Lec 9 ECG prt II
1/104
Earn XP
Description and Tags
Flashcards covering ECG interpretation, timing, rhythm analysis, MI evolution, and anatomical localization based on the provided technical transcript.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
105 Terms
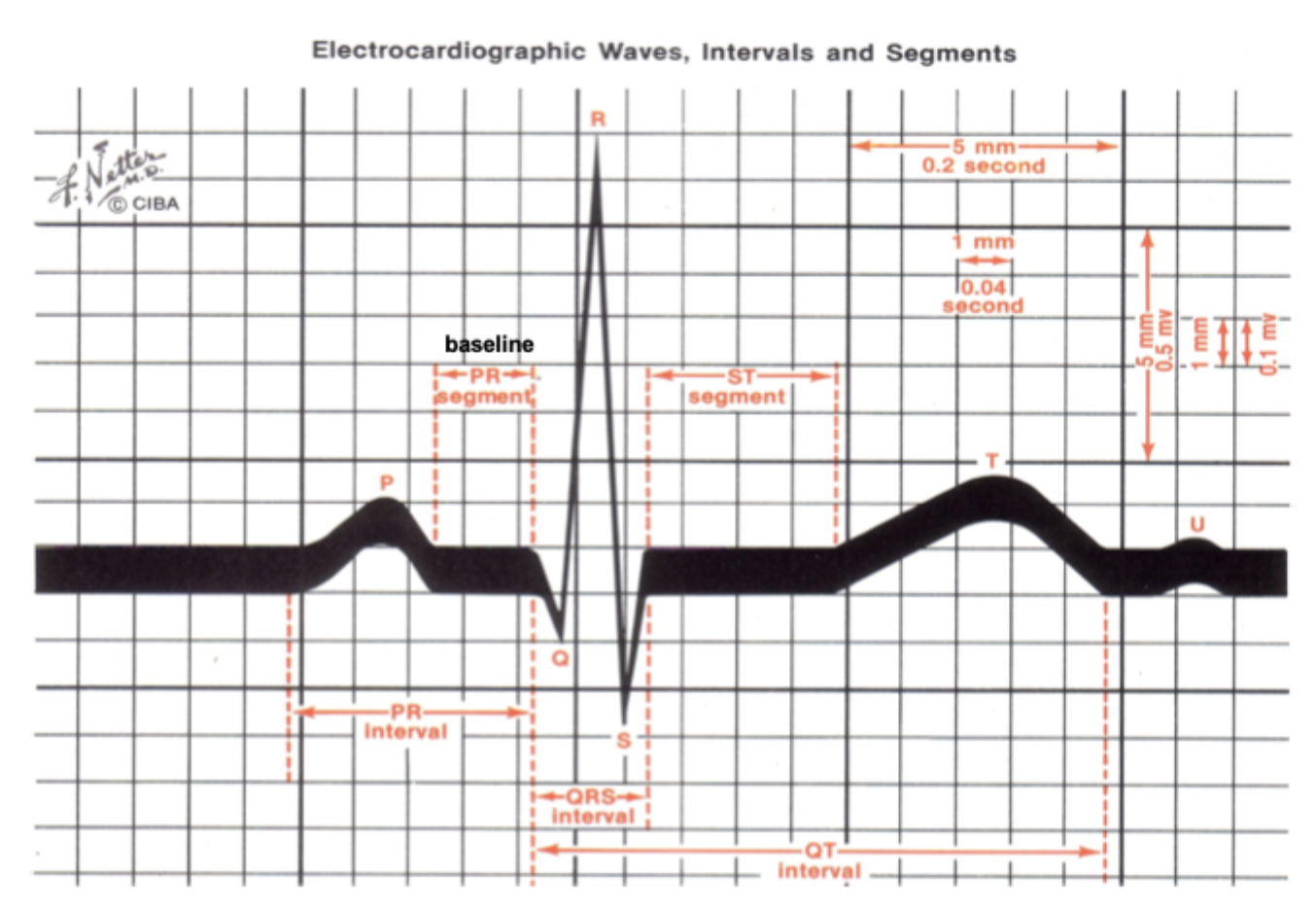
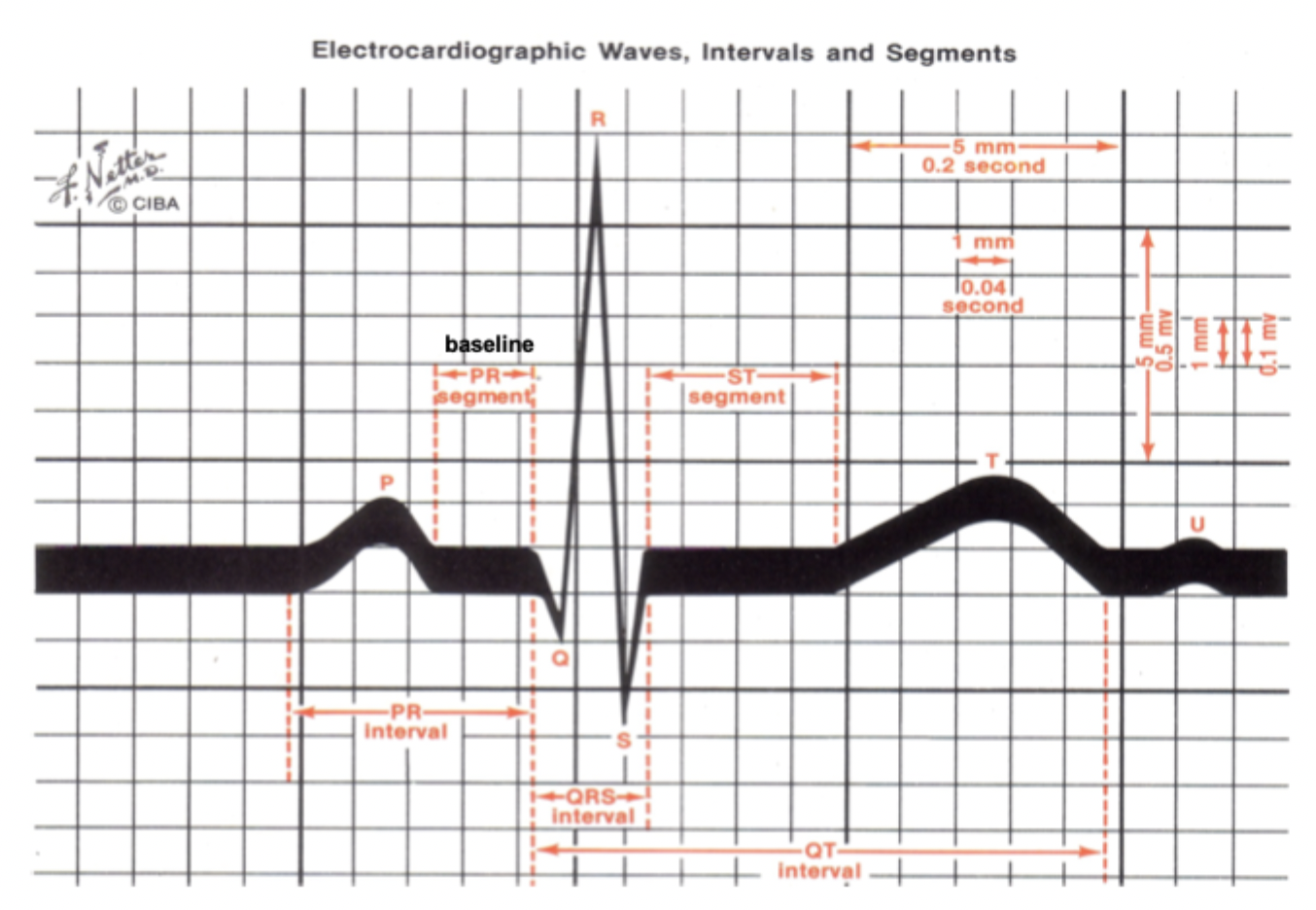
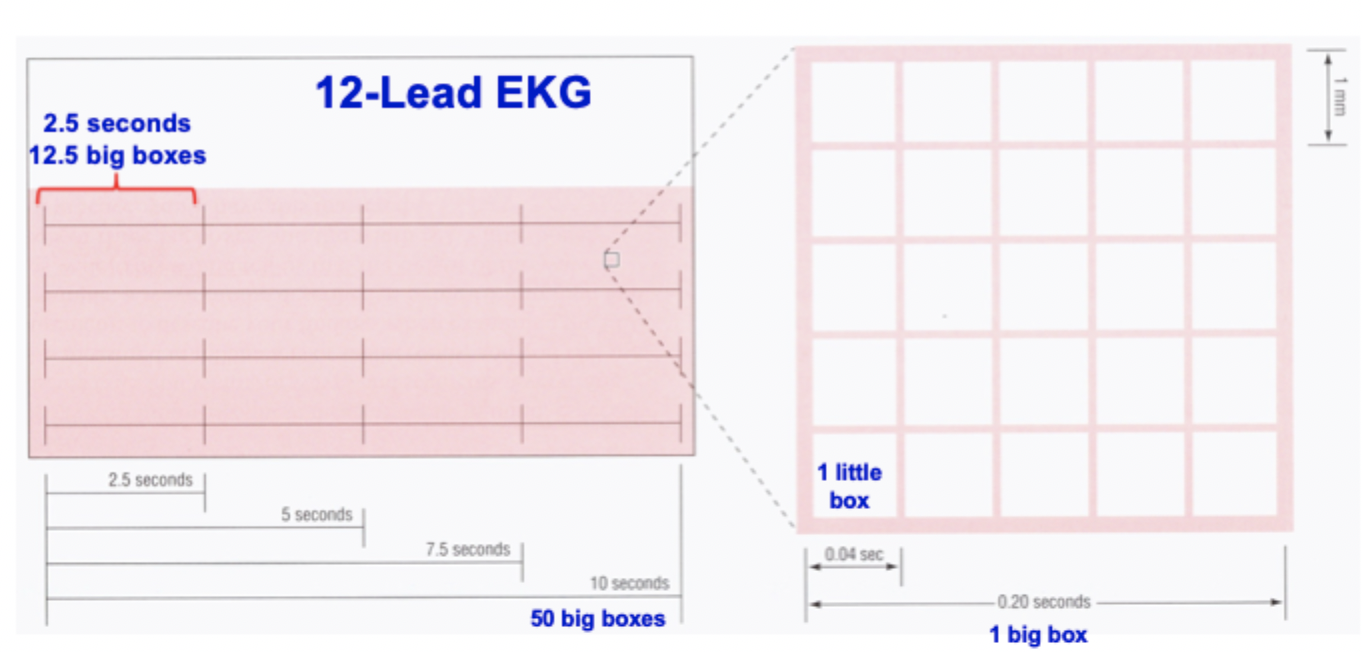
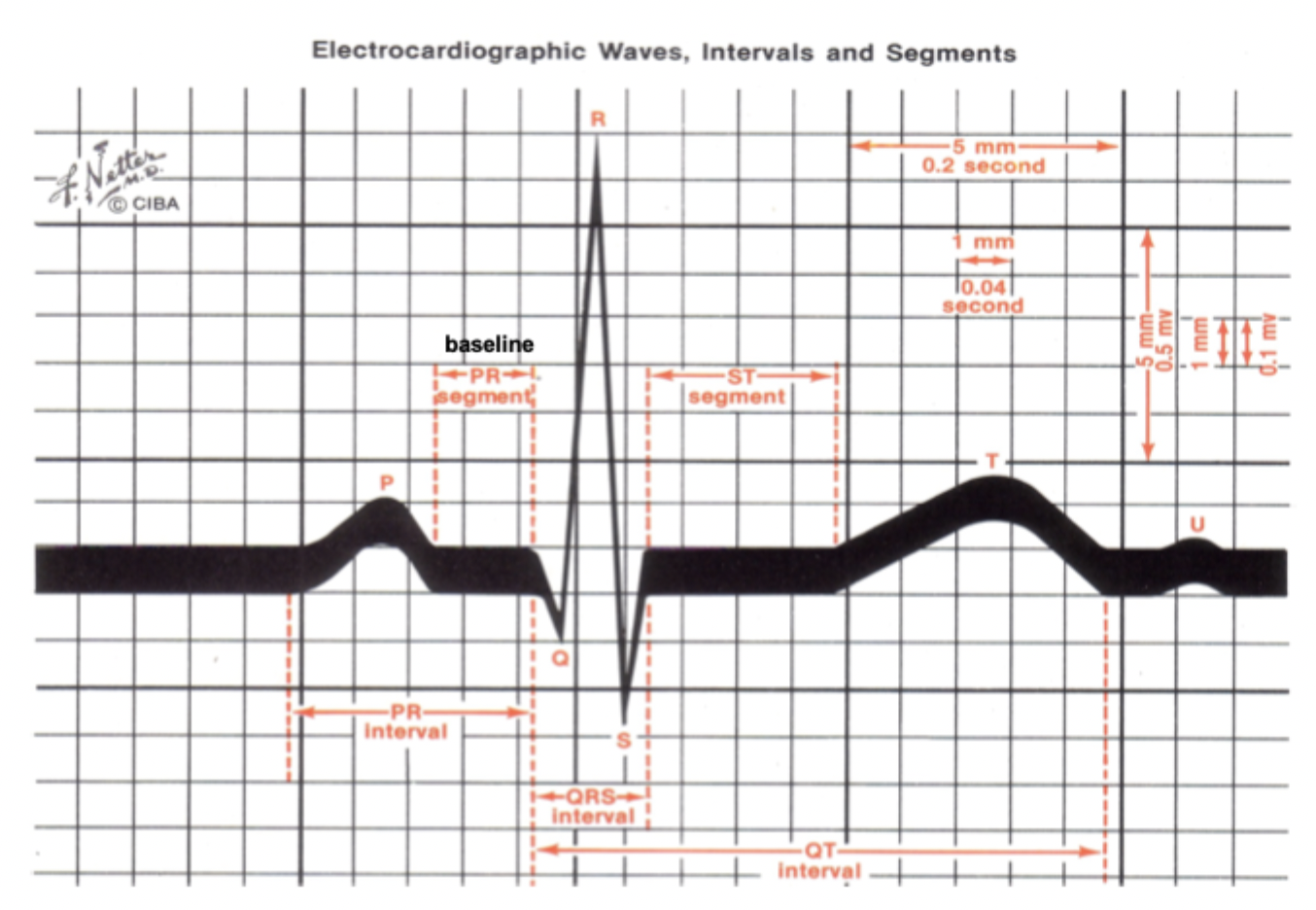
What is the time equivalent of one 'Little Box' on an ECG graph paper?
0.04 seconds (1mm)
How many millimeters and big boxes are equivalent to a duration of 5.0 seconds?
125.0mm or 25.0 Big Boxes
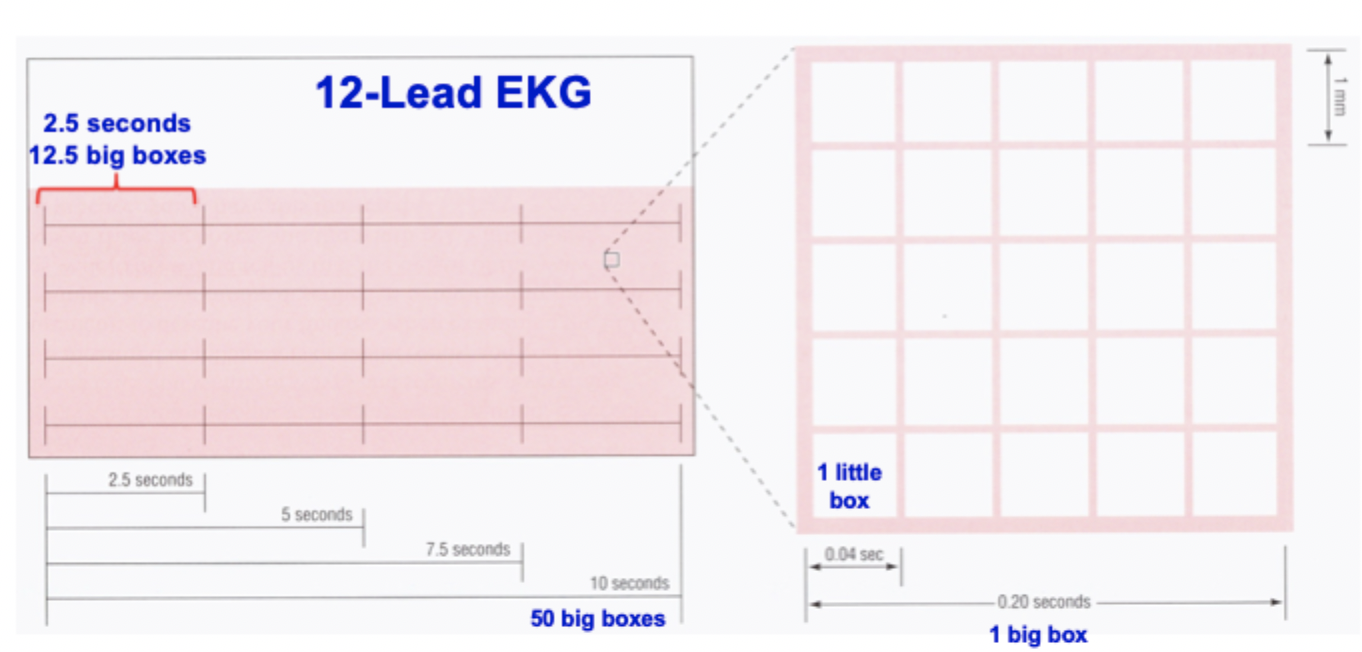
What is the standard measurement for a 'Big Box' in terms of little boxes and time?
5 Little Boxes equaling 0.20 seconds (5mm)
How many big boxes are contained in a 10.0-second ECG strip?
50.0 Big Boxes equaling 250.0mm
According to the Standard Interval Thresholds, what is the maximum duration for a normal PR interval?
<1 big box (0.20 s)
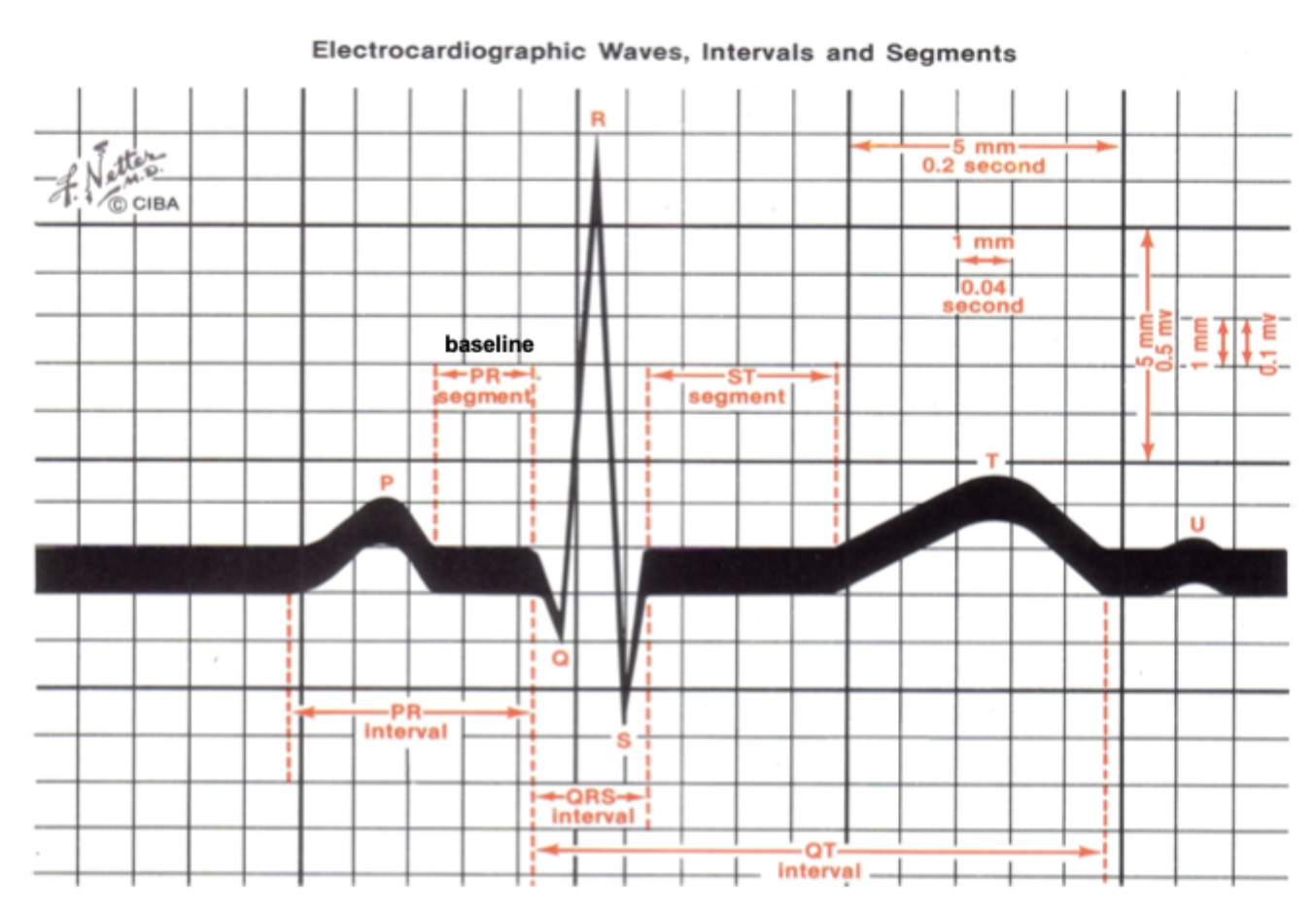
What is the maximum normal width for a QRS complex according to the 'Big Box' shortcuts?
<1/2 of a big box (0.10 s)
What is the standard temporal boundary for a normal QT interval?
<1/2 of the preceding RR interval
In the Systematic Rhythm Analysis Framework, what are the '3 R’s'?
Regular (distance between complexes)
Rate (fast, slow, or normal)
Related (P waves married to QRS)
What does the ECG 'Marriage' metaphor describe?
The gold standard for evaluating AV synchrony, specifically if P waves are linked to QRS complexes with a fixed PR interval
What does a 'divorce' or abnormal P-QRS relationship indicate in a rhythm analysis?
Transmission failures or heart blocks
What is a specific hallmark of heart blocks visible on an ECG regarding wave counts?
The presence of more P waves than QRS complexes
Which lead should P waves typically be upright in during a systematic check?
