Looks like no one added any tags here yet for you.
Typical Angina Pectoris
Classic angina presents with substernal chest pain that’s described as “squeezing” or “pressure-like.” **Levine’s sign**
Can radiate to the arms or jaw and is made worse by exertion or emotion and made better by rest or nitroglycerin
When should an EKG be taken in the ER?
<10mins from telling triage nurse chest pain/SOB
What is the first cardiac biomaker that raises with an MI?
Myoglobin
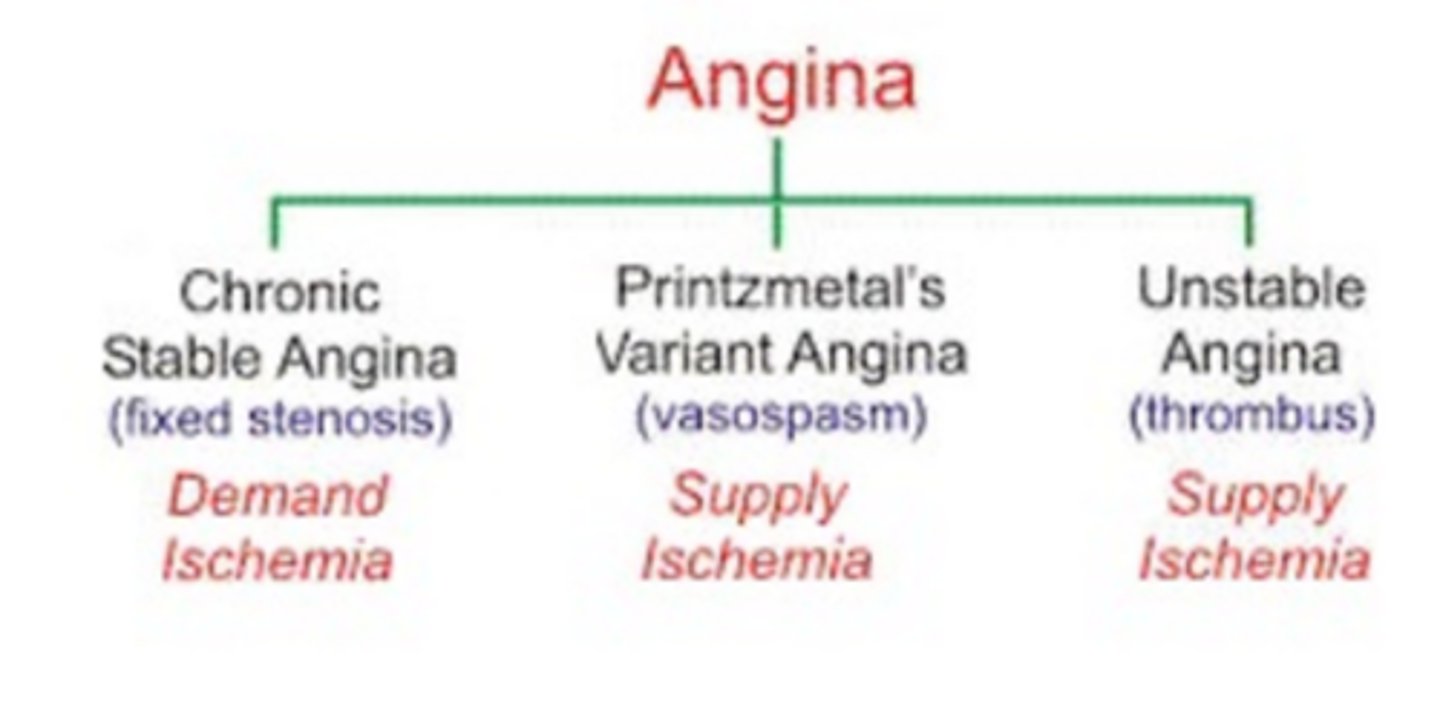
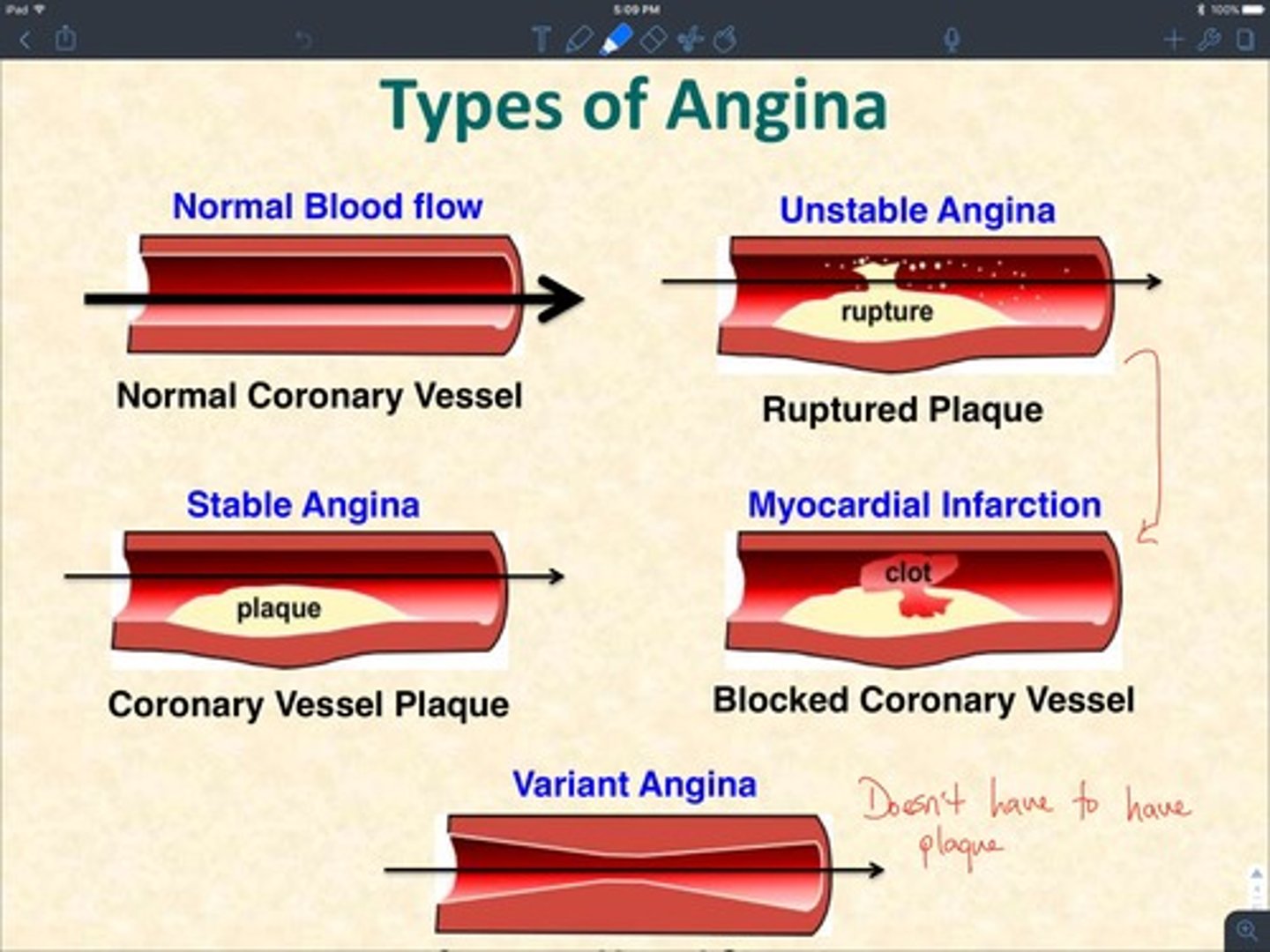
Stable Angina
Pain in chest w/ exertion, relieved with rest
Unstable Angina
Symptoms of ACS: chest pain, exertional pain and pain at rest: supply ischemia
Tx:
- Anti-platelet therapy:
- Anti-coagulation
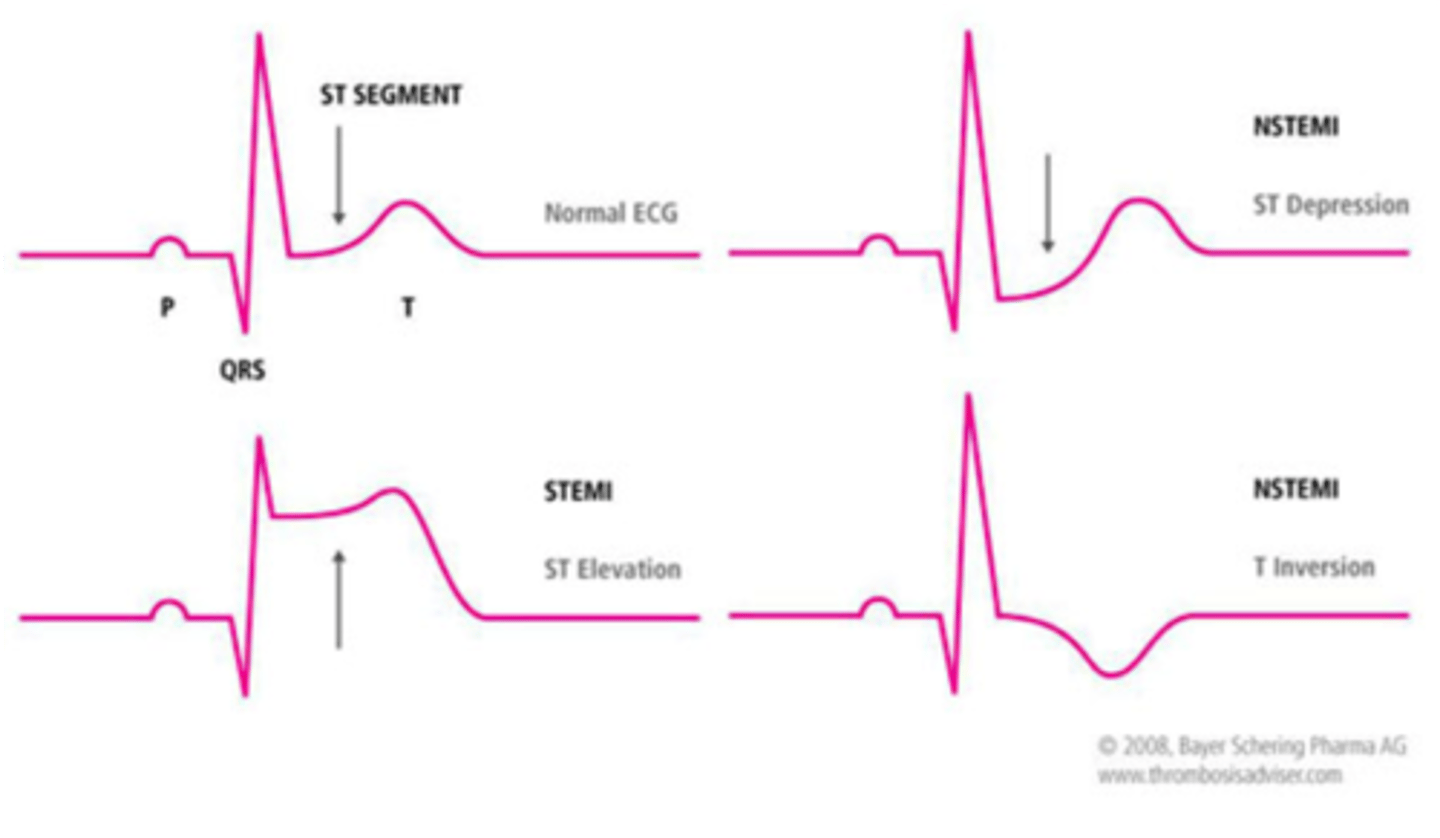
STEMI
ST elevation MI, real-time ongoing death of heart tissue due to ischemia
- (+) Cardiac biomarkers (don't wait for labs)
Tx:
- Select reprofusion strategy (Primary PCI strongly preferred)
- Anti-platelet therapy
- Anti-coagulation
STEMI Criteria
ST elevation in 2 contiguous leads is required to diagnose STEMI
> 2mm in precordial leads= STE
> 1mm in limb leads= STE
The presence of reciprocal ST depression helps confirm the diagnosis
STEMI - Cath Lab (TIMING)
Door to EKG time is 10 minutes
Door to Balloon time in PCI capable: <90 minutes
ACS Risk stratification
HEART Score: (perferred)
