesions may make operation difficult and postoperative wound infections are common. If the hernia is not strangulated, a bag truss to support the hernia may be an appropriate treatment*
19
New cards
causes of inguinal hernia recurrence\*\*\*
* Inappropriate technique—suture darn (Bassini) type repairs have a high recurrence rate.
* Operator inexperience—some techniques, especially laparoscopic repairs, have a long learning curve.
* Technical failure—failure to recognise and remove an indirect sac at operation; insufficient coverage of the defect; suture or mesh failure.
* Missed diagnosis of a concomitant femoral hernia.
* Inherently poor musculature or connective tissue, chronic cough, urinary obstruction, constipation or resumption of heavy work too soon after repair.
* Underlying physiological problems that impair healing, such as poorly controlled diabetes or smoking—smokers have twice the recurrence rates of nonsmokers. It is important to screen for problems of this type and address them before hernia surgery.
* Operator inexperience—some techniques, especially laparoscopic repairs, have a long learning curve.
* Technical failure—failure to recognise and remove an indirect sac at operation; insufficient coverage of the defect; suture or mesh failure.
* Missed diagnosis of a concomitant femoral hernia.
* Inherently poor musculature or connective tissue, chronic cough, urinary obstruction, constipation or resumption of heavy work too soon after repair.
* Underlying physiological problems that impair healing, such as poorly controlled diabetes or smoking—smokers have twice the recurrence rates of nonsmokers. It is important to screen for problems of this type and address them before hernia surgery.
20
New cards
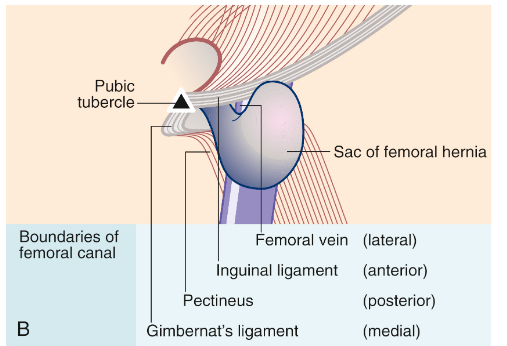
femoral hernias
* formed by a protrusion of peritoneum into the potential space of the femoral canal
* 40% present with strangulation
* incidence is higher in women and increases with age
→ increased intra-abdominal pressure, and other factors related to pregnancy, may be important in females, since the incidence of femoral hernia is higher in parous than nulliparous women
* clinical features:
* usually small, appearing as a lump immediately below the inguinal ligament and just lateral to its medial attachment to the pubic tubercle
* femoral canal is narrow so a cough impulse can rarely be detected
* the hernia is usually irreducible → small femoral hernias may be difficult to distinguish from other lumps arising in the femoral canal, such as a lipoma or enlarged Cloquet lymph node but *a hernia is deeply fixed, whereas the others tend to be more mobile*
* in contrast to strangulated inguinal hernia, there are often ==__no__== obvious localising symptoms and signs (for strangulation but the classic presenting features are those of distal small bowel obstruction) → diagnosis of strangulated femoral hernia is easily missed
* femoral hernia can easily be missed in an obese patient, CT of the abdomen may be required to clarify the diagnosis
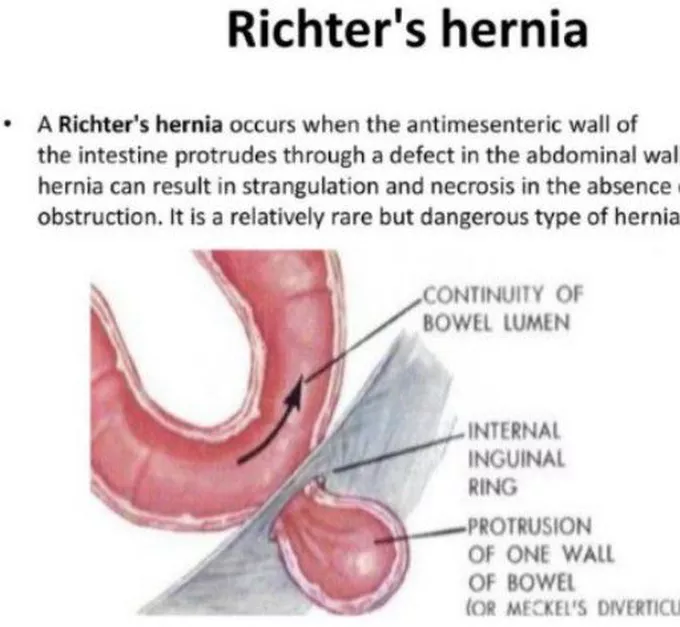
* 30% of femoral hernias are ==__Richter hernias__== = only a portion of the bowel circumference is trapped in the hernial sac so strangulation occurs but not obstruction → bowel lumen remains patent and they are able to pass flatus etc but peristalsis is sufficiently disrupted for other signs of obstruction to occur, notably vomiting
