Lines and Tubes
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
Purpose of IV/AV lines
Administer drugs and fluids: quick response, high concentration
To collect blood samples: monitor blood gases, alcohol, poison, sugar, etc
3 methods of injection
bolus
gravity infusion
infusion pump
Bolus
injection with hand-held syringe or automatic injection over short period of time
Gravity Infusion
bag of solution connected to tubing and needle
Infusion pump
electronic control of rate and volume of injection
When would an infusion pump alarm
low battery, air or foreign body in line, kinked, solution depleted, disconnected line, infiltration/extravasation
Parenteral solutions
saline - clear fluid
5% dextrose (D5) - clear fluid provides energy and carbs
total parenteral nutrition (TPN) -milky white, replace GI nutrition
vitamins
Standard height
18-20" above injection site
Drip rate
follow order of MD/pharmacy per specific drug amount over period of time
What should you check a solution for
clarity
expiration
container condition
label (correct dose and drug, correct concentration and rout of administration)
Gauge
unit that IV catheters are measured in to describe diameter
Larger the number the smaller the diameter
6 rights to administering meds
right time
right route
right medication
right dose
right patient
right reaction
DOCUMENT!
Extravasation
escape of fluid or blood from a vessel into surrounding tissue (blown vein)

Extravasation signs/symptoms
puffy near injection site
poor infusion
pain at injection site
swelling
cool to touch
pale skin at sight
Extravasation Response
STOP IV
call RN/MD
elevate effected area
warm compress
Phlebitis
inflammation of a vein
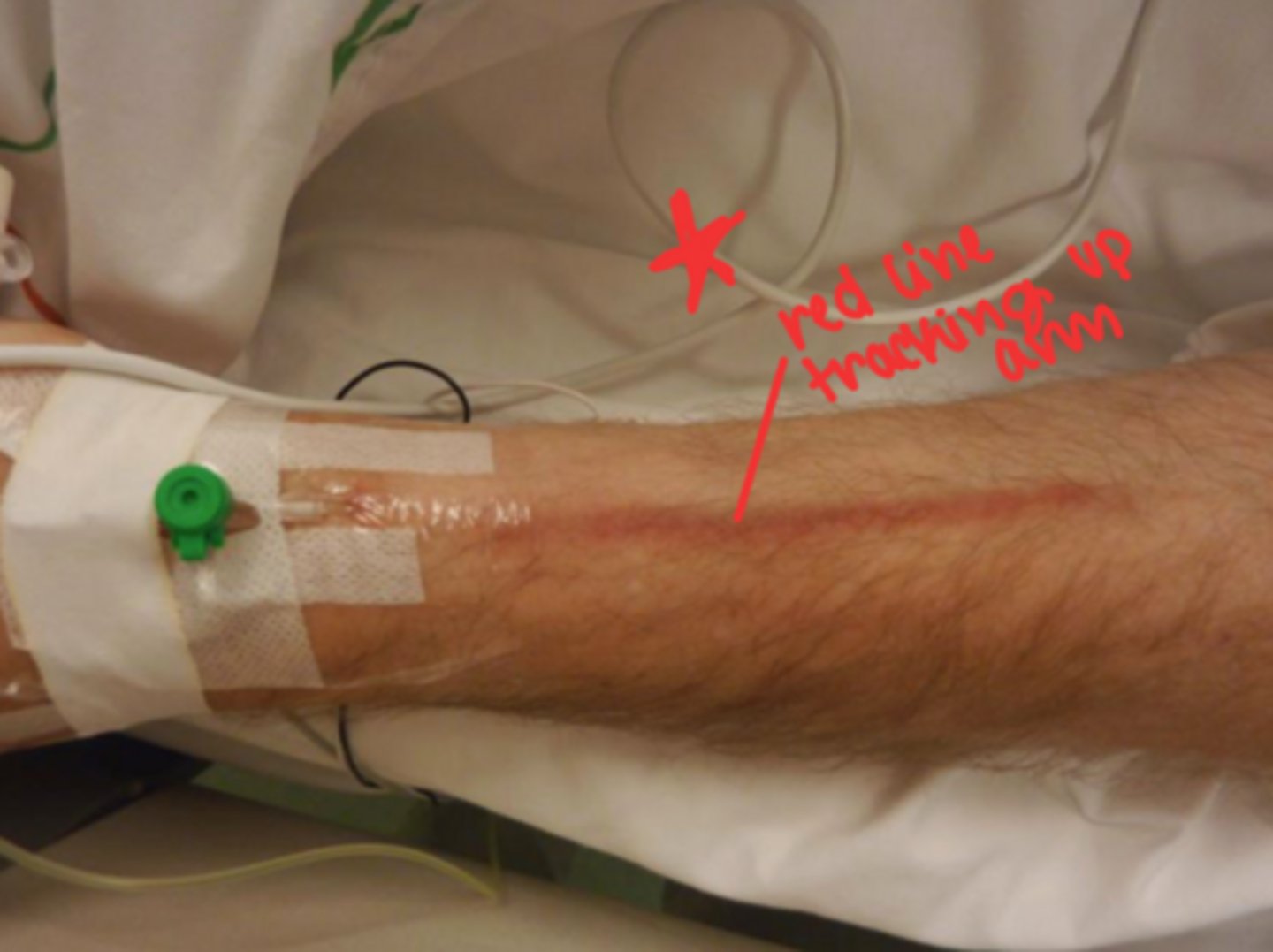
Phlebitis signs and symptoms
red line along vein going up the arm
poor infusion
blood backup in line
swollen red vein
pain proximal to puncture sight
phlebitis response
Call RN/MD
elevate effected part
warm compress
discontinue IV
Venous Thrombosis
The formation of blood clots within a vein (stationary clot)

Venous thrombosis signs/symptoms
poor infusion
blood backup in line
redness (but not up the arm like phlebitits)
Venous thrombosis response
call MD and RN
alert for pulmonary embolus
Embolus
blood clot or foreign material travels to narrow site in a vessel, creating occlusion
Types of embolus
Pulmonary emboli (most common)
