GW BGZ2026 Case 4 - In the hepatologist´s practice
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
How are carbohydrates (especially glucose, galactose, and fructose) absorbed in the intestine?
Carbohydrate uptake occurs in a highly coordinated transporter system in the small intestine:
Glucose & galactose uptake
Via SGLT1 (Sodium-Glucose Linked Transporter 1)
Uses Na⁺ gradient (secondary active transport)
Allows absorption even against glucose gradient
Fructose uptake
Via GLUT5
Facilitated diffusion (no energy required)
Exit into bloodstream
All monosaccharides leave enterocytes via GLUT2
Enter portal circulation → liver first-pass metabolism
Key concept:
Intestinal absorption is transporter-specific and energy-dependent (for glucose/galactose) but passive for fructose
How is glucose transported in blood and stored in the body?
Glucose transport and storage are highly regulated to maintain blood glucose homeostasis:
Transport in blood
Glucose is freely soluble in plasma
Does NOT require carriers in blood (unlike lipids)
Storage forms
Glycogenesis (glycogen synthesis):
Liver → maintains blood glucose levels between meals
Muscle → local energy reserve (not released into blood)
Excess glucose fate
Converted into fatty acids (lipogenesis) in liver
Stored as triglycerides in adipose tissue
Key concept:
Glucose is a short-term energy buffer, while fat is long-term energy storage
How are dietary lipids absorbed and transported in the body?
Lipid absorption requires emulsification and packaging due to their hydrophobic nature:
Digestion in intestine
Bile acids emulsify fat droplets
Pancreatic lipase breaks triglycerides → fatty acids + monoacylglycerols
Absorption in enterocytes
Re-esterification → triglycerides reform inside cells
Transport in blood
Packaged into lipoproteins:
Chylomicrons → dietary fat transport
VLDL → liver-derived triglycerides
Delivery to tissues
Lipoprotein lipase (LPL) breaks TG → free fatty acids
Fatty acids taken up by muscle/adipose tissue
Key concept:
Lipids require structural packaging (lipoproteins) for transport in aqueous blood
How is glucose metabolized in glycolysis?
Glycolysis is the cytosolic pathway that converts glucose into energy:
Main purpose
Glucose → pyruvate + ATP + NADH
Key regulatory step
Fructose-6-P → Fructose-1,6-bisP via PFK-1
This is the rate-limiting enzyme
Energy yield
Net: 2 ATP + 2 NADH per glucose
Fate of pyruvate
Aerobic → acetyl-CoA (mitochondria)
Anaerobic → lactate (regenerates NAD⁺)
Key concept:
Glycolysis is fast ATP production, especially important in hypoxia or high demand
How are free fatty acids metabolized (β-oxidation)?
β-oxidation breaks down fatty acids into energy-rich acetyl-CoA units:
Step 1: Activation
Fatty acid → fatty acyl-CoA (ATP-dependent)
Step 2: Transport
Carnitine shuttle via CPT-1 (rate-limiting step)
Step 3: β-oxidation cycle
Each cycle produces:
Acetyl-CoA
NADH
FADH₂
Outcome
High ATP yield after oxidative phosphorylation
Key concept:
Fatty acids are a high-energy, slow-burning fuel source
What is the role of the citric acid (TCA) cycle?
The TCA cycle is the central hub of energy metabolism:
Location
Mitochondrial matrix
Function
Oxidizes acetyl-CoA → CO₂
Energy output per acetyl-CoA
3 NADH
1 FADH₂
1 GTP (ATP equivalent)
Importance
NADH/FADH₂ feed into oxidative phosphorylation → major ATP production
Key concept:
TCA cycle is the final common pathway for carbohydrate and fat metabolism
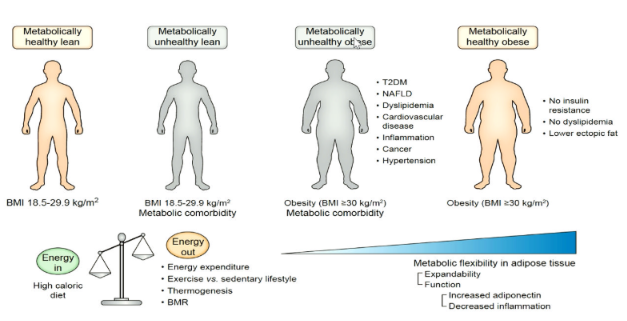
What is ectopic fat and why is it metabolically harmful?