- Risk stratifies based on History, EKG, Age, Risk Factors, Troponin [Score], to identify low risk patients
EDACS:
- Emergency Department Assessment of Chest Pain Score safely identifies a higher proportion of patients as low-risk for MACE than other ACS clinical decision scores. No EKG or labs used for EDACS
Aortic Dissection
Tearing Pain radiating to back: think dissection
Tx of Stable Patient:
- Propranolol (to decrease heart contractility)
- Diltiazem (to relax aortic smooth muscle)
- Enalapril (to lower blood pressure)
Tx of Unstable Patient:
- Fluids and Pressors
- Surgery
Pulmonary Embolism
1. Sinus Tachycardia
2. RV strain = T wave inversions in V1-V4 & II,III, aVF
3. Cor Pulmonale (RV failure) = S1Q3T3
CXR: (Board question, not realistic, Olsmmer will beat us w/ wet noodle)
- Hampton's Hump
- Westermark sign
Assess with Wells PE Score:
- Low Probability = Use PERC score to r/o PE
- Moderate Probability = Use D-dimer to r/o PE
- High Probability = Use CT scan to r/o PE
Tx - Stable Patient:
- Rivaroxaban (Xarelto) 20 mg PO qd **PREFERRED**
Tx - Unstable Patient:
- Thrombolysis aka TPA (Alteplase 100mg over 2hrs)
- Thrombectomy if contraindications to thrombolysis
What is a the gold standard for diagnosing a pulmonary embolism?
CTA PE protocol
What is a PESI score?
Pulmonary Embolism Severity Index
**Helps determine PE severity for treatment options
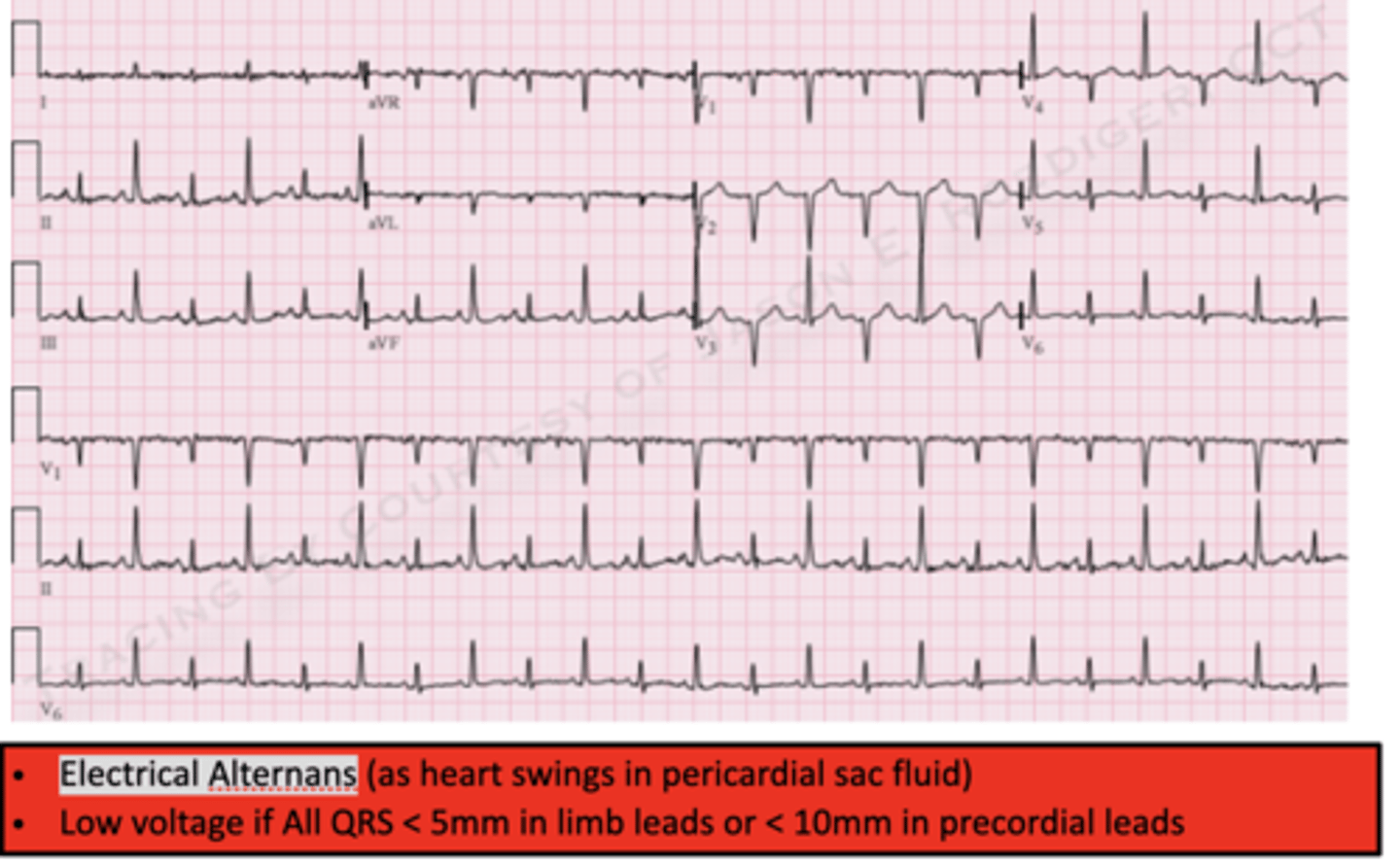
Electrical alternans is a possible finding on EKG in what condition?