Lead II
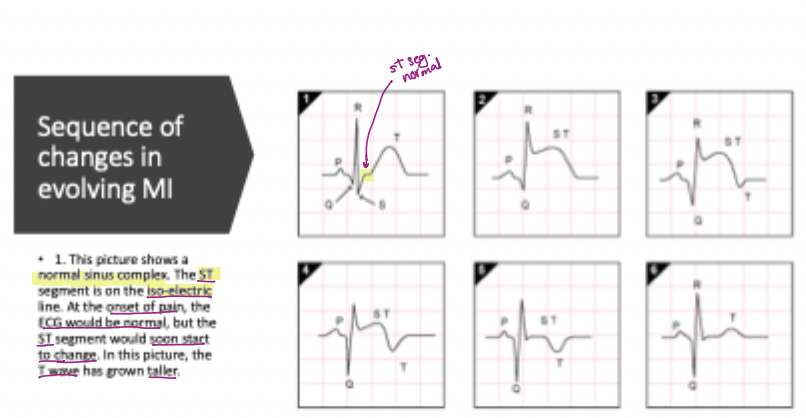
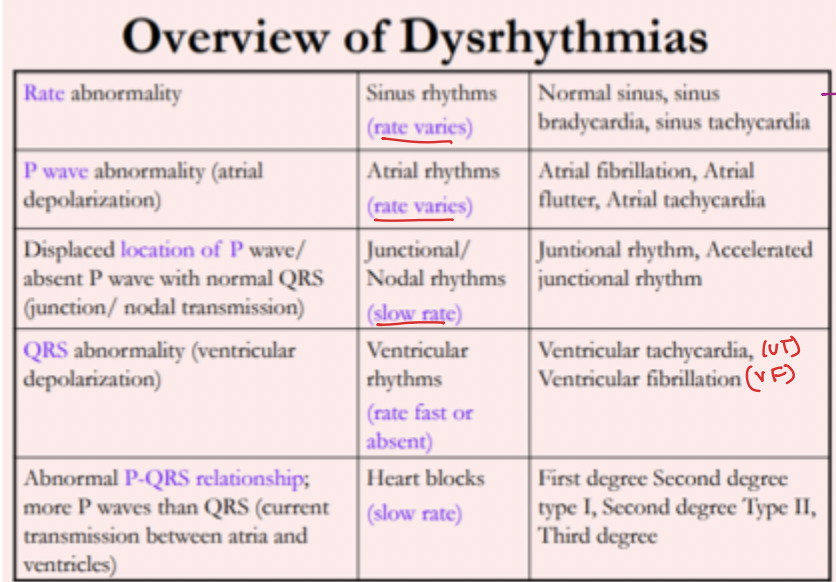
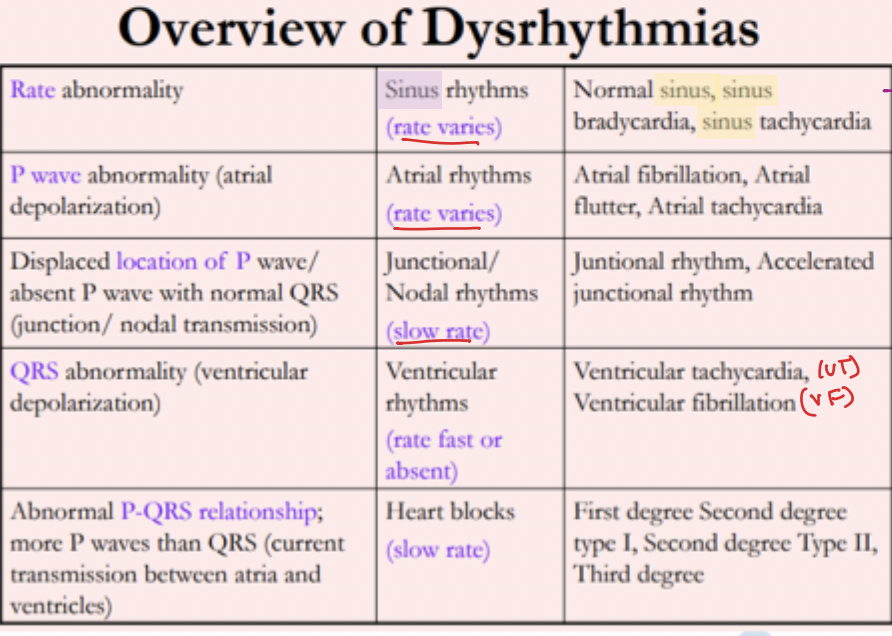
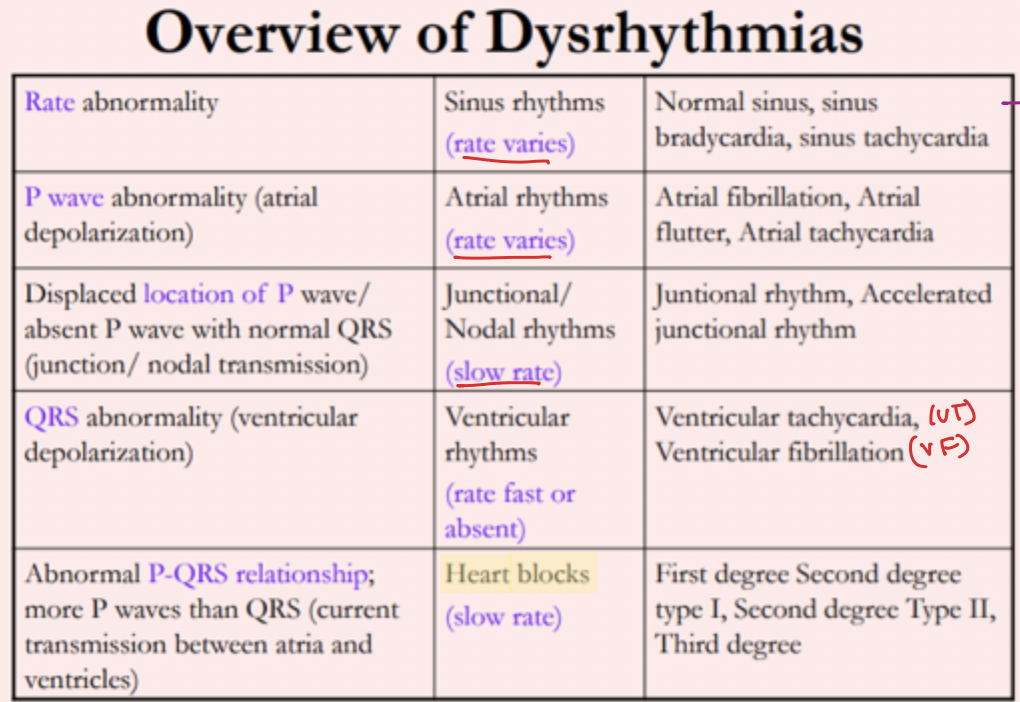
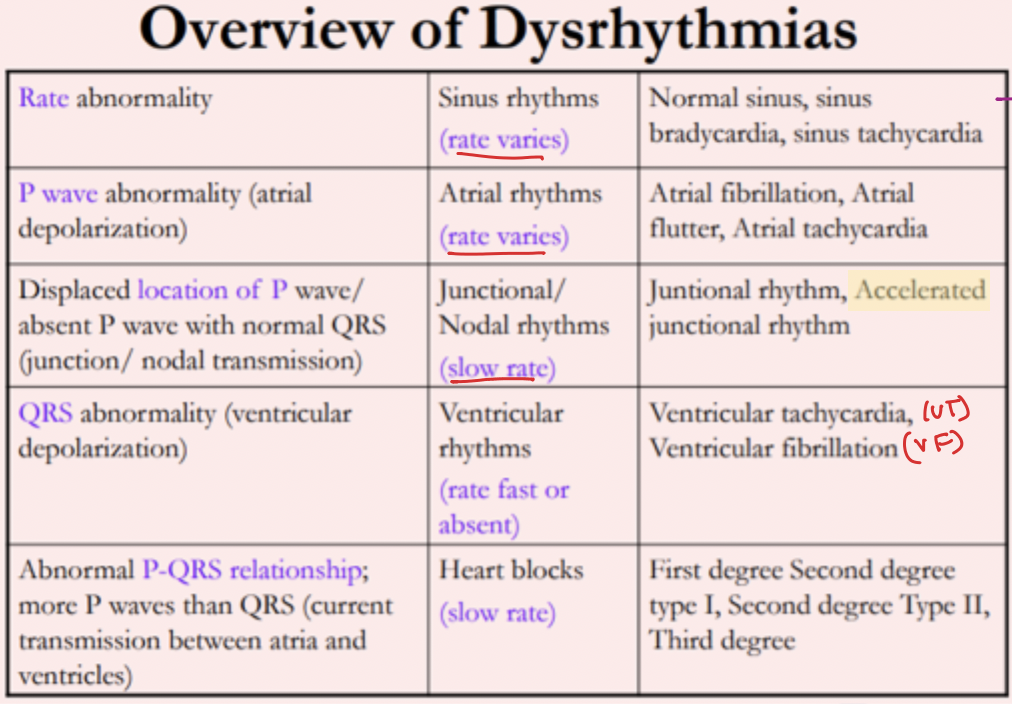
What is the defining characteristic of 'Atrial Rhythms' according to the master chart?
Rate varies; atrial depolarization focus (Displaced/Absent P)
fibrillation, flutter, tachycardia
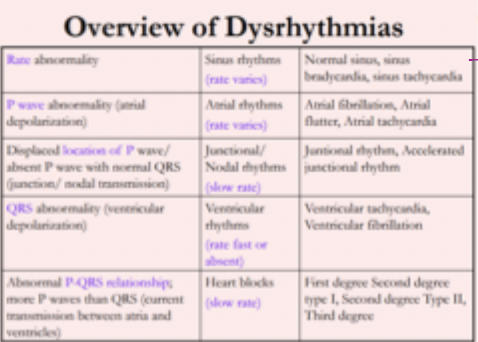
How are 'Junctional/Nodal' rhythms characterized in terms of rate and focus?
Slow rate with a junctional transmission focus —displaced location/absent P wave
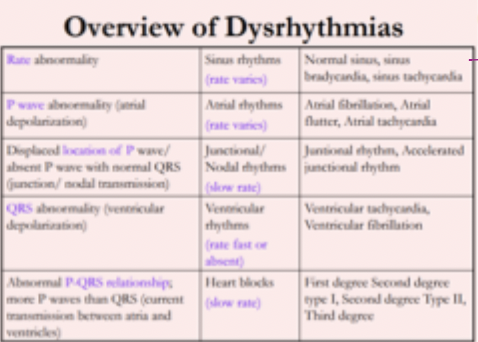
What are the primary defining characteristics of 'Ventricular Rhythms' like VT or VF?
Rate fast or absent with a ventricular focus and QRS abnormality
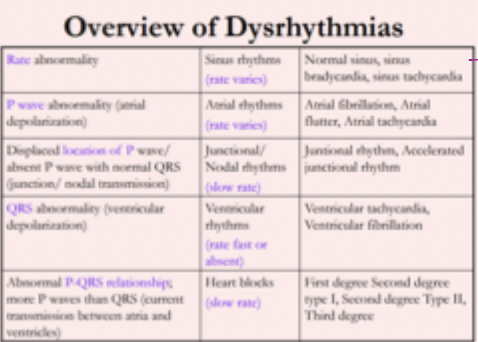
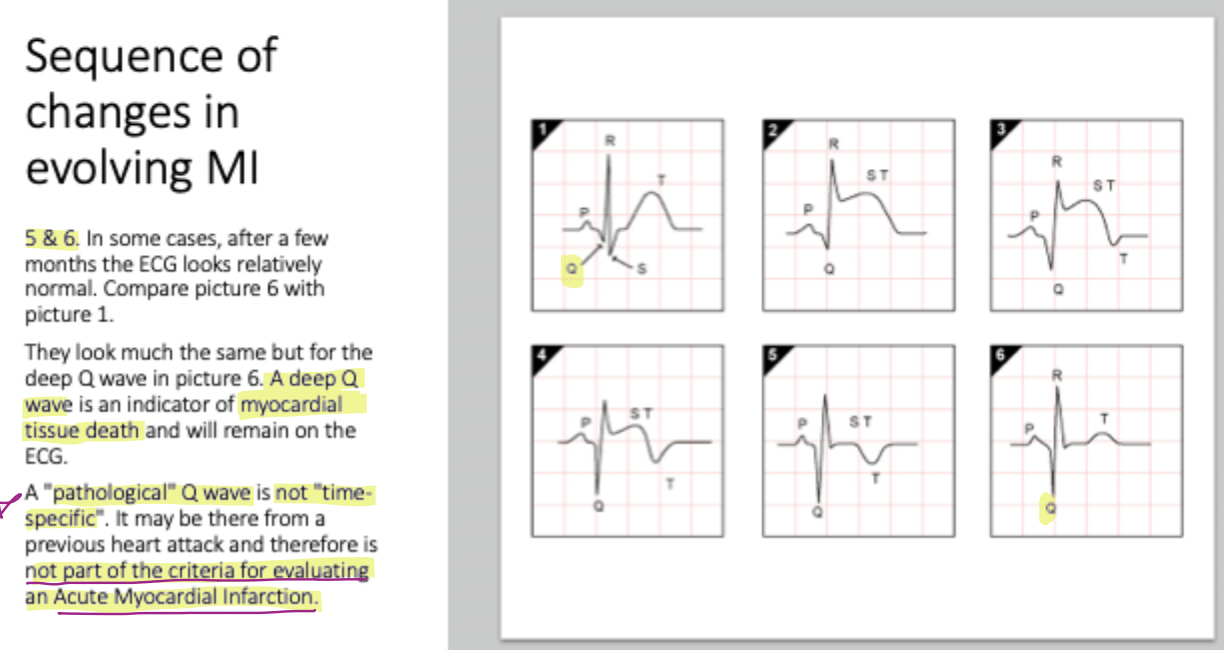
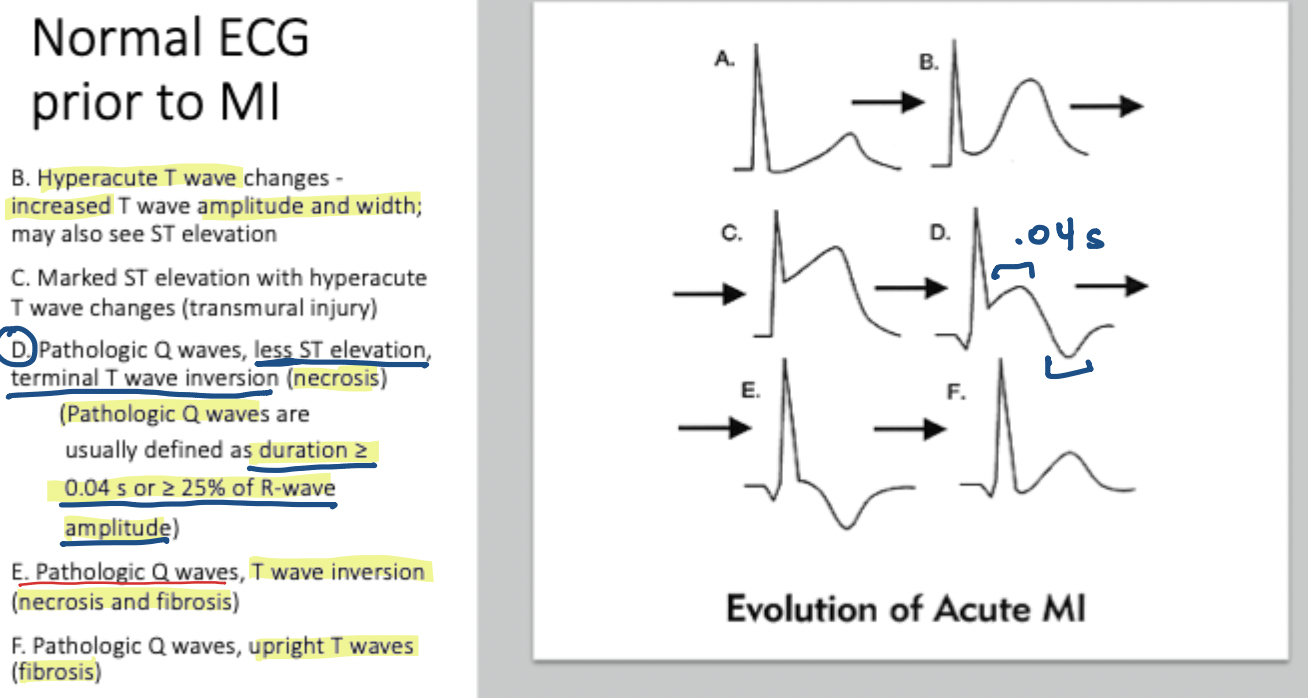
What anatomical change is responsible for a Pathological Q wave?
Permanent necrosis & fibrosis (myocardial tissue death)
T wave inversion
not time specific —not a criteria for evaluating acute myocardia infarction
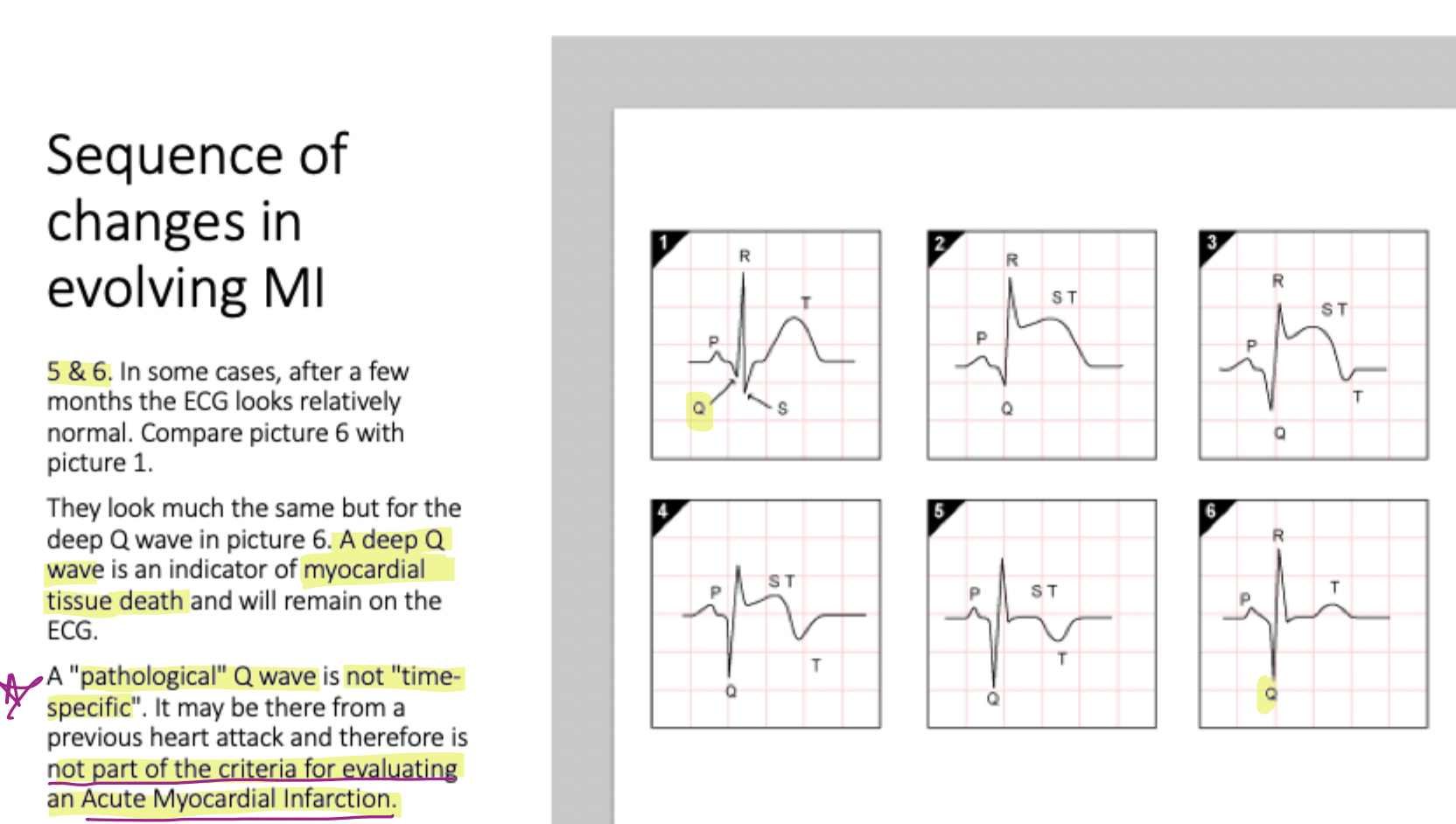
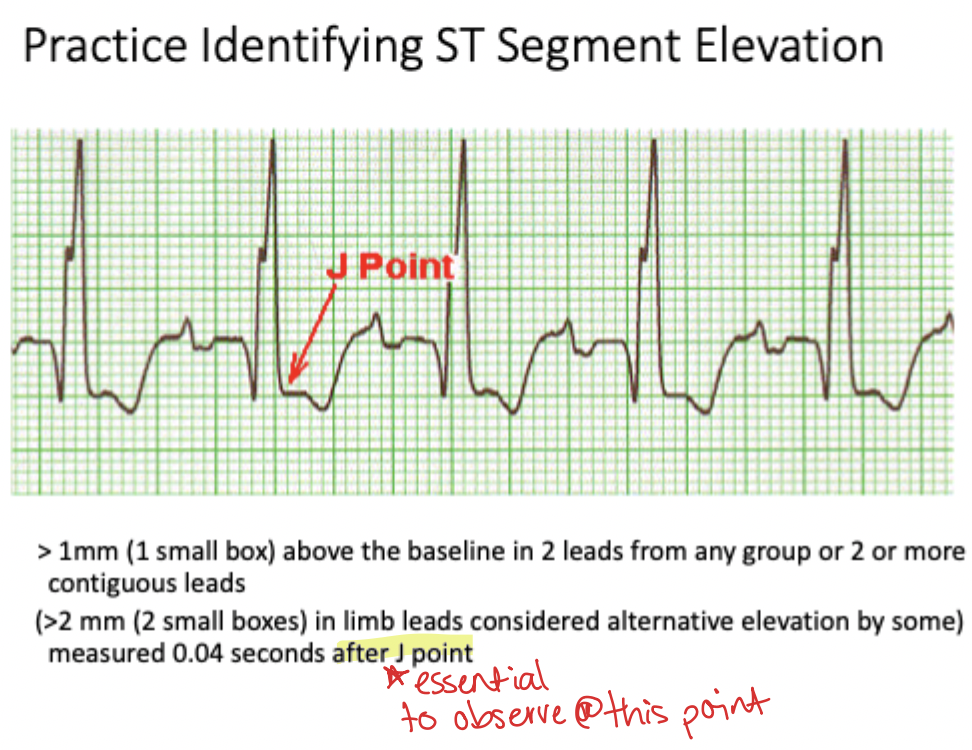
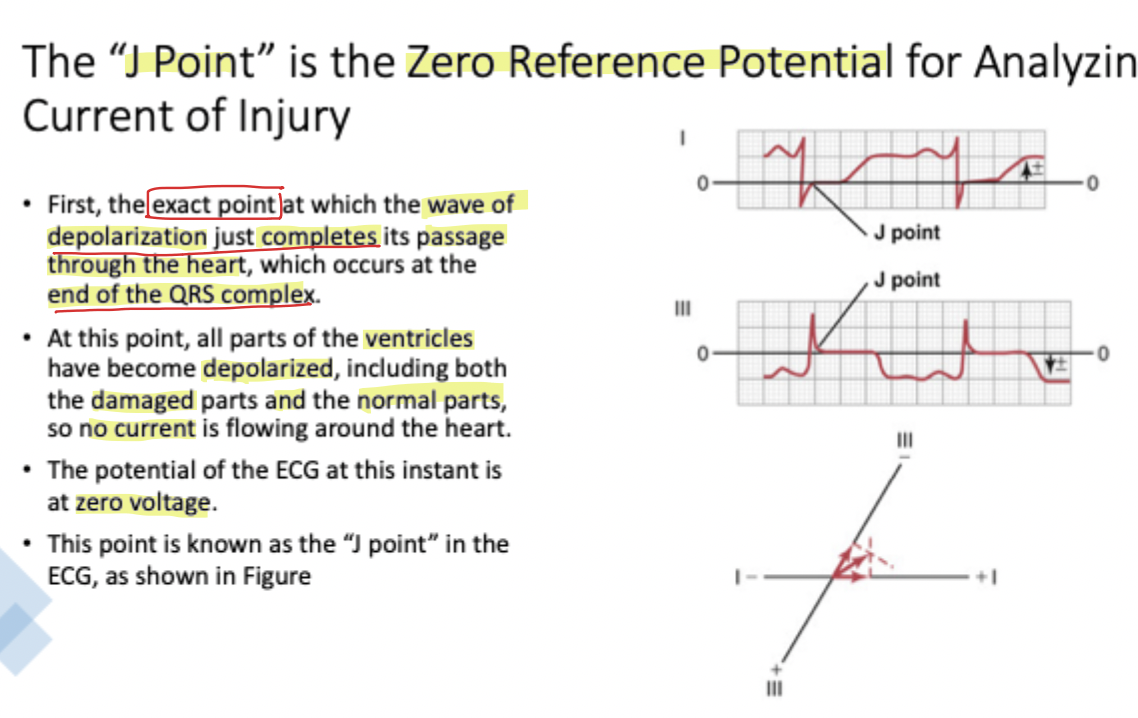
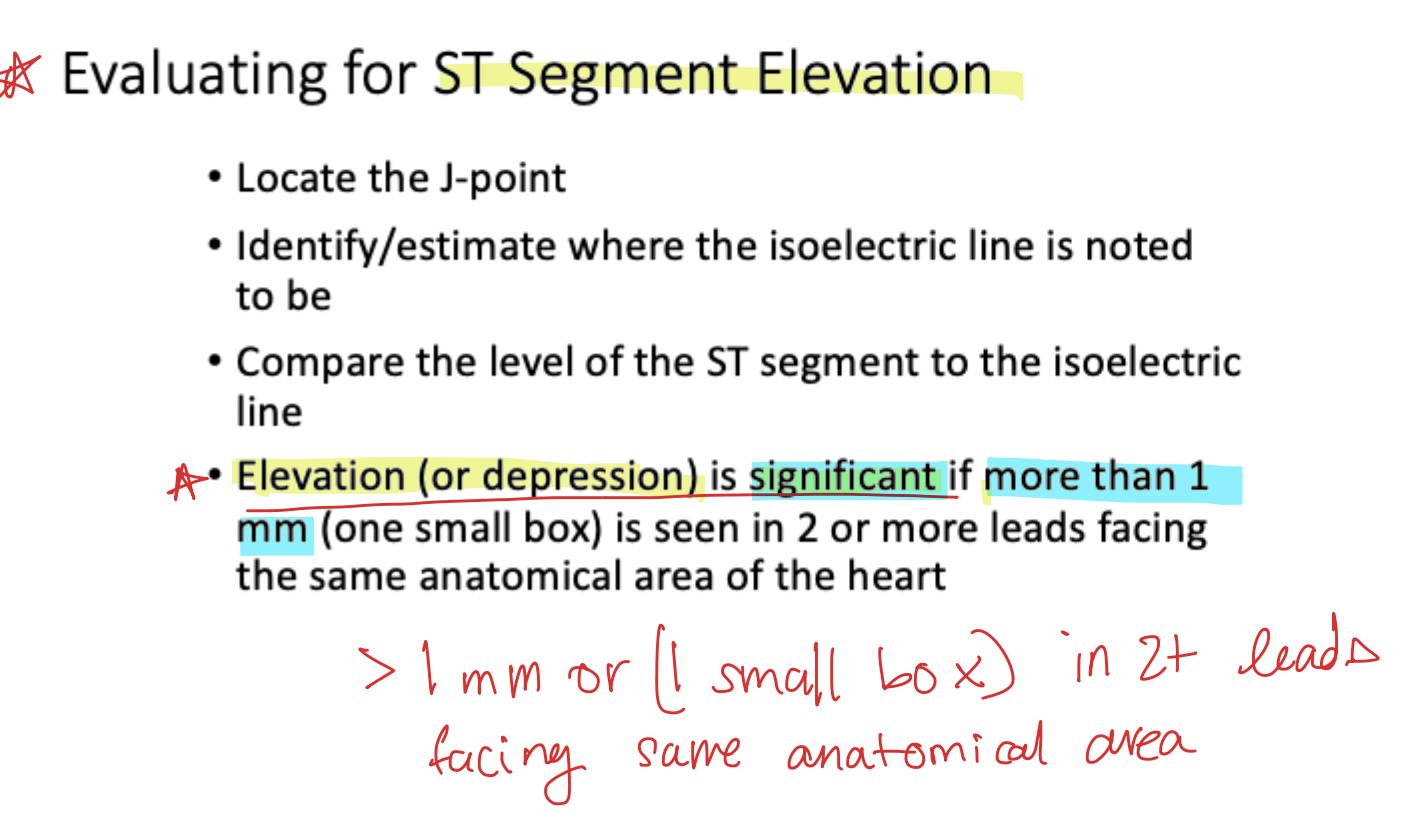
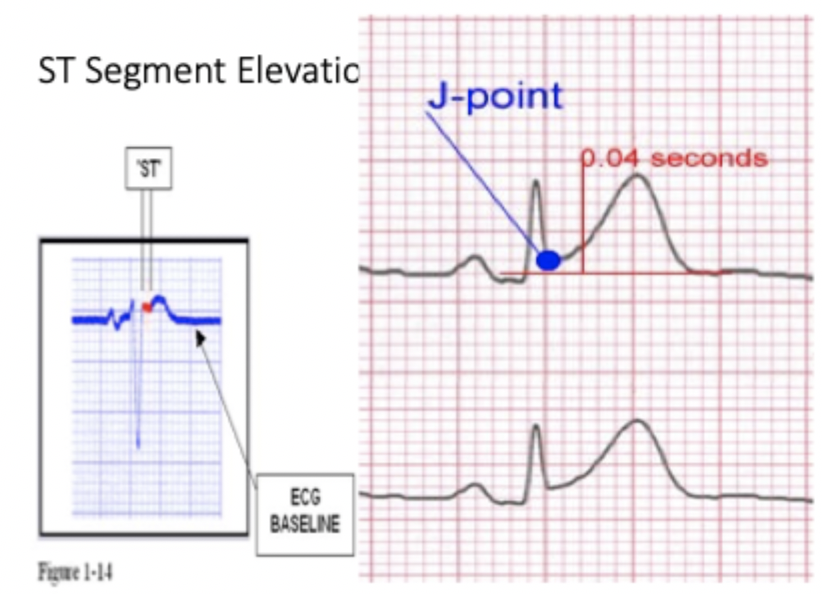
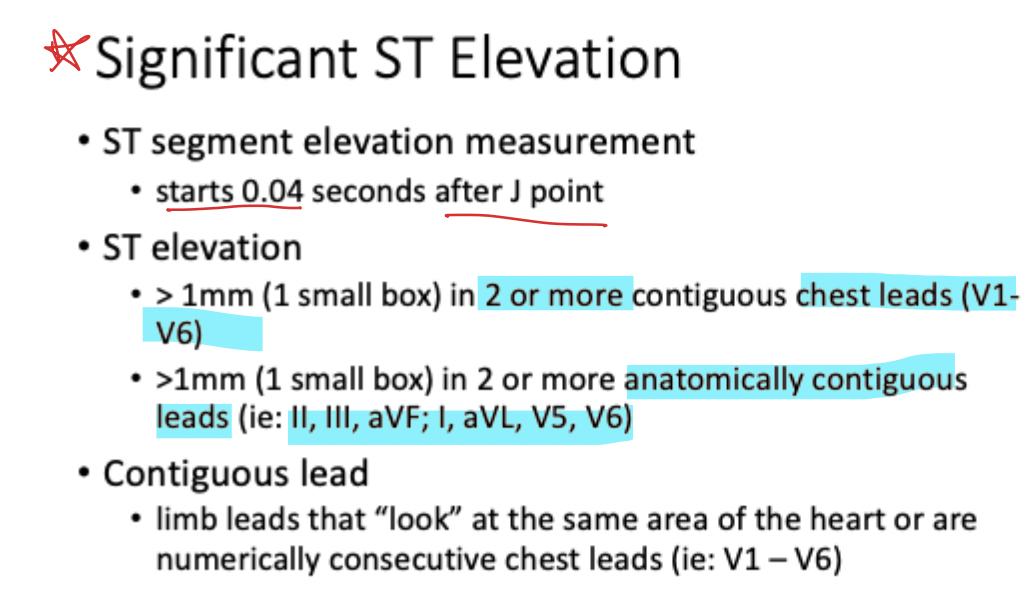
Define the 'J point' in electrocardiographic measurement.
