Step 1 Cardio
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
Sinus Venosus
Cornary sinus
Common Cardinal Veins
Superior Vena Cava
Truncus Arteriosus
What is the physiologic process?
Ascending aorta & pulm trunk
Process:
Neural crest cells from hindbrain migrate to form division of truncus arteriosus into aorta & pulmnary artery (aorticopulmonary septum) ⟶ Spiraling
Primitive Ventricle
Trabeculated portion of Ventricles
Bulbus cordis
Smooth portion of L & R ventricle
Endocardial Cushions
Valves & membranous portion of ventricular septum
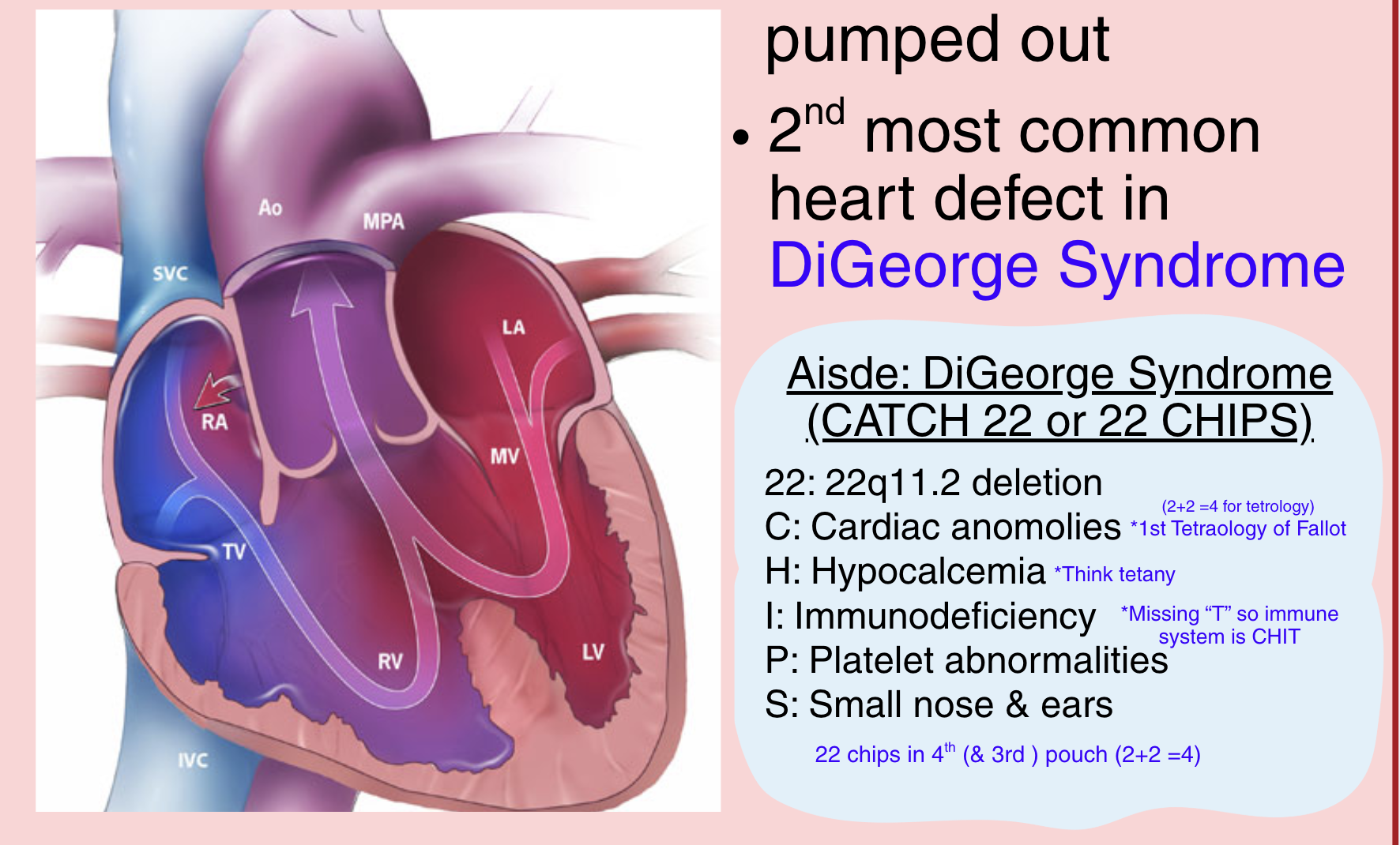
Persistent Truncus Arteriosus
What is it?
Association?
Aorticopulmonary septum incomplete ⟶ so oxygenated blood from LV & deoxygenated blood from RV mix
2nd most common heart defect in DiGeorge Syndrome (22 Chips)
22: 22q11.2 deletion
C: Cardiac anomalies (1st Tetralogy of Fallot. Think 2+ 2 = 4)
H: Hypocalcemia
I: Immunodeficiency
P: Platelet abnormalities
S: Small nose & ears
Transposition of Great Vessels
Failed spiraling of aorticopulmonary septum à reversal of pulmonary artery and aorta
Compatible with life only if Patent Ductus Arteriosus (PDA) present ⟶ So some oxygenated blood can mix in (machine like murmur)
Give prostagladin to keep PDA open!
Associated with gestational diabetes
*Think high blood sugar ⟶ cardiac risks ⟶ cardiac embryonic development affected
Atrial Septation Process
2 Potential Defects?
Step 1: Septum Primum Forms
• Forms inferiorly from superior primitive atrium
• Foramen primum: opening b/w septum primum + AV cushions
• Step 2: Foramen and Septum Secundum Form
• Foramen Secundum: Forms within septum primum
• Septum Secundum: Superior and inferior segment
• Step 3: Foramen Ovale Closes
• Foramen Ovale: Formed by area between septum primum and secundum
• ↓ pulmonary vascular resistance, ↑ LAP, ↓ RAP
Patent Foramen Ovale:
• Incomplete joining of septum primum and septum secundum
• Most patients are asymptomatic
• Cryptogenic cerebrovascular accident, paradoxical embolism
Atrial Septal Defect:
• Secundum-type is most common and tend to be isolated
• Primum-type generally associated with additional heart defects
• Cryptogenic cerebrovascular accident, paradoxical embolism
Wide fixed split S2 heart sound bc it takes longer for the pulmonic valve to close if there is more blood (coming from the Left Atrium) due to increased blood flow through the right side of the heart.