Ectopic fat is lipid storage in non-adipose tissues due to overflow from adipose tissue:
Normal storage site
Adipose tissue (safe triglyceride storage)
Ectopic sites
Liver → fatty liver (MASLD)
Muscle → insulin resistance
Pancreas → β-cell dysfunction
Mechanism of toxicity
Lipid overload → DAGs + ceramides
These interfere with insulin signaling pathways
Clinical consequences
Type 2 diabetes
Metabolic syndrome
NAFLD/MASH
Key concept:
Fat becomes harmful when storage capacity is exceeded
Is dietary fat harmful or beneficial?
The effect of dietary fat depends on type and metabolic context:
Harmful fats
Saturated fats → ↑ LDL cholesterol
Trans fats → inflammation + cardiovascular risk
Beneficial fats
MUFA (olive oil) → improves lipid profile
PUFA (omega-3) → anti-inflammatory effects
Modern understanding
Total energy balance matters more than fat alone
Overnutrition → fat accumulation regardless of source
Key concept:
Dietary fat is not inherently bad—metabolic context determines outcome
How are carbohydrate and fat metabolism integrated?
Carbohydrate and fat metabolism are tightly interconnected energy systems:
Fed state (high insulin)
Glucose → glycogen + fat (lipogenesis)
Energy storage dominates
Fasted state (low insulin, high glucagon)
Fatty acids → β-oxidation
Glucose spared for brain
Metabolic convergence
Both pathways produce acetyl-CoA
Enter TCA cycle for ATP production
Key concept:
Energy metabolism is state-dependent (fed vs fasting) and highly flexible
What are the main causes and risk factors of obesity?
Lifestyle / environmental factors (majority ~60–70%)
Excess calorie intake (energy surplus)
Ultra-processed foods (high sugar/fat, low fiber)
Sugary drinks + large portions
Physical inactivity (low NEAT, sedentary behavior)
Poor sleep / circadian disruption
Stress → emotional eating
“Obesogenic environment” (cheap, available high-calorie food)
Biological / genetic factors (~30–40%)
Polygenic risk (most common)
Rare monogenic obesity (e.g., leptin pathway defects)
Family history
Medical factors
Hypothyroidism, Cushing syndrome
Medications (antipsychotics, corticosteroids, some antidepressants, SSRIs)
key idea: Obesity results from energy imbalance + susceptibility (genetic + biological)
What are the consequences of obesity?
Obesity affects multiple organ systems through insulin resistance and inflammation.
Metabolic
Insulin resistance → type 2 diabetes
Dyslipidaemia (↑ TG, ↓ HDL)
Metabolic syndrome
Cardiovascular
Hypertension
Atherosclerosis
↑ MI and stroke risk
Liver
MASLD → MASH → fibrosis → cirrhosis
Other effects
Sleep apnea, osteoarthritis
Infertility / hormonal changes
Increased cancer risk (colon, breast, endometrial)
Depression and reduced quality of life
Key idea: Obesity is a systemic inflammatory + metabolic disease
How does obesity lead to type 2 diabetes?
Obesity causes insulin resistance, which eventually leads to β-cell failure.
Process
Visceral fat releases FFAs → insulin resistance
Cytokines (TNF-α, IL-6) → inflammation
Muscle ↓ glucose uptake
Liver ↑ glucose production
Progression
Insulin resistance
Hyperinsulinaemia (compensation)
β-cell exhaustion
Persistent hyperglycaemia → T2D
Key idea:
T2D = failure of pancreatic compensation
How are obesity, diabetes, and hypertension linked?
They are different outcomes of the same underlying process: insulin resistance.
Core mechanism
Obesity → visceral fat inflammation
Insulin resistance develops
Effects
T2D: β-cell failure → hyperglycaemia
Hypertension:
↑ sympathetic activity
RAAS activation
Na⁺ retention
Endothelial dysfunction
Key idea:
One disease network = metabolic syndrome
Why is obesity central in metabolic disease?