→ resuscitation and urgent operation are required, as for completely strangulated hernias
* the abdominal orifice of the femoral canal is small and indistensible, so abdominal contents finding their way into the canal strangulate much more readily than in inguinal hernias = all femoral hernias (even if asymptomatic) should be repaired without delay
* 40% present with strangulation
* incidence is higher in women and increases with age
→ increased intra-abdominal pressure, and other factors related to pregnancy, may be important in females, since the incidence of femoral hernia is higher in parous than nulliparous women
* clinical features:
* usually small, appearing as a lump immediately below the inguinal ligament and just lateral to its medial attachment to the pubic tubercle
* femoral canal is narrow so a cough impulse can rarely be detected
* the hernia is usually irreducible → small femoral hernias may be difficult to distinguish from other lumps arising in the femoral canal, such as a lipoma or enlarged Cloquet lymph node but *a hernia is deeply fixed, whereas the others tend to be more mobile*
* in contrast to strangulated inguinal hernia, there are often ==__no__== obvious localising symptoms and signs (for strangulation but the classic presenting features are those of distal small bowel obstruction) → diagnosis of strangulated femoral hernia is easily missed
* femoral hernia can easily be missed in an obese patient, CT of the abdomen may be required to clarify the diagnosis
* 30% of femoral hernias are ==__Richter hernias__== = only a portion of the bowel circumference is trapped in the hernial sac so strangulation occurs but not obstruction → bowel lumen remains patent and they are able to pass flatus etc but peristalsis is sufficiently disrupted for other signs of obstruction to occur, notably vomiting
→ resuscitation and urgent operation are required, as for completely strangulated hernias
* the abdominal orifice of the femoral canal is small and indistensible, so abdominal contents finding their way into the canal strangulate much more readily than in inguinal hernias = all femoral hernias (even if asymptomatic) should be repaired without delay
21
New cards
richter hernia
22
New cards
management of femoral hernias
* elective repair is performed by first isolating, emptying and excising the peritoneal sac
* then close the femoral canal
* the canal can be exposed by several different methods. The most common are: (1) the **femoral** or low approach; (2) the **Lotheissen** or high approach, via the posterior wall of the inguinal canal and (3) the **McEvedy** or pararectus extraperitoneal approach (virtually a laparotomy and is rarely used)
???? why are we exposing it???
* *occasionally a femoral hernia containing bowel cannot be safely reduced via a local approach, or bowel of doubtful viability escapes back into the abdominal cavity. In either case, a laparotomy incision is required to safely complete the operation*
* then close the femoral canal
* the canal can be exposed by several different methods. The most common are: (1) the **femoral** or low approach; (2) the **Lotheissen** or high approach, via the posterior wall of the inguinal canal and (3) the **McEvedy** or pararectus extraperitoneal approach (virtually a laparotomy and is rarely used)
???? why are we exposing it???