The zero-reference potential marking the end of the QRS complex where depolarization completes
Why is the ECG potential at zero voltage during the J point?
The heart is fully depolarized, so both damaged and healthy parts are in the same electrical state and no current flows
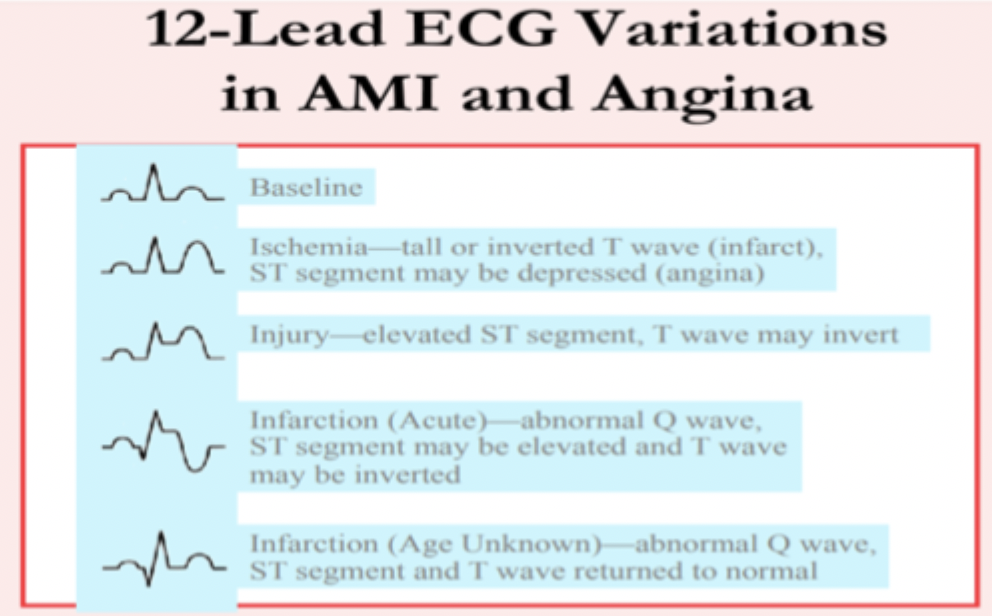
How does 'Ischemia' typically present on an ST-segment analysis?
ST-segment depression
What ECG finding indicates 'Injury' or prolonged myocardial hypoxia or ischemia?
ST-segment elevation
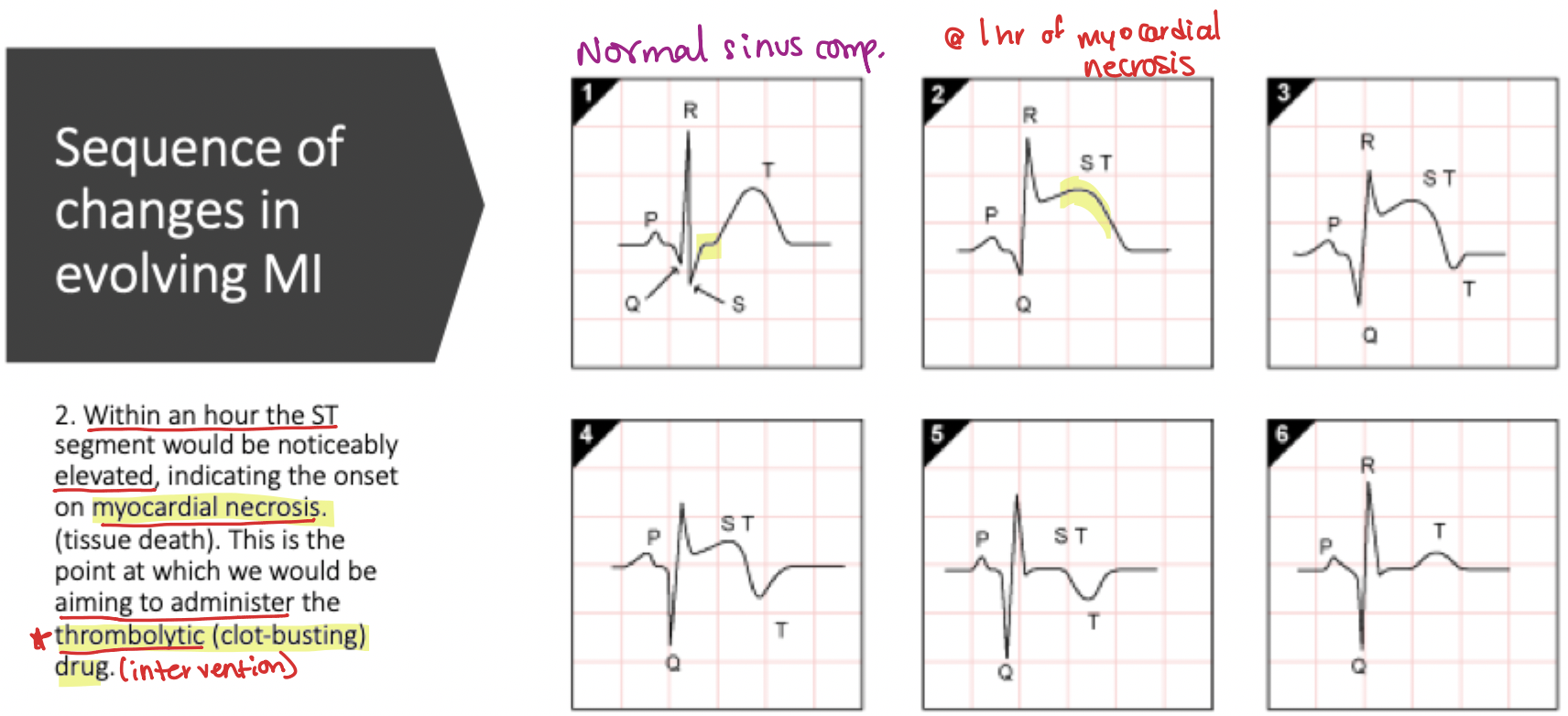
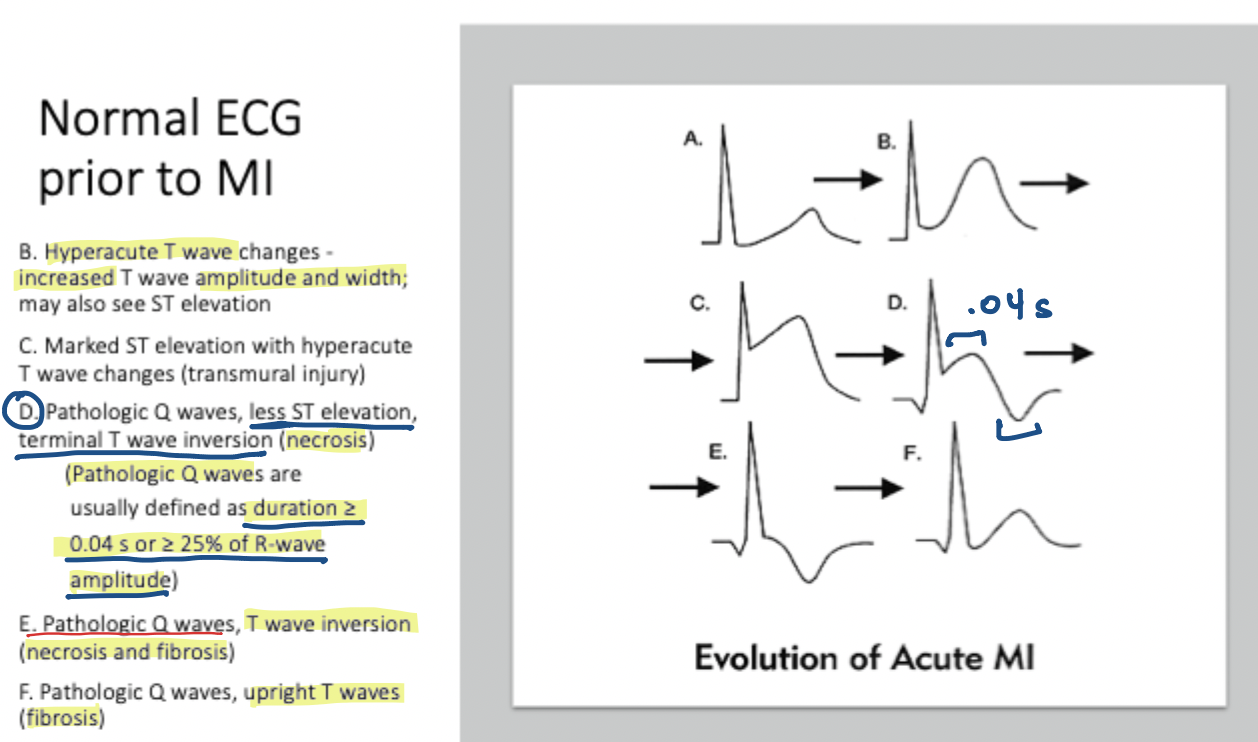
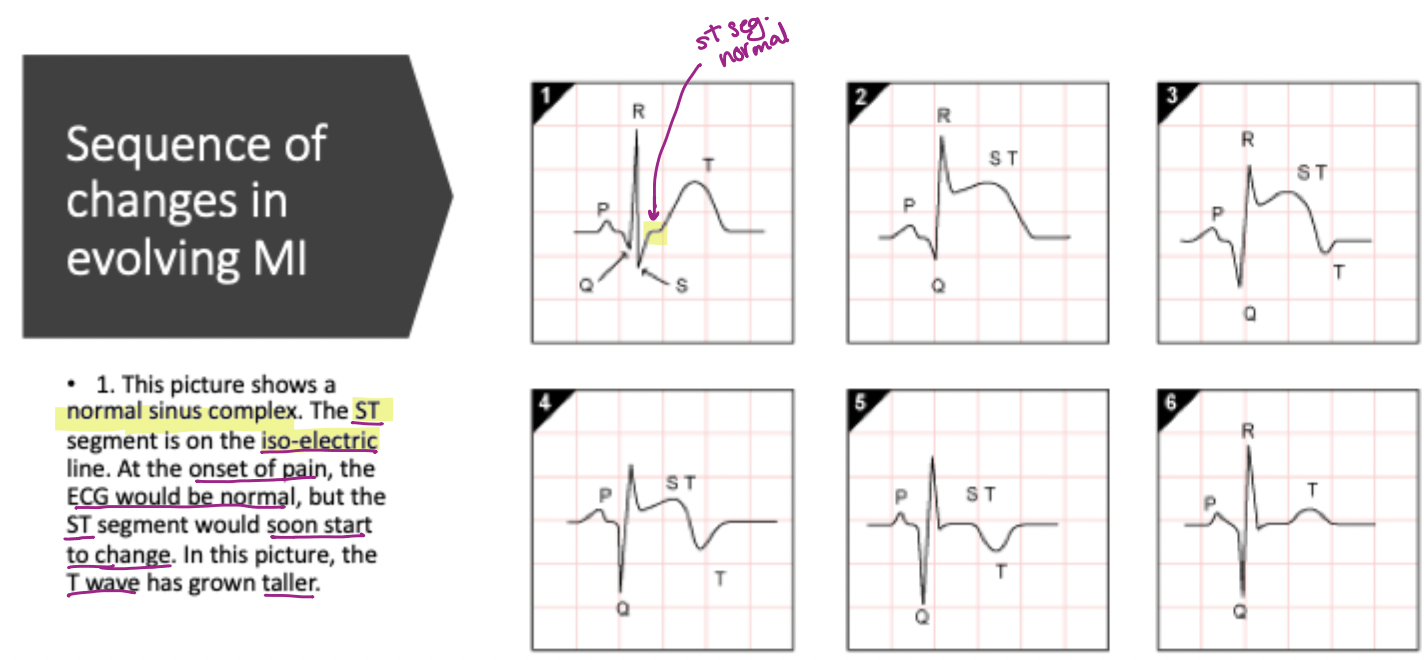
Within the MI evolution timeline, what occurs during the first hour of myocardial necrosis?
Noticeable ST elevation begins; this is the primary window for thrombolytic intervention
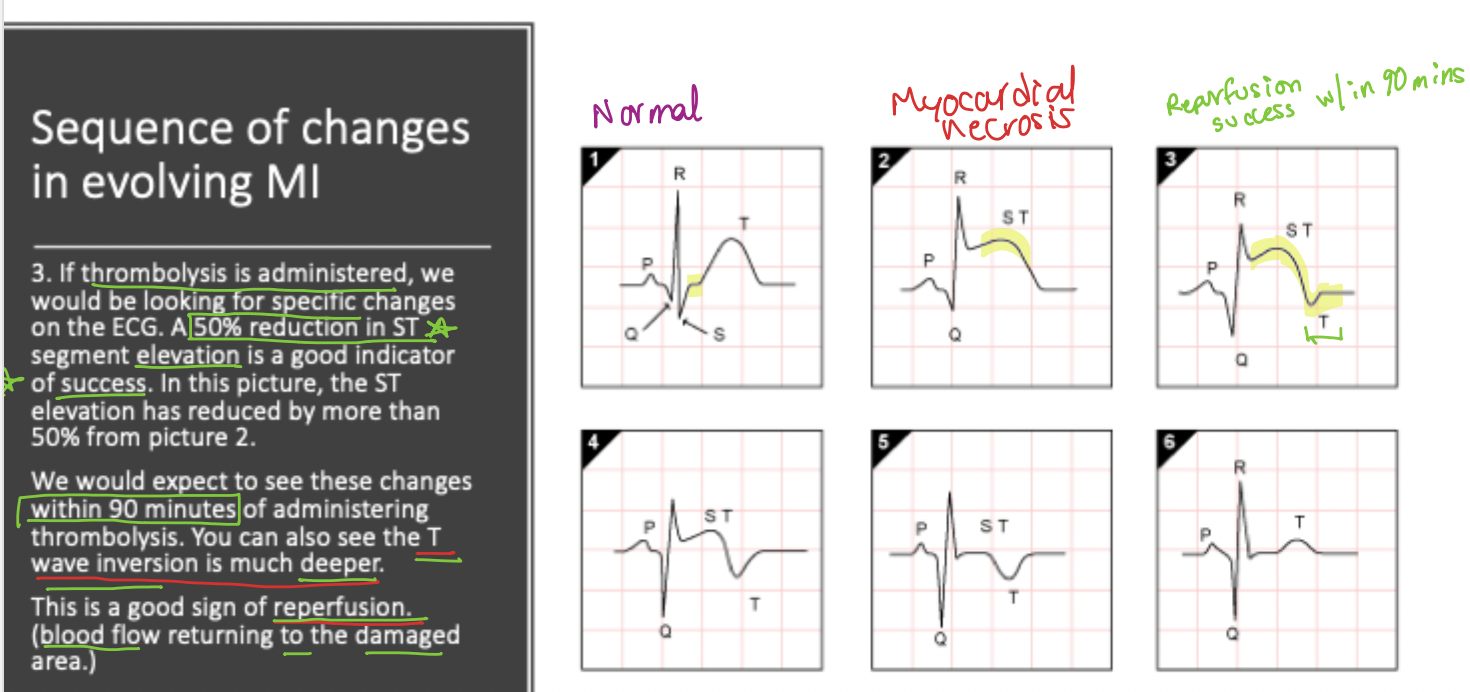
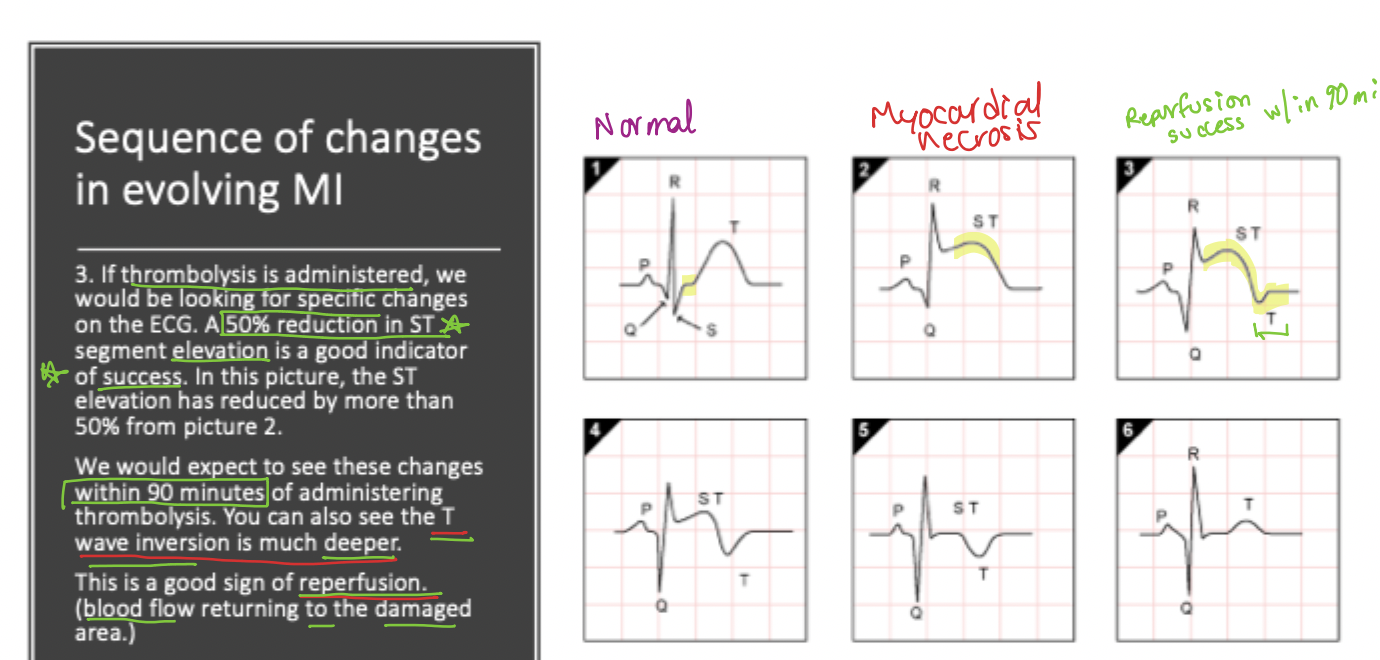
What ECG changes signify successful reperfusion (blood flow returning to damaged area) w/in 90min of treatment?
A 50% reduction in ST elevation and deep T-wave inversion = success
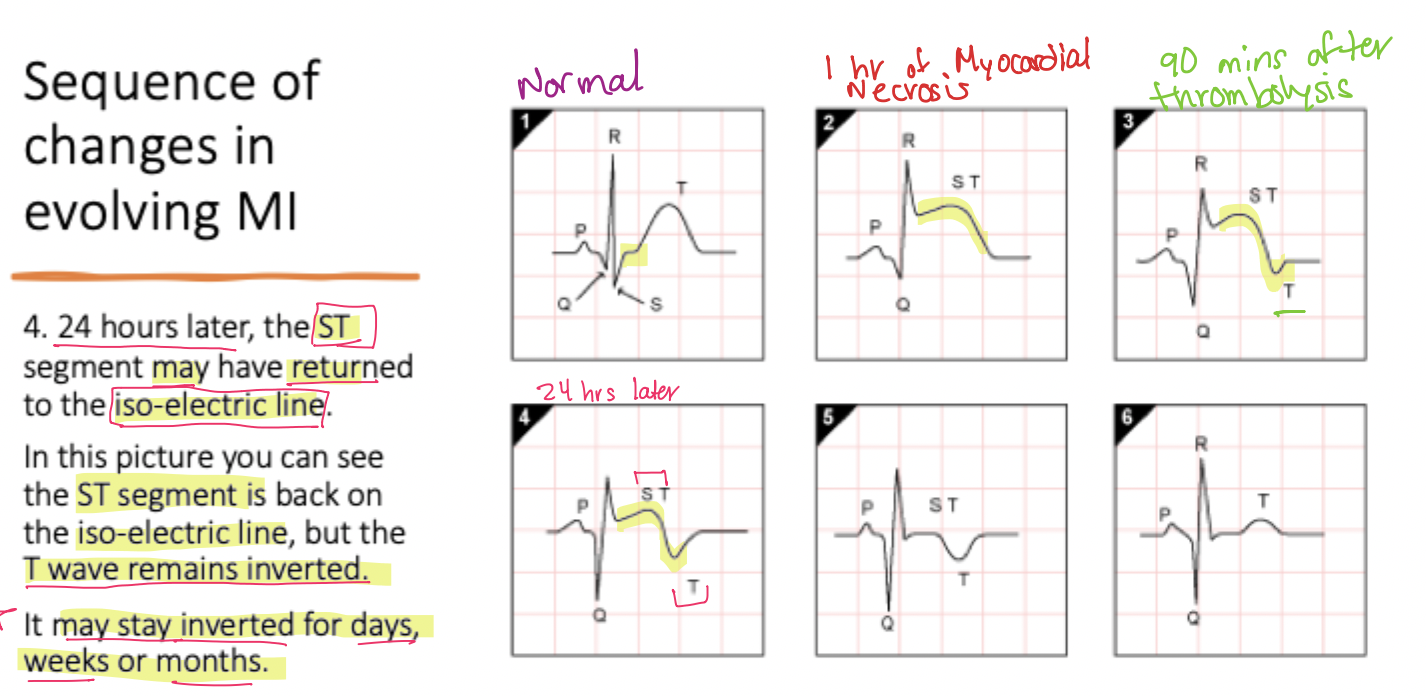
In the evolution of an MI, what is expected to occur after 24 hours?
The ST segment returns to the isoelectric line, while the T-wave remains inverted
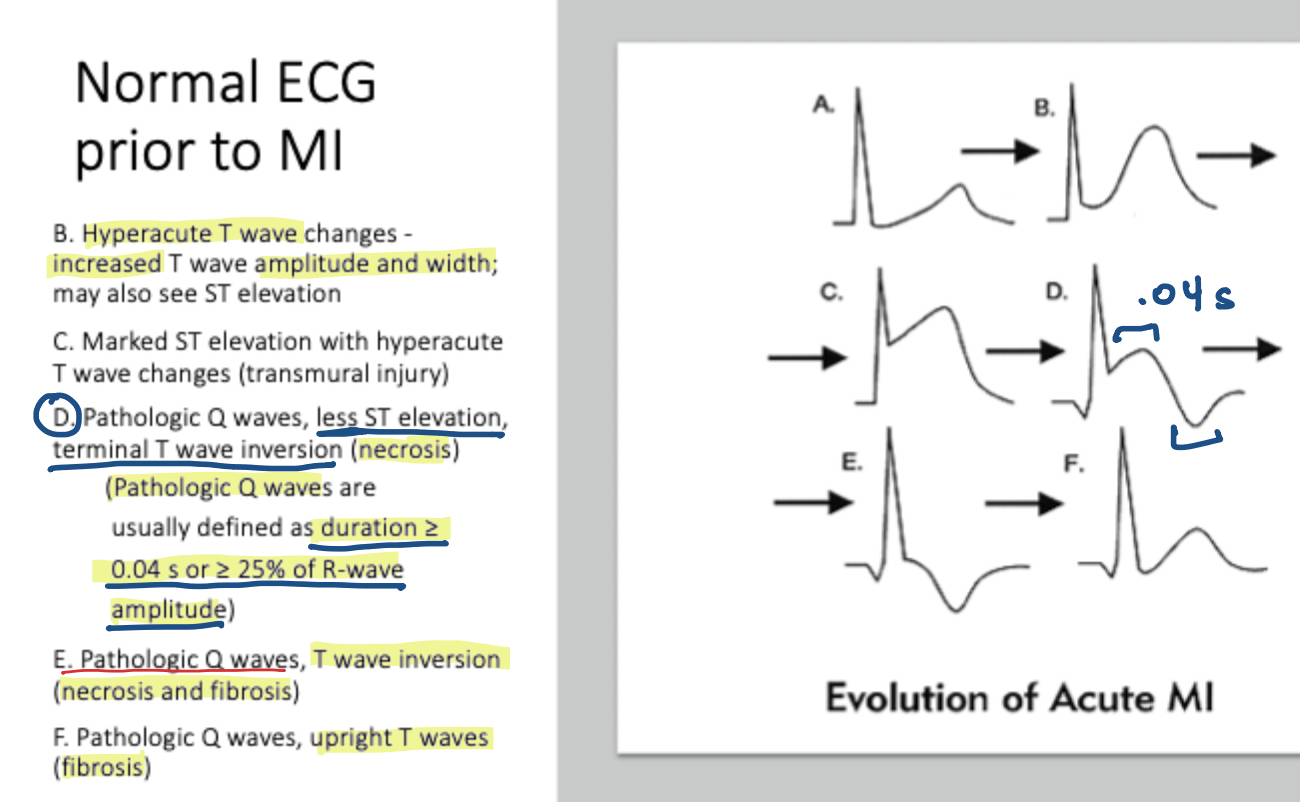
What is the time-specific criteria for a Q wave to be considered 'pathological'?