Obesity is the upstream driver of most metabolic and cardiovascular disease.
Clinical effects
Insulin resistance → T2D
Dyslipidaemia → atherosclerosis
Liver fat → MASLD/MASH
Hypertension → vascular dysfunction
Markers in patients
High BMI + waist circumference
↑ glucose
↑ triglycerides
↑ liver enzymes (ALT/AST)
Key idea:
Treating obesity addresses the root cause of metabolic disease
What is Metabolic dysfunction-associated steatohepatitis (MASH, formerly NASH)?
MASH (Metabolic dysfunction-associated steatohepatitis) is the inflammatory form of MASLD (Metabolic dysfunction-associated steatotic liver disease).
It develops when fat accumulation (≥5% of hepatocytes) is accompanied by:
Hepatocyte injury
Inflammation
Fibrosis (scar formation)
MASH can progress to:
Cirrhosis
Liver failure
Hepatocellular carcinoma
Association
Considered the hepatic manifestation of metabolic syndrome.
Strongly associated with:
Obesity
Type 2 diabetes
Hypertension
Dyslipidaemia
Insulin resistance
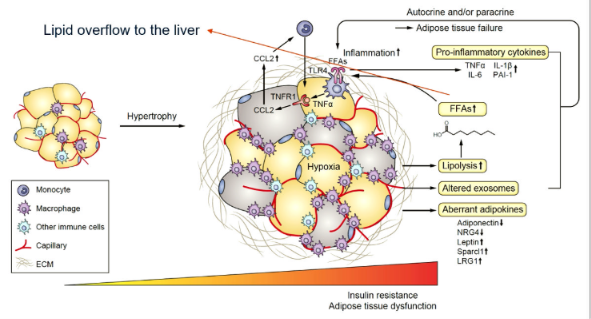
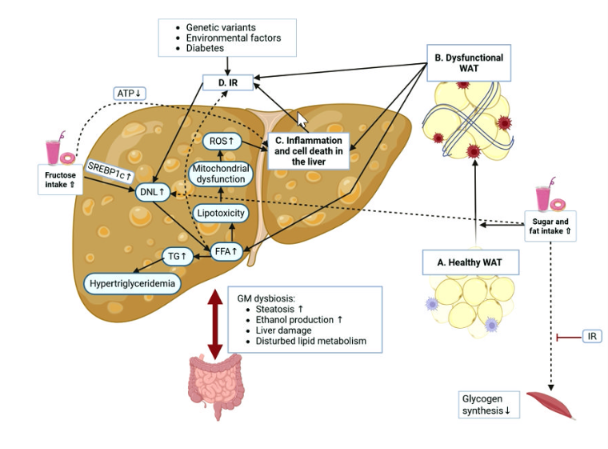
How does MASH develop?
The multiple-hit hypothesis explains that several mechanisms occur simultaneously:
Insulin resistance
Increased lipolysis
More free fatty acids (FFAs) delivered to the liver
Increased de novo lipogenesis
Causes hepatic steatosis
Lipotoxicity
Toxic lipids (ceramides and diacylglycerols) damage hepatocytes
Leads to mitochondrial dysfunction, ER stress and apoptosis
Oxidative stress
Fat accumulation increases ROS production
CYP2E1 further increases ROS
ROS damages DNA, proteins and lipids
Chronic inflammation
Damaged hepatocytes activate Kupffer cells
Cytokines released:
TNF-α
IL-6
IL-1β
Fibrosis
Stellate cells become activated
Produce collagen
Fibrosis may progress to cirrhosis
Gut microbiome
Dysbiosis increases intestinal permeability
LPS enters portal circulation
Further promotes inflammation and fibrosis
Explain the role of CYP2E1 in MASH.
CYP2E1 contributes to oxidative liver injury.
Upregulated in fatty liver disease.
Produces reactive oxygen species (ROS) during fatty acid metabolism.
ROS causes:
Lipid peroxidation
Mitochondrial damage
ER stress
Hepatocyte injury
Key pathway
CYP2E1 → ROS → Oxidative stress → MASH
How does obesity contribute to MASH?