* *occasionally a femoral hernia containing bowel cannot be safely reduced via a local approach, or bowel of doubtful viability escapes back into the abdominal cavity. In either case, a laparotomy incision is required to safely complete the operation*
23
New cards
4 margins of the femoral canal
24
New cards
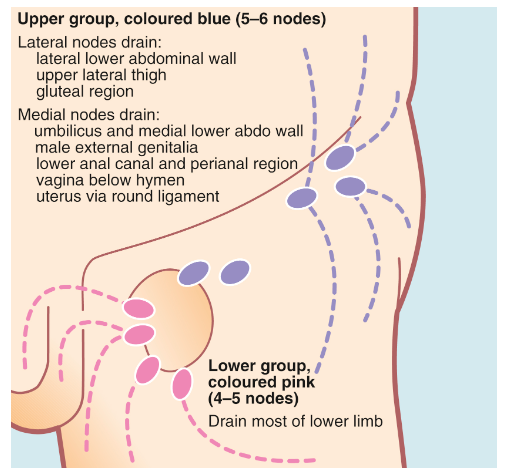
enlarged inguinal lymph nodes
* inguinal lymph nodes are clustered into 3 anatomical groups → drain the lower abdominal wall and lower back, perineum (including vulva and vagina), anal canal, penis and scrotal skin and the whole lower limb
* the testes are derived from the retroperitoneal area and hence drain to the upper paraaortic nodes within the abdomen rather than inguinal nodes
* may become secondarily enlarged as a result of local disease in their field of drainage
may also be part of a generalised lymphadenopathy in lymphoma or a systemic infection
* inguinal nodes may also become involved in tuberculosis
* clinical features:
* pain or a lump in the groin
* often discovered incidentally
* recognised by their anatomical position and by excluding hernias or vascular abnormalities
* usually mobile but become fixed to the surrounding tissues, when infiltrated by tumour
* if in doubt → US usually gives a definitive answer + can guide percutaneous needle biopsy
* typically nodes <1 cm are unlikely to be malignant
* *the history may need to be reviewed for clues as to the origin of any nodes. A history of systemic manifestations of lymphoma, TB or AIDS should be sought. These include malaise, periodic fevers and weight loss. There may be a history of a ‘mole’ or ‘wart’ having been removed, even many years before. If this was a malignant melanoma or squamous carcinoma, it could now have metastasised. Other symptoms of tumours that metastasise to inguinal lymph nodes should be sought; for example, anal pain or bleeding might indicate an anal carcinoma, and an unretractable foreskin may hide a penile carcinoma*
* examination:
* palpate lymph nodes in the neck and axillae
* palpate the liver and spleen
* skin of the whole drainage field should be examined closely, especially the back, perineum and feet and beneath the foreskin
* examination may reveal infection, squamous cell carcinoma or malignant melanoma
* rectal examination is mandatory to exclude anal carcinoma
* a blood test for HIV antigen may be indicated
* *if enlarged lymph nodes cannot be explained by simple local factors or a systemic illness, nodes should be sampled for histology. If metastatic malignancy is suspected, fine-needle aspiration or needle core biopsy is appropriate, but if lymphoma is likely, a node should be surgically removed or be subject to an open biopsy to obtain substantial tissue for histological typing*
* the testes are derived from the retroperitoneal area and hence drain to the upper paraaortic nodes within the abdomen rather than inguinal nodes
* may become secondarily enlarged as a result of local disease in their field of drainage
may also be part of a generalised lymphadenopathy in lymphoma or a systemic infection
* inguinal nodes may also become involved in tuberculosis
* clinical features:
* pain or a lump in the groin
* often discovered incidentally
* recognised by their anatomical position and by excluding hernias or vascular abnormalities
* usually mobile but become fixed to the surrounding tissues, when infiltrated by tumour
* if in doubt → US usually gives a definitive answer + can guide percutaneous needle biopsy
* typically nodes <1 cm are unlikely to be malignant