Duration ≥ 0.04s | ≥ 25% or R-wave amplitude
What amplitude criteria defines a pathological Q wave?
≥25% of R-wave amplitude
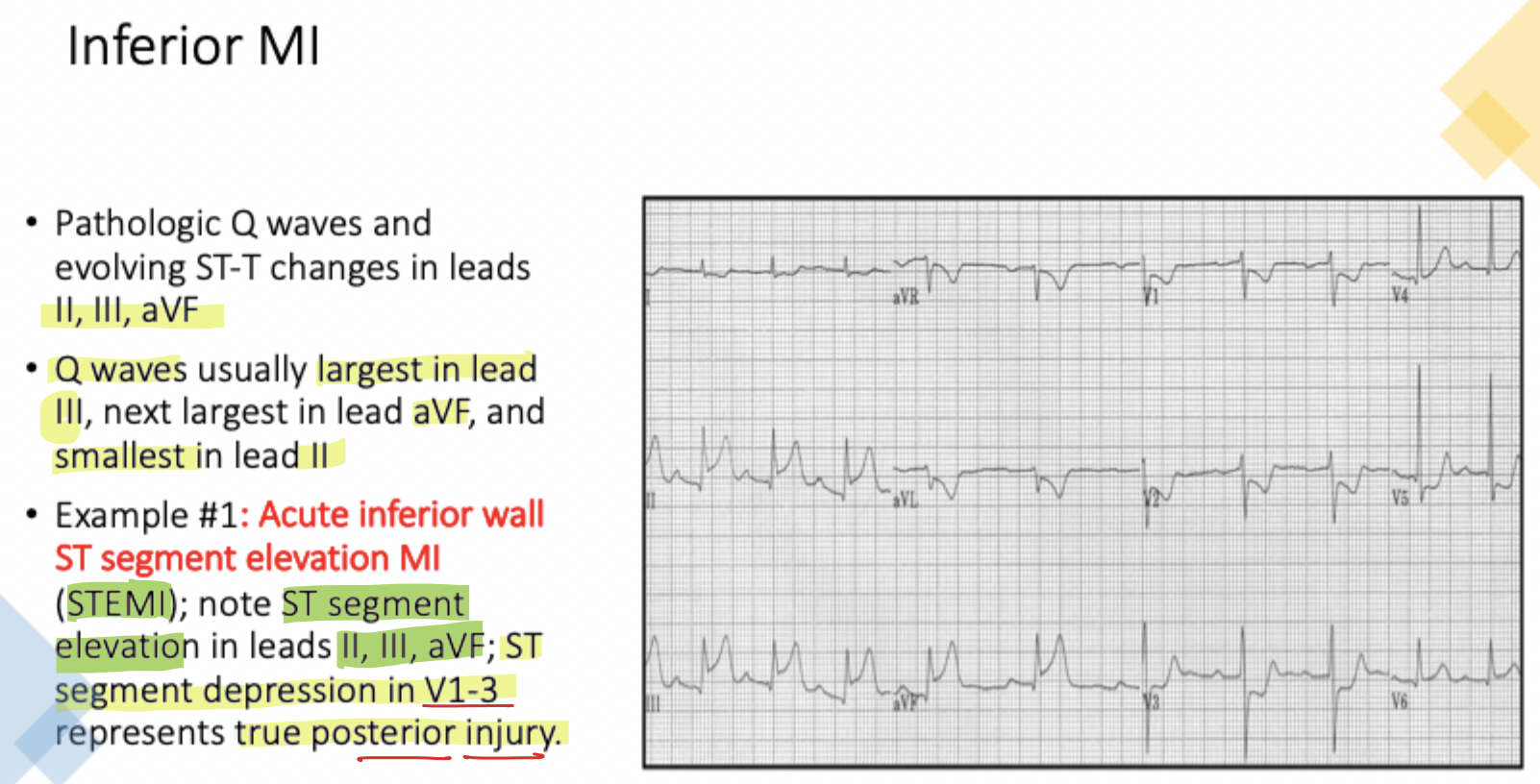
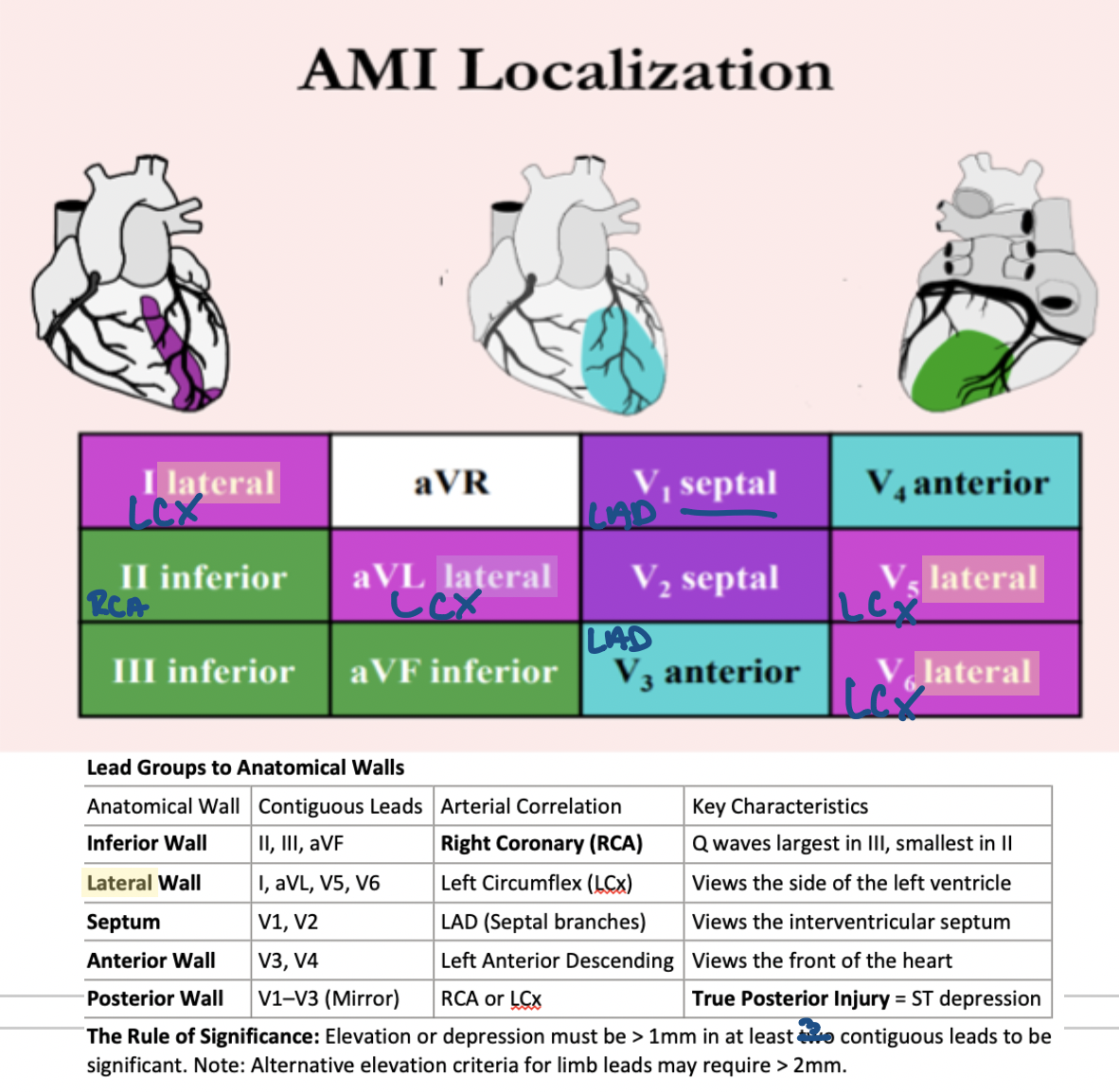
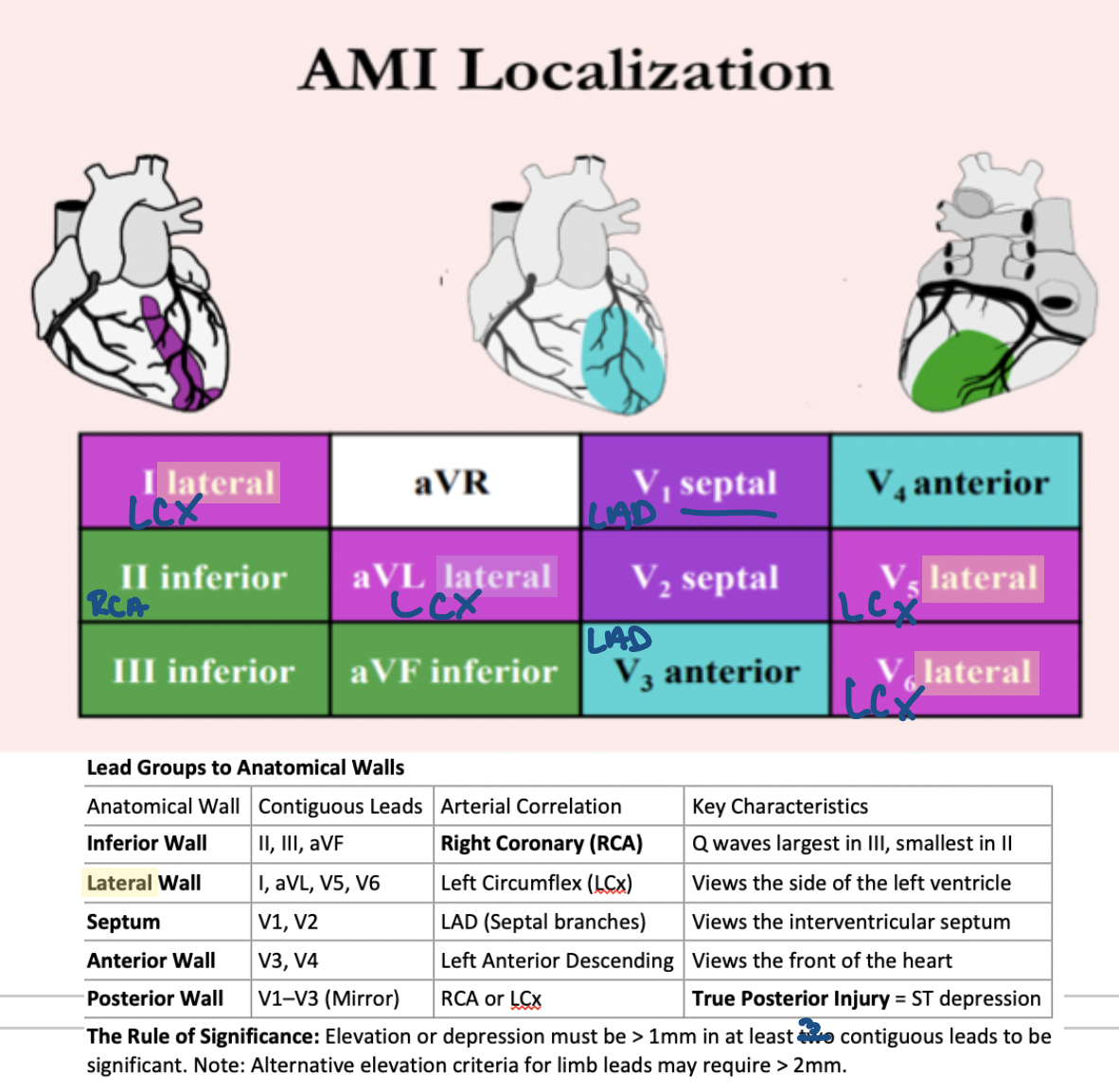
Which contiguous leads view the Inferior Wall of the heart?
Leads II, III, aVF
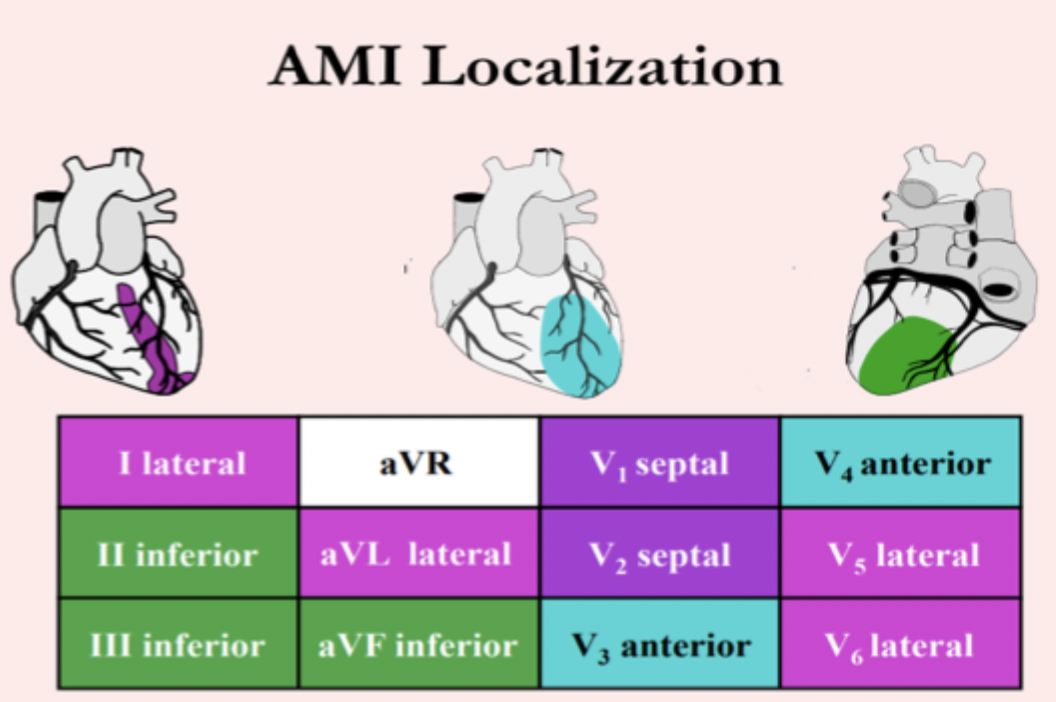
What is the primary arterial correlation for the Lateral Wall of the heart?
Left Circumflex (LCx)
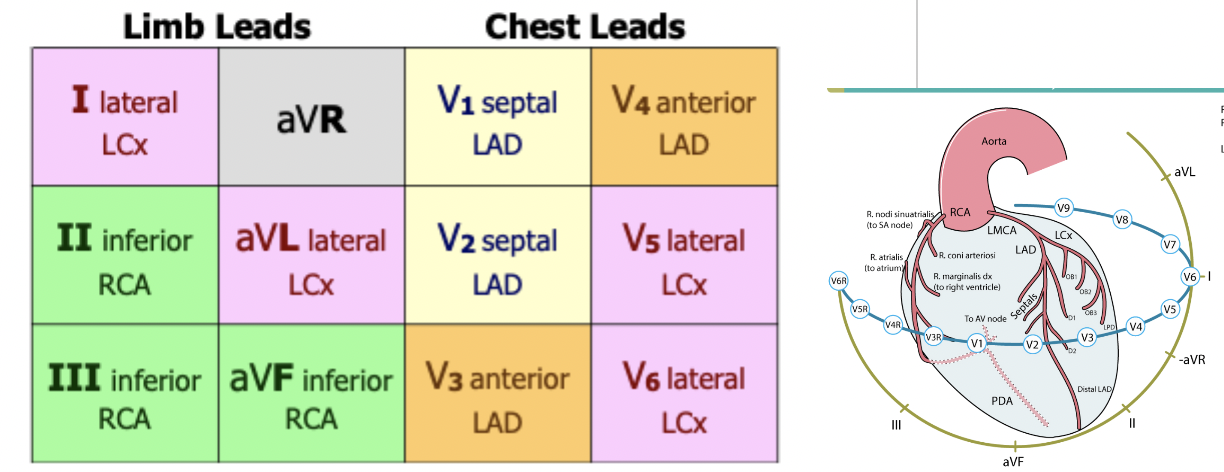
Which leads view the Septum and what is their arterial correlation?
V1, V2; correlated with the LAD (Septal branches)
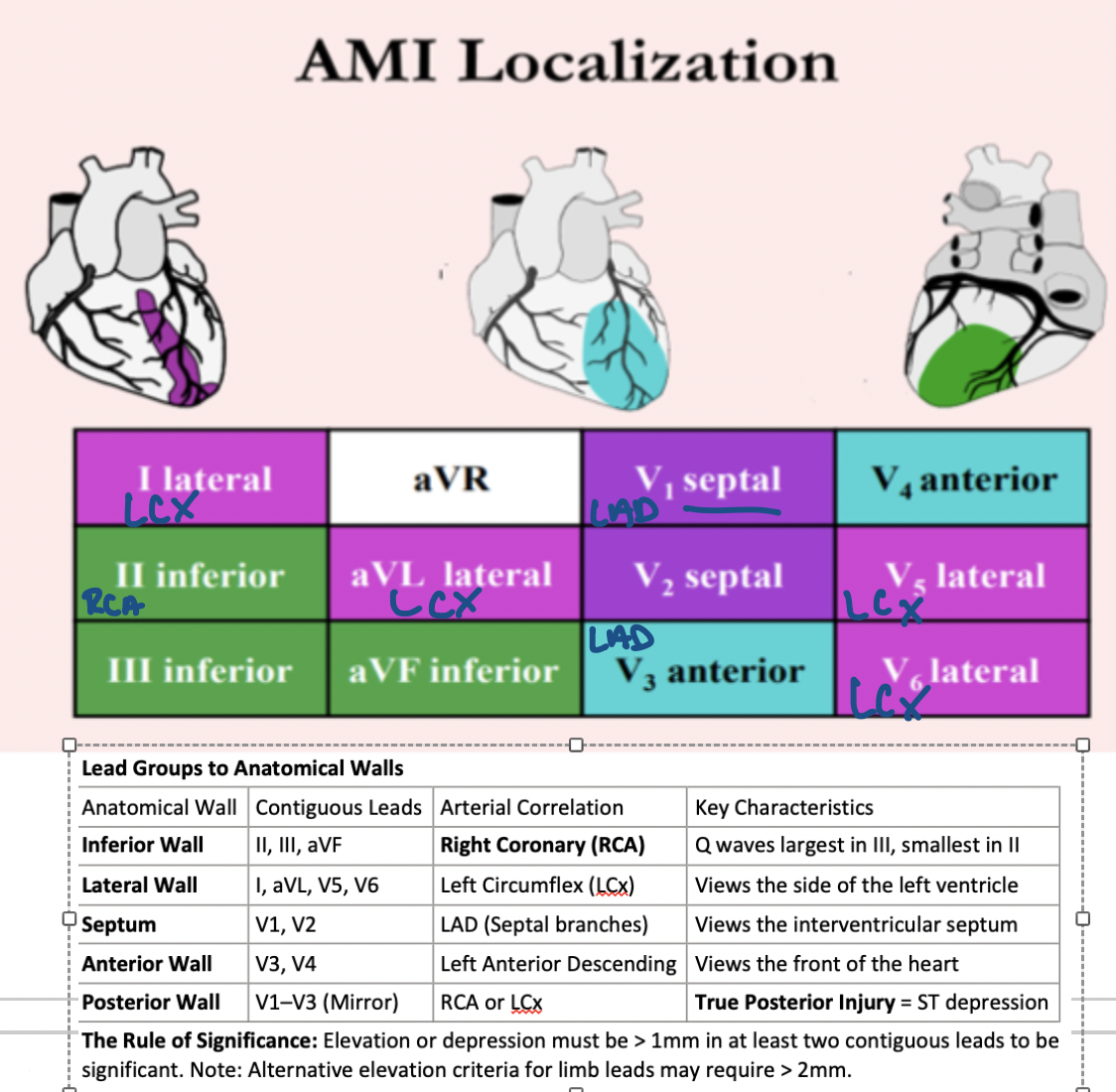
Which leads view the Anterior Wall and what is their arterial correlation?
V3, V4; correlated with the Left Anterior Descending (LAD)
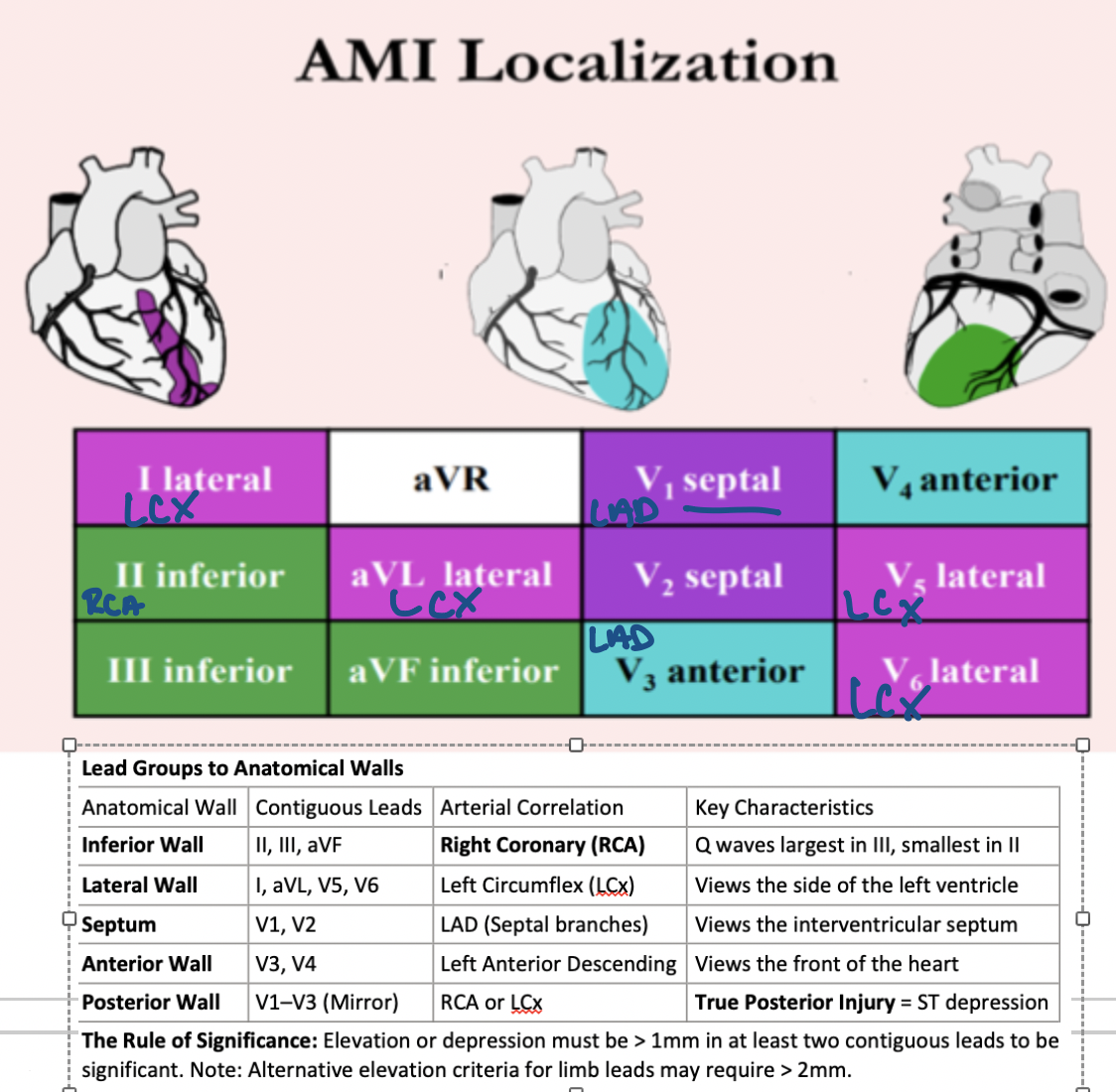
How is a True Posterior Injury identified on a standard 12-lead ECG?
