2026 NAPLEX Renal and Hepatitis/Liver Disease
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
Common Causes of Renal Disease
- uncontrolled DM
- HTN
Types of AKI
Pre-renal:
Intrinsic:
Pre-renal: volume depletion (e.g. dehydration) , presents with BUN:SCr ration >20:1
Intrinsic: caused by tubular damage
Functional unit of the Kidneys
Nephron
Afferent arteriole delivers ___ into the ___
blood
glomerulus
Small molecular weight substances (most drugs), pass through glomerular capillaries into filtrate and are ___
excreted in the urine
Larger substances (e.g. albumin, protein-bound drugs) are not filtered in glomerulus, stay in the blood and exit via the ___
efferent arteriole
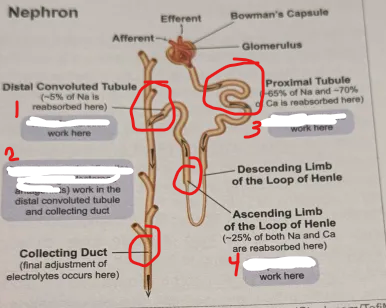
The first place the filtrate travels after exiting the glomerulus is the ____ ____.
Proximal tubule
At the proximal tubule ____, ___, and ___ are ____
Na, Cl, Ca ; reabsorbed
What is blood pH regulated by
exchanged hydrogen and bicarbonate ions
As the filtrate moves through descending limb of loops of Henle, ____ is reabsorbed back into blood, ____ and ____ ARE NOT
H20 ; Na and Cl ARE NOT
As filtrate moves through ascending limb of loop of Henle,
Na and Cl are reabsorbed, but water is NOT (unless ADH or vasopressin is present)
Thiazides
Potassium-sparring diuretics (including aldosterone antagonists)
SGLT-2 inhibitors
Loops
Recognize electrolyte changes associated with different diuretics (i.e. potassium, magnesium, calcium).
Thiazides:
(-)
(+)
Loops:
(-)
(+)
Potassium sparring:
Loops:
(-) K/Mg, Na, Ca
(+) uric acid
Thiazides:
(-) Na, K/Mg
(+) Ca, glucose, uric acid
Potassium sparring: Hyperkalemia, hyper uricemia
Loop diuretics MOA
Inhibit Na/K/Cl in the ascending loop → decreasing Na reabsorption into blood, less water is reabsorbed, and less Ca is reabsorbed *(can lead to hypocalcemia and loss of bone density long-term)*
Thiazide Diuretics MOA
inhibit Na-Cl pump in distal convoluted tubule, increasing Ca reabsorption *(protective to bones long-term)*
Potassium-sparing Diuretics MOA
work in DCT and distal convoluted tubule to ↓ Na and H20 reabsorption and ↑ K reabsorption
Drugs that are Nephrotoxic
abx (5)
immunosuppressant (2)
other (3)
Aminoglycosides, Amphotericin B, Cisplatin, Polymyxins, Vancomycin
Cyclosporine, Tacrolimus
Loop diuretics (due to excessive vol loss), NSAIDs, Radiographic contrast dye
BUN
increases as kidney function declines
Scr normal range
0.6-1.3 mg/dL ; as GFR declines, SCr increases
Accuracy of Cockgrauft-Gault Equation decreased when ___
LOW muscle mass
*over-estimates CrCl*
When is Cockgrauft-Gault Equation not preferred
- young children
- ESRD or unstable renal function
- very low muscle mass patients
CKD Confirming Criteria
presence of either for ≥ 3 months:
1. eGFR < 60 mL./min
2. Albuminuria (AER ≥ 30 mg/24 hours)
Medications for Delaying Progression of CKD
1___ or ___
(3 pearls)
2. if eGFR _____, use SGLT-2 inhibitor
3. if eGFR_____, use finerenone in patients with (1)_____ and (2) _____, and max (3) _____ and ____
1. ACE or ARB
expect initial up to 30% inc SCr ; do NOT stop
SCr and K monitored 2-4 weeks after initiation
avoid potassium and salt substitutes
2. if eGFR ≥ 20 mL/min, use SGLT-2 inhibitor
3. if eGFR ≥25 mL/min, use finerenone in patients with persistent albuminuria and TD2M on max ACE/ARB and SGLT-2 already
ACE/ARB's help Albuminuria by inhibiting _______, results in efferent arteriolar _____which reduces glomerulus pressure and decreases filtration of albumin into urine
inhibit RAAS (production/activity of angiotensin II) ; dilation
Select Drugs that are Contraindicated in CKD
CrCl <60: _____
CrCl <50: TDF-containing HIV treatment (e.g. _____, _____, _____) and _____IV (d/t vehicle)
CrCl <30: TAF-containing HIV treatment (e.g. _____, _____, _____, _____, _____), _____, _____, _____
GFR <30: _____
others: _____
CrCl <60: Nitrofurantoin
CrCl <50: TDF-containing HIV treatment (e.g. Complera, Delstrigo, Stribild) and voriconazole IV (d/t vehicle)