Obesity promotes MASH through several mechanisms:
Causes insulin resistance
Increases release of free fatty acids
Increases liver fat accumulation
Alters the gut microbiome (dysbiosis)
Increases gut permeability
Allows LPS to enter the liver
Promotes chronic inflammation
Reduces adiponectin
Increases leptin, promoting fibrosis
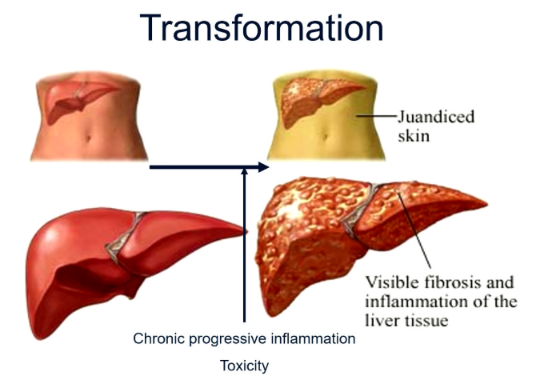
Describe the progression from fatty liver to cirrhosis.
The progression occurs in several stages:
Steatosis
Fat accumulates in hepatocytes.
Steatohepatitis (MASH)
Lipotoxicity
Oxidative stress
Inflammation
Cell death
Apoptosis and necrosis
DAMP release
Fibrosis
Activation of hepatic stellate cells
Collagen deposition
Cirrhosis
Extensive scarring
Nodular liver
Liver failure risk
What are the major risk factors for MASH?
Major risk factors include:
Obesity (especially visceral obesity)
Type 2 diabetes
Insulin resistance
Metabolic syndrome
Hypertension
Hypertriglyceridaemia
Sedentary lifestyle
High-fat and high-fructose diets
Genetic variants:
PNPLA3
TM6SF2
What is metabolic syndrome and its main mechanism?
Metabolic syndrome is a cluster of risk factors driven by insulin resistance and visceral obesity.
Criteria (≥3):
Abdominal obesity
↑ triglycerides
↓ HDL
Hypertension
↑ fasting glucose / T2D
Mechanism
Visceral fat → ↑ FFAs + cytokines (TNF-α, IL-6)
↓ adiponectin → reduced insulin sensitivity
Chronic low-grade inflammation
Effects
Endothelial dysfunction → hypertension
Insulin resistance → T2D
Liver fat accumulation → MASLD/MASH
Key idea: Metabolic syndrome = insulin resistance + visceral fat inflammation
What type of inflammation occurs in metabolic syndrome?
The inflammation is chronic low-grade systemic inflammation.
Characteristics include:
Continuous immune activation
No acute infection present
Increased inflammatory cytokines:
TNF-α
IL-6
IL-1β
MCP-1
This inflammation worsens:
Insulin resistance
Endothelial dysfunction
Atherosclerosis
Liver fibrosis
What are the diagnostic criteria for metabolic syndrome?
Diagnosis requires 3 or more of the following:
Central obesity
Triglycerides ≥1.7 mmol/L
Low HDL cholesterol
Blood pressure ≥130/85 mmHg
Fasting glucose ≥5.6 mmol/L or type 2 diabetes
How is MASH diagnosed?
Diagnosis requires a combination of:
History & Examination
Obesity
Diabetes
Hypertension
Hepatomegaly
Blunt liver edge
Blood tests
ALT
AST
GGT
Ferritin
Glucose
Lipid profile
Imaging
Ultrasound
FibroScan
MRI-PDFF
Fibrosis assessment
FIB-4
NAFLD Fibrosis Score
ELF test
Gold standard
Liver biopsy
What is the significance of ALT and AST in MASH?
ALT
More liver-specific.
Usually higher than AST in early disease.
AST
Found in liver, muscle and heart.
Often becomes higher than ALT in advanced fibrosis or cirrhosis.
Important limitation
ALT and AST cannot distinguish simple steatosis from MASH.
Normal values do not exclude disease.
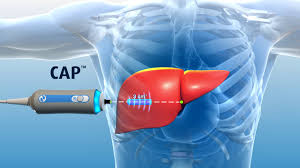
What imaging techniques are used in MASH?