ST depression in leads V1–V3 (Mirror image)
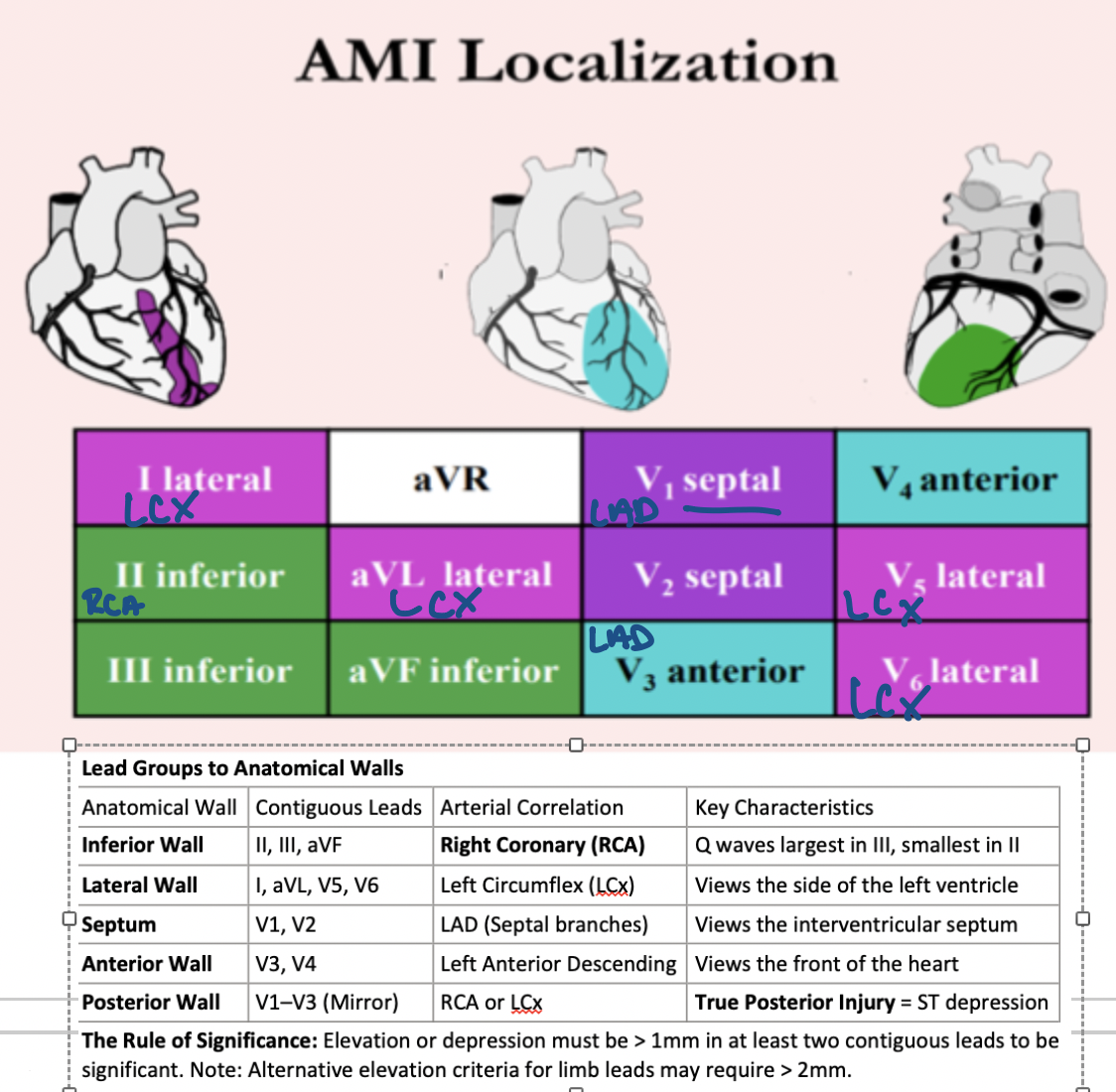
What is the 'Rule of Significance' for ST-segment changes?
ST elevation or depression must be > 1mm in 2+contiguous leads
Which lead shows ST elevation > ST elevation in V1 in an Acute Left Main Coronary Artery Occlusion?
Lead aVR
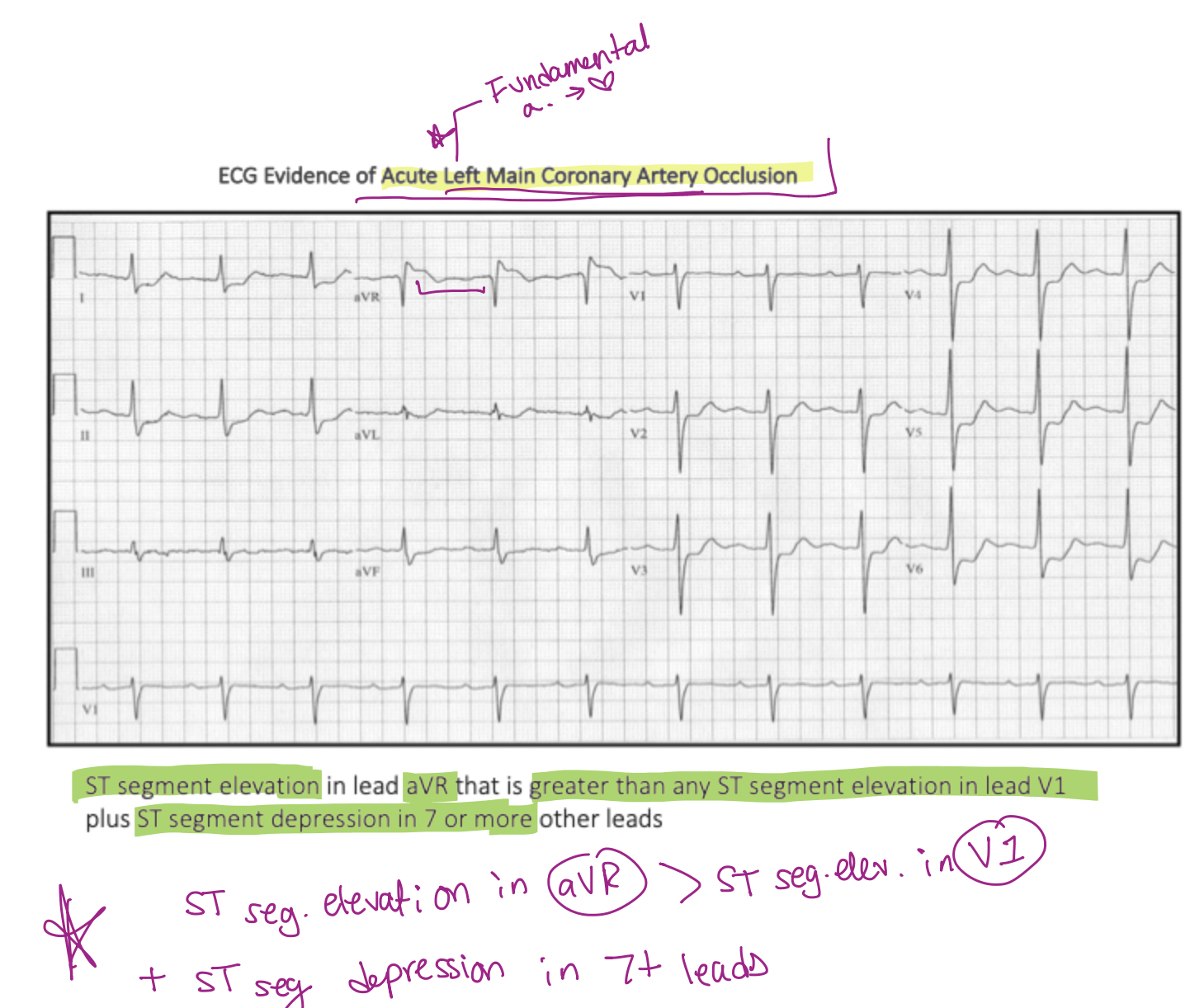
How many leads must show widespread ST depression to suspect a Left Main Coronary Artery Occlusion?
7 or more leads
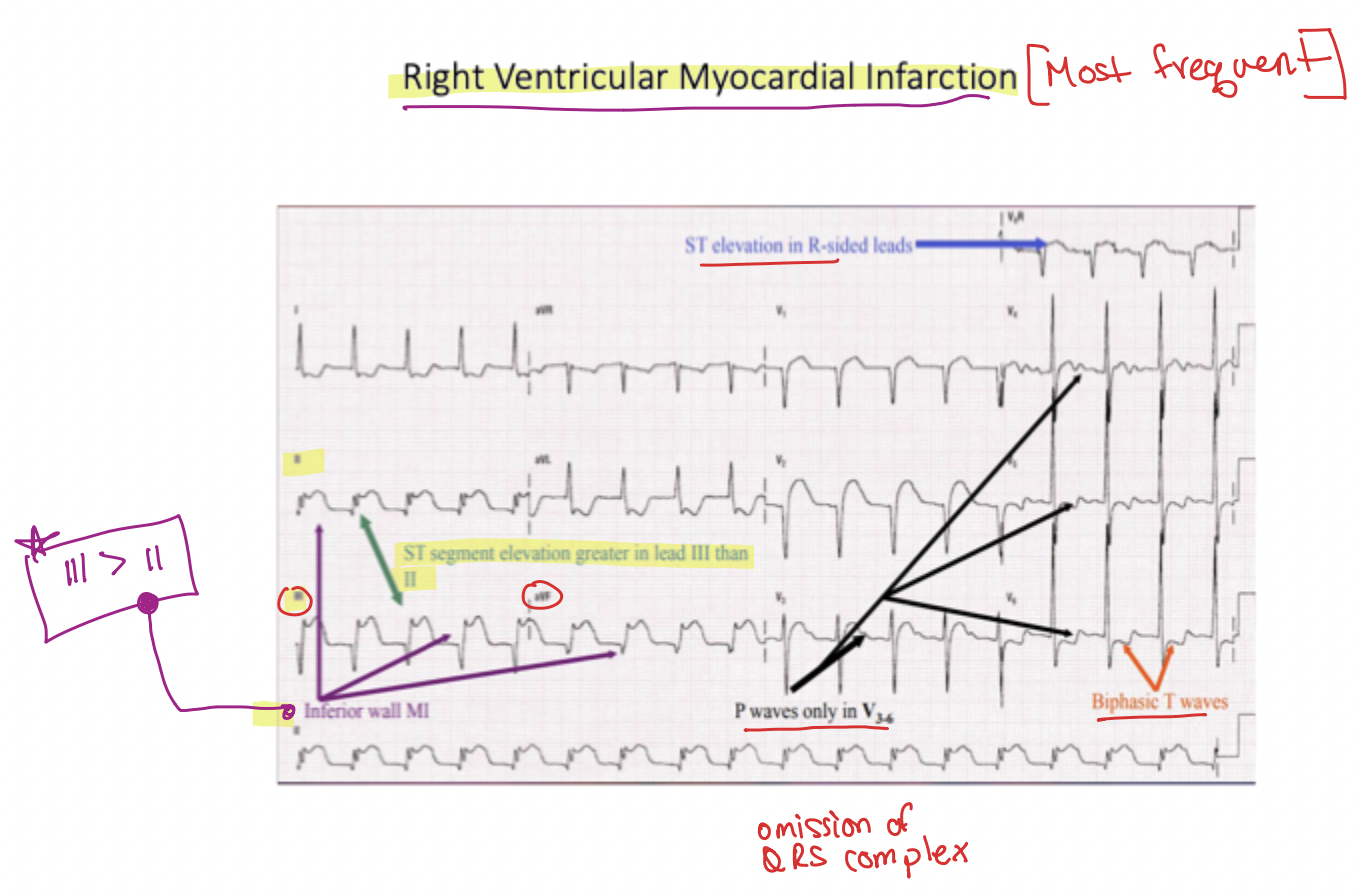
What lead relationship suggests a Right Ventricular MI in the context of an Inferior wall MI?
ST elevation in Lead III > II
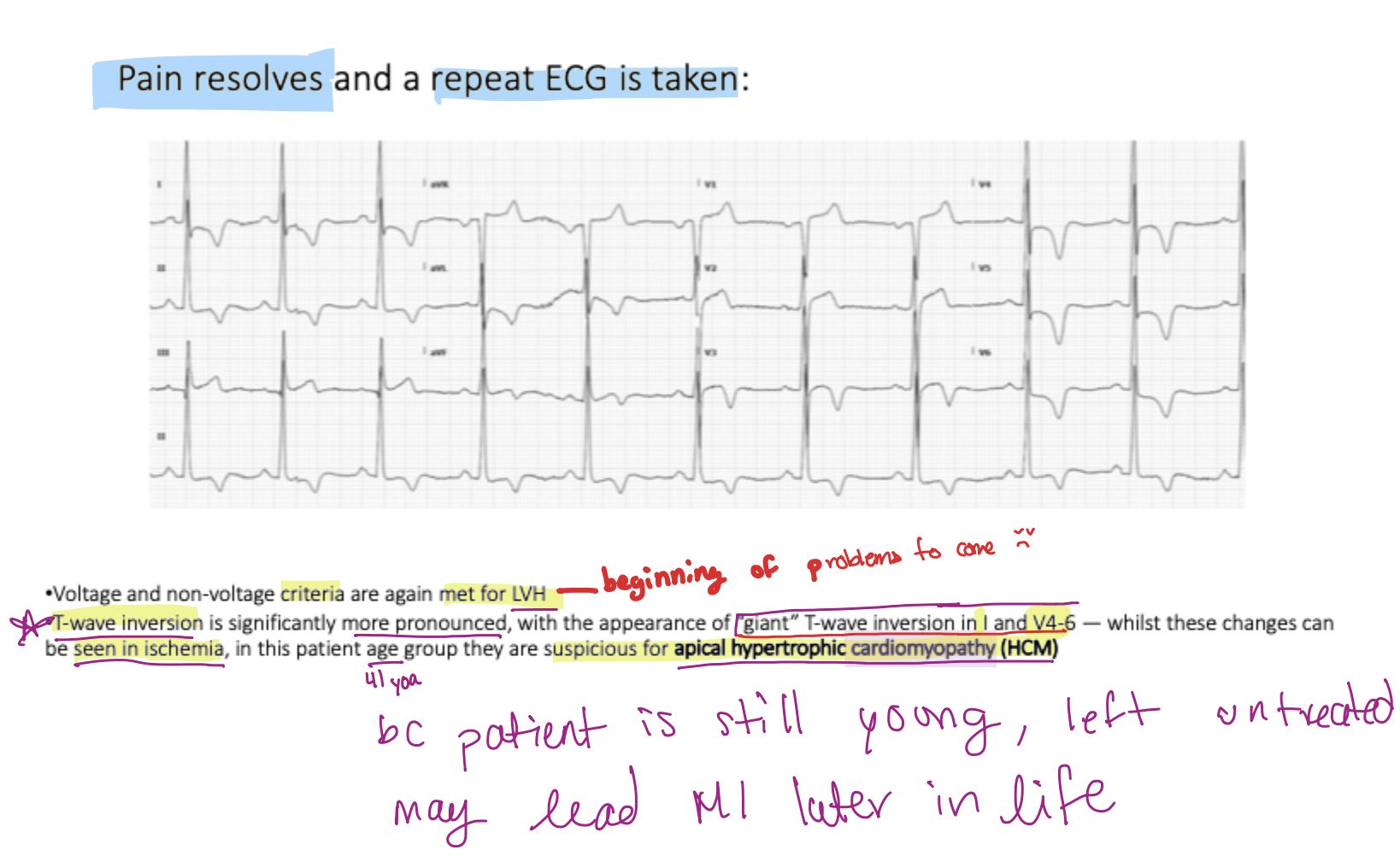
What condition mimics ischemia with 'giant' T-wave inversion in leads I, V4–V6, and voltage criteria for LVH?
Apical Hypertrophic Cardiomyopathy (HCM)
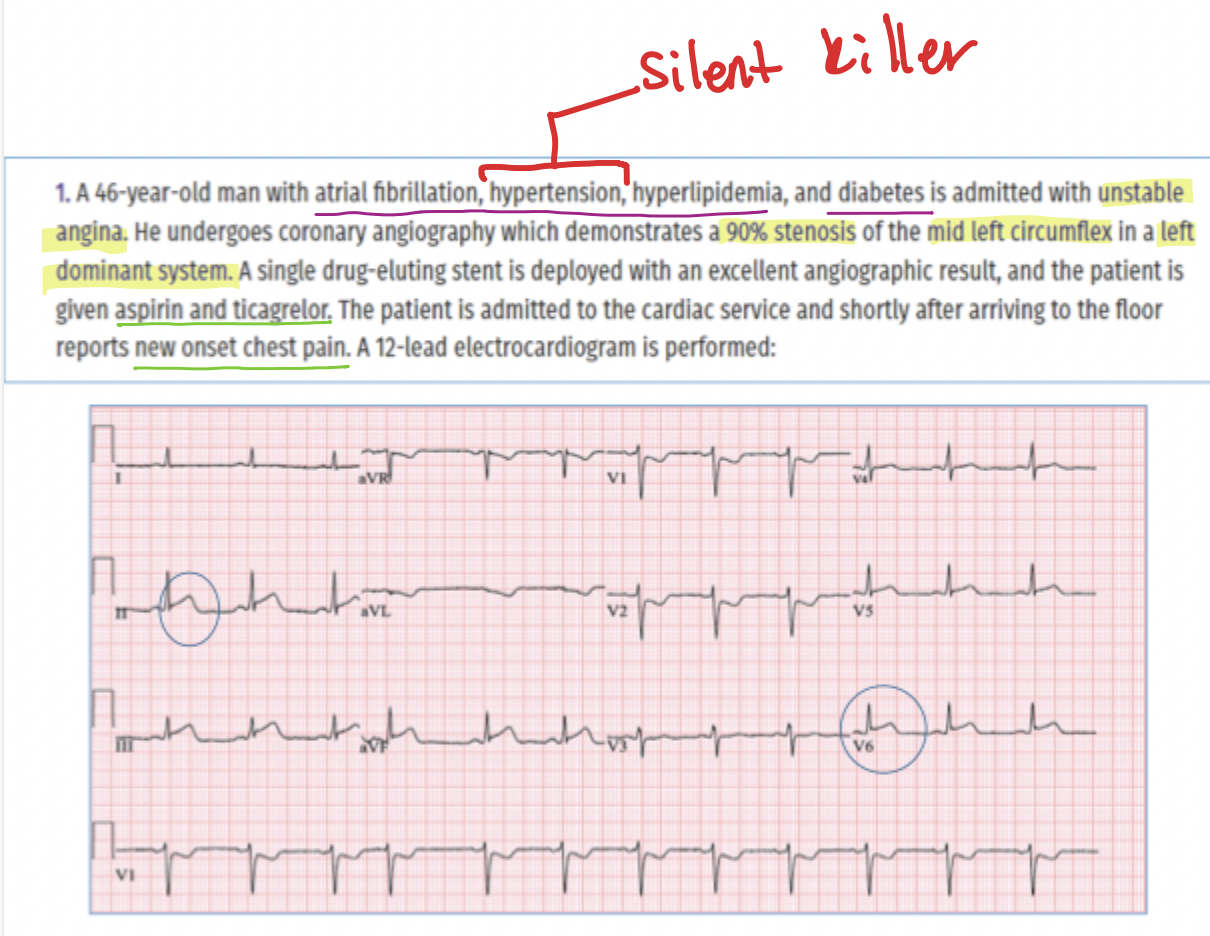
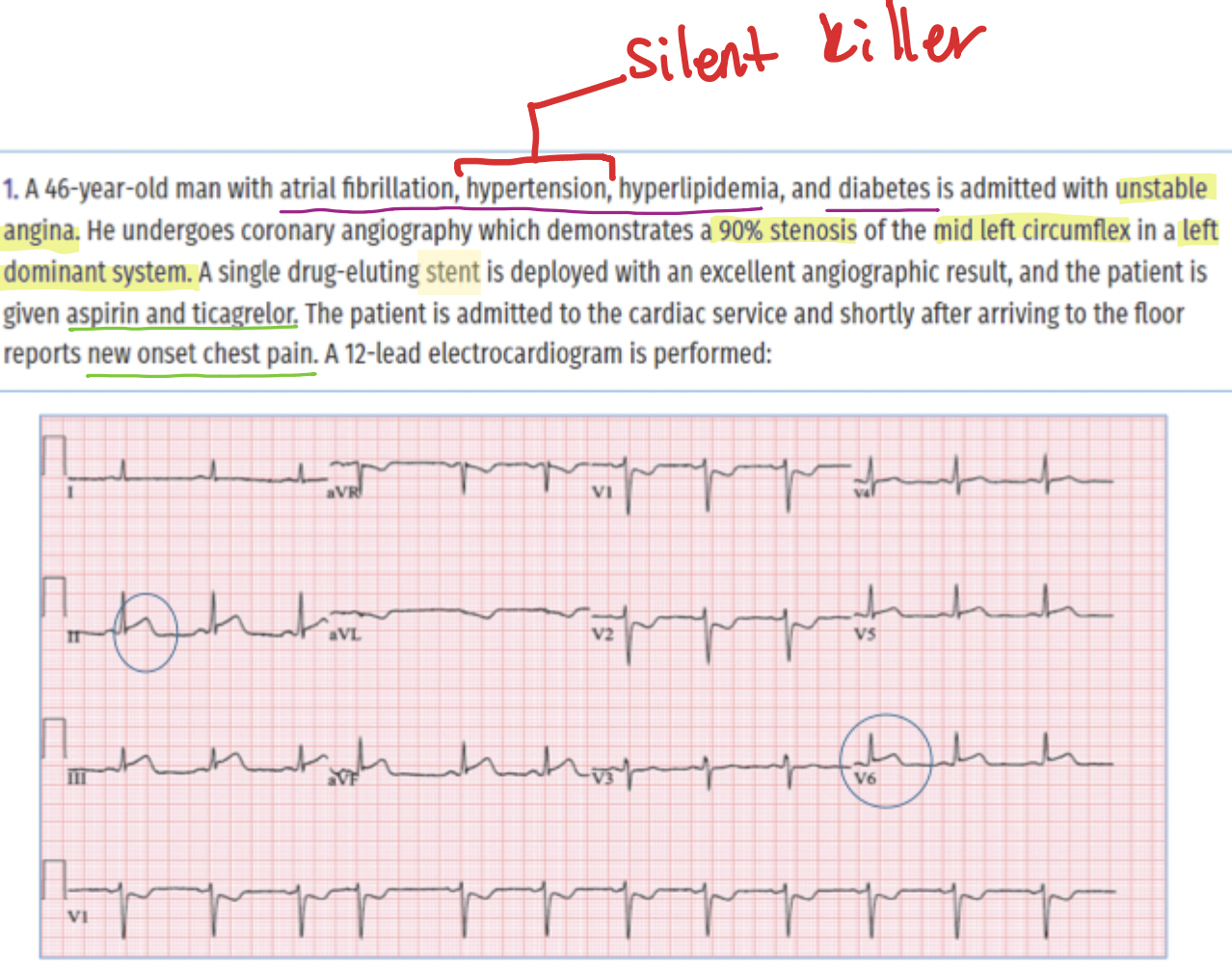
What is the clinical decision logic for a patient with new chest pain after an 'excellent' angiographic result and DAPT administration?
Urgent repeat coronary angiography due to suspected stent thrombosis or coronary dissection
What is the common side effect of Ticagrelor that might mimic cardiac symptoms?