* *the history may need to be reviewed for clues as to the origin of any nodes. A history of systemic manifestations of lymphoma, TB or AIDS should be sought. These include malaise, periodic fevers and weight loss. There may be a history of a ‘mole’ or ‘wart’ having been removed, even many years before. If this was a malignant melanoma or squamous carcinoma, it could now have metastasised. Other symptoms of tumours that metastasise to inguinal lymph nodes should be sought; for example, anal pain or bleeding might indicate an anal carcinoma, and an unretractable foreskin may hide a penile carcinoma*
* examination:
* palpate lymph nodes in the neck and axillae
* palpate the liver and spleen
* skin of the whole drainage field should be examined closely, especially the back, perineum and feet and beneath the foreskin
* examination may reveal infection, squamous cell carcinoma or malignant melanoma
* rectal examination is mandatory to exclude anal carcinoma
* a blood test for HIV antigen may be indicated
* *if enlarged lymph nodes cannot be explained by simple local factors or a systemic illness, nodes should be sampled for histology. If metastatic malignancy is suspected, fine-needle aspiration or needle core biopsy is appropriate, but if lymphoma is likely, a node should be surgically removed or be subject to an open biopsy to obtain substantial tissue for histological typing*
25
New cards
where does the lymph of testes drain and why
the testes are derived from the retroperitoneal area and hence drain to the upper paraaortic nodes within the abdomen rather than inguinal nodes
26
New cards
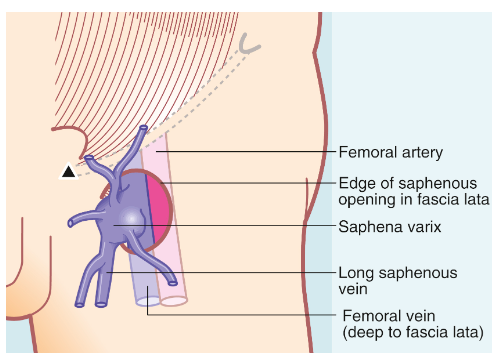
saphena varix
* = a dilatation of the long saphenous vein in the groin just proximal to its junction with the femoral vein
* caused by vascular incompetence at that point
* there are usually substantial varicose veins elsewhere in the long saphenous system
* swelling is soft and diffuse
* ==__diagnostic feature__== → empties with minimal pressure and refills on release
* cough impulse is invariably present and a fluid thrill can be felt if varicosities further down the thigh are tapped lightly
* treatment → high saphenous ligation, as for saphenofemoral reflux associated with varicose veins
* caused by vascular incompetence at that point
* there are usually substantial varicose veins elsewhere in the long saphenous system
* swelling is soft and diffuse
* ==__diagnostic feature__== → empties with minimal pressure and refills on release
* cough impulse is invariably present and a fluid thrill can be felt if varicosities further down the thigh are tapped lightly
* treatment → high saphenous ligation, as for saphenofemoral reflux associated with varicose veins
27
New cards
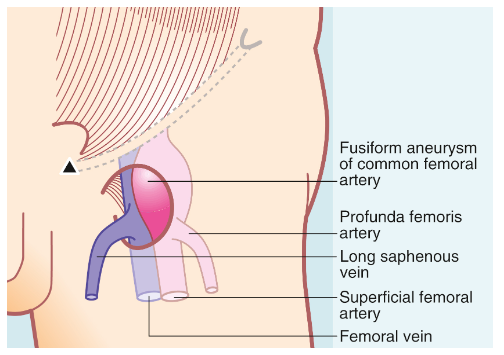
femoral artery aneurysms
* uncommon as a cause of lumps in the groin
* may occur as part of a generalised aneurysmal disease or isolated
* ==__diagnosis is made on clinical examination; the lump lies below the midpoint of the inguinal ligament and has a characteristic expansile pulsation__==
* may occur as part of a generalised aneurysmal disease or isolated
* ==__diagnosis is made on clinical examination; the lump lies below the midpoint of the inguinal ligament and has a characteristic expansile pulsation__==
28
New cards
chronic groin pain