Ultrasound
First-line investigation.
Detects moderate-to-severe steatosis.
FibroScan
Measures liver stiffness.
Estimates fibrosis.
Measures steatosis using CAP.
MRI-PDFF
Most accurate for liver fat quantification.
CT
Can detect fatty liver but is rarely used.
How is type 2 diabetes treated in patients with MASH?
Main medications include:
Metformin
Improves insulin sensitivity.
Reduces hepatic gluconeogenesis.
GLP-1 receptor agonists (e.g. Semaglutide)
Weight loss
Improves insulin resistance
Reduces liver fat
Improves steatohepatitis
SGLT2 inhibitors
Weight loss
Cardio-renal protection
Reduces liver fat
Pioglitazone
Improves MASH histology
May cause weight gain
DPP-4 inhibitors
Weight neutral
Mild glucose lowering
Little benefit for MASH
How do DPP-4 inhibitors work?
Mechanism
Inhibit the DPP-4 enzyme.
Prevent breakdown of:
GLP-1
GIP
This results in:
Increased glucose-dependent insulin secretion.
Reduced glucagon secretion.
Advantages
Low hypoglycaemia risk.
Weight neutral.
Disadvantages
Minimal weight loss.
Little improvement in liver fat or fibrosis.
Why are GLP-1 receptor agonists beneficial in MASH?
GLP-1 receptor agonists:
Increase glucose-dependent insulin secretion.
Reduce glucagon.
Slow gastric emptying.
Increase satiety.
Clinical benefits:
Significant weight loss.
Improved insulin sensitivity.
Reduced hepatic steatosis.
Reduced inflammation.
Lower cardiovascular risk.
They directly target the underlying metabolic dysfunction driving MASH.
What is the cornerstone treatment for MASH?
Weight loss is the cornerstone of treatment.
Benefits include:
≥5% weight loss
Improves steatosis.
7–10% weight loss
Improves inflammation.
Improves hepatocyte ballooning.
≥10% weight loss
May improve fibrosis.
Lifestyle changes include:
Mediterranean diet.
Caloric restriction.
Aerobic exercise.
Resistance training.
What is the role of Vitamin E, Vitamin C and UDCA in MASH?
Vitamin E
Antioxidant.
Reduces oxidative stress.
Improves steatosis and inflammation.
Limited benefit in patients with diabetes.
Vitamin C
Antioxidant.
Regenerates Vitamin E.
Limited evidence for improving MASH.
UDCA
Hydrophilic bile acid.
Protects hepatocytes.
Improves bile flow.
Not recommended as standard treatment because it has not consistently improved MASH histology.
What are the main therapeutic priorities in a patient with MASH?
Treatment aims to address the underlying metabolic dysfunction:
Weight loss (most important intervention)
Improve insulin resistance
Metformin
GLP-1 receptor agonists
Reduce cardiovascular risk
Control blood pressure
Manage dyslipidaemia
Slow liver disease progression
Prevent cirrhosis and liver failure
The overall goal is to reverse steatosis, reduce inflammation, and prevent fibrosis progression.
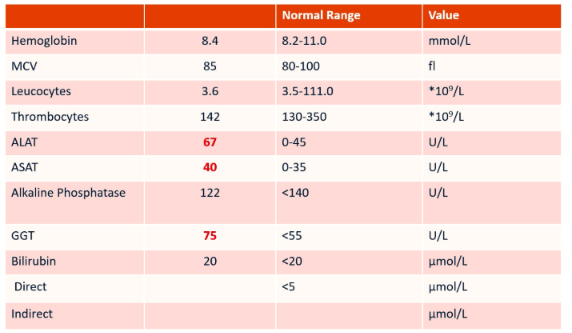
Interpret these liver tests
Enzymes involved in mitochondria in liver.
Serum Transaminases
Hepatocyte damage (viral hepatitis, (N)AFLD, etc.)
Aspartate aminotransferase (AST)
Heart, muscle, kidney, brain
Alanine aminotransferase (ALT)
More liver specific, ALT usually higher than AST (except in alcoholic liver disease)
Cholestatic liver tests
Biliary obstruction (primary billiary cholangitis, bile duct stone/tumor, etc.)