Dyspnea (shortness of breath), which may be interpreted by the patient as chest tightness or pressure
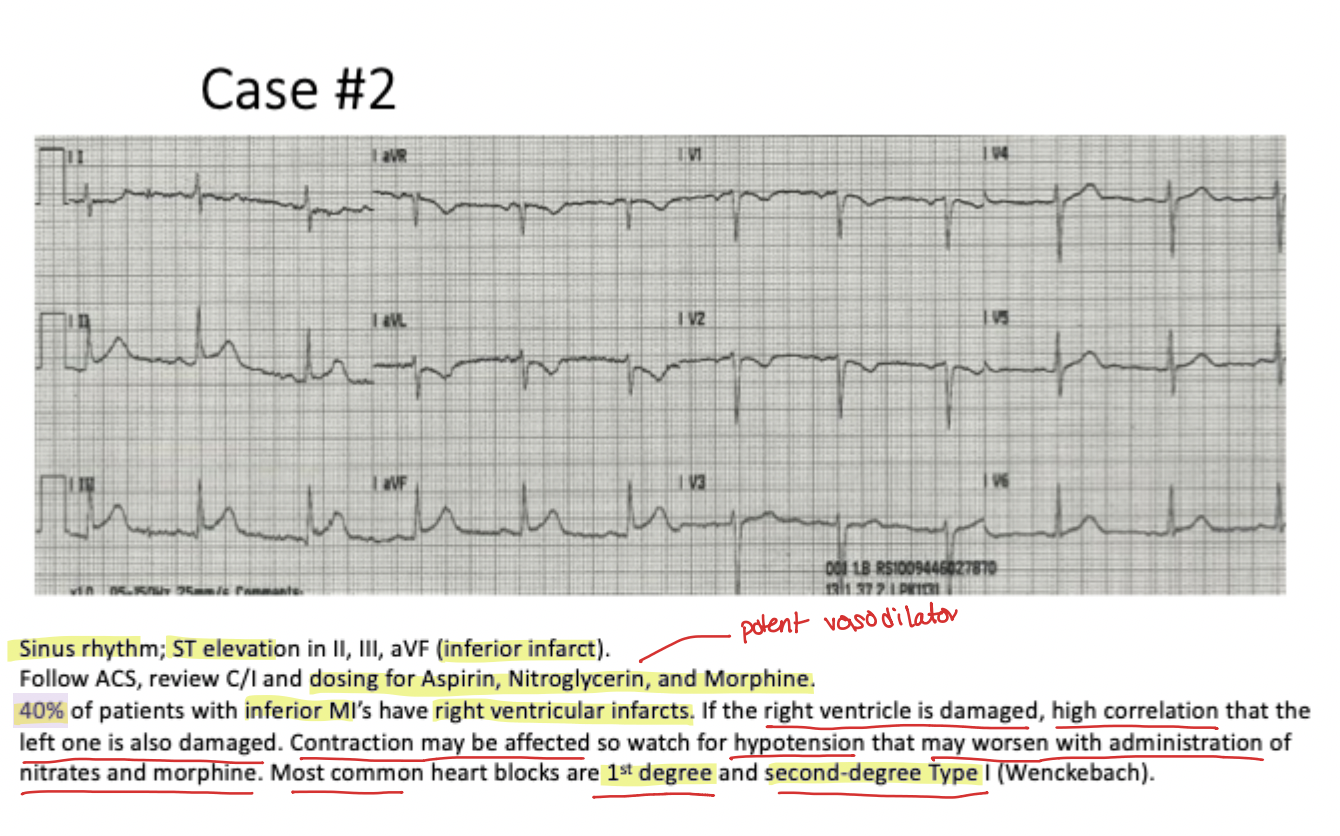
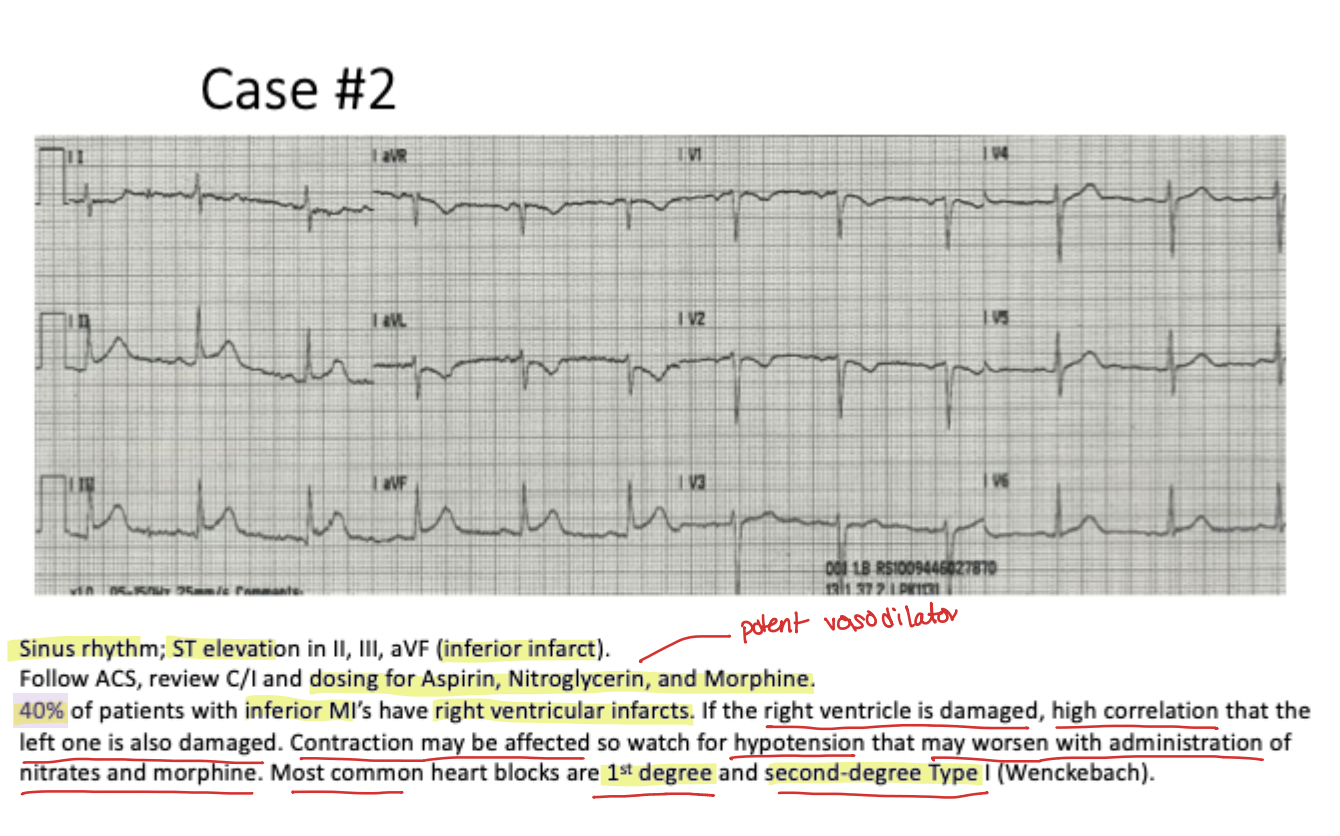
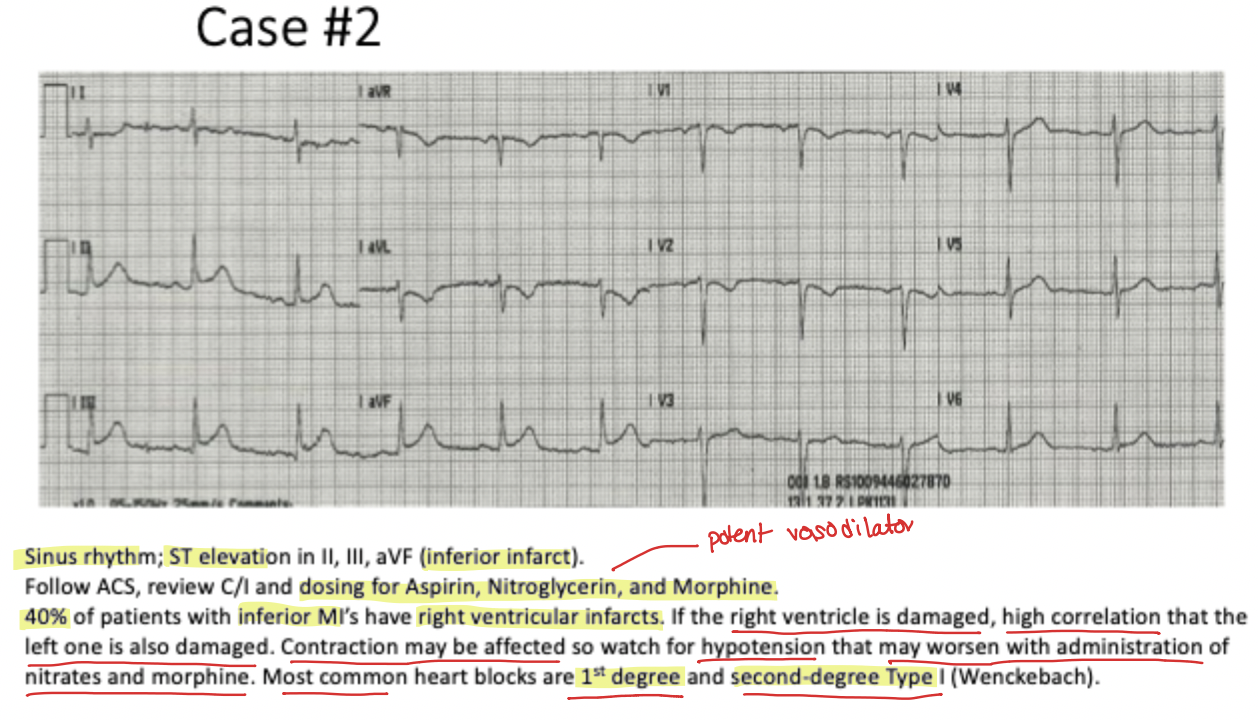
What % of patients with inferior MIs also have Right ventricular infarcts?
40%
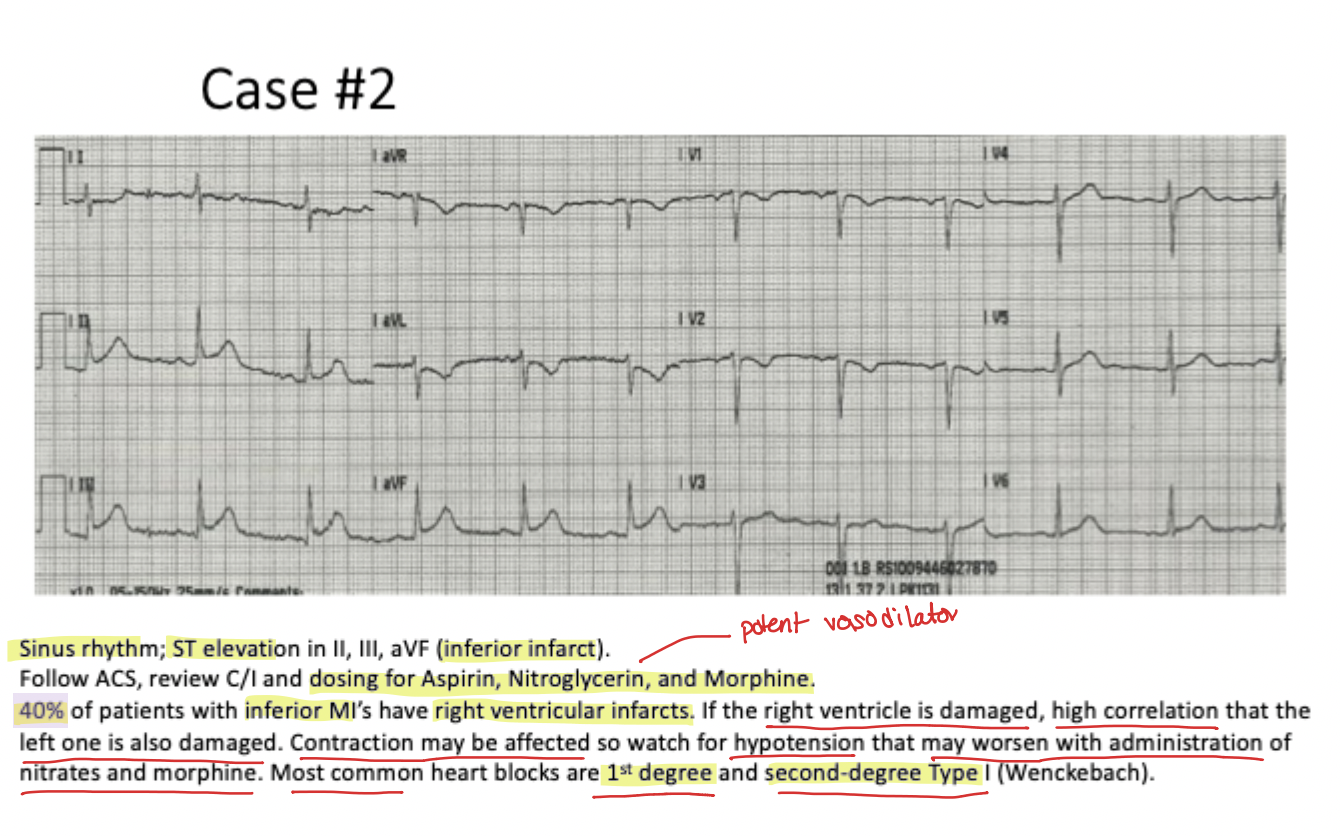
Why is it dangerous to administer nitrates or morphine to a patient with a Right Ventricular MI?
They are potent vasodilators that can cause life-threatening hypotension by further reducing the heart's pumping ability against impaired contraction
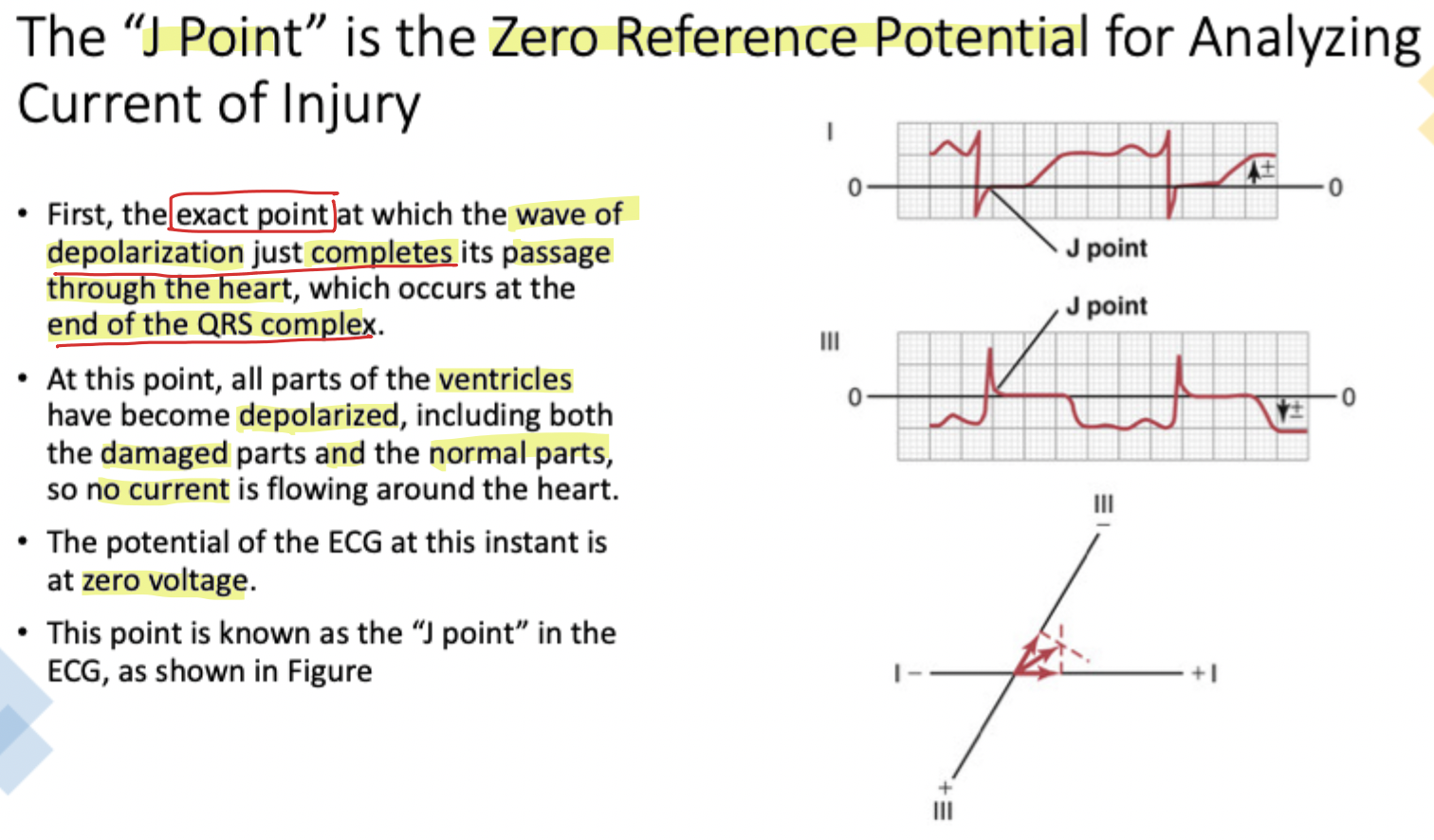
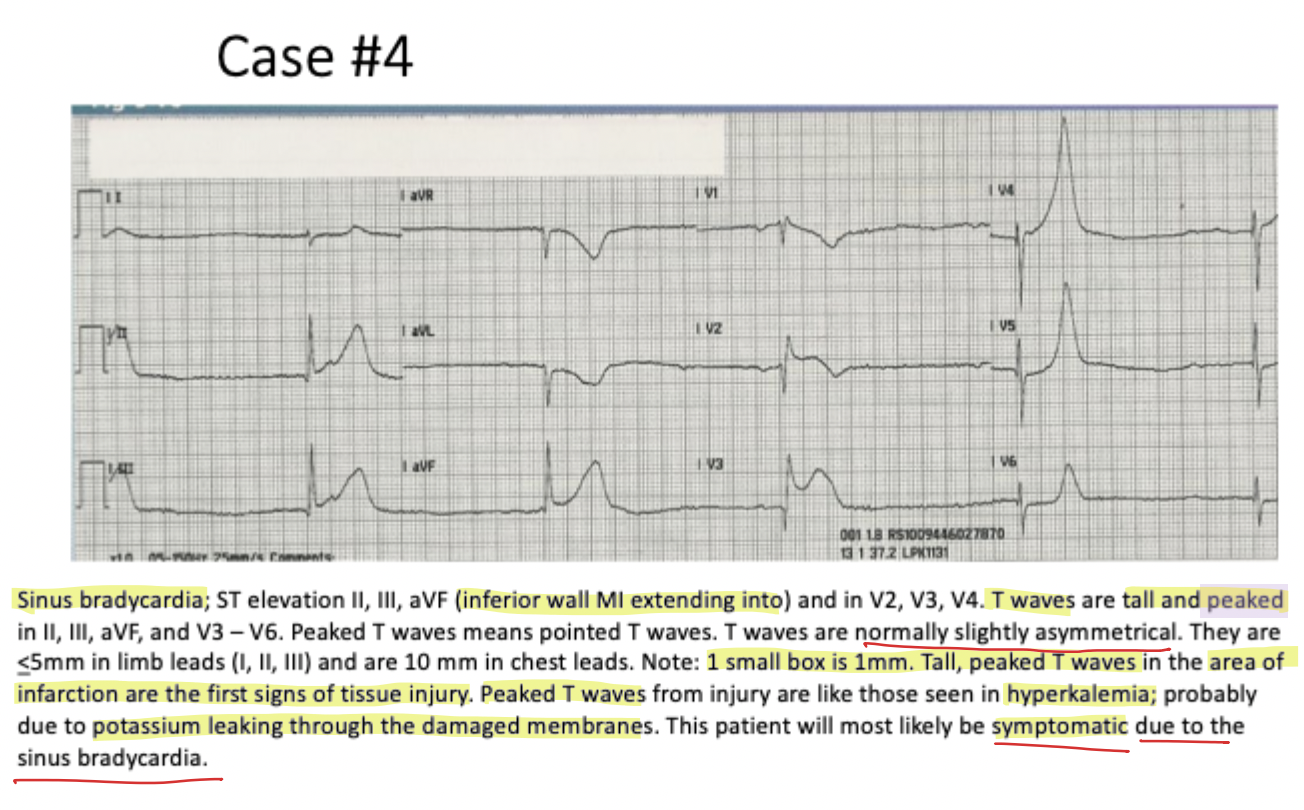
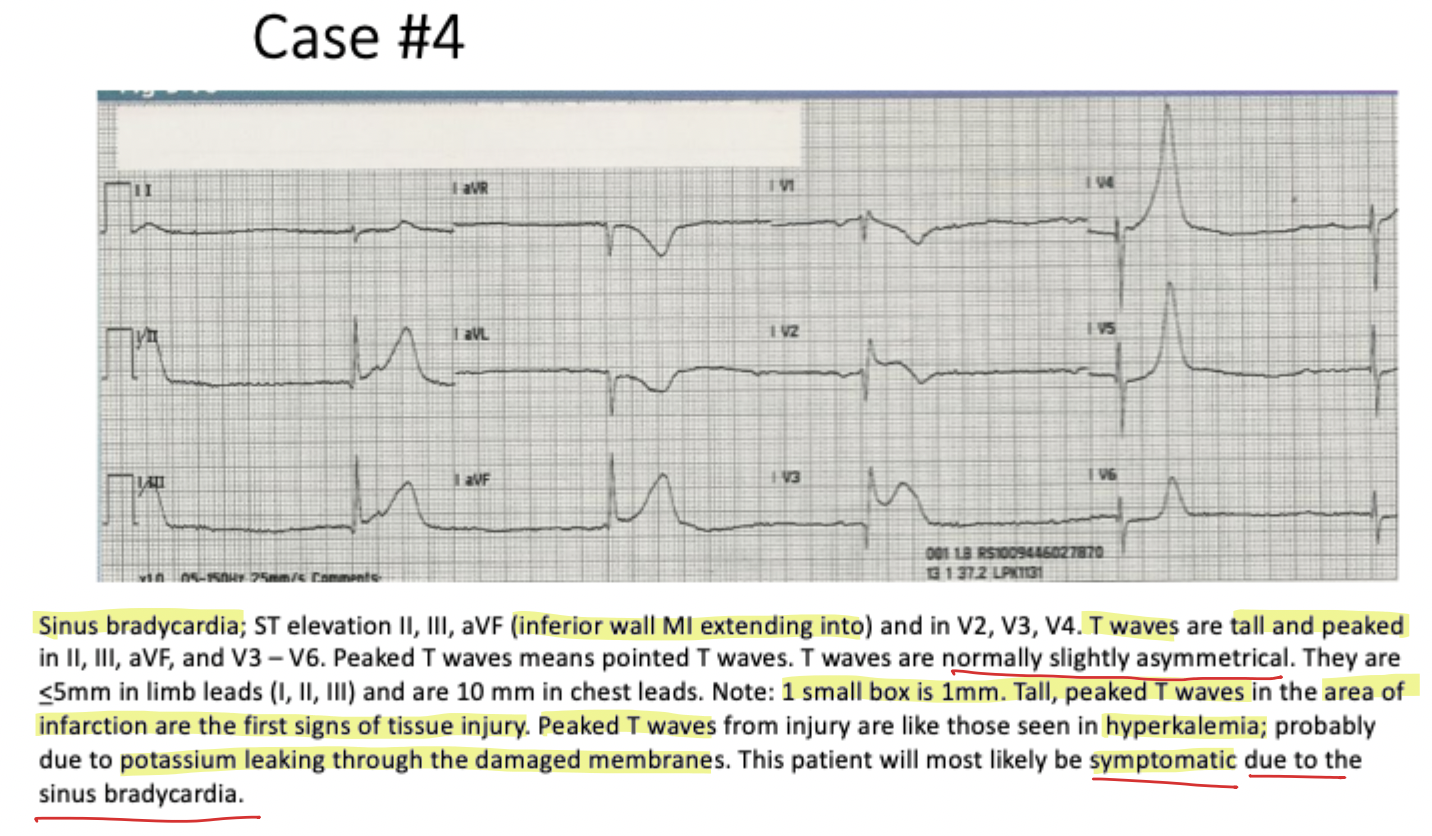
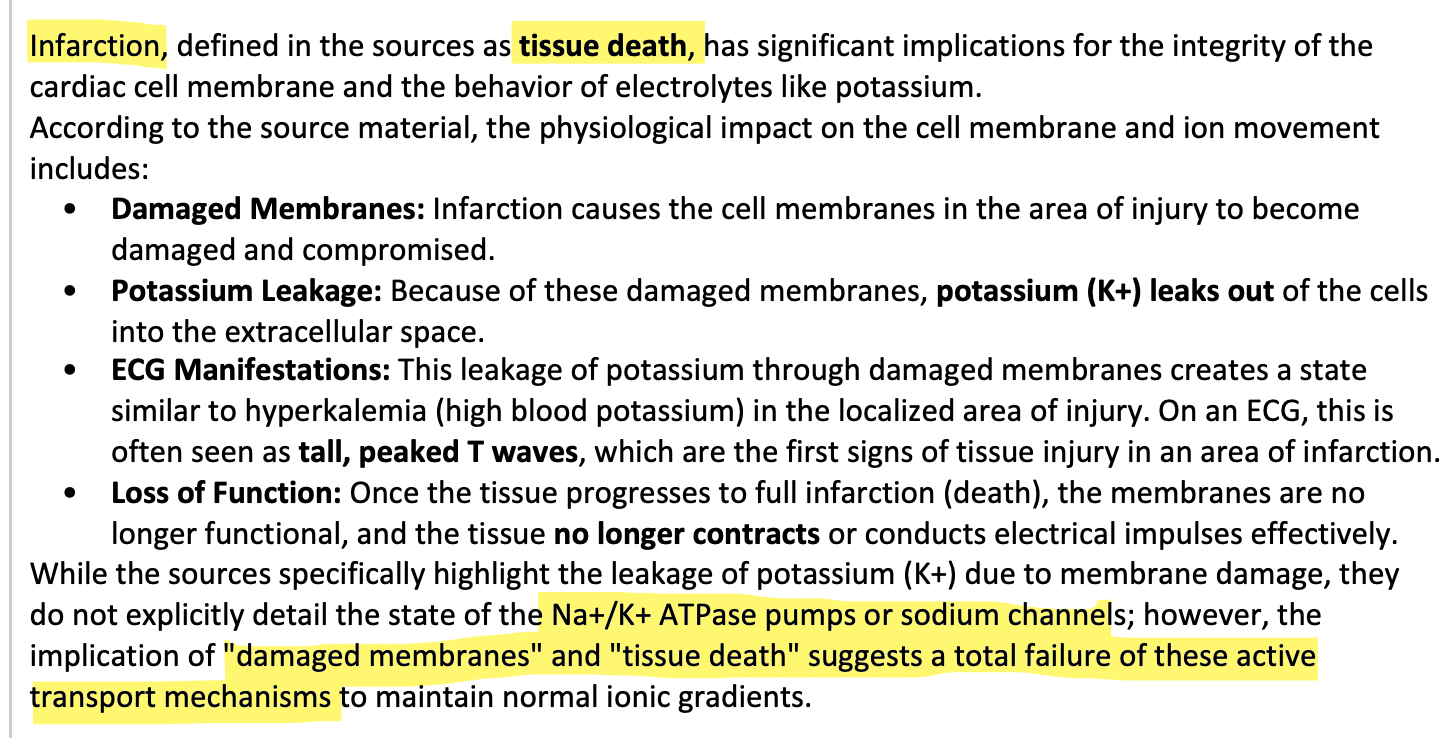
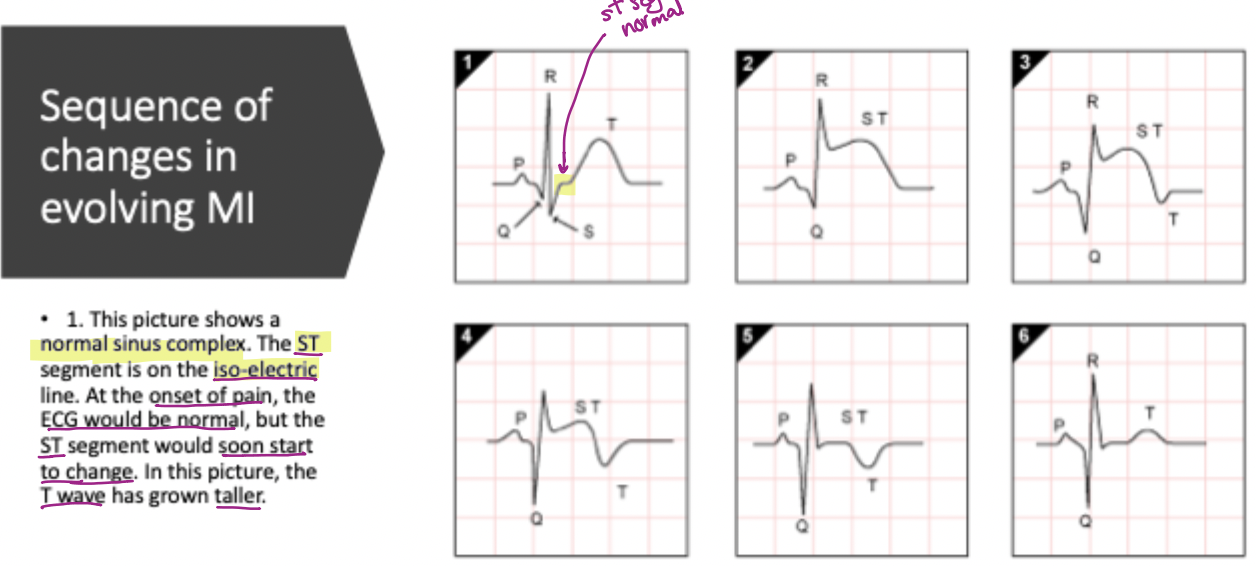
What physiological event causes tall, peaked T waves during the first signs of tissue injury?