Atrial Septal Defect
How common are the 2 types? Are they associated with different things?
Association?
Heart Sound?
• Secundum-type is most common and tend to be isolated
• Primum-type generally associated with additional heart defects
• Cryptogenic cerebrovascular accident, paradoxical embolism
Wide fixed split S2 heart sound bc it takes longer for the pulmonic valve to close if there is more blood (coming from the Left Atrium) due to increased blood flow through the right side of the heart.
Ventricular Septal Defects
Ventricular Septal Defects most commonly occur due to defects in the membranous portion of the interventricular septum aka endocardial cushions
What comes from 1st Aortic Arch?
Maxillary Artery
What comes from fourth aortic arch? (L & R)
Left Fourth Arch: Aortic Arch
• Classic Pathology: Coarctation of the aorta
Right Fourth Arch: Proximal Right Subclavian Artery
What comes from sixth aortic arch? (L & R)
Left Sixth Arch: Ductus Arteriosus and Proximal Pulmonary Arteries
• Classic Pathology: Patent ductus arteriosus
Right Sixth Arch: Proximal Pulmonary Arteries
Aortic Coarctation
Potential Locations
Origina/Derivative
Associations
Presentations (w/ & w/o PDA)
Imaging
Management
Locations: (1) juxtaductal narrowing (aortic isthmus) (2) Pre-ductal: infantile fform & most common (3) Post-ductal: Adult form
Origin: Derived from Left 4th arch
Associations:
(1) Turner Syndrome
(2) Williams Syndrome: Elfin face, hypersocialability, Hypercalcemia & supra valvular aortic stenosis *Think: William the social elf gave out too much CAndy & that's bad for the heart
(3) Berry aneurysm --> increased risk of rupture --> SAH
Presentation:
w/o PDA:
Harsh systolic murmur at multiple locations along left sternal border
Differential cyanosis: Arms are good, but legs are not perfused
Brachial-femoral delay: Brachial pulse strong, femoral weak
w/ PDA: Generally asymptomatic
#3 is PDA which allows for perfusion to lower body
Locations: (1) juxtaductal narrowing (aortic isthmus) (2) Pre-ductal: infantile fform & most common (3) Post-ductal: Adult form
Origin: Derived from Left 4th arch
Associations:
(1) Turner Syndrome
(2) Williams Syndrome: Elfin face, hypersocialability, Hypercalcemia & supra valvular aortic stenosis *Think: William the social elf gave out too much CAndy & that's bad for the heart
(3) Berry aneurysm --> increased risk of rupture --> SAH
Presentation:
w/o PDA:
Harsh systolic murmur at multiple locations along left sternal border
Differential cyanosis: Arms are good, but legs are not perfused
Brachial-femoral delay: Brachial pulse strong, femoral weak
w/ PDA: Generally asymptomatic
#3 is PDA which allows for perfusion to lower body
Imaging:
Rib notching on CXR (silation of vessel w/ blood looks like notch on rib)
Management:
Neonates --> prostagladin E1 (to keep PDA open)
Operative repair
Patent Ductus Arteriosus
If in a premature newborn and we want to close it, give prostaglandin inhibitors like indomethacin
Origin/derivative: Left 6th Arch (which is in charge of ductus arteriosus & proximal pulmonary arteries
Murmur: Continuous machine-like murmur @ L infra clavicular. Palpable thrill.
Radiofrequency Ablation Locations
A Fib?
A Flutter?
Afib —> in LA myocardium (near pulm vein ostium)
A Flutter —> In space between inferior vena cava and tricuspid valve
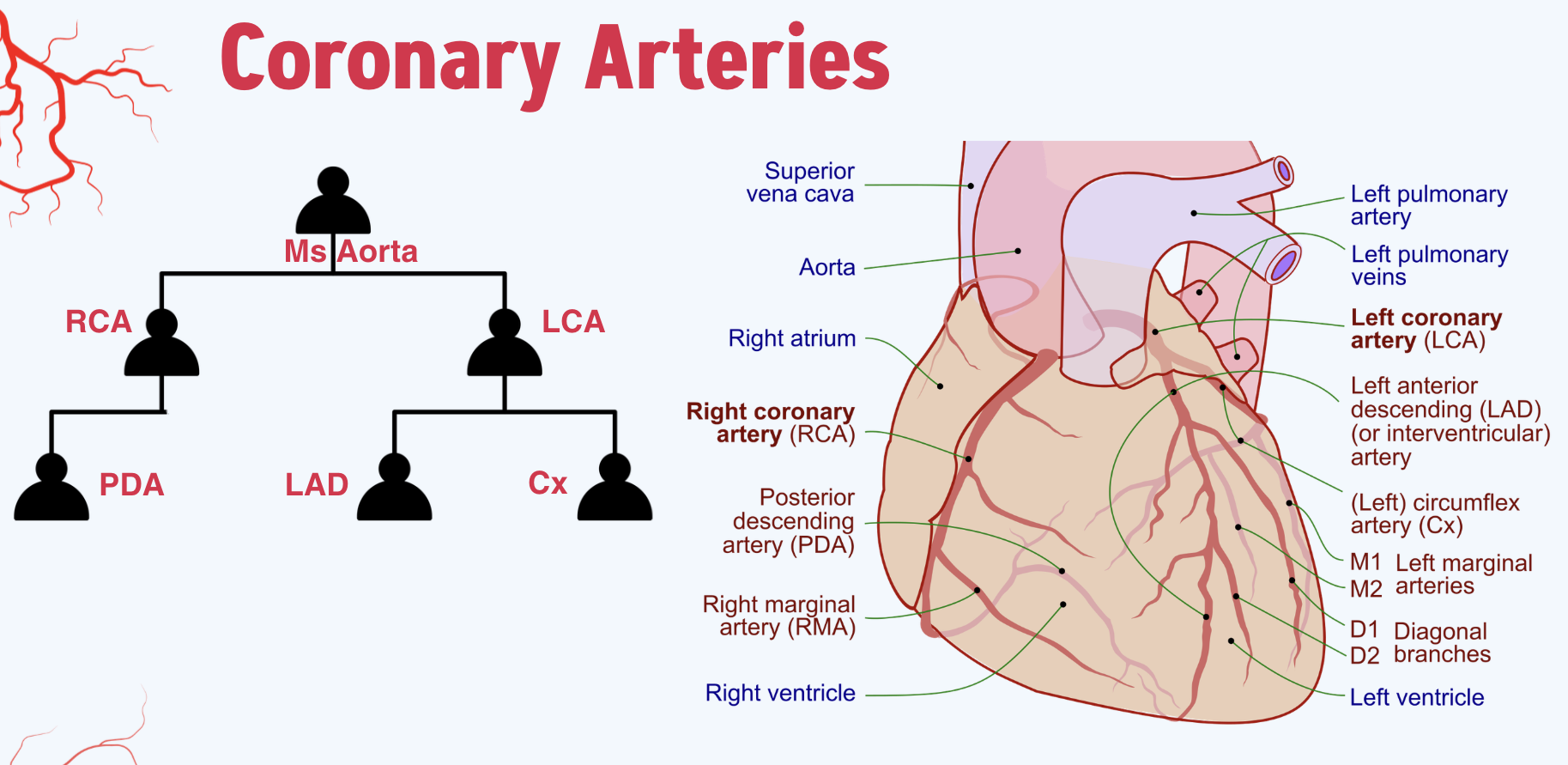
Coronary Artery Anatomy
Right Coronary Artery (RCA):
• Majority of right-side of heart
• Sinoatrial node
• Left Coronary Artery (LCA):
• Majority of left-side of heart
• Two major branches:
• Left Anterior Descending Artery (LAD)à Anterior 2/3
of interventricular septum, anterolateral papillary
muscle, anterior left ventricle
• Left Circumflex Artery (LCX) à Posterolateral LA and
LV, anterolateral papillary muscle
• Posterior Descending Artery (PDA):
• ~85% R-dominant, 8% L-dominant, 7% co-dominant
• Primarily inferior borders of heart
• Posterior 1/3 of interventricular septum
• Posteromedial papillary muscle
Ms Aorta had RCA & LCA
LCA had a LAD & a kid who liked to flex (L circumFLEx)
LAD: (also called IVY - interventricular artery): Anterior left ventricle, anterior 2/3s interventricular septum & anterolateral papillary muscles aka muscle of the LV/mitral valve
LCA: left atrium, posterior LV, anterolateral papillary muscles aka muscle of the LV/mitral valve
RCA focused on doing things “right” (aka entire right side of heart) and had PDA which showed too much PDA so that diva was relegated to back of the heart (inferior borders, inferior 1/3 of ventricular septum)
Coronary Sinus
All coronary veins drain into the coronary sinus
• Location: Left posterior atrioventricular groove
• Drains directly into the right atrium
• Embryologic derivative: Sinus venosus
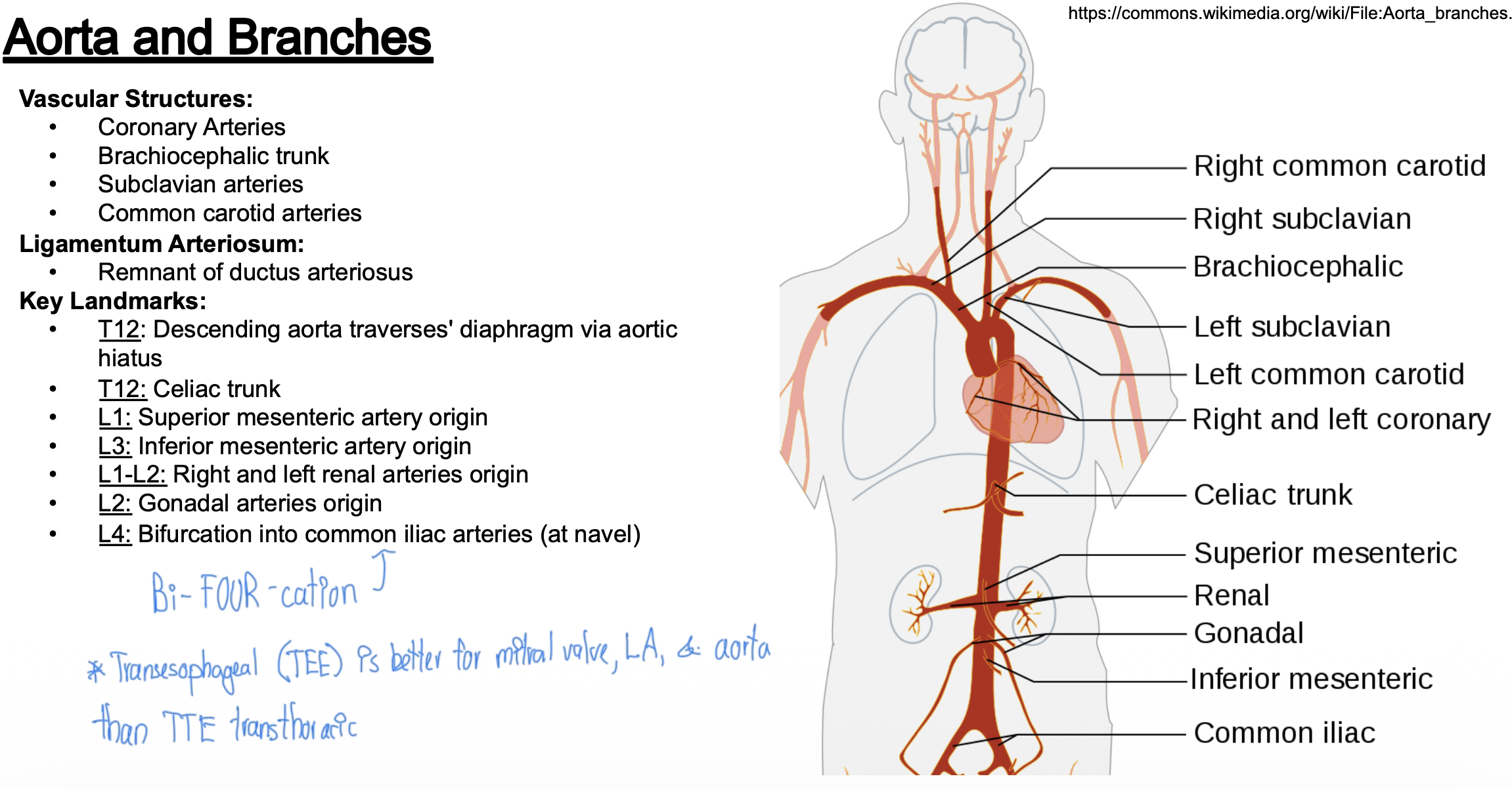
Aorta
What are her branches?