Alkaline phospatase
Bone, liver, (placenta, intestine)
General enzyme
Gamma-glutamyl transpeptidase (G-GT)
Hepatocytes, biliary epithelial cells, kidney, seminal vesicles, pancreas, spleen, heart and brain.
Bilirubin
Think at prehepatic (hemolysis), hepatic, post-hepatic causes (cholestasis)
Liver function tests: INR, albumin and in advanced liver disease also bilirubin
The diagnosis
Alcoholic liver disease (ALD)
Metabolic dysfunction associated steatotic liver disease (MASLD)
What is liver cirrhosis?
Liver cirrhosis is the end stage of chronic liver disease.
Characteristics include:
Progressive fibrosis.
Replacement of healthy liver tissue with scar tissue.
Distortion of normal liver architecture.
Reduced liver volume.
Vascular remodeling leading to portal hypertension.
Complications include:
Liver failure
Portal hypertension
Ascites
Variceal bleeding
Hepatocellular carcinoma
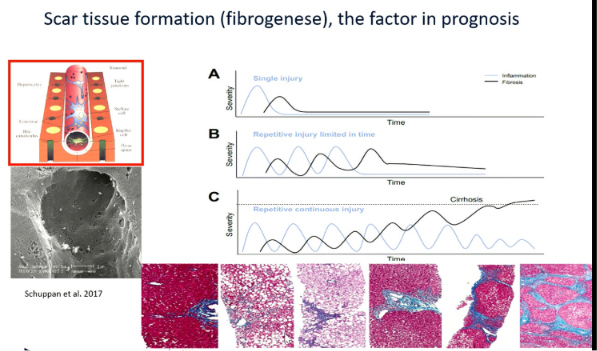
How does fibrosis develop?
Fibrosis develops following repeated liver injury.
The process involves:
Chronic hepatocyte injury.
Activation of hepatic stellate cells.
Transformation into collagen-producing myofibroblasts.
Progressive deposition of connective tissue.
Development of cirrhosis if injury continues.
What are the Milan criteria for liver transplantation in hepatocellular carcinoma?
Patients qualify if they meet all of the following:
One tumour ≤5 cm, or
Up to three tumours, each ≤3 cm
No vascular invasion
No extrahepatic metastases
Meeting these criteria gives good post-transplant survival.
What are the requirements for orthotopic liver transplantation (OLT)?
Patients should have:
No alcohol use for at least 6 months
HCC within Milan criteria
Good physical condition:
No severe obesity
No sarcopenia
No chronic infection
No active viral hepatitis
How does the Western lifestyle contribute to MASLD?
The Western lifestyle promotes obesity and insulin resistance through:
High-calorie diets.
Excess carbohydrates.
High saturated fat intake.
High fructose consumption.
Processed foods.
Low fibre intake.
Low antioxidant intake.
Alcohol consumption.
Physical inactivity.
These factors promote visceral obesity, fat accumulation, and chronic inflammation.
Why is visceral fat more harmful than subcutaneous fat?
Visceral fat is metabolically active and acts as an endocrine organ.
It:
Releases free fatty acids.
Produces inflammatory cytokines.
Promotes insulin resistance.
Alters adipokine production.
Increases risk of:
Type 2 diabetes
MASLD
Cardiovascular disease
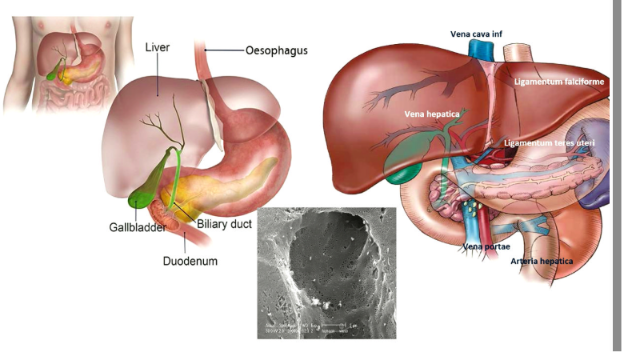
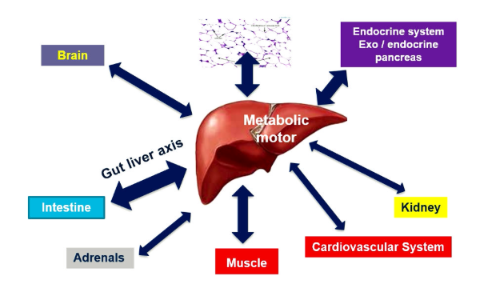
What are the major functions of the liver?