Potassium (K+) leaking out of cells into the extracellular space through damaged membranes
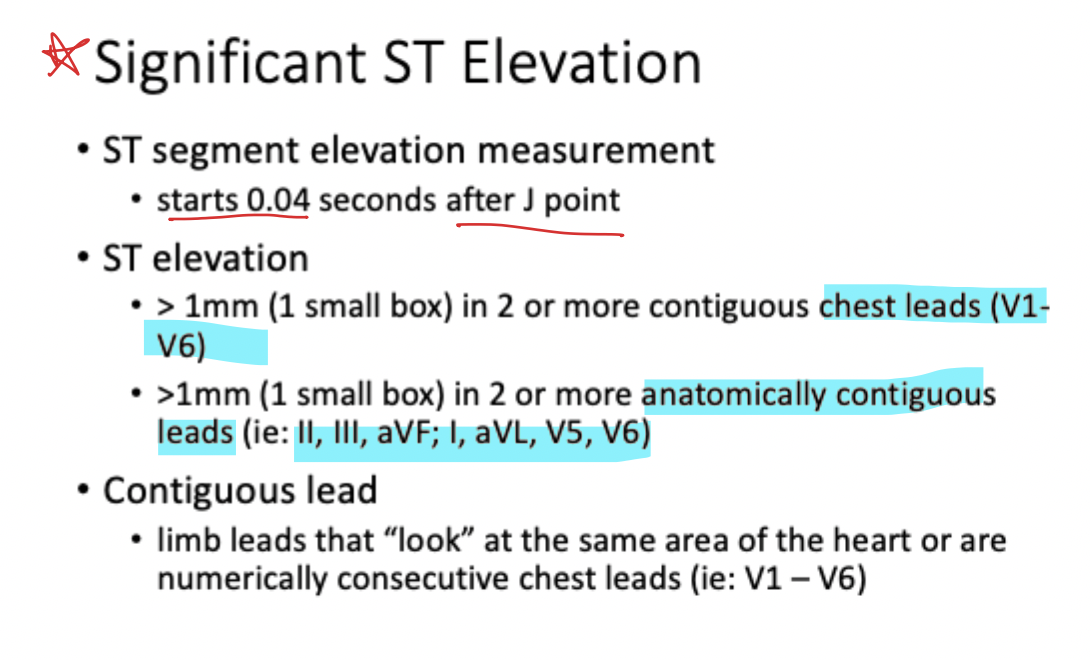
Where is the ST segment evaluated for elevation measurement relative to the J point?
0.04s (1 small box) after the J point
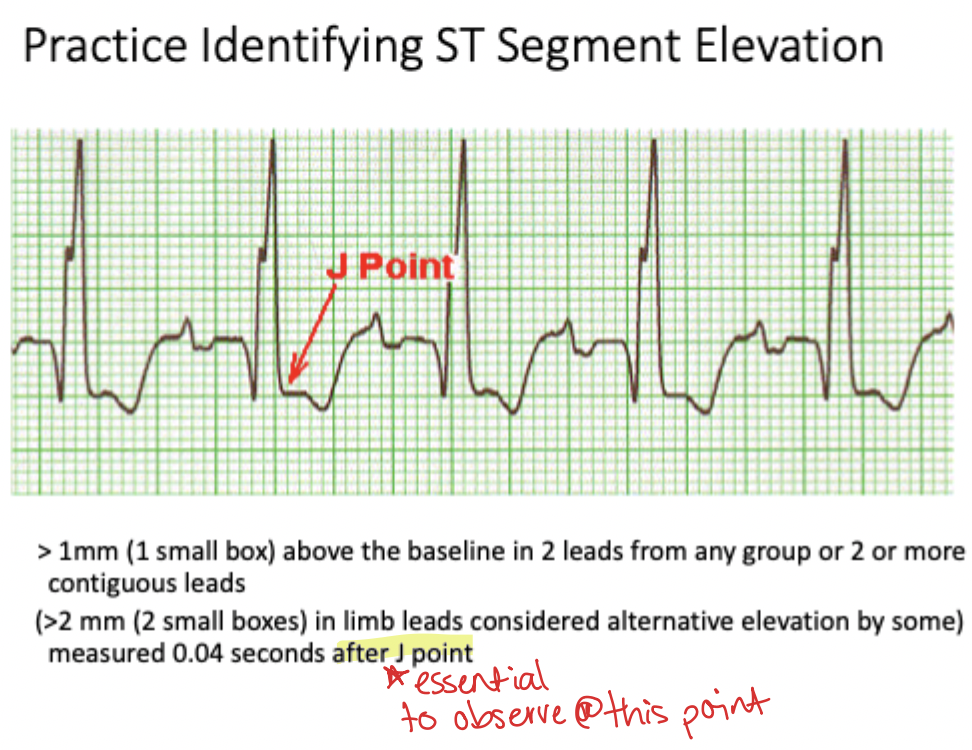
How much ST elevation is required in limb leads for some alternative criteria?
>2 mm (2 small boxes)
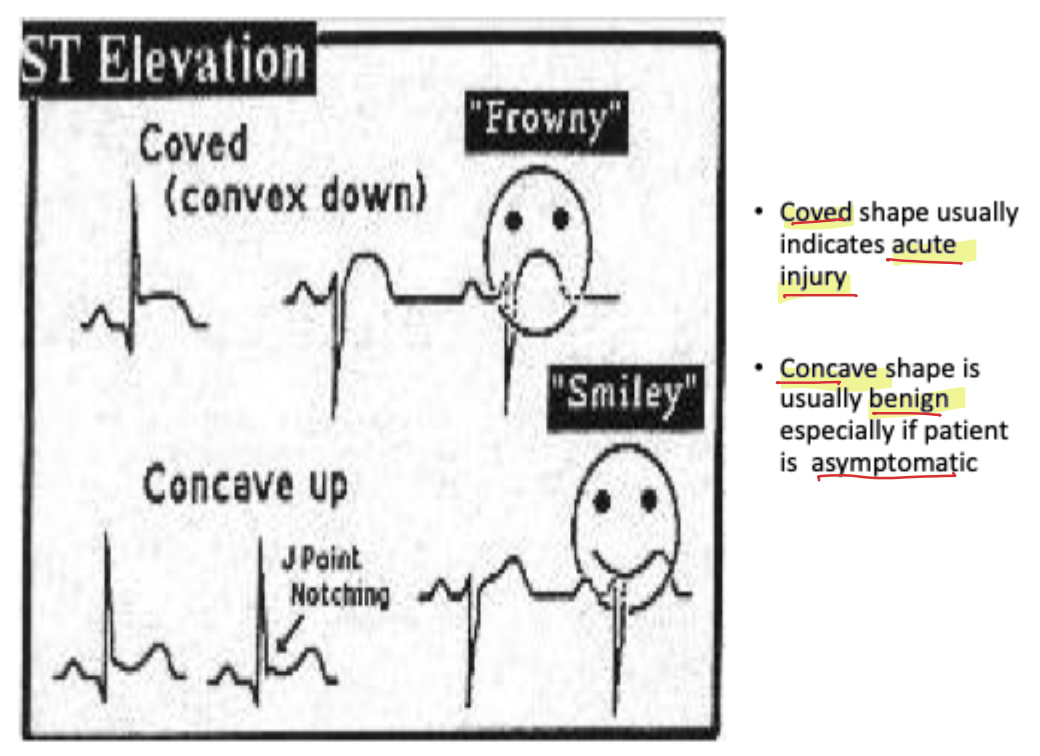
What does a 'Coved' or convex down (frowny) ST-segment shape usually indicate?
Acute injury
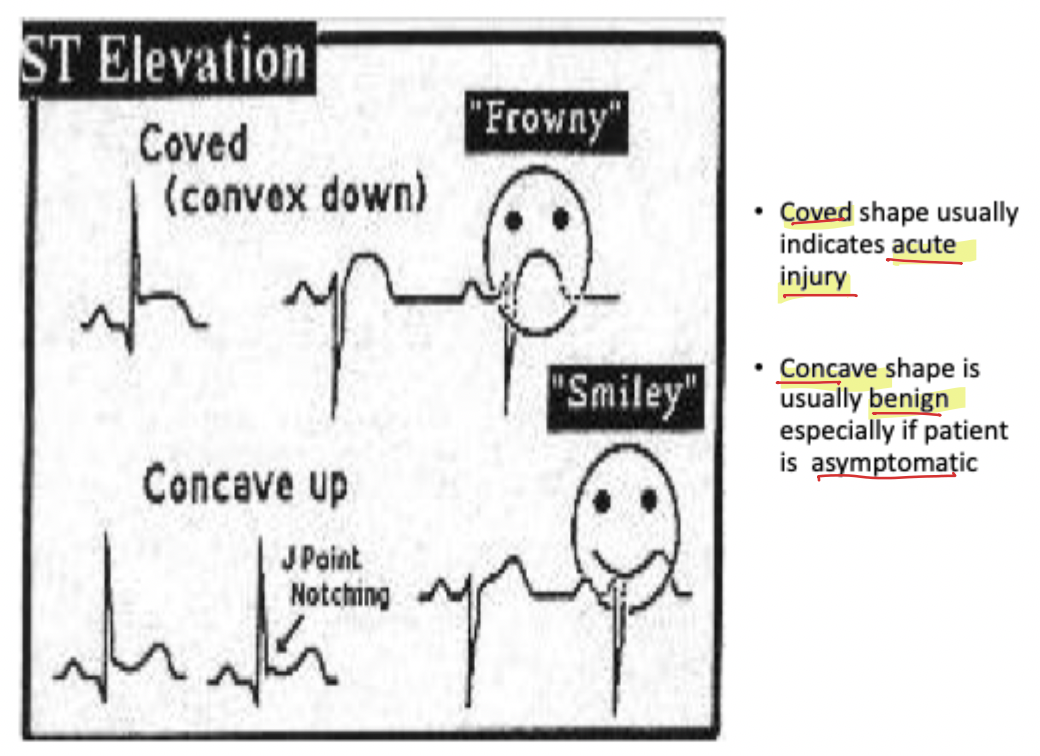
What does a 'Concave up' (smiley) ST-segment shape usually suggest?
Usually benign, especially if the patient is asymptomatic
In an aging MI (Age Unknown), what typically remains on the ECG?
Abnormal Q wave; ST segment and T wave have returned to normal
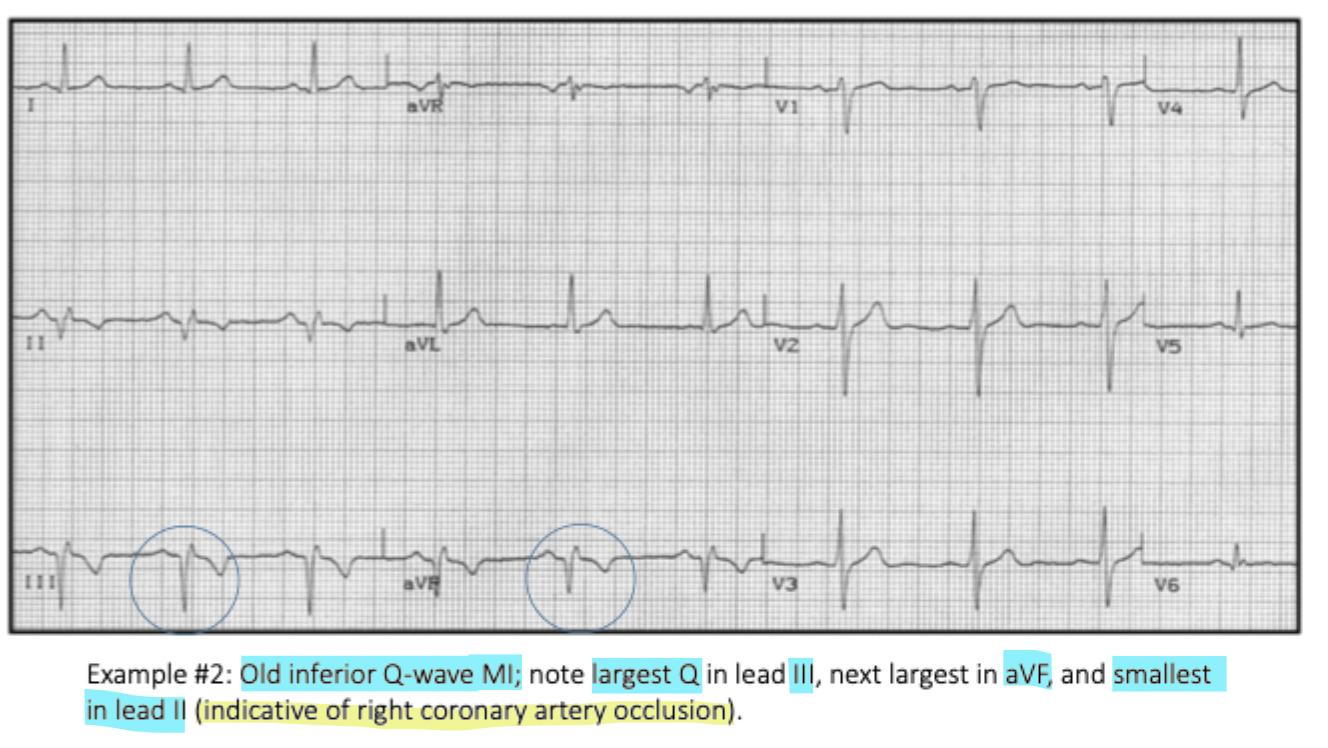
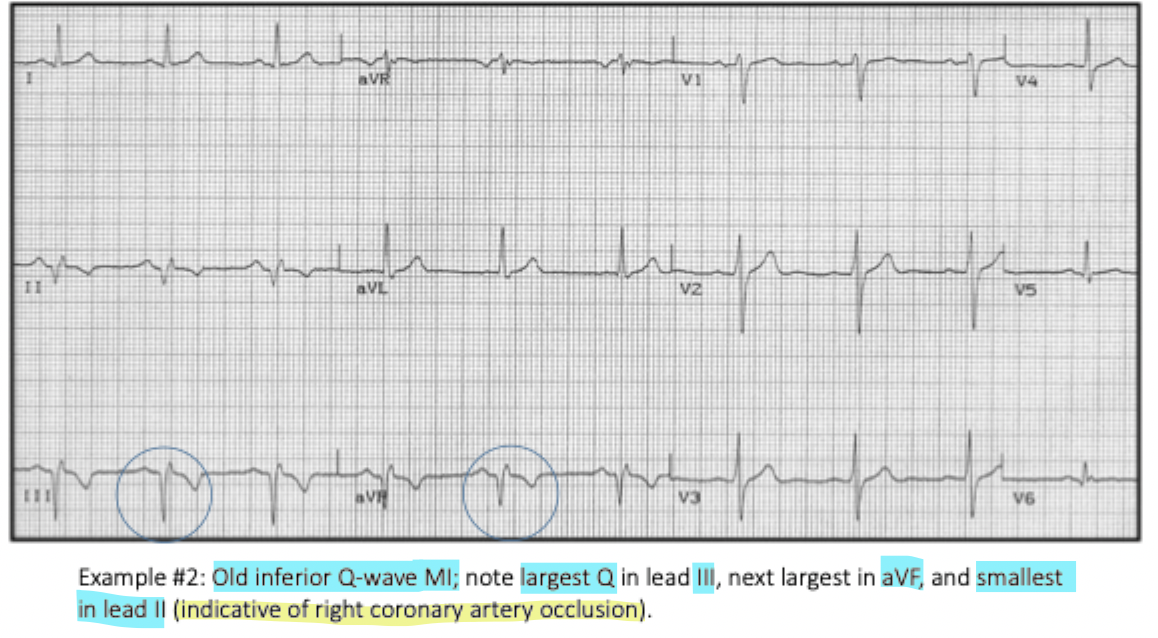
Which lead shows the largest Q wave in a typical inferior wall MI?
Lead III
Which leads view the 'Laterial wall' according to the localization chart?
I, aVL, V5, V6
What is 'Infarction' defined as in the lecture notes?
Tissue death
What is the purpose of Dual Antiplatelet Therapy (DAPT) post-stent?
ex Aspirin & ticagrelor
To prevent blood from clotting on the foreign surface of the newly placed drug-eluting stent
What are the standard medical ranges for BP, Pulse (P), and Respiration (R) mentioned for comparison?
BP 120/80
P 60–100
R 12–20
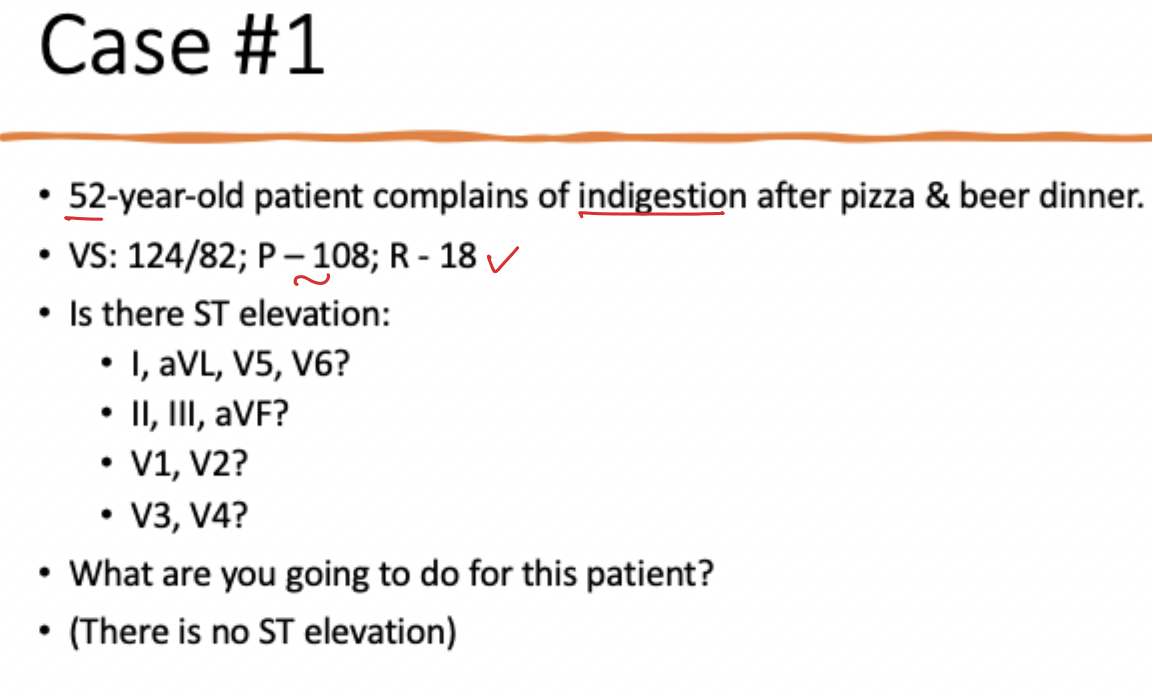
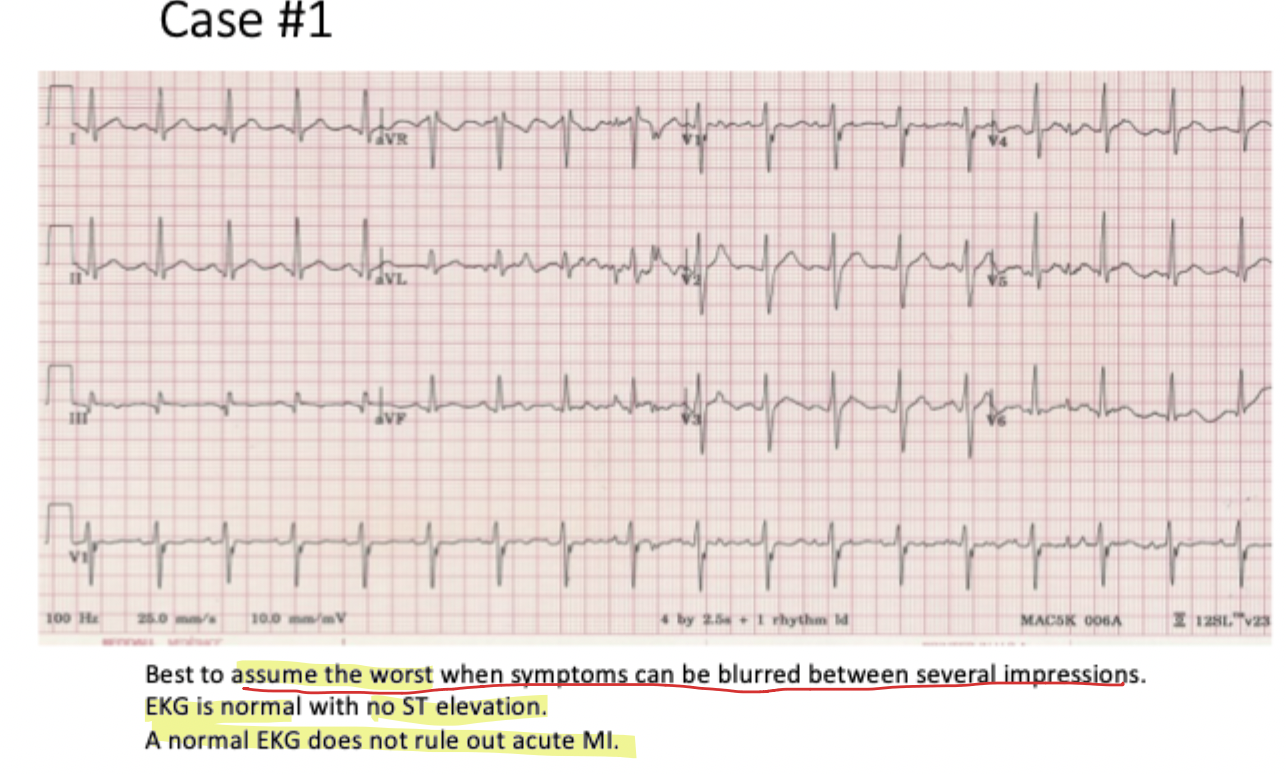
In Case #1, why was a normal ECG not enough to rule out MI?
The clinician must 'assume the worst' because cardiac symptoms often mimic gastric issues like indigestion
What Happens: A 52-year-old reports indigestion after a heavy meal. Vital signs show mild tachycardia (P=108), but the ECG is normal with no ST elevation.
Logic: Clinicians must "assume the worst" because cardiac symptoms often mimic gastrointestinal issues like indigestion.
Association: It is critical to remember that a normal ECG does not rule out an acute MI, especially if the patient is symptomatic.
What are the most common heart blocks associated with Inferior Wall MI?