*Chronic groin pain without any clues in the history and without swelling is difficult to diagnose and treat. Groin pain may be caused by* ***inflamed inguinal lymph nodes*** *secondary to infection in their field of drainage.* ***Strained muscle attachments*** *to the bony pelvis sometimes cause groin pain; this particularly affects the hip adductor attachments near the pubic tubercle and usually follows extreme physical activity. Groin pain may also be* ***referred*** *from a diseased hip joint. ‘Groin strain’ (a.k.a. athletic pubalgia or sportsman’s groin) is a difficult entity to understand and often affects professional sports people. It starts acutely but often becomes chronic; the diagnosis is one of exclusion. A newly appeared inguinal hernia may cause groin pain, often on sitting, yet be too small to detect clinically. Unfortunately, there is no dependable test for an early hernia other than laparoscopy, although ultrasound in experienced hands is fairly reliable. There is increasing interest in the use of magnetic resonance imaging for investigating chronic groin pain but the science is still young.*
29
New cards
ventral hernias
= epigastric, umbilical and paraumbilical hernias
\
1. epigastric hernias:
* = midline herniations through defects in the linea alba, anywhere between xiphoid process and umbilicus
* Common, incidence of 5%
* 4:1 male to female
* often tiny, most are asymptomatic
* the presence of a lump and sometimes episodic sharp pain on exertion are the usual presenting complaints
* Present either as a small painless mass which becomes painful with activity or a small painful incarcerated mass
* Can be multiple hernias
* treatment is by surgical repair since they do not resolve → closing the hernial defect and usually reinforcing the closure with mesh
* Should not be confused with diastasis recti which is generalised weakness of the linea alba from umbilicus to xiphoid and almost always resolves by 10 y/o
2. umbilical and para umbilical hernias:
* common disorder in children
* Unlike other hernias of childhood, a fascial defect is present at birth but may resolve without the need for an operation
* Failure of any of the closure processes (next flashcard) may result in an umbilical hernia
* The hernia sac is peritoneum and is usually very adherent to the dermis of the umbilical skin
* Extent of skin protrusion is not always indicative of the size of the fascia defect, frequently, small defects can result in alarmingly large probiscis like protrusions → hernia must be palpated by reducing the hernia to assess whether operative or non operative treatment is appropriate
* Patients with small fascial defects appear more prone to incarceration
* Higher incidence in SGA and premature babies
Also in children with beckwith, hurler syndrome, trisomies, congenital hypothyroidism and children requiring peritoneal dialysis
* Typically close spontaneously (>90% by 1 y/o) so it is safe to watch and wait until they’re 4-5 y/o
but there is a risk of incarceration of strangulation but it is rare (<1%)
* **paraumbilical hernias** are acquired rather than congenital
* occur in all age groups
* five times more common in females
* the abdominal wall defect is in the linea alba, generally above or below the umbilical cicatrix
* the swelling lies adjacent to the umbilicus, with the umbilicus itself pushed to the side to produce the characteristic ‘smile’ of a paraumbilical hernia
* **True umbilical hernias** are the 3rd most common abdominal hernia in adults
* occur directly through the umbilical cicatrix
* occur more commonly in females
* obesity and poor muscle tone are predisposing factors
* range from asymptomatic small protrusions, through larger and occasionally painful lumps, to very large, irreducible and intermittently painful swellings
* Pressure depressing and other devices to keep the hernia reduced or not suggested and do not enhance the closure process instead they may result in skin irritation and breakdown
* both paraumbilical and umbilical hernias become progressively larger and surgical repair is the treatment of choice. This is by suture closure of the hernial defect and reinforcement with mesh
contradiction???