brain emboli
coronary emboli
Increased risk of embolus
central lines
trauma
valve defects
atherosclerosis
venous stasis
post-op
Embolus signs/symptoms
sudden onset of symptoms
chest pain
dyspnea
rapid pulse
pallor
diaphoresis
clammy skin
Embolus Response
rapid response
contact RN
Infection
systemic or localized infection because of lack of asepsis or poor continued care of IV

Infection signs and symptoms
fever
angry and red appearance of site
elevated WBC
chills or headaches, backaches, nausea
Infection response
Report to RN/MD
discontinue IV
antibiotics
3 Basic types of Upper GI devices
Nasogastric (NG)
Orogastric (OG)
Nasoentric (NE)
Nasogastric (NG)
nose to stomach
Orogastric (OG)
mouth and stomach
Nasoenteric (NE)
nose to small intestine
Purpose of Upper GI devices
feed, give meds (NE tube), remove GI content, connect to suction
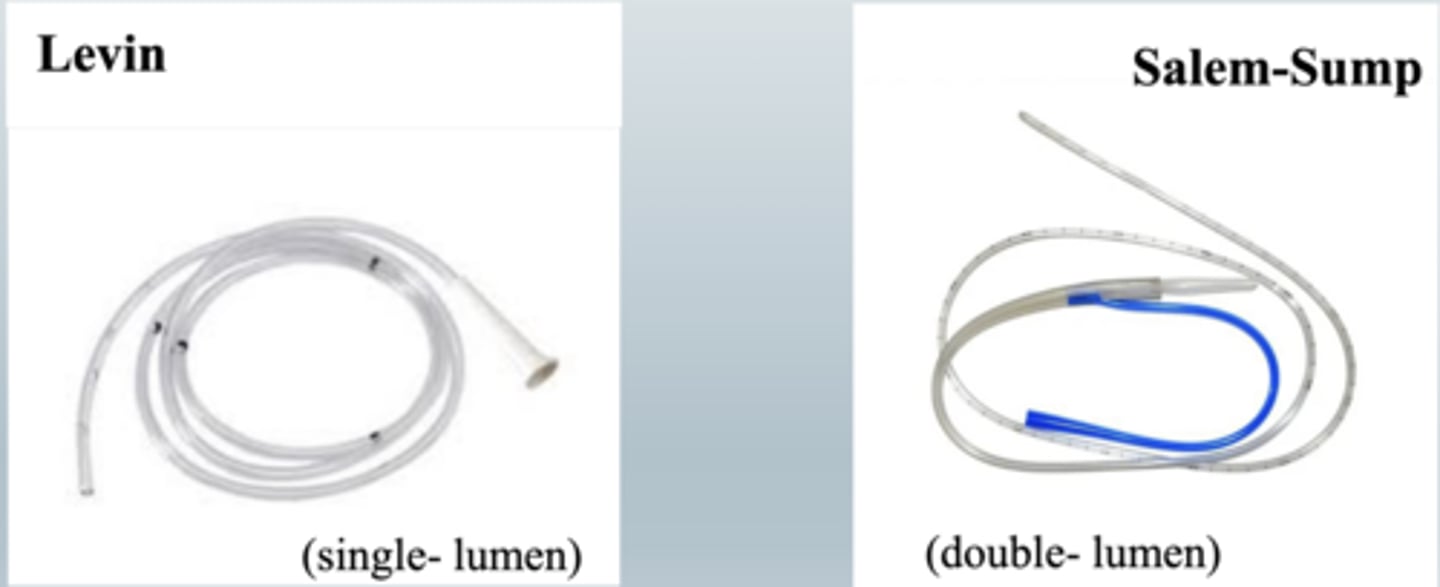
2 types of nasogastric tubes
Levin (single lumen)
Salem-sump (double lumen)
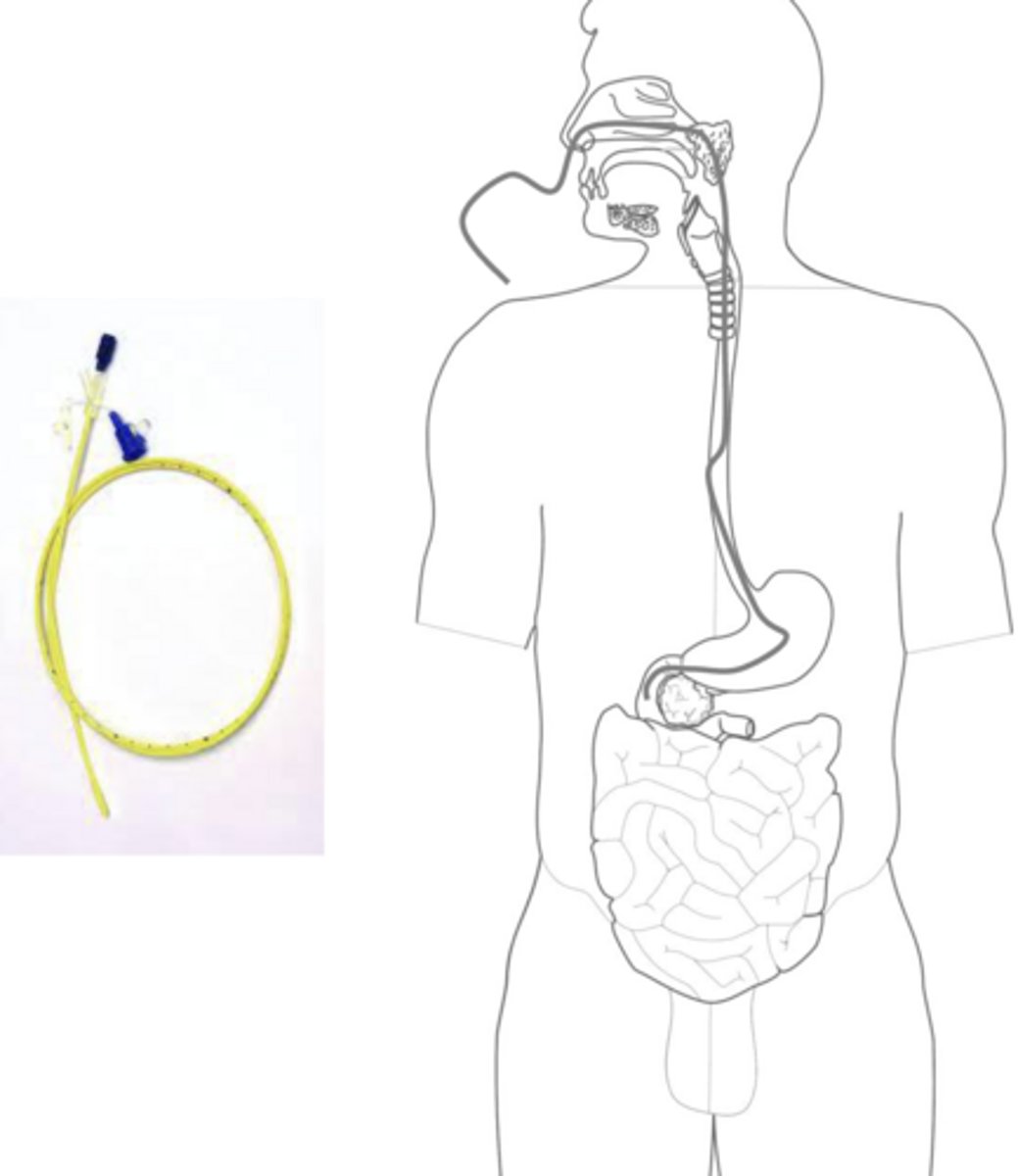
Pathway of NG tube
nose -> esophagus -> stomach
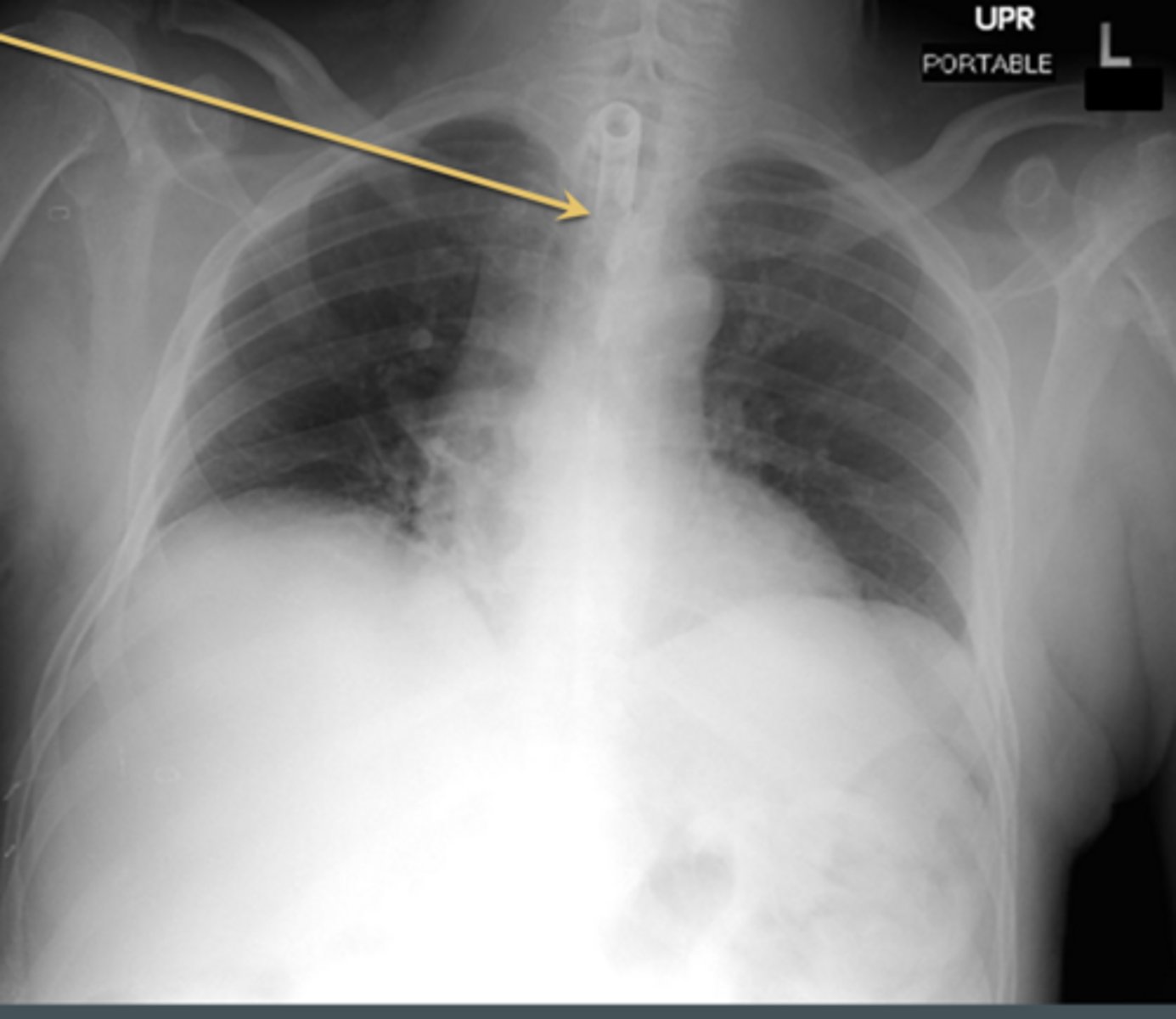
What's wrong with this NG tube
the tube is not fully in the stomach

RT role in placement of GI tube
watch for improper placement
radiographic verification
How to find NG tube
find line in the neck and follow it to the stomach and the loop it makes in stomach
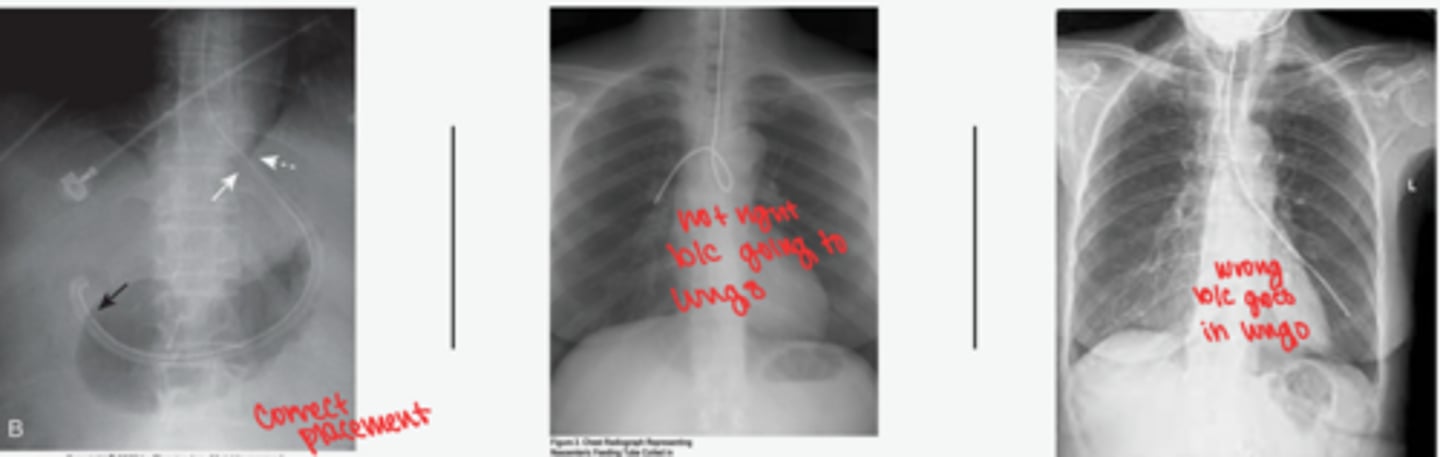
NG tube in lung
Alert

NE tubes function
introduce materials into small intestine
minimize reflux, regurgitation, aspiration
NE tube pathway
nose -> esophagus -> stomach -> duodenum
inserted through nose, mouth, or surgical opening
NE tubes other names and info
AKA: Dobbhoff
small lume gets easily blocked
weighted tip to carry it along GI tract
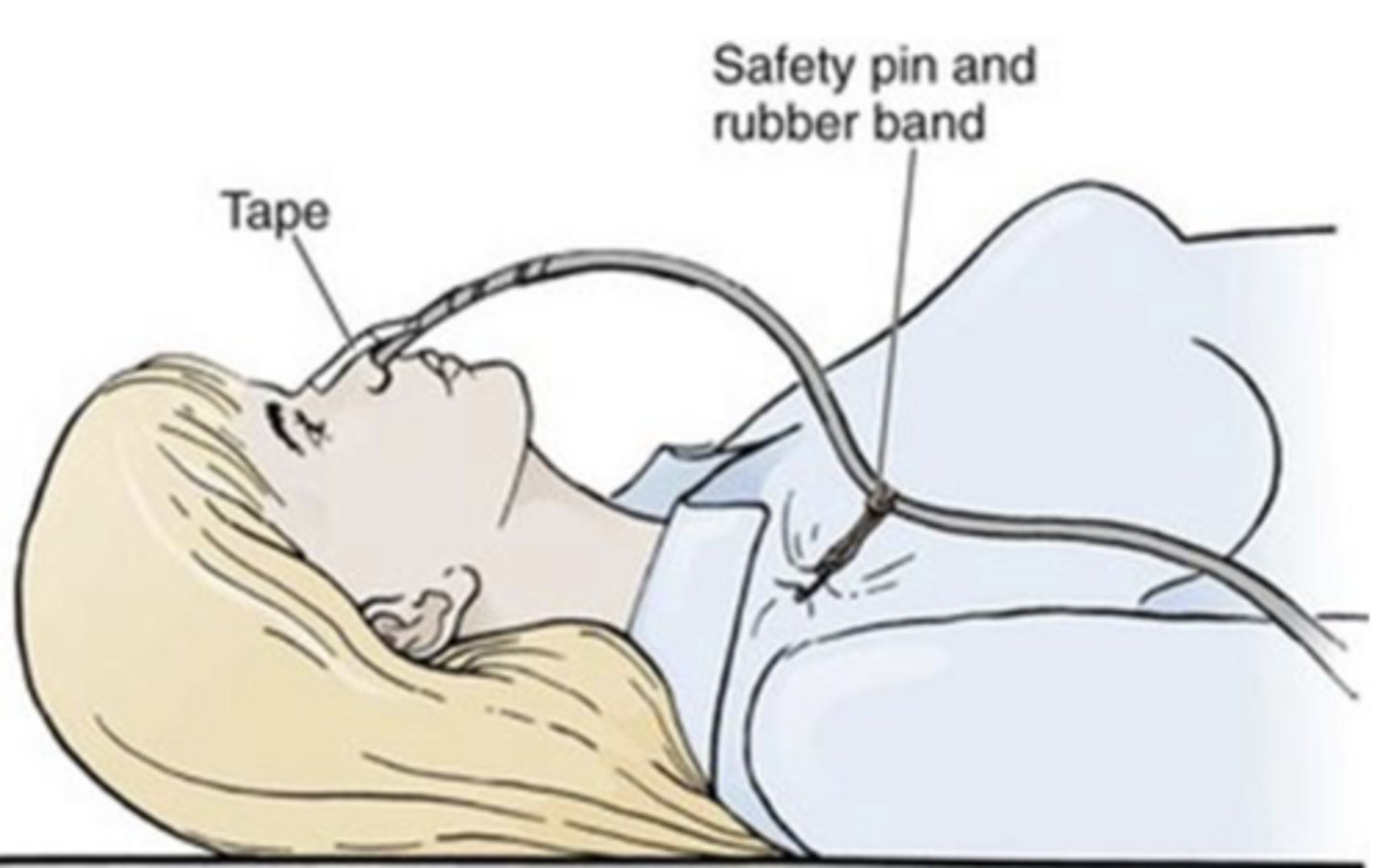
NE tube care during imaging
avoid tension on line
pin tube to clothing
GENTLY brush tube out of xray field
report to RN if concerned placement is incorrect
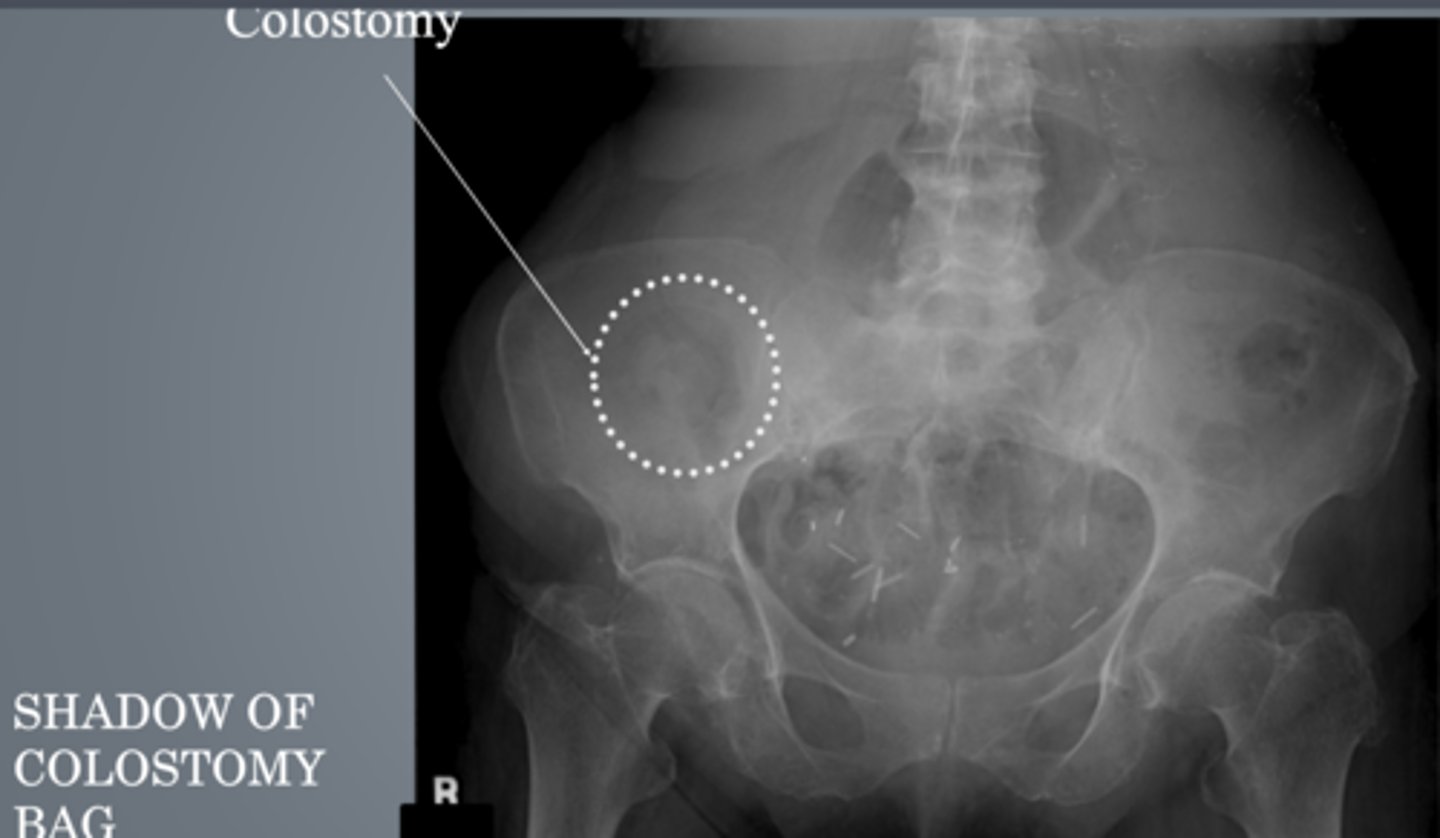
Colostomy Bag (Lower GI)
connection between colon and external abdominal wall
empties into collection bag
temporary or permanent
Ileostomy
connection between small intestine and external abdominal wall
Ostomy Bag care
don't usually do anything, outpatients can usually care for their own bag
if dislodges, clean and dry area
What is a Tupperware seal for an ostomy bag?