1st & 2nd degree Type I (Wenckebach)
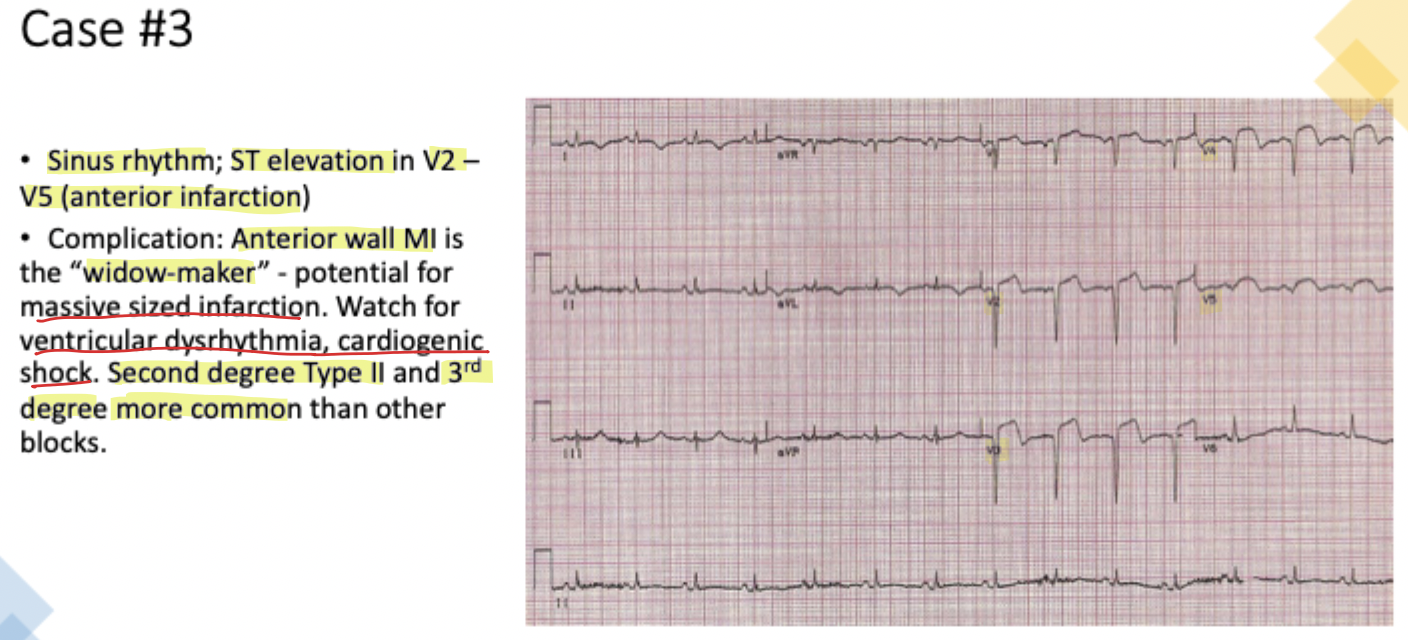
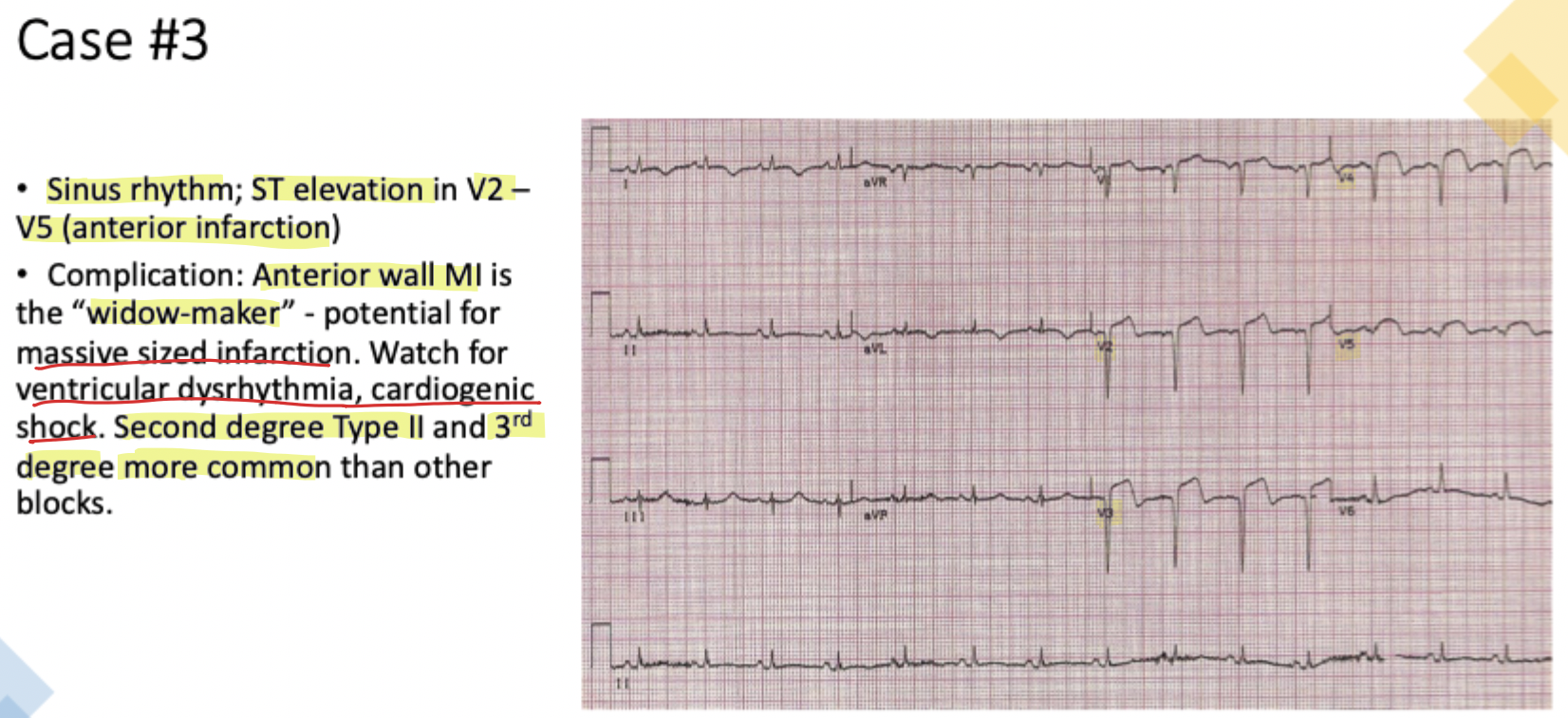
Why is an Anterior Wall MI (leads V2–V5) known as the 'widow-maker'?
It involves the largest part of the heart muscle and carries a potential for massive infarction, cardiogenic shock, and ventricular dysrhythmias
What Happens: A 45-year-old presents with chest heaviness and hypotension (90/56). The ECG shows ST elevation in leads V2–V5.
Logic: This indicates an Anterior Wall MI, which involves the largest part of the heart muscle.
Association:
Severity: This is known as the "widow-maker" due to the potential for massive infarction.
Complications: High risk for cardiogenic shock and ventricular dysrhythmias.
Heart Blocks: More dangerous blocks like 2nd degree Type II and 3rd degree are common.
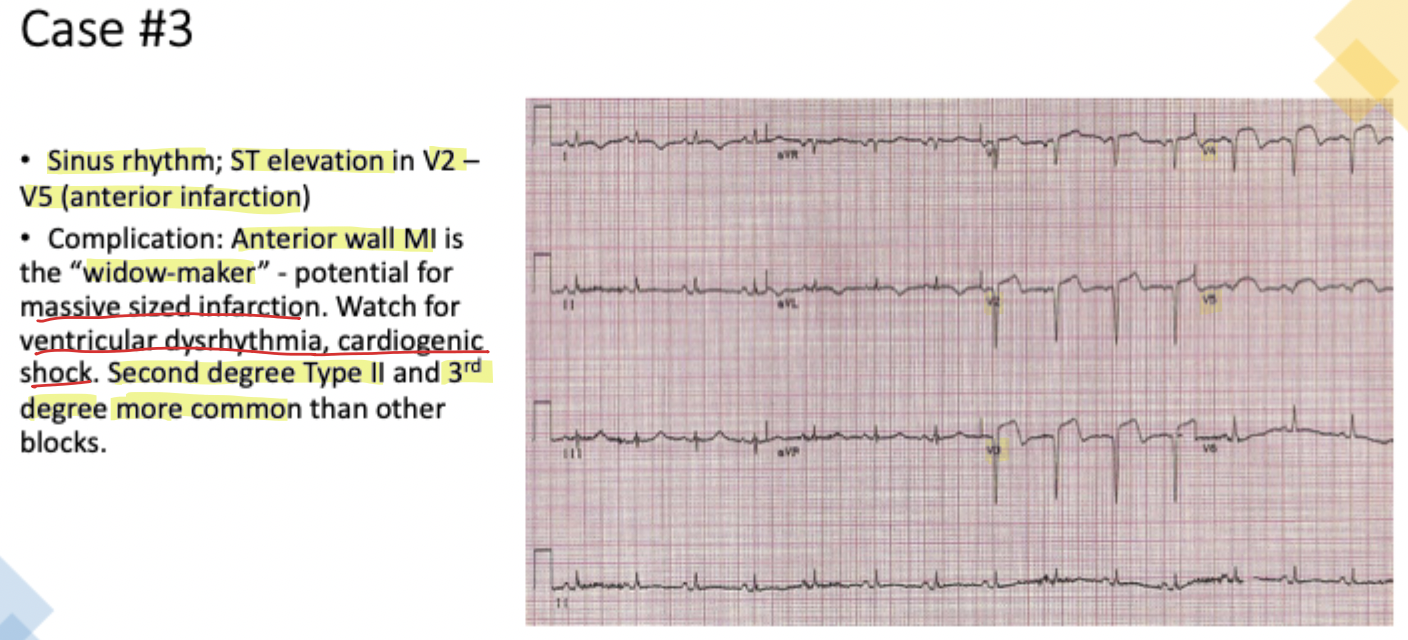
Which heart blocks are common and dangerous in the setting of an Anterior Wall MI?
2nd degree Type II & 3rd degree
In Case #4, what was the clinical consequence of the patient's pulse of P=30?
Symptomatic bradycardia leading to dizziness due to reduced oxygen delivery to the brain
What Happens: An 87-year-old presents with dizziness and extreme fatigue. Her pulse is dangerously slow (P=30). The ECG shows ST elevation in leads II, III, aVF, and V2–V4, along with tall, peaked T waves.
Logic: The patient has an extensive MI covering both the inferior and anterior walls. The tall, peaked T waves are the first sign of tissue injury.
Association:
Ionic Cause: These peaked T waves occur because potassium leaks through damaged cell membranes, mimicking hyperkalemia in the local area of injury.
Symptomatic Bradycardia: The patient's dizziness is logically associated with the severe sinus bradycardia (P=30), which drastically reduces oxygen delivery to the brain.
What is the normal amplitude for a T-wave in the limb leads?
≤5mm
What is the normal amplitude for a T-wave in the chest leads?
≤10mm
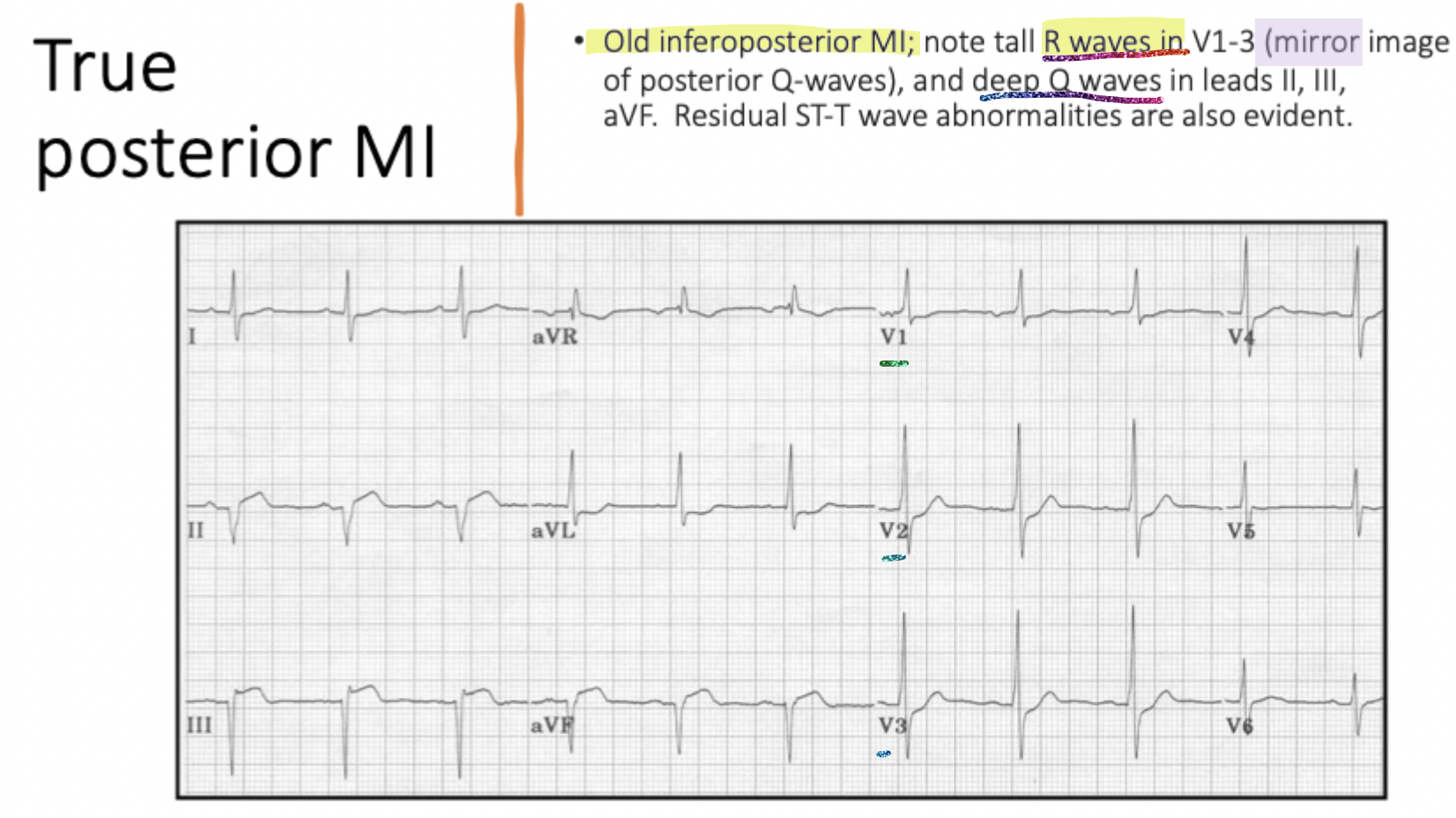
What does the presence of tall R waves in V1-V3 suggest regarding posterior injury?
It is a mirror image of posterior Q-waves
True or False: Fibrous tissue can contribute to the heart's pumping action.
False; fibrous tissue is non-contractile
Fibrous tissue cannot replace muscle to produce a normal ECG because it is essentially dead tissue that no longer contracts and does not conduct electrical impulses in the same way as healthy myocardium. While the heart uses fibrous tissue (scarring) to repair the area damaged during a myocardial infarction (MI), this tissue lacks the physiological properties required for the heart's electrical cycle to return to its original "normal" state.
What does an ECG potential of zero voltage at the J point signify about the ventricles?
Both damaged and normal parts are fully depolarized
Why is identifying past events (permanent Q waves) vital for a patient’s history?
A pathological Q wave is not 'time-specific' and serves as a permanent record of a previous heart attack
What is the primary indicator of True Posterior Injury?
Reciprocal ST depression in V1–V3
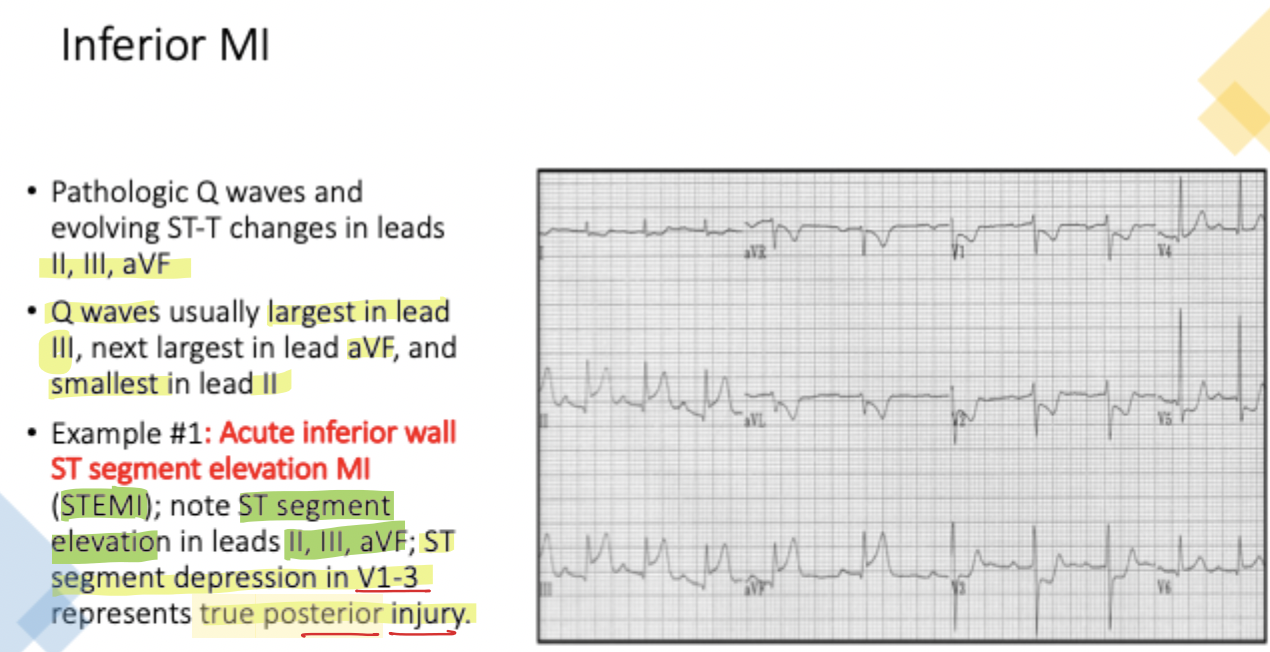
In Case #2, a patient with chest and jaw pain had ST elevation in II, III, and aVF. What is the diagnosis?
Inferior Wall MI
If thrombolysis is successful, what change do we expect in the ST segment within 90 minutes?
50% reduction in elevation
Where are leads V7-V9 located when doing a 15-lead EKG?
On the patient's back at the 5th intercostal space
What is the time value of 37.5 Big Boxes?
7.5 Seconds
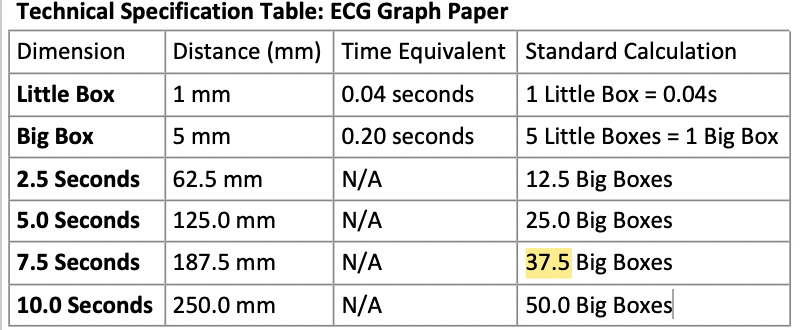
What is the distance equivalent for 2.5 seconds on ECG paper?
62.5mm
In the 'Marriage' metaphor, what does a divorce with more P's than QRS's specifically indicate?
Heart Block
How does necrosis affect the cell's active transport mechanisms?
There is a total failure of the Na+/K+ ATPase pumps to maintain normal ionic gradients
What is the 'Success Marker' time frame for thrombolytic efficacy?
90 min
Which artery is most associated with an Inferior Q-wave MI?
Right Coronary Artery (RCA)
How is significant ST elevation defined in contiguous chest leads?
>1mm in 2+ leads (V1-V6)
What are the defining characteristics of 'Sinus Rhythms'?
Rate varies from standard range, but focus is standard
What occurs at the 'Onset' stage of an evolving MI on an ECG?
Normal sinus complex or hyperacute T-wave changes (increased amplitude/width)
Identify the ECG leads for the 'Septum' group.
V1, V2
Identify the ECG leads for the 'Lateral Wall' group.
I, aVL, V5, V6
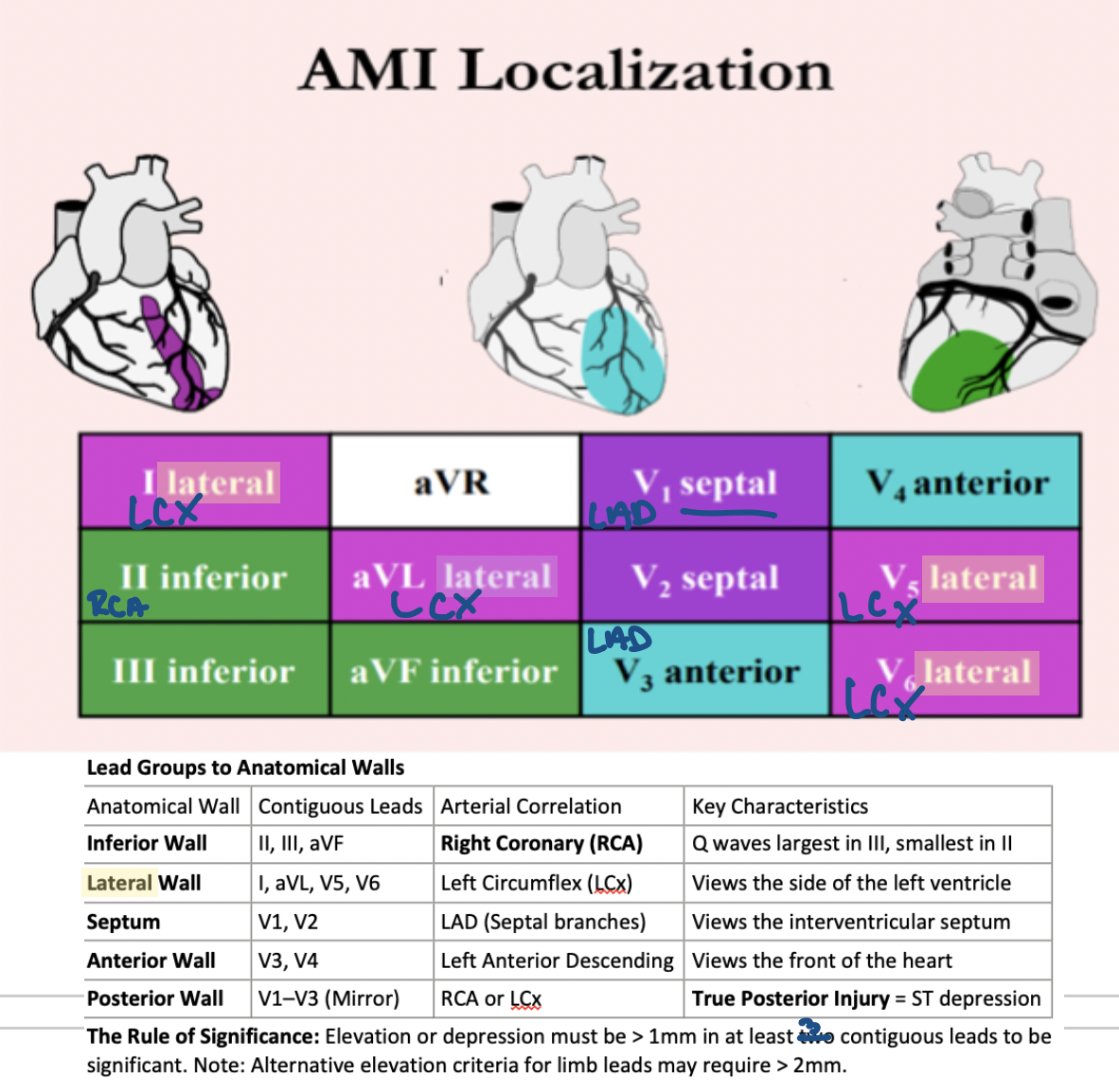
What is the anatomical wall associated with leads II, III, and aVF?
Inferior Wall
What provides the 'zero-reference' for analyzing ST-segment deviation?
The J point
How much deviation is required for an ST segment to be considered significant?
> 1\,mm
Does a pathological Q wave indicate an acute emergency?
No, it represents stable scar tissue and is not time-specific
What is the diagnostic significance of a permanent Q wave?
It helps distinguish b/w acute injury (ST elevation) and old necrosis
How can clinicians localize which coronary artery was occluded after an MI has healed?
By identifying the location of fibrous tissue (deep Q waves) in specific leads
A deep Q wave in leads II, III, and aVF indicates what past event?
An old inferior wall MI
In the 12-Lead Master Chart, what is the 'Physiological Focus' of Atrial Rhythms?
Atrial depolarization focus/ P wave abnormality
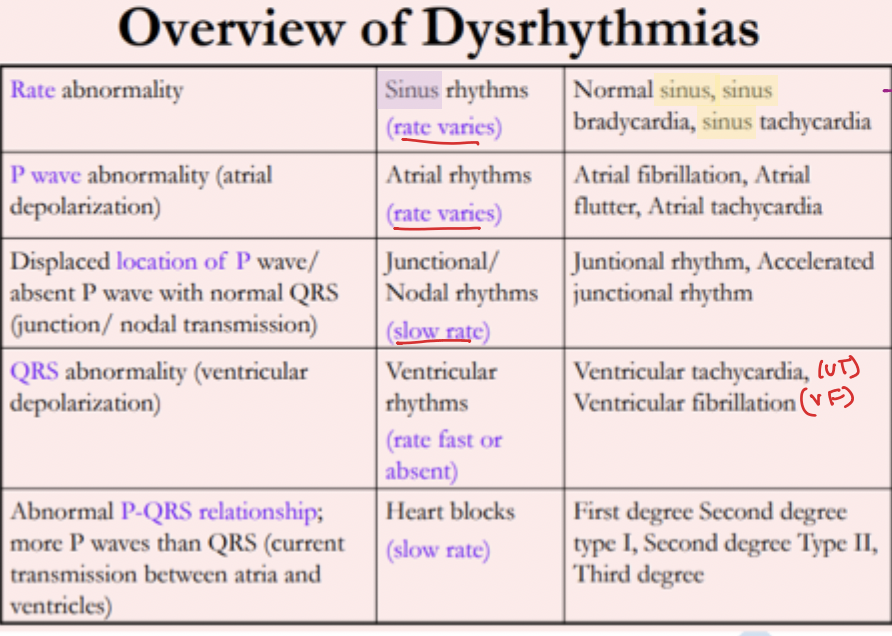
What is the hallmark physiological focus of Heart Blocks?
Current transmission focus b/w atria & ventricles
What category does Sinus Bradycardia fall under?
Rate Abnormality / Sinus Rhythms
What category does Accelerated Junctional fall under?
Junctional/Nodal Rhythms
Why is ST elevation evaluated 0.04 seconds after the J point?
To ensure measurement is taken after the point where the QRS meets the baseline
Case #3 shows ST elevation in V2–V5. What part of the heart is infarcted?
Anterior wall
What is the arterial correlation for a Septal MI (V1, V2)?
LAD (Septal branches)
A 46-year-old post-stent patient develops new chest pain. Clinically, what is always logically assumed?
That the 'excellent' blood flow has been interrupted due to mechanical failure (stent thrombosis) —need urgent repeat coronary angiography
What do tall, peaked T-waves mimic in localized tissue injury?
Hyperkalemia
What should you do if a patient has ST elevation of 1mm in leads II and aVF?
Treat as significant, as these are contiguous inferior leads
In MI evolution, what happens to the ST segment when T-waves become deep and inverted?
The ST elevation typically reduces (by 50%) —reperfusion indicator (blood flow returning to damaged area)
What is the first sign of tissue injury in the area of infarction?
Tall, peaked T waves
What is the BP and Pulse in Case #3?
BP 90/56; Pulse 86
The J point occurs at the moment which wave completes its passage?
The wave of depolarization
What is the relation b/w dead tissue amount and heart function?
The amount of dead tissue (fibrosis) is directly related to the degree of permanent muscle impairment
What is the maximum normal Q-wave duration?
< 0.04\text{ s}
What is the clinical shorthand for 'Related' in systematic analysis?
Fixed PR interval with P waves fixed to QRS
The 3 R’s:
Regular: Is the distance between complexes constant?
Rate: Is it fast, slow, or normal?
Related: Are the P waves "Married" to the QRS complexes with a fixed PR interval?
The "Marriage" metaphor is the gold standard for evaluating AV synchrony.
A "divorce"—or an abnormal P-QRS relationship—indicates current transmission failures or heart blocks. Crucially, a hallmark of heart blocks is the presence of more P waves than QRS complexes, indicating that atrial impulses are failing to conduct to the ventricles.