\
1. epigastric hernias:
* = midline herniations through defects in the linea alba, anywhere between xiphoid process and umbilicus
* Common, incidence of 5%
* 4:1 male to female
* often tiny, most are asymptomatic
* the presence of a lump and sometimes episodic sharp pain on exertion are the usual presenting complaints
* Present either as a small painless mass which becomes painful with activity or a small painful incarcerated mass
* Can be multiple hernias
* treatment is by surgical repair since they do not resolve → closing the hernial defect and usually reinforcing the closure with mesh
* Should not be confused with diastasis recti which is generalised weakness of the linea alba from umbilicus to xiphoid and almost always resolves by 10 y/o
2. umbilical and para umbilical hernias:
* common disorder in children
* Unlike other hernias of childhood, a fascial defect is present at birth but may resolve without the need for an operation
* Failure of any of the closure processes (next flashcard) may result in an umbilical hernia
* The hernia sac is peritoneum and is usually very adherent to the dermis of the umbilical skin
* Extent of skin protrusion is not always indicative of the size of the fascia defect, frequently, small defects can result in alarmingly large probiscis like protrusions → hernia must be palpated by reducing the hernia to assess whether operative or non operative treatment is appropriate
* Patients with small fascial defects appear more prone to incarceration
* Higher incidence in SGA and premature babies
Also in children with beckwith, hurler syndrome, trisomies, congenital hypothyroidism and children requiring peritoneal dialysis
* Typically close spontaneously (>90% by 1 y/o) so it is safe to watch and wait until they’re 4-5 y/o
but there is a risk of incarceration of strangulation but it is rare (<1%)
* **paraumbilical hernias** are acquired rather than congenital
* occur in all age groups
* five times more common in females
* the abdominal wall defect is in the linea alba, generally above or below the umbilical cicatrix
* the swelling lies adjacent to the umbilicus, with the umbilicus itself pushed to the side to produce the characteristic ‘smile’ of a paraumbilical hernia
* **True umbilical hernias** are the 3rd most common abdominal hernia in adults
* occur directly through the umbilical cicatrix
* occur more commonly in females
* obesity and poor muscle tone are predisposing factors
* range from asymptomatic small protrusions, through larger and occasionally painful lumps, to very large, irreducible and intermittently painful swellings
* Pressure depressing and other devices to keep the hernia reduced or not suggested and do not enhance the closure process instead they may result in skin irritation and breakdown
* both paraumbilical and umbilical hernias become progressively larger and surgical repair is the treatment of choice. This is by suture closure of the hernial defect and reinforcement with mesh
contradiction???
30
New cards
What is required for the closure of the umbilical ring
It is the result of complex interactions within the lateral body wall folding in a medial direction, fusion of the rectus abdominis muscles into the linea alba and umbilical orifice contraction that is aided by elastic fibres from the obliterated umbilical arteries
Fibrous proliferation of the surrounding lateral connective tissue plate and mechanical stress from rectus muscle tension also may help with natural closure
Fibrous proliferation of the surrounding lateral connective tissue plate and mechanical stress from rectus muscle tension also may help with natural closure
31
New cards
Embryology of hernias
* Abdominal cavity is lined by parietal peritoneum → out-pouching in front of the testis and gubernaculum = processus vaginalis
First seen at 2-3 months of gestation
* Germ cells are found in the urogenital ridge by the 6th week
* Testes begin to differentiate by week 7
* Testicular descent has two stages → abdominal phase (8-15 weeks gestation, not androgen dependent) and inguinoscrotal phase (25-35 weeks, androgen dependent, i think, check)
*Testicular descent occurs in two stages: the first is an abdominal phase (8-15 weeks gestation) with swelling and strengthening of the distal gubernaculum under the influence of insulin-like hormone 3 (InsL3). The swelling causes the gubernaculum to maintain a fixed length in males. At the same time, fetal testosterone causes regression of the cranial suspensory liga- ment. The testis is thus anchored to the internal ring while the abdominal cavity increases in size. By 25-35 weeks (inguinoscrotal phase), the gubernaculum extends down to the base of the scrotum. Androgenic hormones lead to release of neurotrophins that regulate the sensory branches of the genitofemoral nerve. Calcitonin gene-related peptide (CGRP) release provides a local chemotactic gradient to guide the gubernaculum.! The testis then passes through the inguinal canal and eventually reaches the base of the scrotum*
* Female analogue to pv is canal of nuck which leads to the labia majors
* Both PV and canal of nuck should close by 7 months of foetal life