have patient tighten stomach and reapply device (ostomy bag) to create seal
Enema tips
straight or cuffed
some are triple lumen
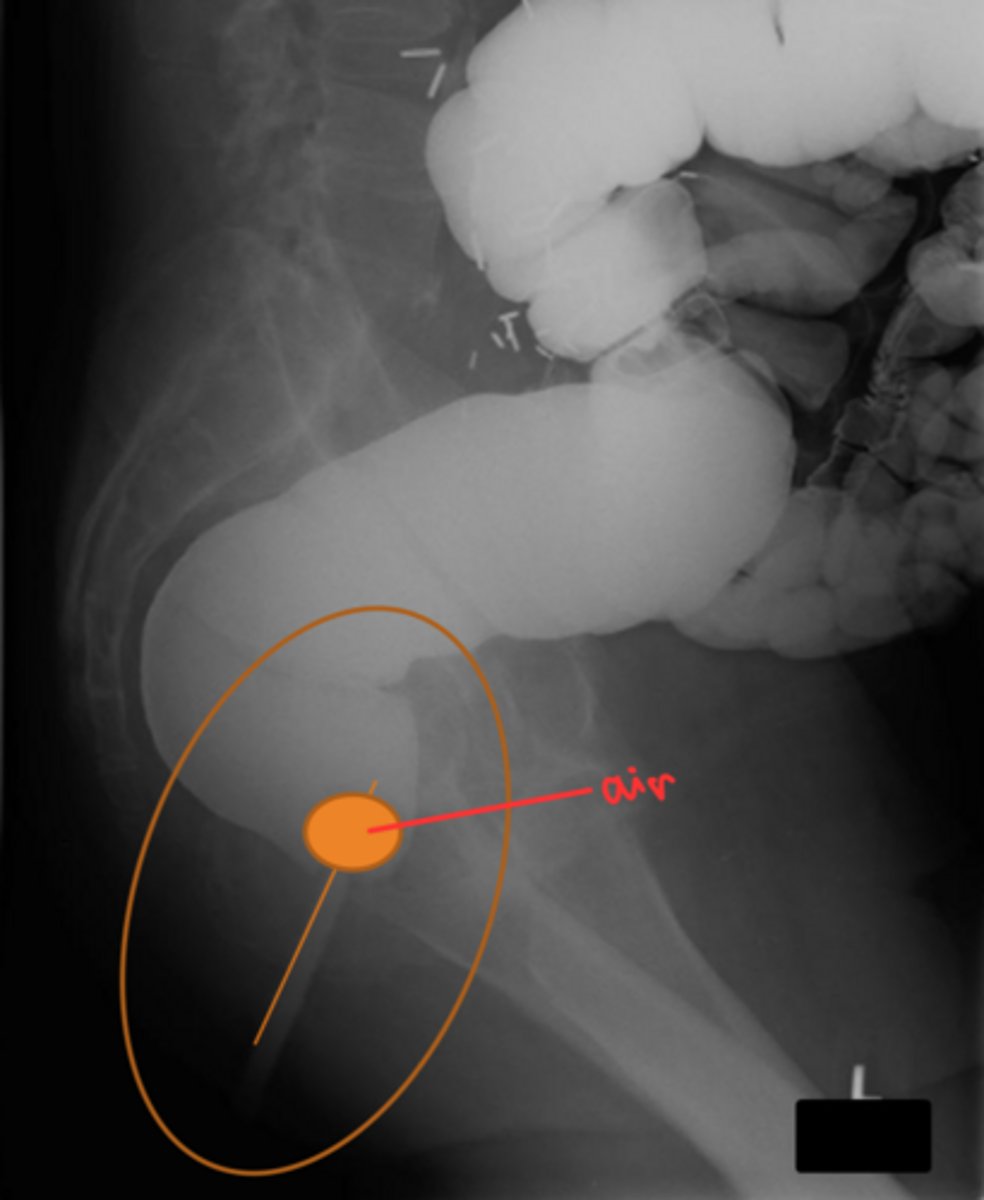
Tripple lumen enema tips
channels for barium, cuff air, colonic air
3 types of urinary catheters
1) foley catheter
2) ureteral stent
3) nephrostomy tube
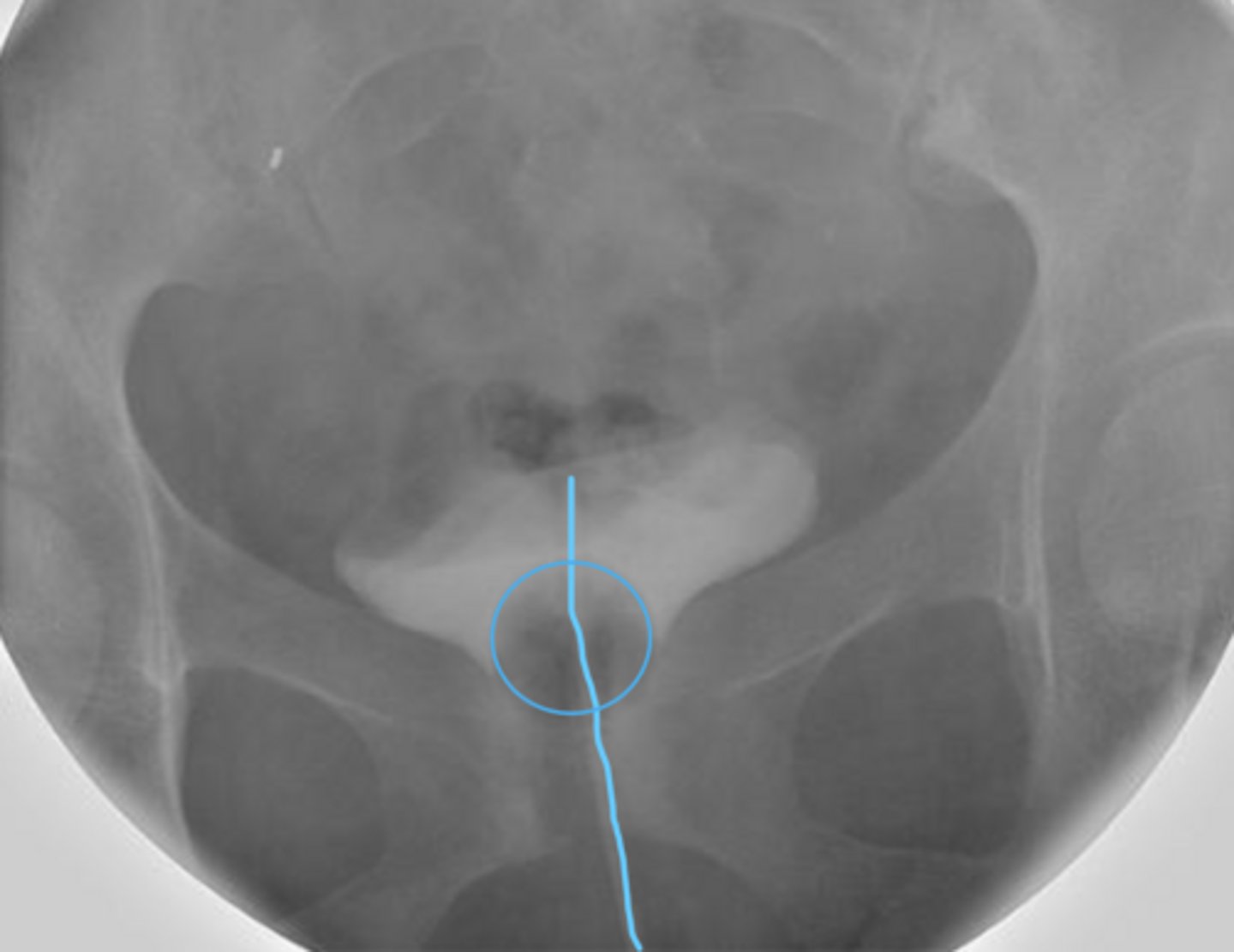
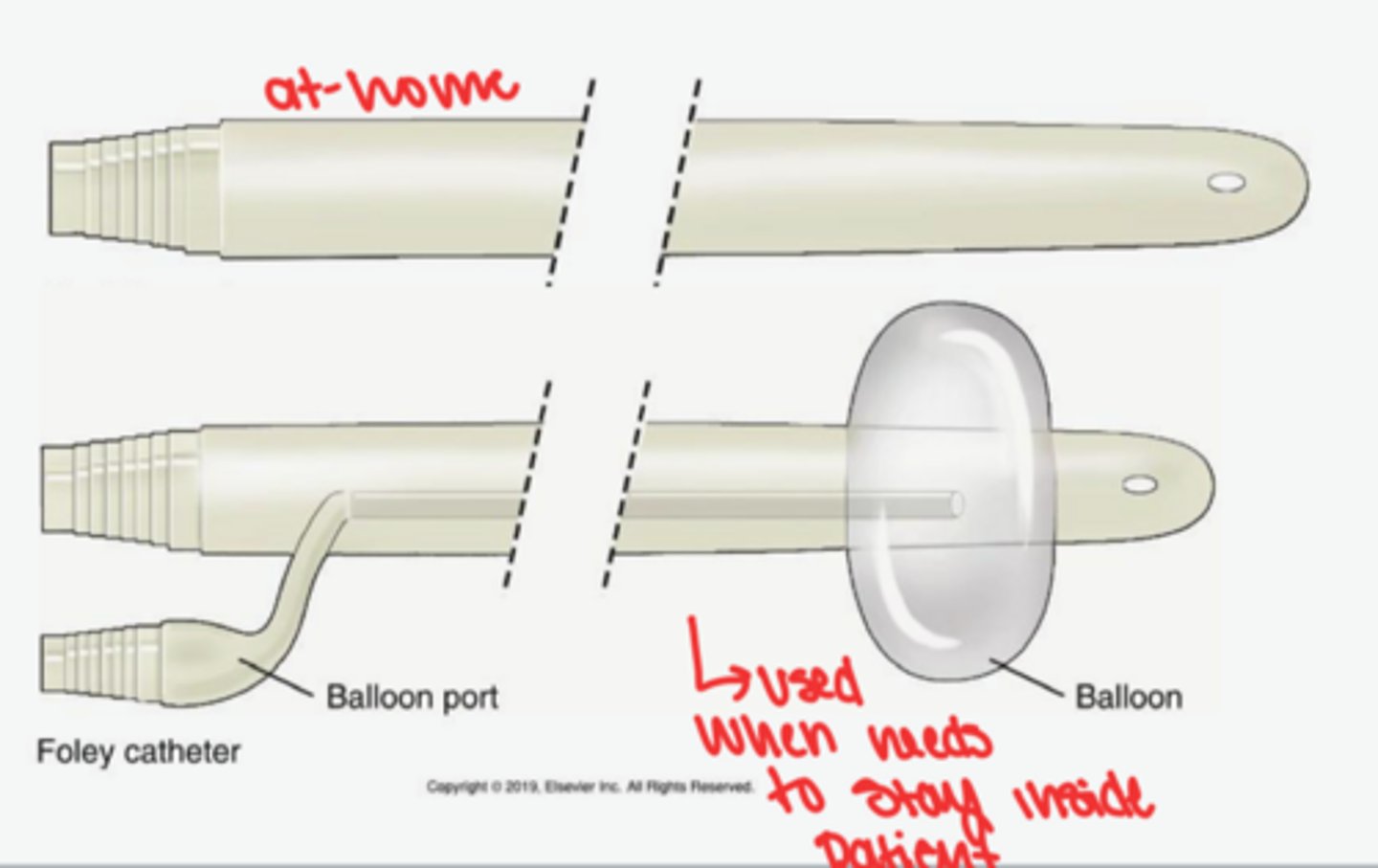
Foley catheter
drain bladder
sometimes to introduce contrast to body
can be seen when put a contrast in bladder
don't xray these but can see during pelvis exam
ureteral stent
kidney to bladder
nephrostomy tube
kidney to outside the body
releases pressure from kindeys
CCU and NCU
cardiac care unit
neurological care unit
Reasons for urinary catheterization
unable to use bedpan
trauma (fractured hip)
post-op
irrigation of bladder
chemo
incontinence
input/output documentation
epidural/spinal where patient cannot feel sensation to void
Urinary catheter sizing
french numbers: increase number=increase diameter
Urinary catheter types
Indwelling (foley)