The liver maintains homeostasis through several functions.
Metabolic functions
Carbohydrate metabolism.
Protein metabolism.
Lipid metabolism.
Synthetic functions
Albumin production.
Clotting factor synthesis.
Bile salt production.
Detoxification
Drugs.
Alcohol.
Toxins.
Storage
Glycogen.
Iron.
Copper.
Vitamin B12.
Immune function
Filters bacteria and endotoxins from portal blood.
What are the main pathogenetic factors in MASLD?
The most important mechanisms include:
Insulin resistance (hallmark).
Dyslipidaemia.
Oxidative stress.
Gut dysbiosis.
Muscular dysfunction.
Together they promote:
Steatosis.
Inflammation.
Fibrosis.
Which factors aggravate MASLD?
Important aggravating factors include:
Poor diet.
Obesity.
Alcohol.
Drugs.
Genetic variants:
PNPLA3
TM6SF2
Gut microbiome alterations.
Increased intestinal permeability.
Viral hepatitis.
Environmental toxins.
Why is the gut microbiome important in MASLD?
The gut-liver axis contributes to liver inflammation.
Mechanisms include:
Gut dysbiosis.
Increased intestinal permeability.
Leakage of lipopolysaccharide (LPS).
Bacterial overgrowth.
Increased endogenous alcohol production.
These processes activate liver inflammation and fibrosis.
What is the most important prognostic factor in MASLD?
The strongest predictor of long-term outcome is:
Fibrosis stage
Advanced fibrosis is associated with:
Increased liver-related mortality.
Greater risk of cirrhosis.
Increased hepatocellular carcinoma.
Increased cardiovascular mortality.

What is the leading cause of death in patients with MASLD?
Most patients with MASLD do not die from liver disease.
The leading cause of death is:
Cardiovascular disease
Examples include:
Myocardial infarction.
Stroke.
Coronary artery disease.
Risk increases further in patients with advanced fibrosis.
Why is MASLD considered a multisystem disease?
MASLD affects many organs because it is driven by chronic low-grade systemic inflammation.
Associated diseases include:
Type 2 diabetes.
Cardiovascular disease.
Chronic kidney disease.
Metabolic syndrome.
Obesity.
Hepatocellular carcinoma.
How does FibroScan work?
FibroScan is a non-invasive ultrasound-based technique.
It measures:
Liver stiffness
Indicates fibrosis.
Controlled Attenuation Parameter (CAP)
Estimates liver fat (steatosis).
It is widely used because it is:
Quick.
Painless.
Repeatable.
More practical than liver biopsy.
What is the stepwise treatment approach for MASLD?
Management follows a stepwise approach:
Lifestyle intervention
Weight loss.
Healthy diet.
Physical activity.
Medical therapy
GLP-1 receptor agonists.
Other metabolic drugs when indicated.
Bariatric surgery
Considered for severe obesity when lifestyle measures fail.
What are the benefits of GLP-1 receptor agonists in MASLD?
Examples include Semaglutide (Ozempic, Wegovy, Rybelsus).
Benefits include:
Significant weight loss.
Reduced hepatic steatosis.
Reduced liver inflammation.
Improved glucose control.
Lower HbA1c.
Improved lipid profile.
Reduced cardiovascular events.
They are most effective when combined with lifestyle modification.
What is Resmetirom and how does it work?
Resmetirom is a thyroid hormone receptor-β agonist approved in the USA for selected patients with MASH.
Its effects include:
Improving lipid metabolism.
Increasing β-oxidation.
Reducing hepatic fat.
Promoting MASH resolution.
Improving fibrosis in some patients.
It represents one of the first targeted drug therapies for MASH.