Important landmarks?
Descending aorta traverses' diaphragm via aortic hiatus
Celiac trunk
Superior mesenteric artery origin
Inferior mesenteric artery origin
Right and left renal arteries origin
Gonadal arteries origin
Bifurcation into common iliac arteries (at navel)
Vascular Structures:
• Coronary Arteries
• Brachiocephalic trunk
• Subclavian arteries
• Common carotid arteries
• Ligamentum Arteriosum:
• Remnant of ductus arteriosus
Key Landmarks:
T12: Descending aorta traverses' diaphragm via aortic hiatus (vs IVC at T8)
T12: Celiac trunk
L1: Superior mesenteric artery origin
L3: Inferior mesenteric artery origin
L1-L2: Right and left renal arteries origin
L2: Gonadal arteries origin
L4: Bifurcation (bi-FOUR-cation) into common iliac arteries (at navel) (vs IVC where it is L5)
List vessels in order of most to least likely to have atherosclerosis
Circle of Willis
Carotid Arteries
Coronary Arteries (which one is most likely)
Popliteal
Abdominal Aorta
Abdominal aorta
Coronary arteries (LAD)
Popliteal Arteries
Carotid Arteries
Circle of Willis
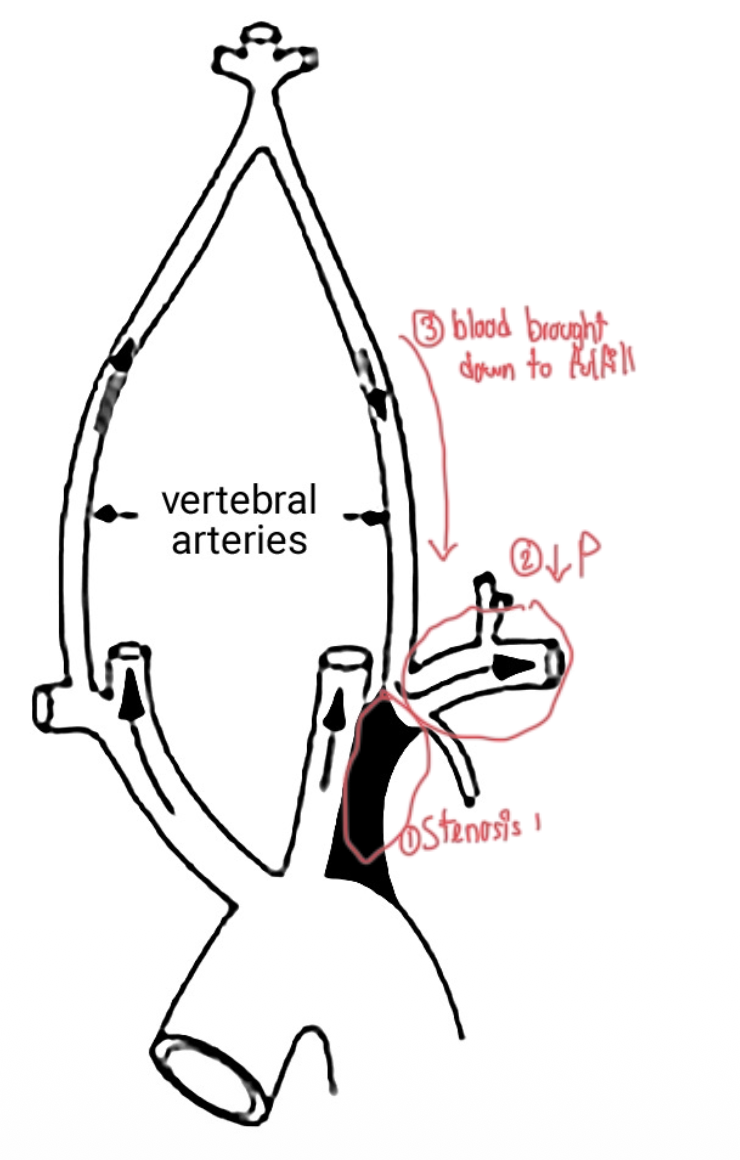
Subclavian Steal Syndrome
Etiology: Atherosclerosis, Takayasu arteritis, previous thoracic (aortic) surgery
• Pathophysiology:
• Subclavian stenosis à contralateral vertebral artery steal phenomena
• Presentation:
• Ipsilateral limb ischemia
• Asymmetric BP between upper extremities
• Dizziness, diplopia, syncope
• Worsening of symptoms during activity of affected limb
• Imaging:
• Reduced contrast uptake in areas distal to stenosis and ipsilateral vertebral artery
Obstructive Venous Drainage
Presentation for each in terms of face and extremity swelling, etc. other sx
Superior Vena Cava Syndrome
Brachiocephalic
Subclavian
Inferior Vena Cava
Superior Vena Cava Syndrome
• Etiology: Mass lesion (malignancy) or thrombosis (venous catheter)
• Edema à bilateral face, bilateral upper extremities
• Jugular venous distention
• Headache, ↑ intracranial pressure
• Brachiocephalic Venous Obstruction
• Etiology: Pancoast tumor or thrombosis (venous catheter)
• Edema à Unilateral face, unilateral upper extremity
• Subclavian and/or Axillary Venous Obstruction
• Edema à Unilateral upper extremity
• No facial involvement
• Inferior Vena Cava Compression
• Supine hypotensive syndrome (3rd trimester)
Edema à Bilateral lower extremities
Fetal hypoxia à improves with repositioning
How do you get femoral access?