CrCl <30: TAF-containing HIV treatment (e.g. Biktarvy, Descovy, Genvoya, Symtuza, Odefsey), NSAIDS, Dabigatran, potassium-sparing diuretics
GFR <30: metformin
others: meperidine
Select Drugs that Require ↓ Dose or ↑ Interval in CKD that Increase Risk of ADE d/t ↓ Clearance
Anti-infectives
- _____, _____, _____, _____, _____, _____
Cardiovascular Drugs
- _____, _____
GI Drugs
- _____
Other
- _____, _____, _____
Anti-infectives
- aminoglycosides, beta-lactams (except nafci/oxacil and ceftriax), fluconazole, NRTI's, quinolones, vancomycin
Cardiovascular Drugs
- anticoagulants, anti-arrythmics (dofetalide, sotatol, digox)
GI Drugs
- H2RA's (famotidine), metaclopramide
Other
- bisphosphonates, lithium, PDE-5 inhibitors
Key Monitoring Parameters for CKD (4)
PTH, phosphorus, Ca and vitamin D levels
Hyperphosphatemia contributes to elevated ___ levels and must be treated by restricting ___ - containing foods
PTH levels
phosphorus
Phosphate Binders
MOA:
Drugs:
MOA: block absorption of dietary PO4 by binding it in intestine
Drugs: aluminum-based (e.g. aluminum hydroxide), calcium-based (e.g. calcium acetate) and aluminum/calcium-free products (e.g. sevelamer)
Phosphate Binders: Aluminum hydroxide
ADE:
ADE: aluminum intoxication
Phosphate Binders: Calcium Acetate / Calcium Carbonate
Brand Name:
ADE:
Notes:
Brand Name: Calphron / Tums
ADE: Hypercalcemia, constipation
Notes: hyperCa more likely with vitamin D usage
Which class of phosphorus binders is most expensive, but has least ADE/toxicity risk
Aluminum and calcium free products (e.g. Lanthanum and sevelamer)
Phosphate Binders: Ferric citrate
Brand:
Warnings:
Brand: Auryxia, velphoro
Warnings: iron absorption can occur with ferric citrate
Phosphate Binders: Lanthanum carbonate
Brand:
ADE:
Notes:
Brand: Fosrenal
ADE: N/V, diarrhea, constipation
Notes: must chew tablet thoroughly
Phosphate Binders: Sevelamer carbonate/HCl
Carboante Brane Name:
HCl Brand Name:
ADE:
Notes:
Carboante Brane Name: Renvela
HCl Brand Name: Renagel
ADE: N/V, diarrhea
Notes: can lower total cholesterol and LDL
Separate phosphate binders from what drugs?
Levothyroxine, quinolones and tetracyclines
Vitamin D deficiency in CKD occurs when the kidneys cannot hydroxylate via D to final active form ___
1,25-dihydroxy vitamin D
Vitamin D3 (cholecalciferol)
Produced in the skin by UV light
Vitamin D2 (ergocalciferol)
vitamin D derived from plants in the diet
vitamin D analogues should be reserved for stage
4 and 5 of CKD
vitamin D analogues effets on calcium reabsorption and PTH
↑ calcium reabsorption and ↓ in PTH
Cinacalcet can inhibit
PTH release
Vitamin D analog: Calcitriol
Warnings:
Notes:
Warnings: hyperCa
Notes: calcitriol is the active form of vitamin D3
Calcimimetics: Cinacalcet
Brand Name:
Warnings:
Brand Name: Sensipar
Warnings: hypoCa
Calcimimetics: Etelcalcetide
ADE:
ADE: muscle spasms, parasthesia
Primary Problem of Anemia in CKD
lack of EPO's
-epoetin or dabepoetin ; risks = HTN, DVT/PE, only initiate if _____ and d/c if _____ , only work if adequate IRON storage
Hgb < 10 g/dL ; Hgb>11
Drugs that raise K Levels (4)
Canagliflozin
Drospirenone-containing OC's
Calcineurin inhibitors
Bactrim
SE of high K
muscle weakness, bradycardia, fatal arrhythmias
K-Binders: SPS
Warnings:
Notes:
Warnings: GI necrosis
Notes: bind other oral meds
K-Binders: Patriomer
Warnings:
ADE:
Notes:
Warnings: hypoMg
ADE: constipation
Notes: binds oral drugs, separate by at least 3 hours
Separate Lokelma from other drugs by ___ hours
2 hours
Monitor what with Drugs that replace Bicarb in CKD
sodium levels
As CKD progresses, bicarbonate elimination is ____
ENHANCED leading to metabolic acidosis
Characteristics of Drugs that are More Likely to be Removed During Dialysis
- small molecules
- small Vd
- low protein-bound drugs
- higher dialysis blood flow rates
- high-flux and high-efficiency HD filters
Normal Phos levels
2.5-4.5 mg/dL