Intermittent/in and out/ straight catheterization (Bardex)
Internal vs external end of catheter
Internal end is in the bladder and secured with balloon cuff
external end attaches to drainage bag
Catheterization precautions
Extreme UTI potential
keep drainage bags BELOW level of bladder but OFF floor
avoid tension on catheter
Nephrostomy
sometimes x-ray for placement
percutaneous (placed in OR) through back into renal pelvis
entrance at kidney from back, exits outside body
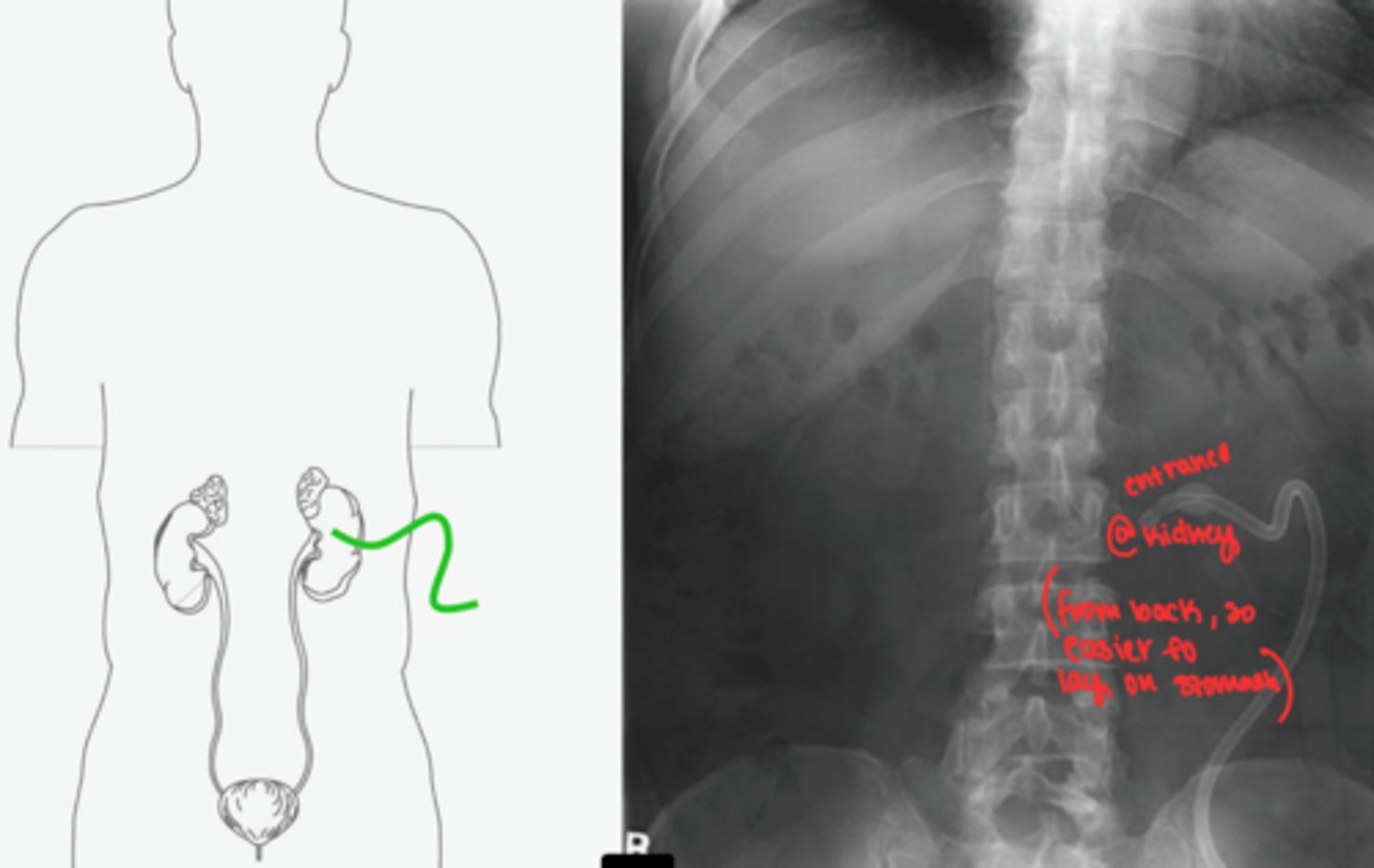
Nephrostomy purpose
drain urine or administer meds
Ureteral stent "pig-tail stents"
connects between kidney and bladder

Oxygen (respiratory device) reminders
high pressure in tank
use roller when transporting tank
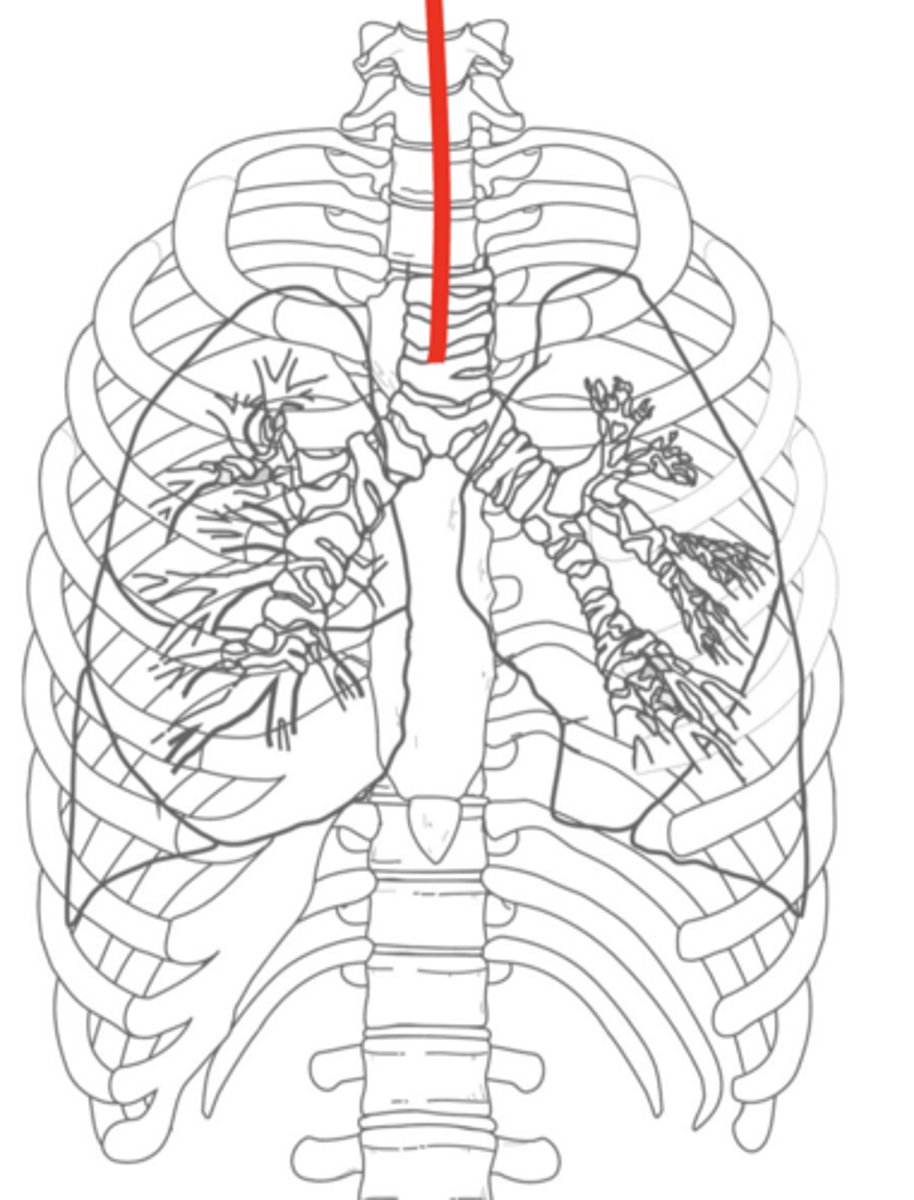
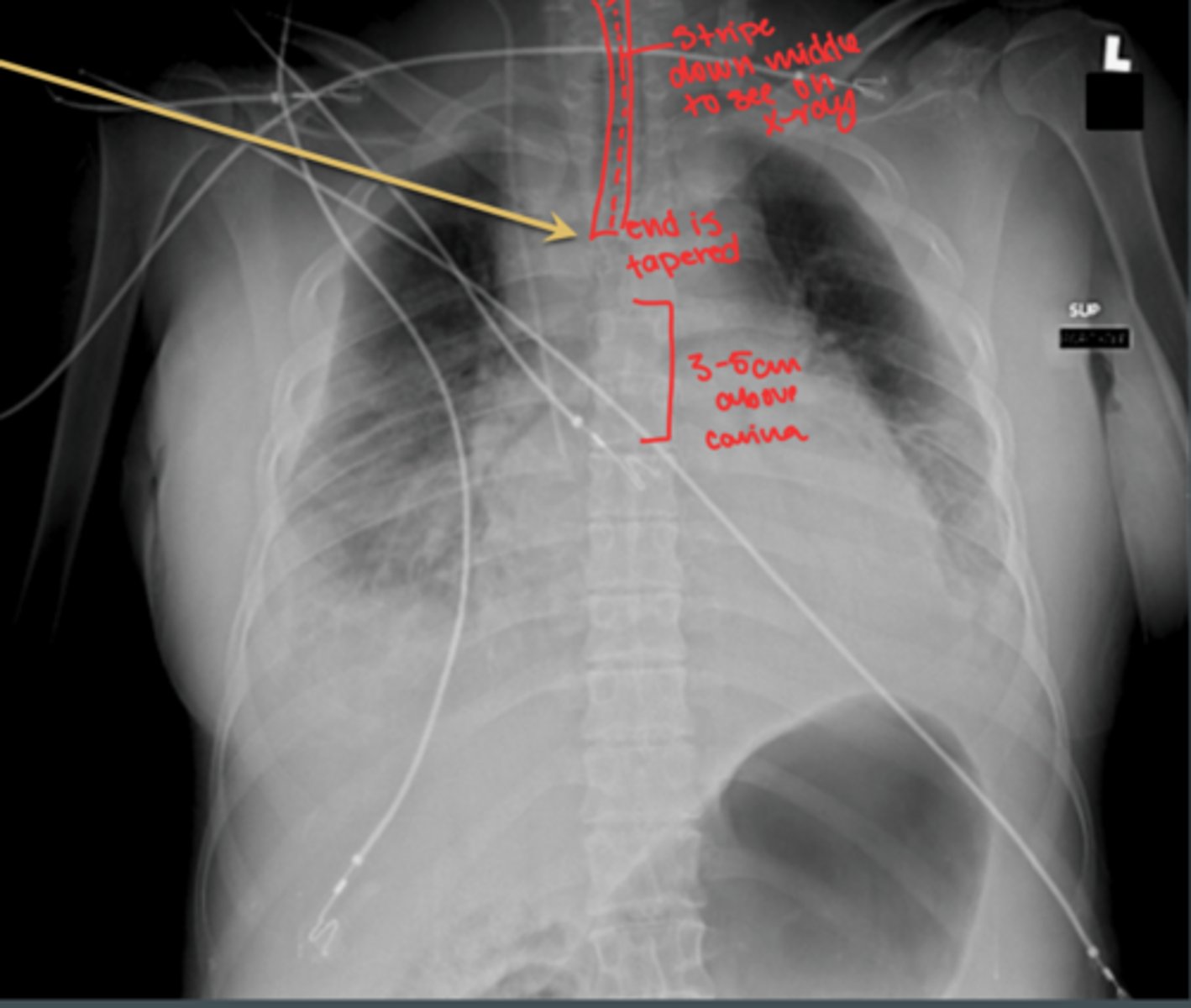
Endotracheal Tube (ETT)
inserted through mouth or nose
emergency situations for short term breathing
can have rattling noise: notify nurse
RN may suction
Pathway: reach 3-5cm proximal to carina
What happens if ETT gets inserted too far?