NAVEL
Which are encased in femoral sheath?
Nerve, Artery, Vein, Empty Space, Lymphatics
Feel for pulsation, then go medial
all but nerve are encased in femoral sheath
When does coronary perfusion occur?
Where in the heart is the most susceptible to ischemic injury?
Coronary perfusion occurs during diastole, primarily when the heart muscle is relaxed. The subendocardium is the most susceptible to ischemic injury due to its position and high demand for oxygen.
Hydralyzine
Arterial vasodilation
Phenylephrine
Arterial vasoconstriction (a2 agonist)
Sodium Nitroprusside
50/50 venous & arterial dilation
Epinephrine, digoxin & dobutamine
All increase contractility
Frank-Starling Mechanism
Principle:
• ↑ Preload à ↑ Contractility à ↑ SV
• Mechanism:
• ↑ Venous return
• ↑ EDV ~ ↑ Preload
• ↑ Myocyte stretch prior to contraction
• ↑ Sarcomere length (↑ active tension and velocity of fiber shortening)
• Frank-Starling Curve:
• X-axis: LVEDP (preload, LVEDV, fiber length)
• Y -axis: Stroke Volume
• Slope of curve: Defined by afterload and contractility
• Point along curve: Defined by venous return (preload)
Two equations for Cardiac Output
MOST IMPORTANT
CO = HR x SV
Fick Principle
CO = VO2 / (CaO2 - CvO2)
Mean Arterial Pressure
Average pressure in a complete cardiac cycle
Pulse Pressure
PP = Systolic Pressure - Diastolic Pressure
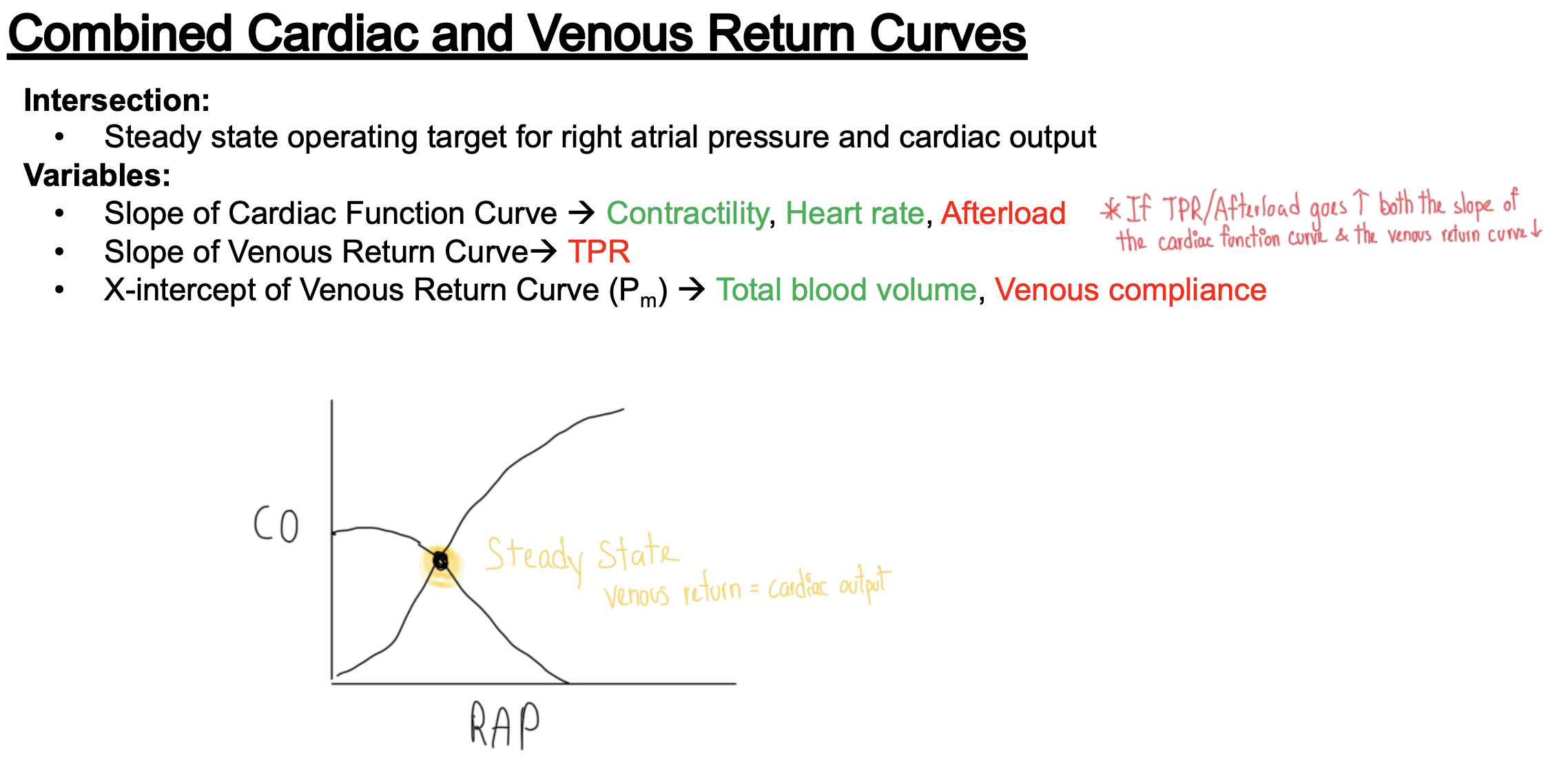
Cardiac Curve w/ Venous Return Curve
Describe x & y axis
What does the x intercept represent? What changes it?
What changes the slopes?