* Initial closure of the internal inguinal ring is followed by obliteration of part of the PV
The residual space between the cranial and caudal portions (funicular process) is normally the last to obliterate
* Disorders with increased abdominal pressure/fluid (eg. Ascites, chronic cough) are associated with increased incidence of indirect inguinal hernias
* Prematurity results in delivery prior to completion of normal descent and obliteration, and is associated with an increased incidence of inguinal hernia ranging from 10-30%, depending on the degree of prematurity
* Check the ipad photos from anatomy to see which abdominal muscle/fascia is continuous with those in the spermatic cord/inguinal canal
* !! The PV envelops the testis as the visceral and parietal layers of the tunica vaginalis
First seen at 2-3 months of gestation
* Germ cells are found in the urogenital ridge by the 6th week
* Testes begin to differentiate by week 7
* Testicular descent has two stages → abdominal phase (8-15 weeks gestation, not androgen dependent) and inguinoscrotal phase (25-35 weeks, androgen dependent, i think, check)
*Testicular descent occurs in two stages: the first is an abdominal phase (8-15 weeks gestation) with swelling and strengthening of the distal gubernaculum under the influence of insulin-like hormone 3 (InsL3). The swelling causes the gubernaculum to maintain a fixed length in males. At the same time, fetal testosterone causes regression of the cranial suspensory liga- ment. The testis is thus anchored to the internal ring while the abdominal cavity increases in size. By 25-35 weeks (inguinoscrotal phase), the gubernaculum extends down to the base of the scrotum. Androgenic hormones lead to release of neurotrophins that regulate the sensory branches of the genitofemoral nerve. Calcitonin gene-related peptide (CGRP) release provides a local chemotactic gradient to guide the gubernaculum.! The testis then passes through the inguinal canal and eventually reaches the base of the scrotum*
* Female analogue to pv is canal of nuck which leads to the labia majors
* Both PV and canal of nuck should close by 7 months of foetal life
* Initial closure of the internal inguinal ring is followed by obliteration of part of the PV
The residual space between the cranial and caudal portions (funicular process) is normally the last to obliterate
* Disorders with increased abdominal pressure/fluid (eg. Ascites, chronic cough) are associated with increased incidence of indirect inguinal hernias
* Prematurity results in delivery prior to completion of normal descent and obliteration, and is associated with an increased incidence of inguinal hernia ranging from 10-30%, depending on the degree of prematurity
* Check the ipad photos from anatomy to see which abdominal muscle/fascia is continuous with those in the spermatic cord/inguinal canal
* !! The PV envelops the testis as the visceral and parietal layers of the tunica vaginalis
32
New cards
Hernia risk factors
* prematurity is the main one
* CF
* Ventriculoperitoneal shunts for hydrocephalus
* Genitourinary anomalies
* CF
* Ventriculoperitoneal shunts for hydrocephalus
* Genitourinary anomalies
33
New cards
Usual presentation of hernia in a child is…
An asymptomatic, intermittent, unilateral inguinal bulge
Since it is usually intermittent, it is common to have a normal examination and a suggestive history
\
The most common examination finding is a reduced inguinal or scrotal vulde, more prominent during Valsalva manoeuvres
Since it is usually intermittent, it is common to have a normal examination and a suggestive history
\
The most common examination finding is a reduced inguinal or scrotal vulde, more prominent during Valsalva manoeuvres
34
New cards
When is the incarceration of an inguinal hernia most common
First year of life (3-16%)
Other risk factors → prematurity, increasing wait time for elective hernia repair, no difference in gender once a hernia has occurred
Many series of incarcerated hernias note a period history of an unrepaired inguinal hernia
But sometimes, incarceration may be the presenting sign of the inguinal hernia
Other risk factors → prematurity, increasing wait time for elective hernia repair, no difference in gender once a hernia has occurred
Many series of incarcerated hernias note a period history of an unrepaired inguinal hernia
But sometimes, incarceration may be the presenting sign of the inguinal hernia
35
New cards
Late signs of incarceration
Abdominal distension, bowel obstruction and bloody stools
Peritoneal signs suggest strangulated intestine
Peritoneal signs suggest strangulated intestine
36
New cards
What is an absolute contraindication to attempted reduction of a hernia
Peritonitis, haemodynamic instability or septic shock
Ischaemic or gangrenous bowel is NOT always a contraindication
Ischaemic or gangrenous bowel is NOT always a contraindication
37
New cards
After reduction of an incarcerated hernia…
A delay of 24-48 hrs to allow resolution of the oedema prior to open repair is recommended
(But i thought incarcerated means it cant be reduced???)