goes down right lung, only that side receives air
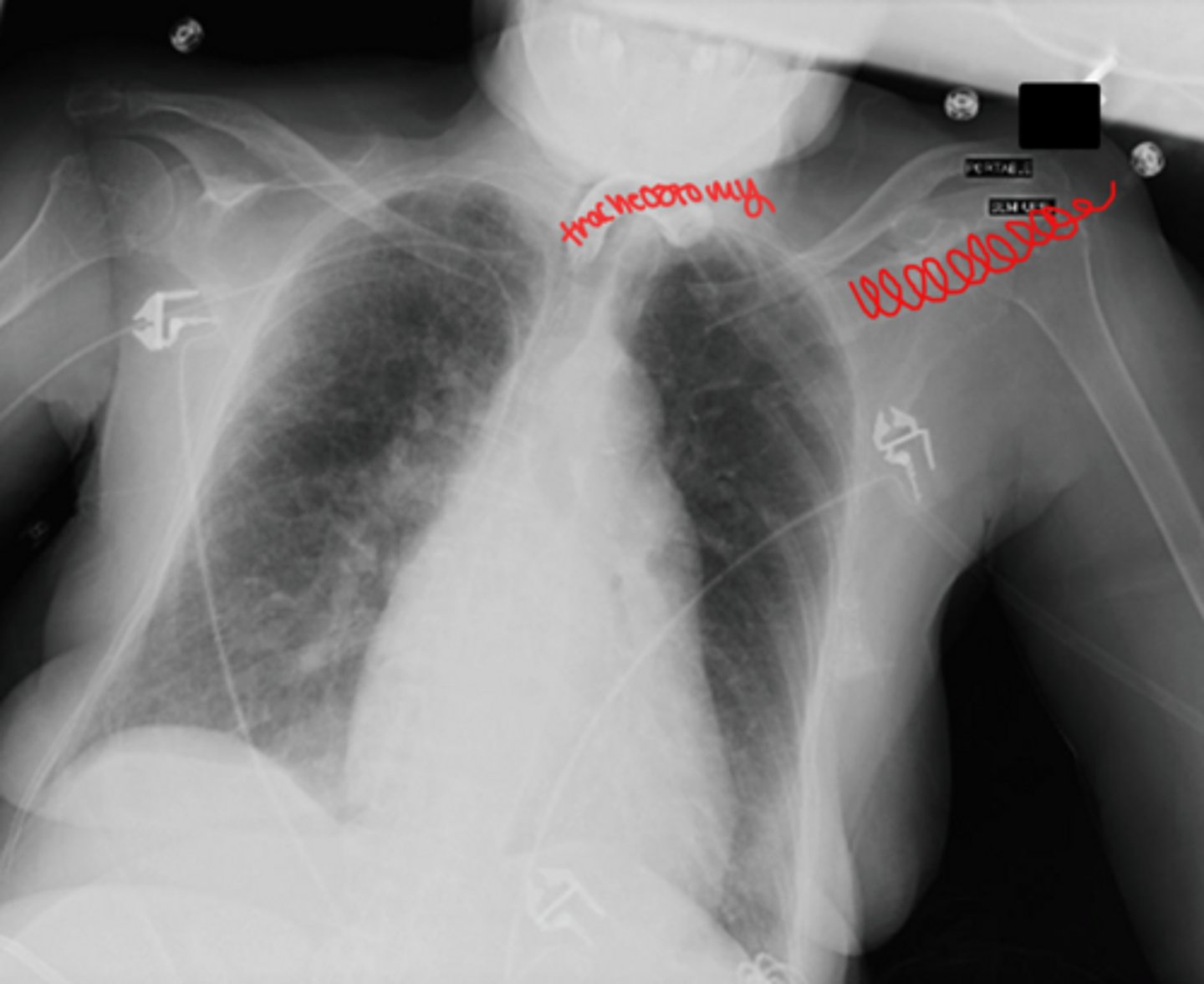
Tracheostomy
surgical creation of an opening into the trachea through the neck
Pathway: ends halfway between stoma and carina (level of T3)
long term
Carina
Point at which the trachea bifurcates (divides) into the left and right mainstem bronchi
What to do if ETT or tracheotomy tube are dislodged?
immediate code
Ventilator
partial or complete mechanical breathing
DO NOT disconnect
Why do ventilator tubing have corrugated appearance?
to prevent collapse of tube when breathing
What to do if ventilator disconnection alarm sounds?
promptly reattach
Time exposures with breathing cycle of ventilator when taking x-rays
Chest x-ray: full inspiration
Abdomen: full expiration
Ventilator tubing; tracheostomy x-ray
Chest tube
used when lung collapses away from chest wall
large diameter tube inserted into pleural space to drain air or fluid, allowing lung to re-inflate
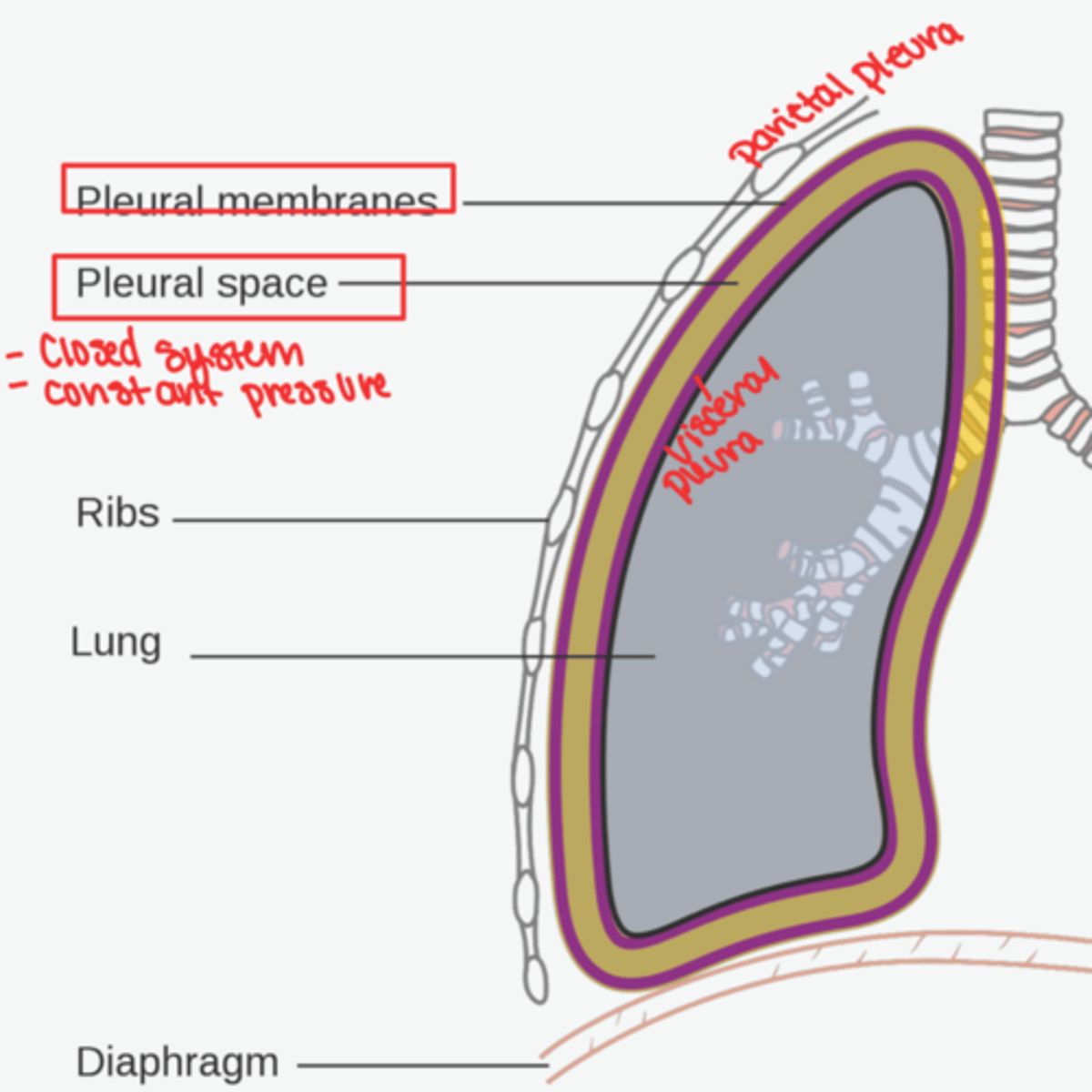