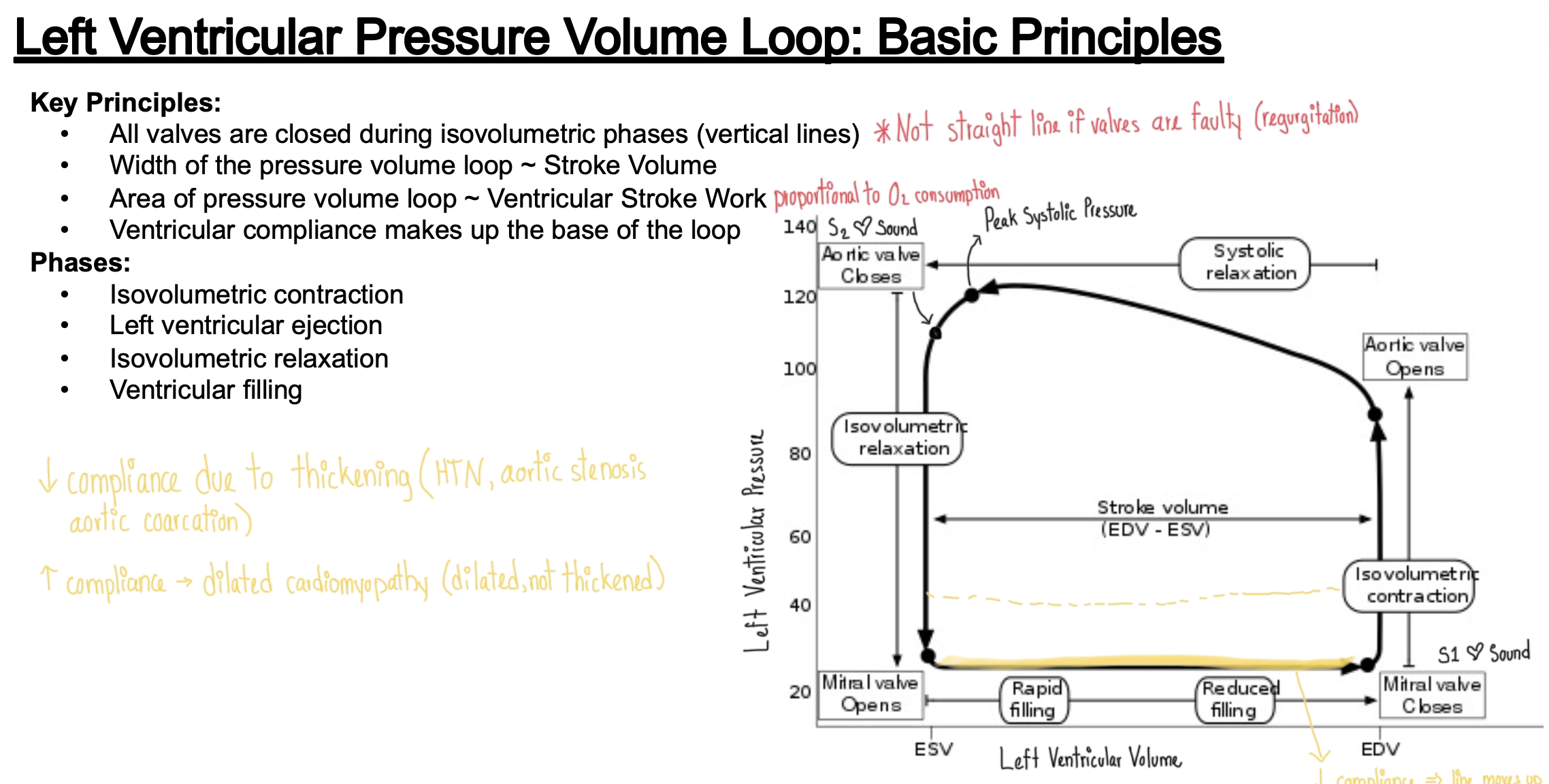
Pressure Volume Loop
What does each corner & line mean?
What factors change them?
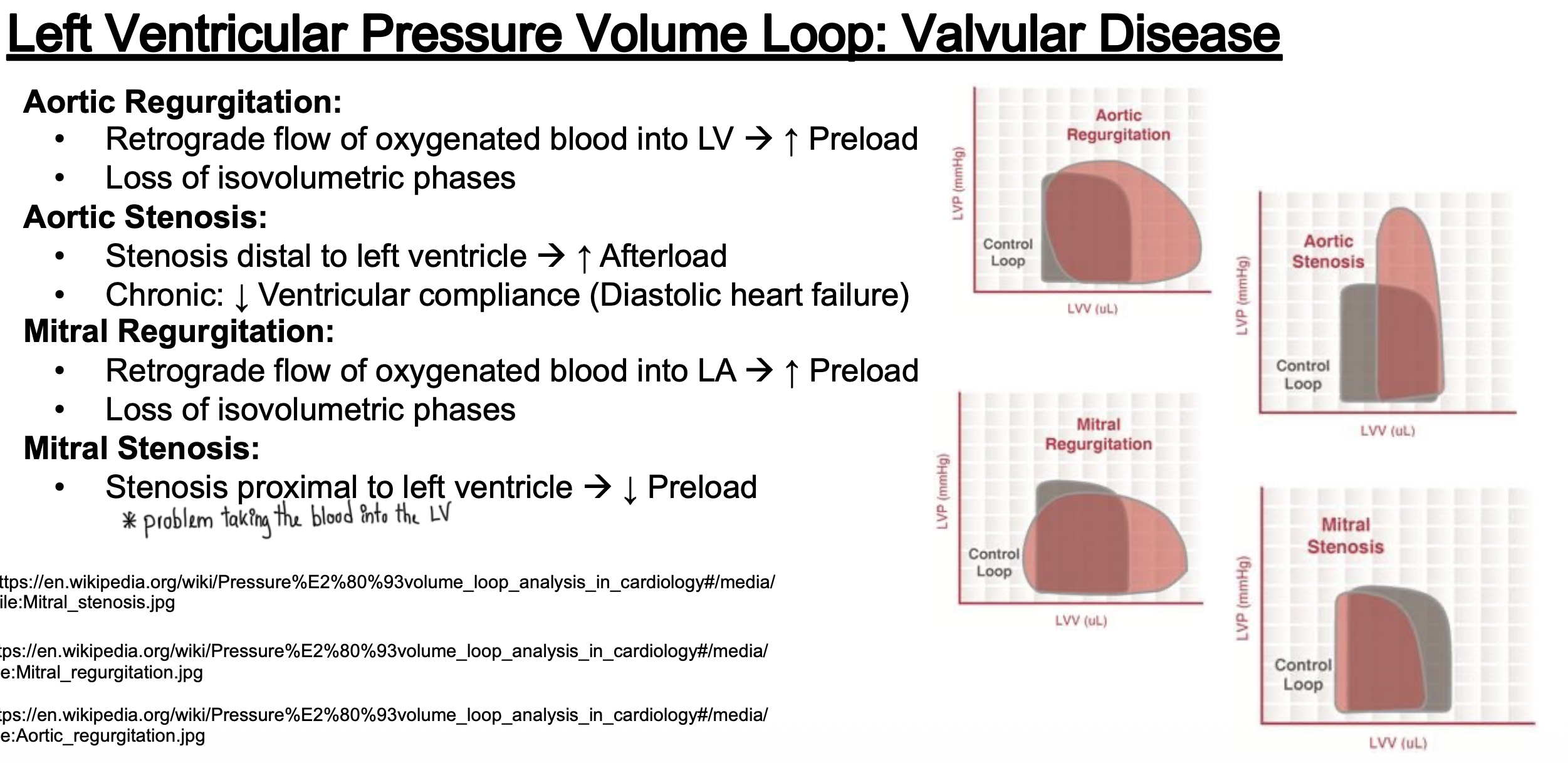
Pressure Volume Curve for Valvular Disease
What does each one look like?
Aortic Regurgitation
Aortic Stenosis
Mitral Regurgitation
Mitral Stenosis
List Endothelial Regulated Dilation Pathway
In the endothelium (which is lined by smooth muscle)
(1) Sheer stress (from blood passing through) or Acetylcholine or Bradykinin —> makes NO from arginine
(2) NO is released & diffuses to smooth muscles
(3) NO leads to conversion of GTP to cGMP
(4) cGMP activates PKG —> decreases cytosolic Ca2+ —> smooth muscle relaxation
Excitation-Coupling constriction Mechanisms for:
Cardiac Myocytes
Smooth Muscle
Skeletal Muscle
Cardiac Myocytes
SA node —> Ca2+ come in through L type Calcium channel