Urgent operation is done if it cant be reduced preferably laparoscopic approach but on occasion the hernia may spontaneously reduce with the induction of general anaesthesia, if laparoscopy is planned it should proceed
(But i thought incarcerated means it cant be reduced???)
Urgent operation is done if it cant be reduced preferably laparoscopic approach but on occasion the hernia may spontaneously reduce with the induction of general anaesthesia, if laparoscopy is planned it should proceed
38
New cards
A sliding hernia is more common in…
Incarcerated hernias, especially in girls
39
New cards
The parents of a boy with an incarcerated hernia should be…
Counselled about the possibility of testicular loss or injury
40
New cards
In girls with an incarcerated hernia…
The ovary and or Fallopian tubes are more commonly involved than the intestines
41
New cards
Operative technique for inguinal hernias (do we need to know this???)\*\*\*
42
New cards
inguinal hernia repair in infants\*\*\*
*Laparoscopy has several advantages when compared with open repair in the treatment of an inguinal hernia in infants. First, with laparoscopy, there is a reduction in postoperative infections. This may result because laparoscopic scars are located higher compared with the inguinal incisions (inside the diaper area), which are subject to urine or fecal contamination. Recent reports have found fewer wound infections following laparoscopic repair versus open repair in infants of similar ages (0 vs 2.3%).68,103 The major technical challenge of the LIHR in infants is the very limited working space that can result from bowel distention. It can be helpful to perform a bowel prep with simethicone and one or two enemas the day before the operation to empty the intestinal loops to create a larger working space.104 In small infants, there is no true triangulation between the telescope and cannulas because the two operative port sites are located higher than usual and are positioned on the umbilical plane at the same level as the telescope to establish an adequate working distance from the internal inguinal ring. In infants it is sometimes preferable to insert the working ports through the cannula of the umbilical optic port—“trocar in trocar” (Fig. 50.25) to prevent injury to the bowel. Also, the length of the needle should be a maximum of about 17–20 mm because bigger needles are difficult to manipulate in infants and may have a higher risk of complications.*
43
New cards
why laparoscopy > open repair
better visualization of the vital cord structures, thereby making dissection of these structures safer. There is no dissection of the abdominal wall or spermatic cord structures, thus theoretically reducing the risk of testicular atrophy, secondary cryptorchidism, or other complications. Serious intraoperative complications such as bladder injury or rupture, which can occur with the open repair with excessive mobilization of the sac, are less likely with the laparoscopic technique due to improved visualization of the anatomy. Another advantage of laparoscopy is identification and treatment of a CPPV, present in up to half the patients, particularly the younger ones (Table 50.1).105 Repair of a CPPV, if needed, should be offered to all families, because 90% desire to have the CPPV repaired at the same operative setting
44
New cards
what disorder (not CF) is associated with inguinal hernias
complete androgen insensitivity syndrome (normal female appearance and external genitalia, with an XY karyotype)
rare
rare
45
New cards
incidental PPV
*Often an incidental PPV is discovered in a child undergoing laparoscopy for an unrelated problem (e.g., appendectomy) (Fig. 50.28).131,132 In a series of 1548 infants and children, the incidence of PPV was 20% (72% male, with a mean age of 4.8 months; most were younger than 1 year of age).131 Only 13% of those found to have a PPV developed a clinical hernia and at a median of 9 months from the original laparoscopy. The surgeon should inform the family of the findings, but most pediatric surgeons recommend observation for incidental asymptomatic PPVs.*
46
New cards
In an adult meta-analysis, there was no evidence of an association between prior inguinal hernia repair (without mesh) and male infertility or obstructive azoospermia.154 Conversely, in series of adults who have obstructive azoospermia, pediatric inguinal hernia repairs are a common cause
47
New cards
Chronic pain after inguinal hernia repair is widely recognized in adults (10–15%), but less so in children
48
New cards
Spigelian and lumbar hernias\*\*\*