what causes a lung to collapse
air or fluid in the pleural space
pneumothorax
air in the pleural cavity
hemothorax
blood in the pleural cavity
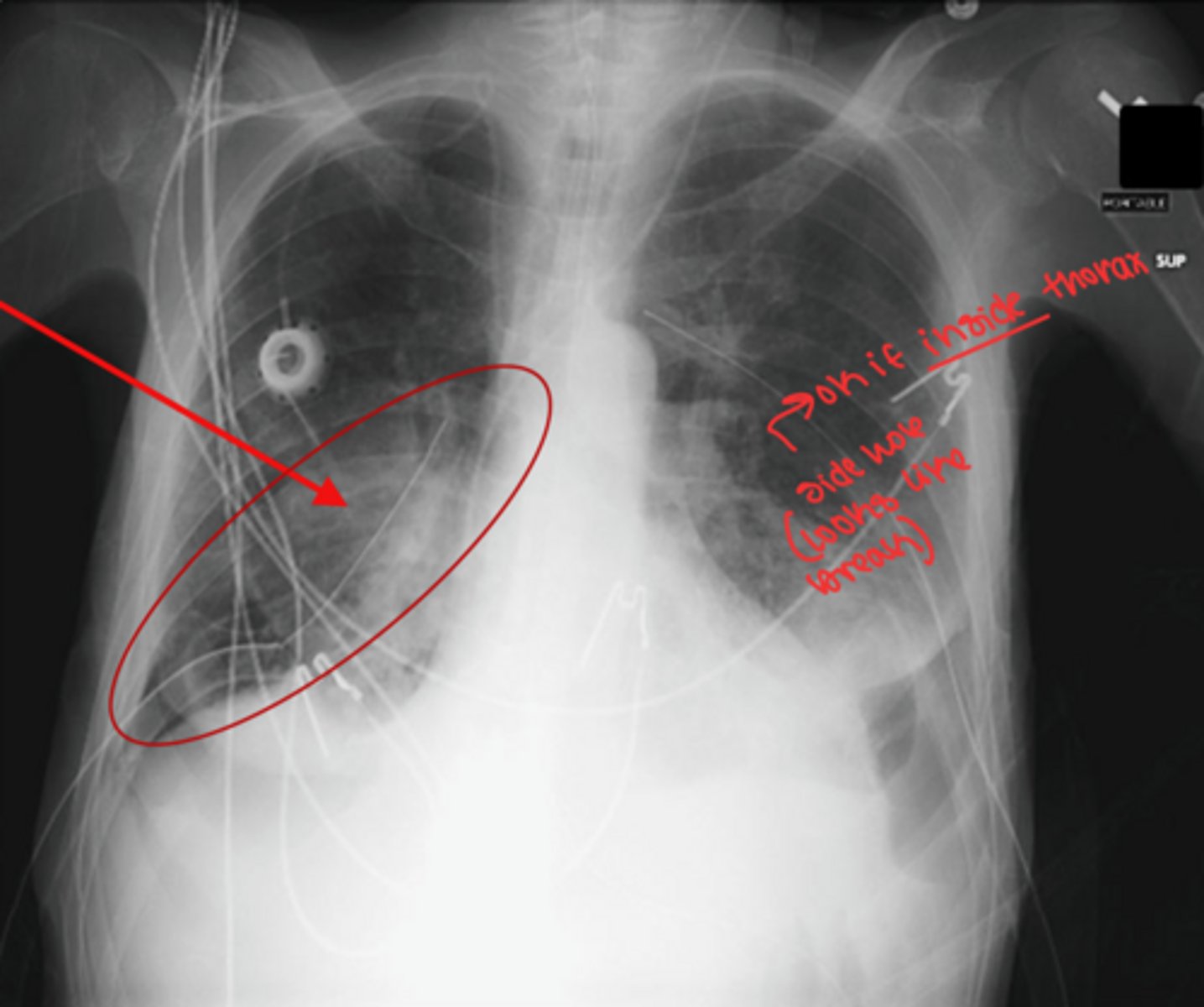
where to insert chest tube
upper thorax if for collapsed lung
lower thorax if for draining fluid
Chest tube precautions
1) KEEP drainage collector lower than chest level
2) DON'T tip drainage collector
3) AVOID tension on tubing
4) COVER if seal is broken, cover puncture site with airtight seal
How to locate chest tube on xray
start looking on outside of body and trace it in and up
Central venous lines
more permanent and travel longer distances than IVs
PICC line (peripheral inserted central catheter)
type of central venous line
placed near heart (SVC)
Purpose of PICC line
administer medication
long term IV therapy
chemo
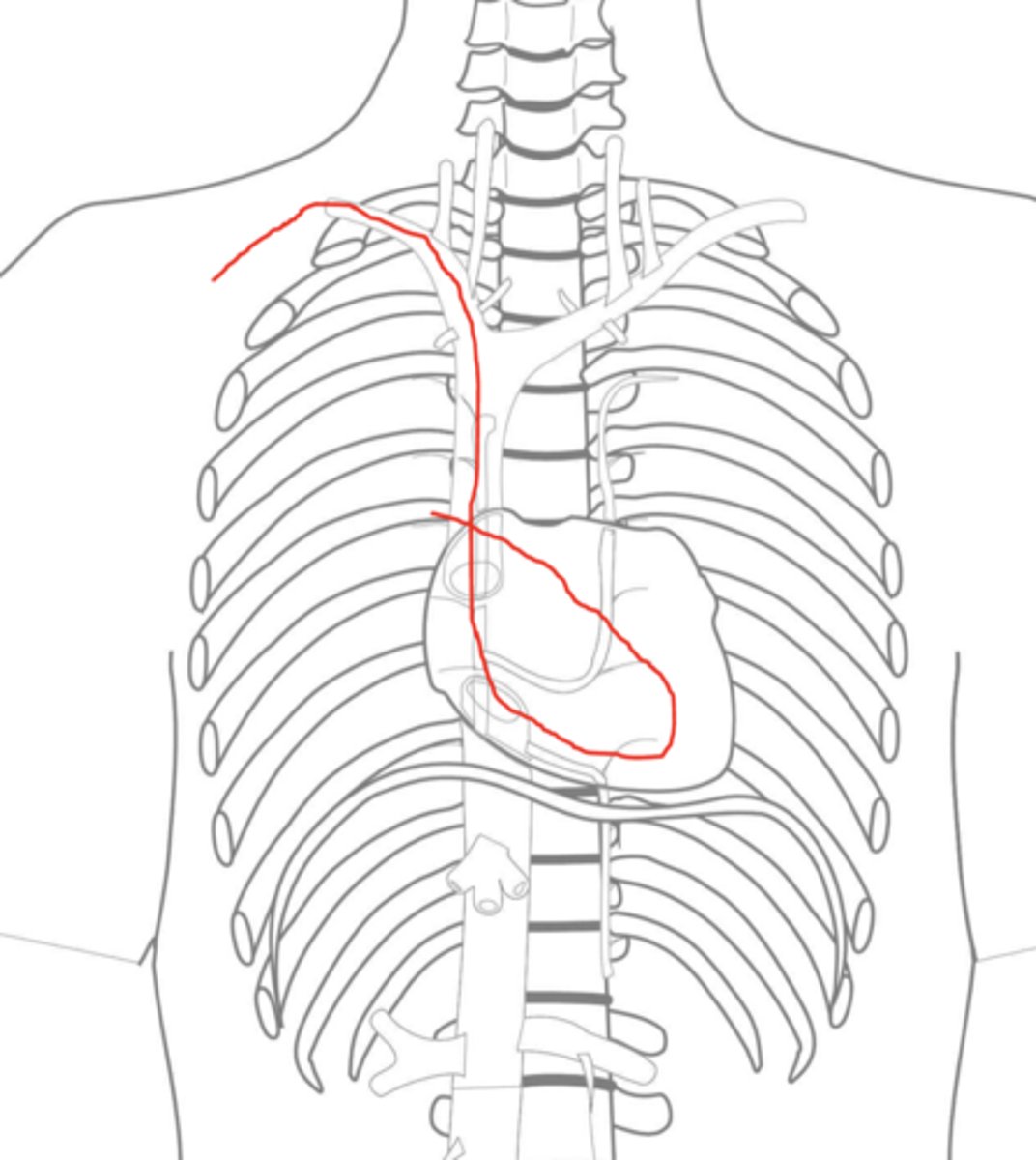
PICC line pathway
ends at SVC, just superior to right atrium
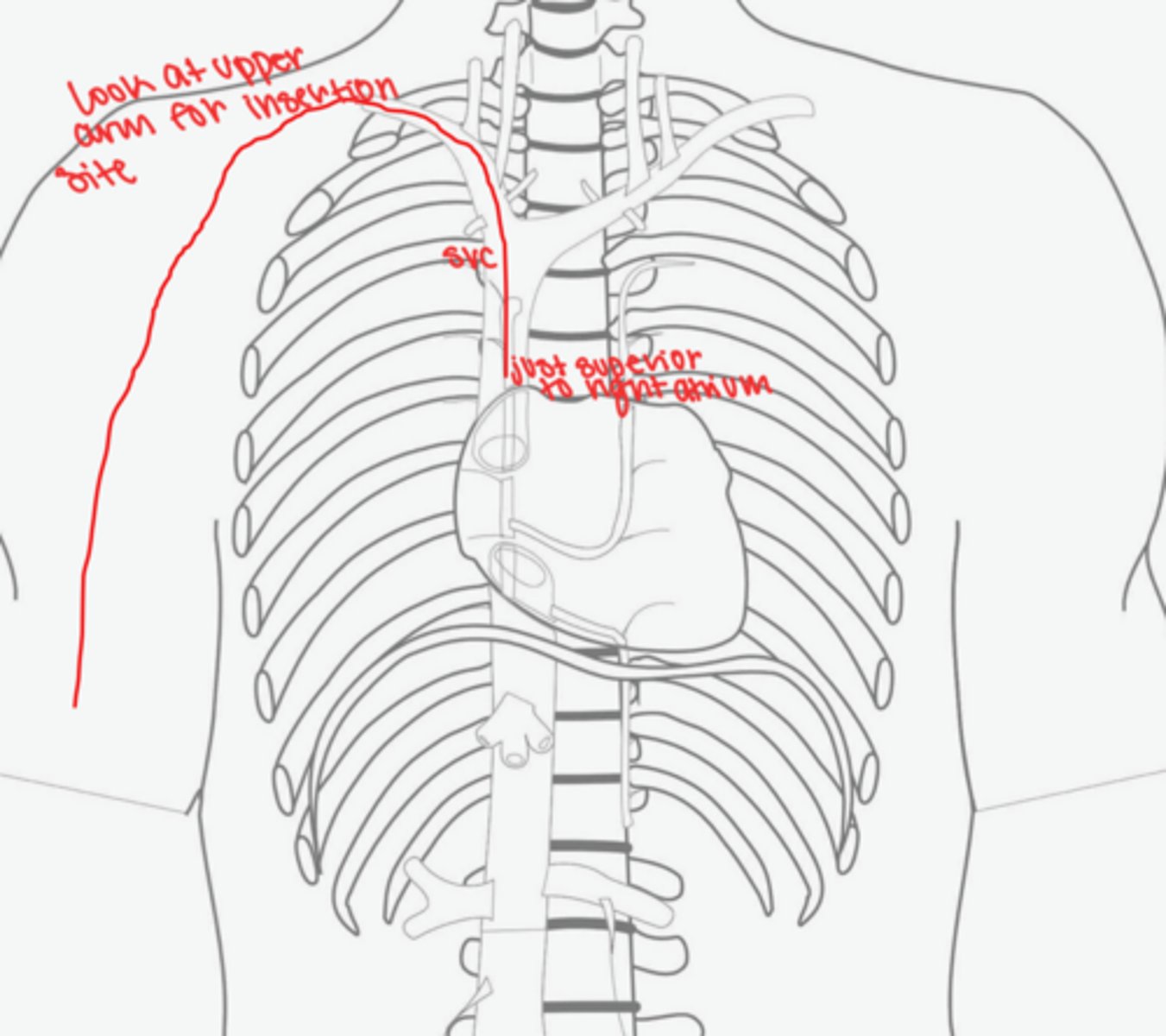
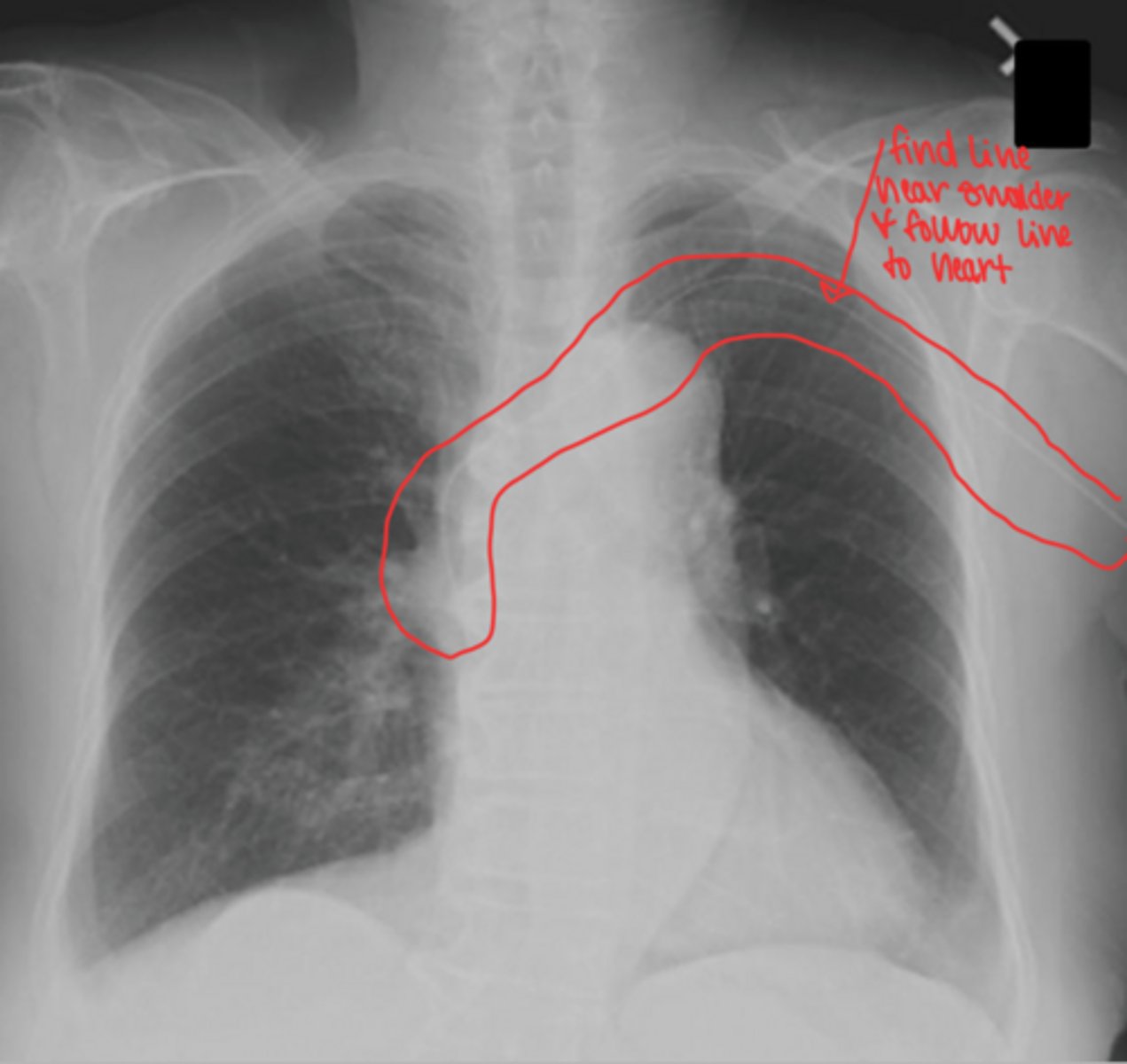