Action potential leads to Ca2+ influx. 2. Ca2+ triggers further Ca2+ release from the sarcoplasmic reticulum. 3. Ca2+ binds to troponin, exposing binding sites on actin. 4. Myosin heads attach to actin, causing contraction.
Smooth Muscle
Same thing as cardiac except we also have the GqPCR pathway —> cleaves PIP2 into IP3 and DAG —> IP2 goes to SR —> releases calcium
intracellular calcium levels, where Ca2+ binds to calmodulin, activating myosin light chain kinase (MLCK) that phosphorylates myosin heads. This promotes myosin-actin interaction, leading to contraction.
To relax: Intracellular Ca2+ levels must decrease, MLCK is inactivated, and myosin light chain phosphatase (MLCP) dephosphorylates myosin.
Skeletal Muscle
Same thing as cardiac myocytes except pathway stimulated by Acetylcholine (no automaticity from SA node)
Mechanical coupling of LType Calcium Channel with RyR (which is why Ca2+ channel blockers do not have a major effect on skeletal muscle)
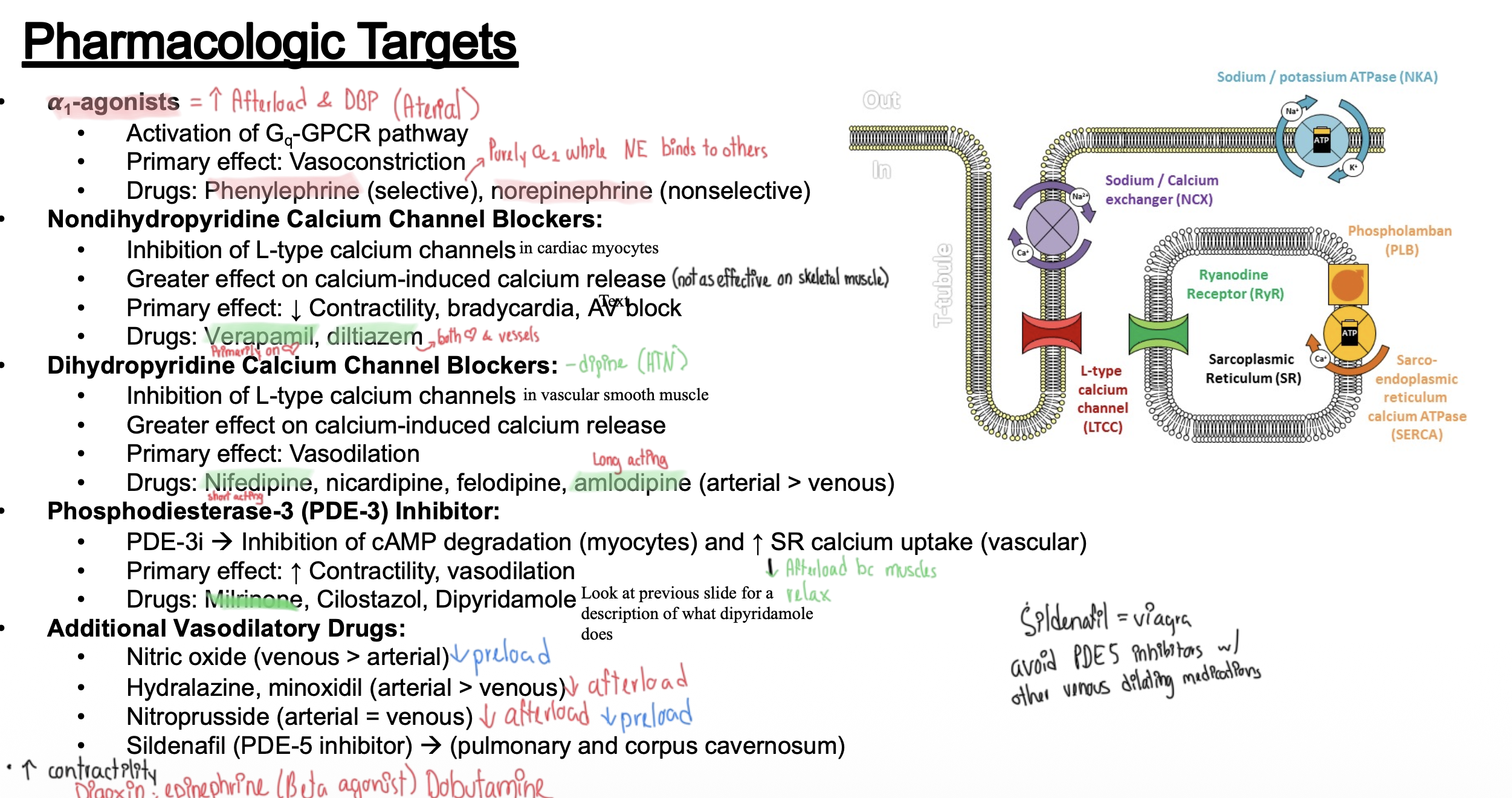
Nifedipine & Amlodipine
Class:
Mechanism:
Primary site of effect:
Class: Dihydropyrindine Ca Channel Blockers
Mechanism: Inhibits L type calcium channel —> vasodilation
Primary site of effect: Mostly vascular smooth muscle cells (arteries)
Diltiazem & Verapamil
Class: Non- Dihydropyrindine Ca Channel Blockers
Mechanism: Inhibits L type calcium channel —> vasodilation
Primary site of effect: Primarily cardiac myocytes, some vascular smooth muscle cells (arteries)
Vasoconsctriction & Vasodilation Targets Meds (Video 4)
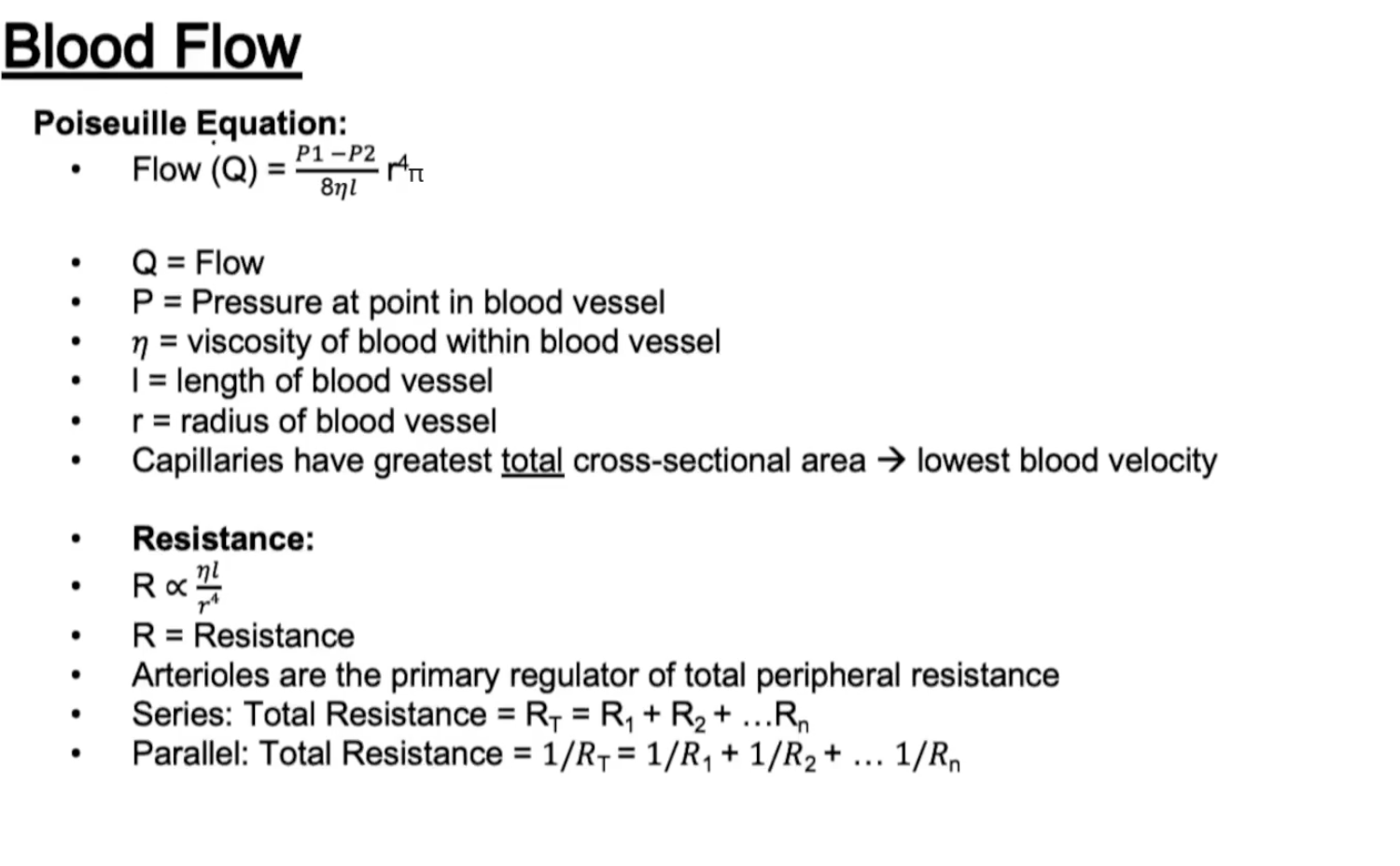
Blood Flow
Poiseuille Equation
Resistance