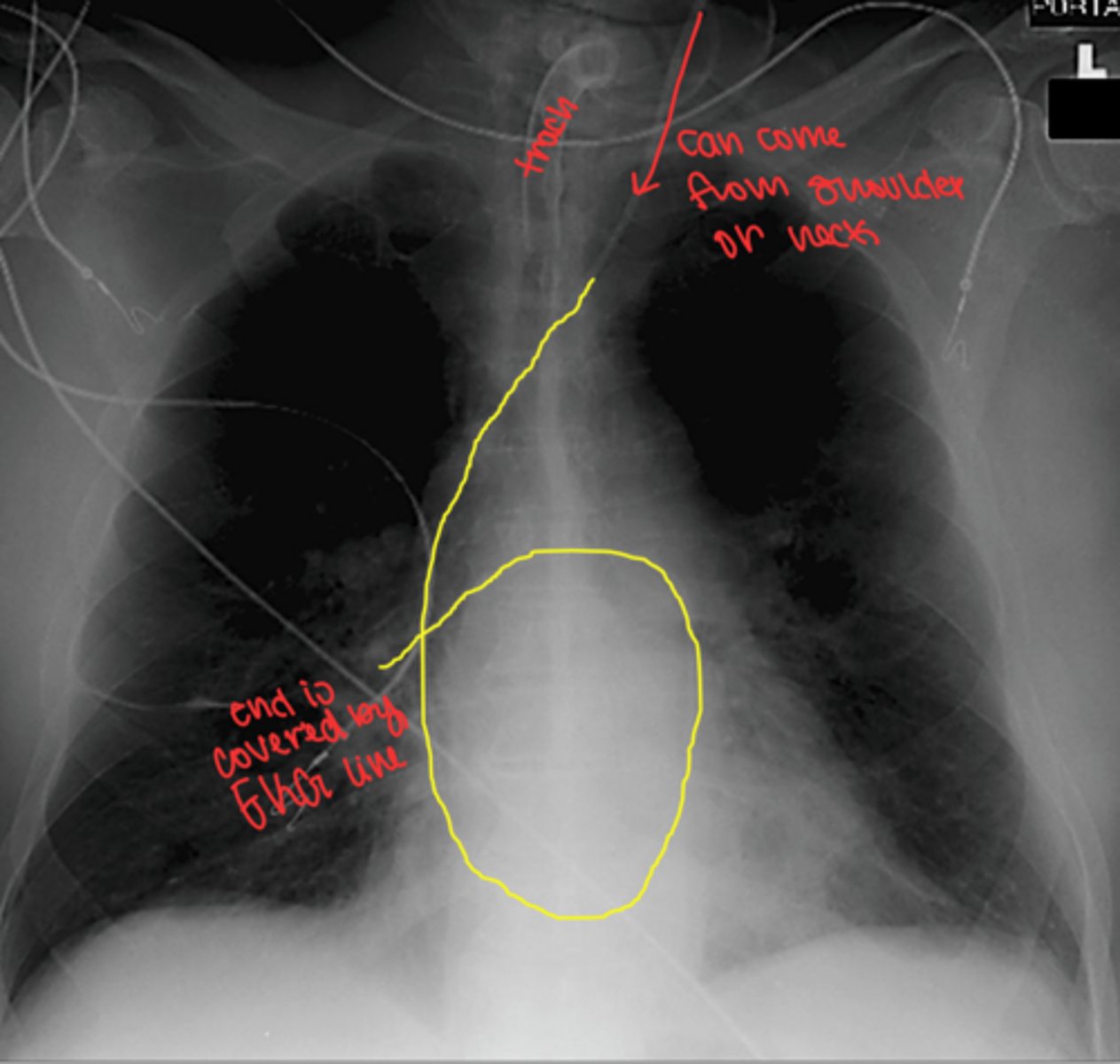
How to trace PICC line
find line near shoulder and follow line to the heart
PICC lines pre-manipulation and direction
don't pre-manipulate image because it prevents radiologist from manipulating it themselves
make sure line goes to SVC and not up towards the brain
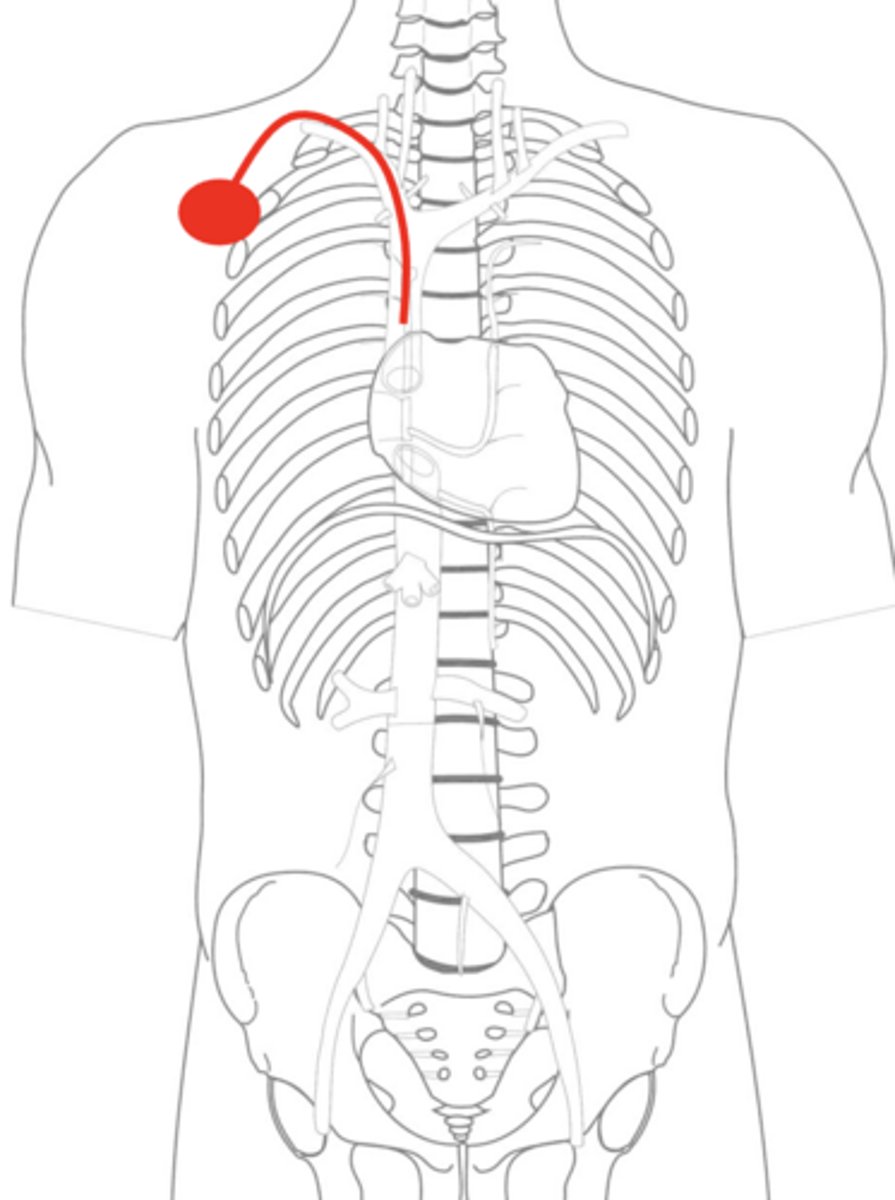
Portcath
long term IV therapy, chemotherapy
preserves vessel puncture site
surgically placed
may be used in CT for contrast injections
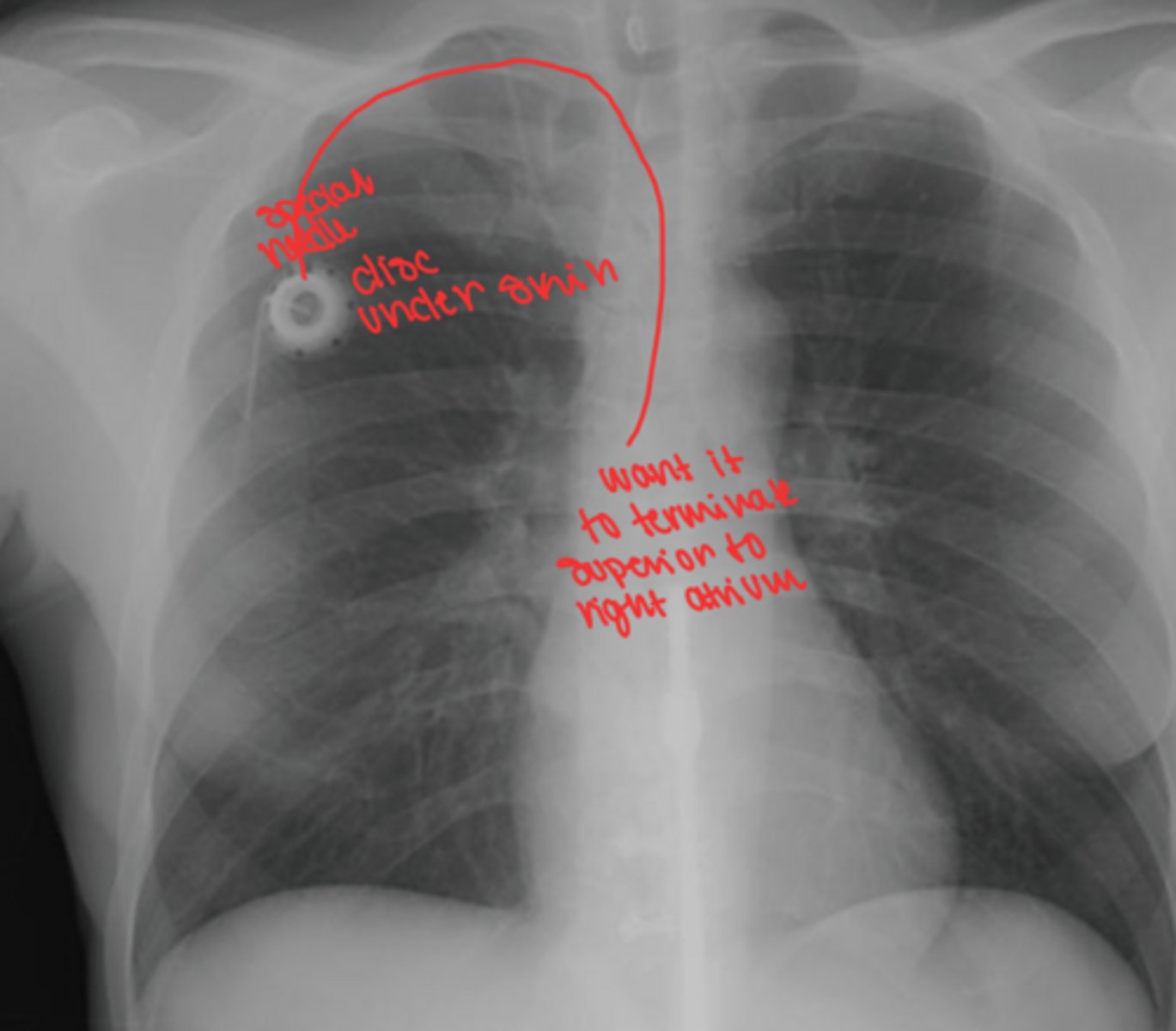
Portcath important locations
special diaphragm disk under skin
special right angle needed to puncture diaphragm
Portcath Pathway
ends just superior to right atrium
Portcath x-ray
Swan Ganz line
only line to go into artery
multiple lumen line
Swan Ganz line purpose
blood gas sample
pressure reading
administer meds
Swan Ganz line pathway
subclavian vein -> SVC -> RA -> RV -> pulmonary artery
ends just past entrance of right pulmonary artery
Pulled central venous line or PICC
patient in steep left lateral trendelenburg position (on left side and drop head down, which keeps air on right side of heart)
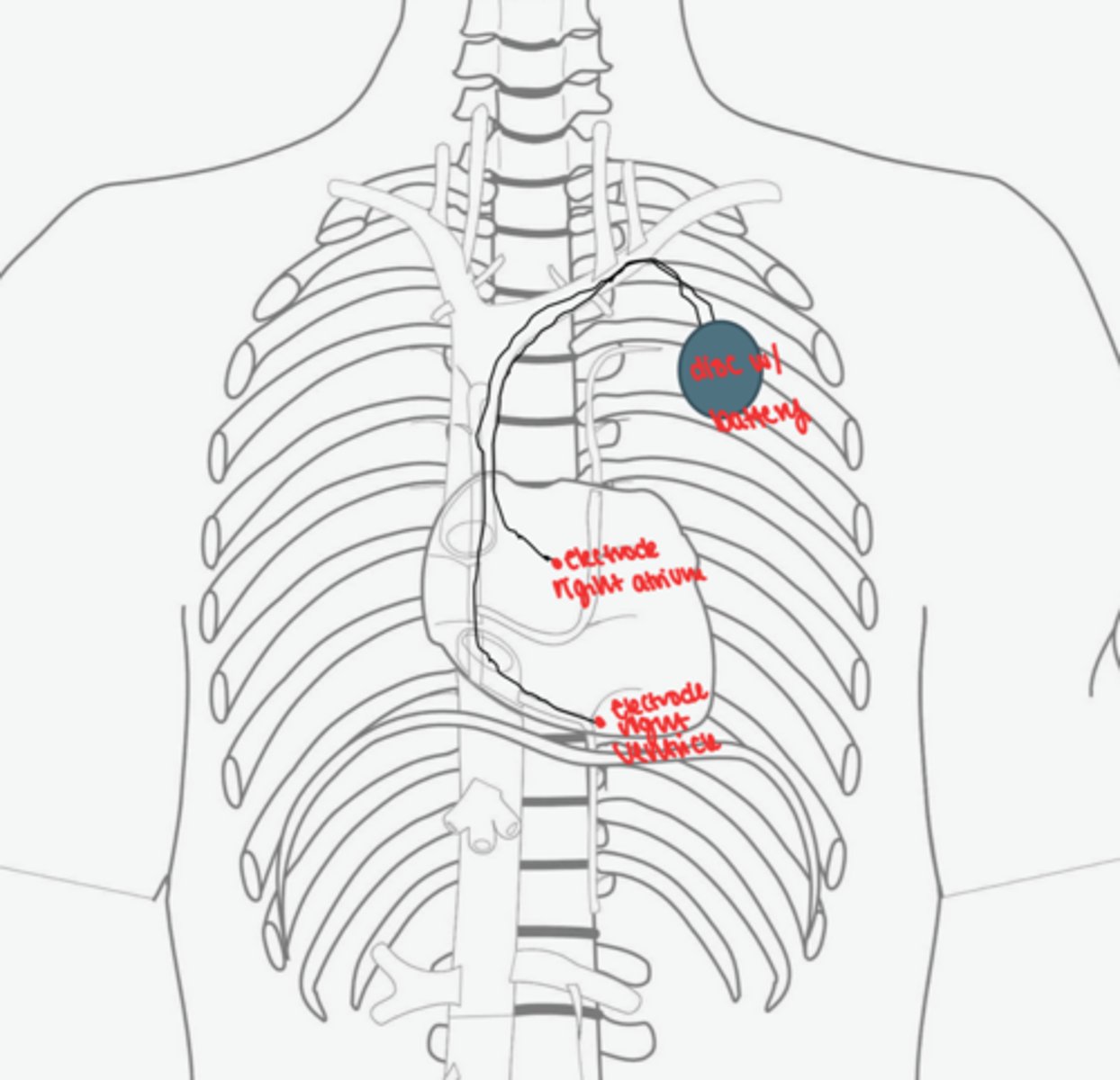
Pacemakers
keep heart beating
temporary or permanent
often 2 electrodes (RA and RV)
x-ray after surgery to ensure correct placement
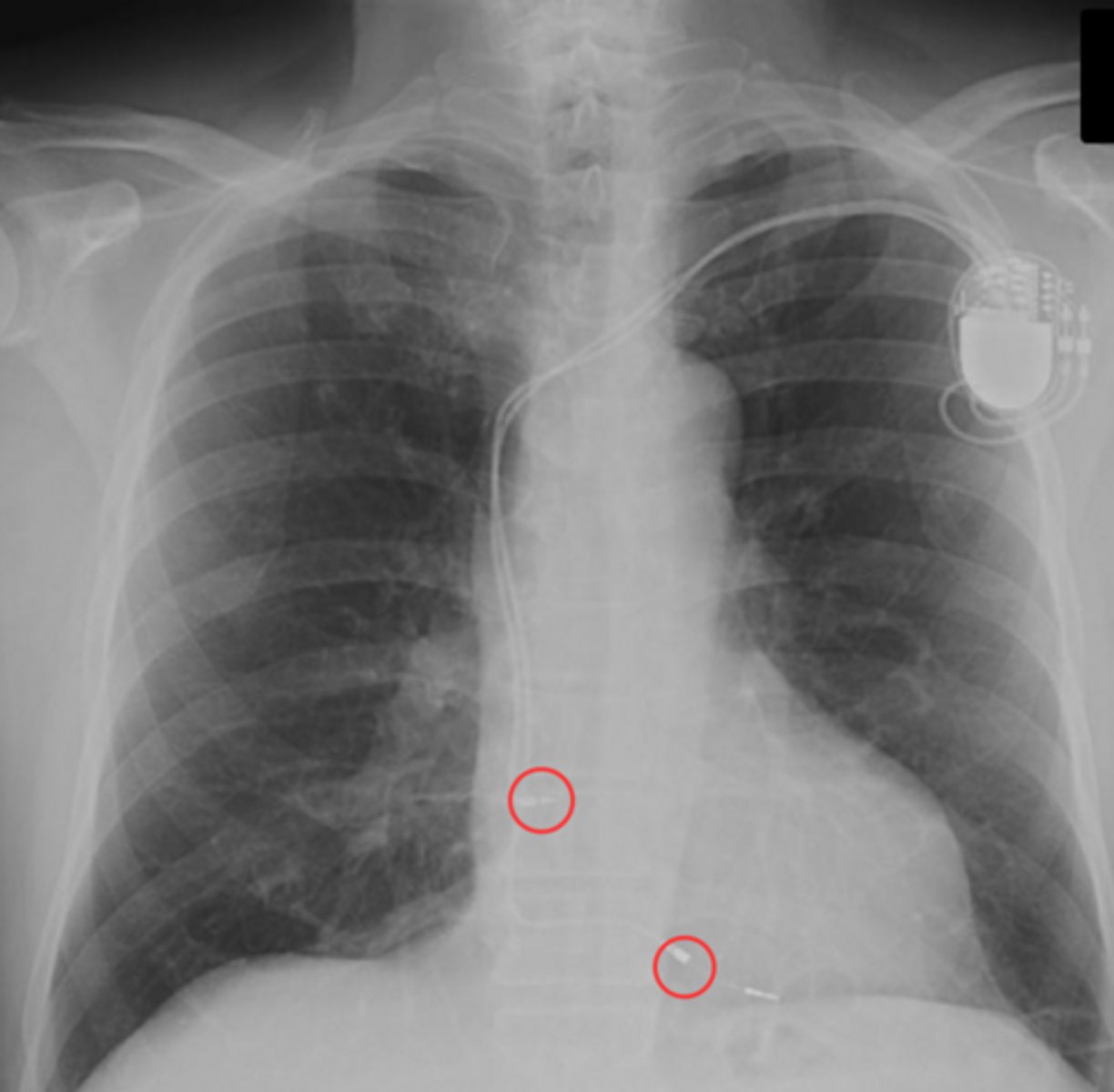
Pacemaker pathway
subclavian vein -> SVC -> RA -> RV -> electrode wedged agains RV wall
automatic implantable cardioverter-defibrillator (AICD)
doesn't fire at all times like pacemaker
corrects arrhythmias
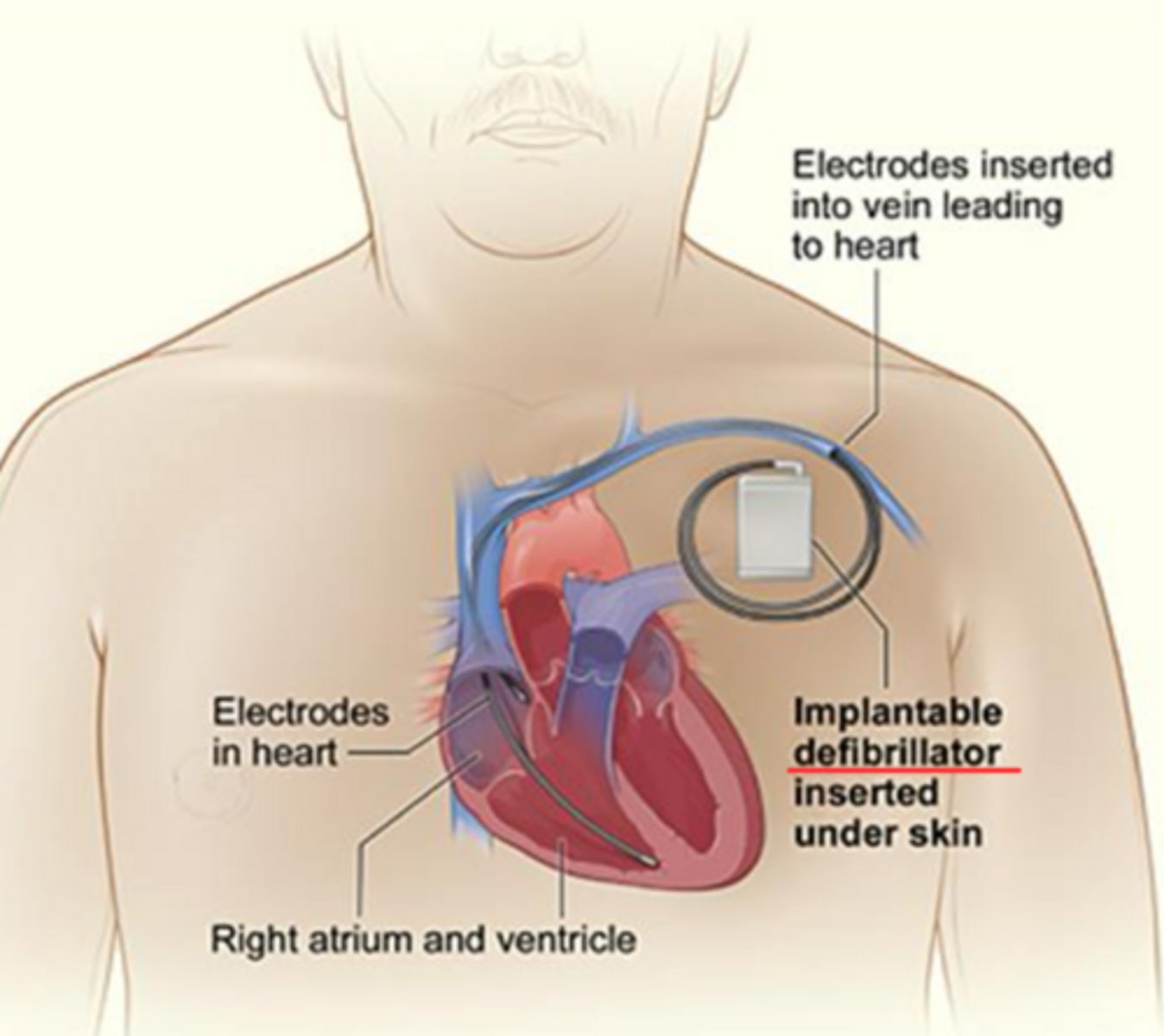
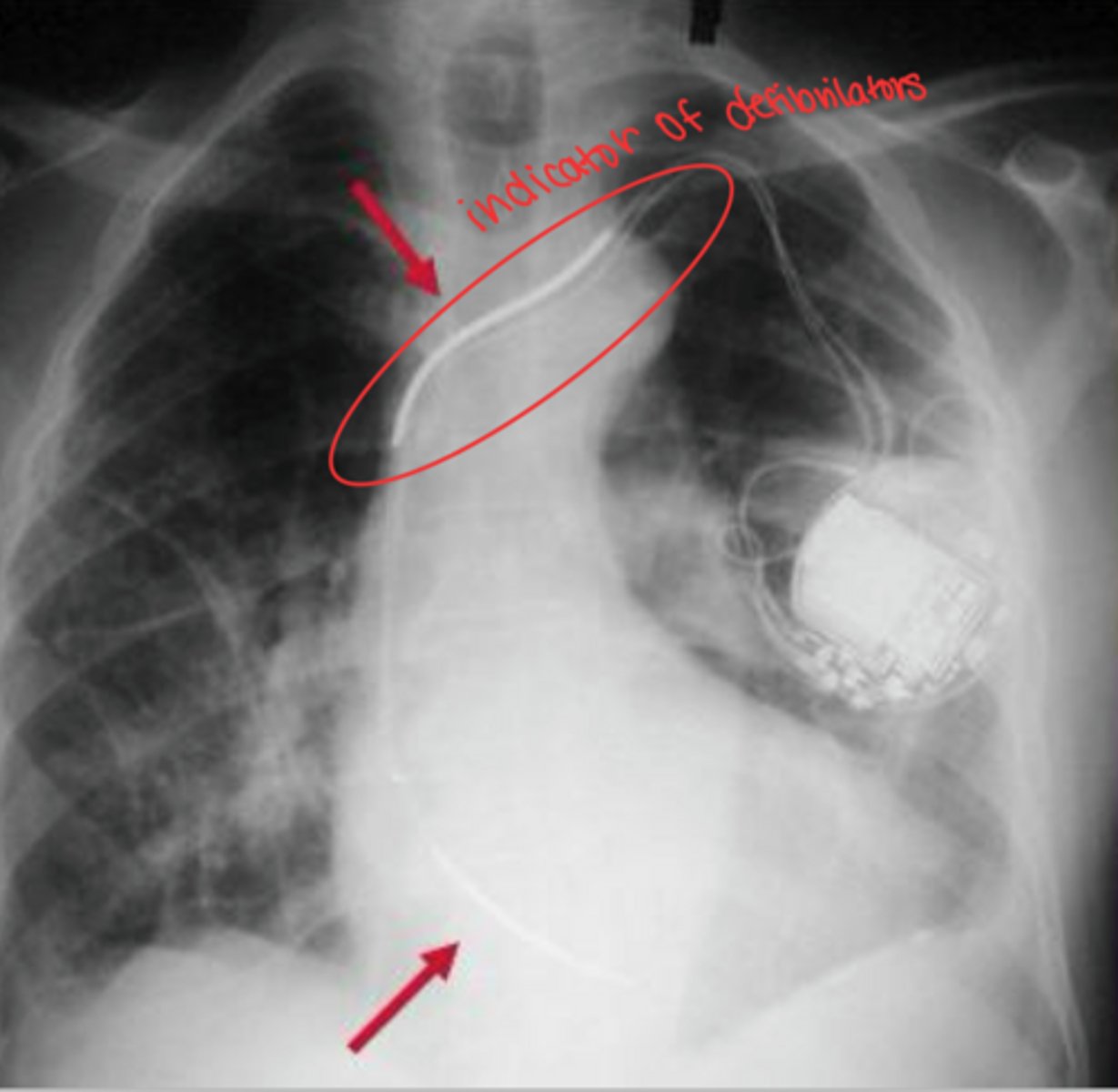
AICD on image
most defibrillators only have one electrode
1) one electrode in SVC or brachiocephalic vein
2) if second is used, apex of RV
Intra-aortic balloon pump (IABP)
temporary treatment used when heart fails b/c working too hard
reduce workload on heart to help heart heal
allows more blood in coronary artery to help heart rest