Cardiac Tamponade
**Also Beck's triad & "water bottle" appearance on CXR
Diffuse ST elevations is a possible finding on EKG in what condition?
Pericarditis
**Does not meet STEMI criteria
How do you treat pericarditis?
NSAIDs or Colchicine are 1st Line
**Steroids for resistant sx
How to treat sinus tachycardia?
Treat underlying condition
- PO fluids, IVFs, antipyretics, anxiolytics
How to treat supraventricular tachycardia (SVT)?
Stable:
- Vagal maneuvers
- Chemical Cardioversion: adenosine (may repeat)
- Amio, cardiology consult
Unstable:
- Synchronized Cardioversion
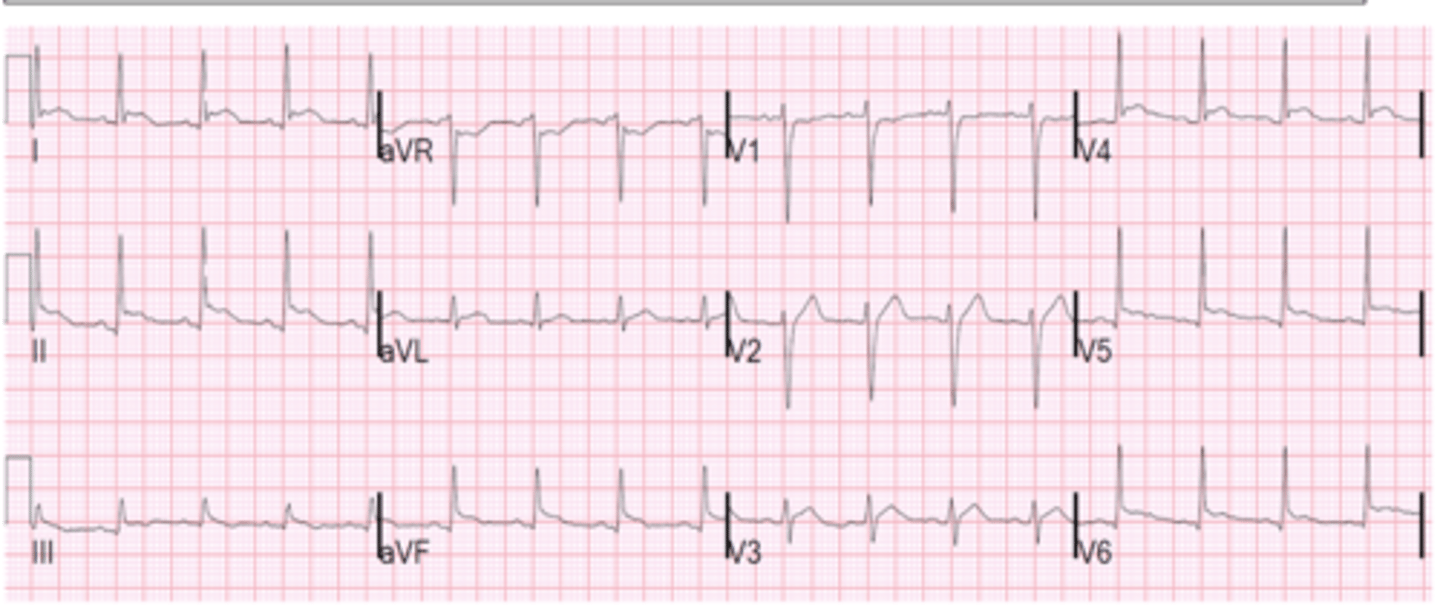
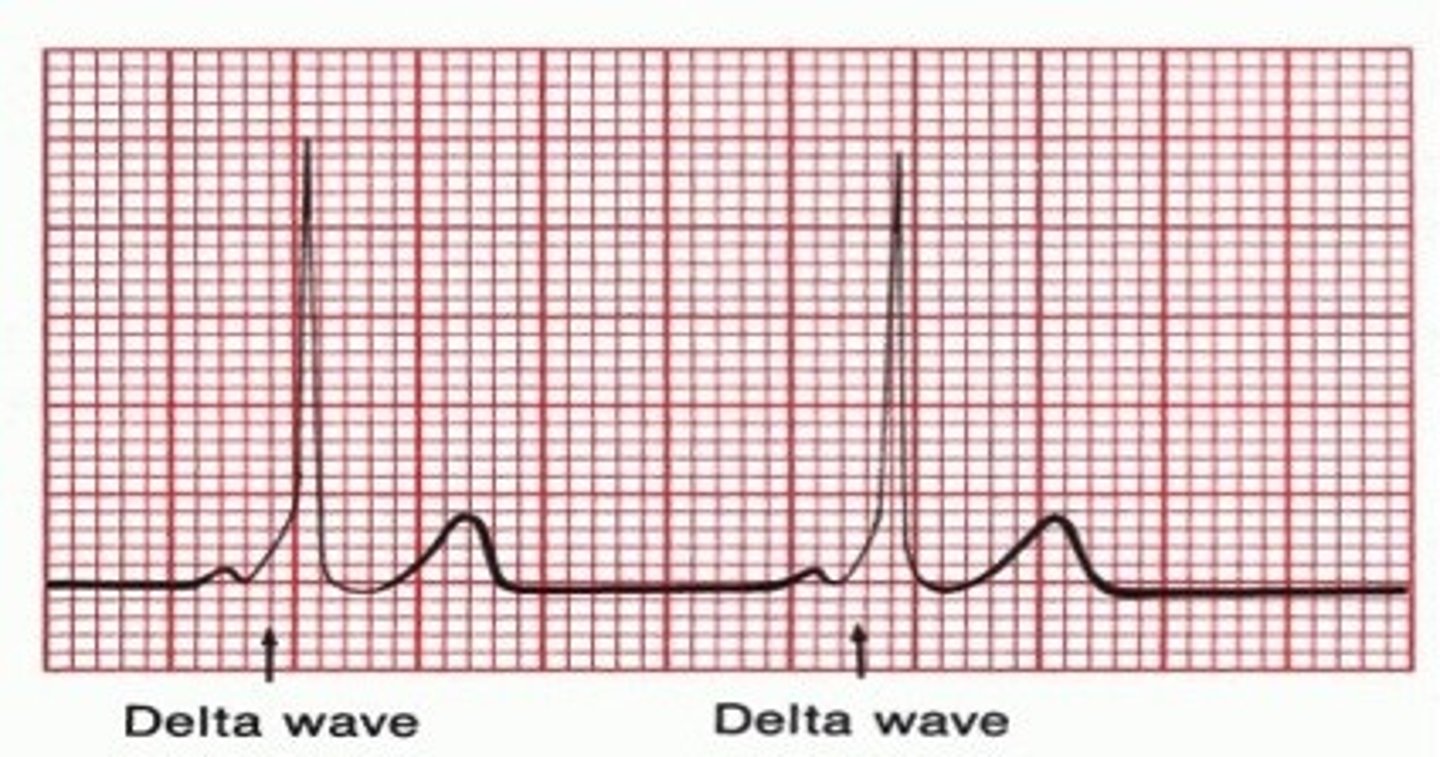
How to treat Wolff-Parkinson-White Syndrome?
Unstable: Cardioversion
Chronic: Ablation
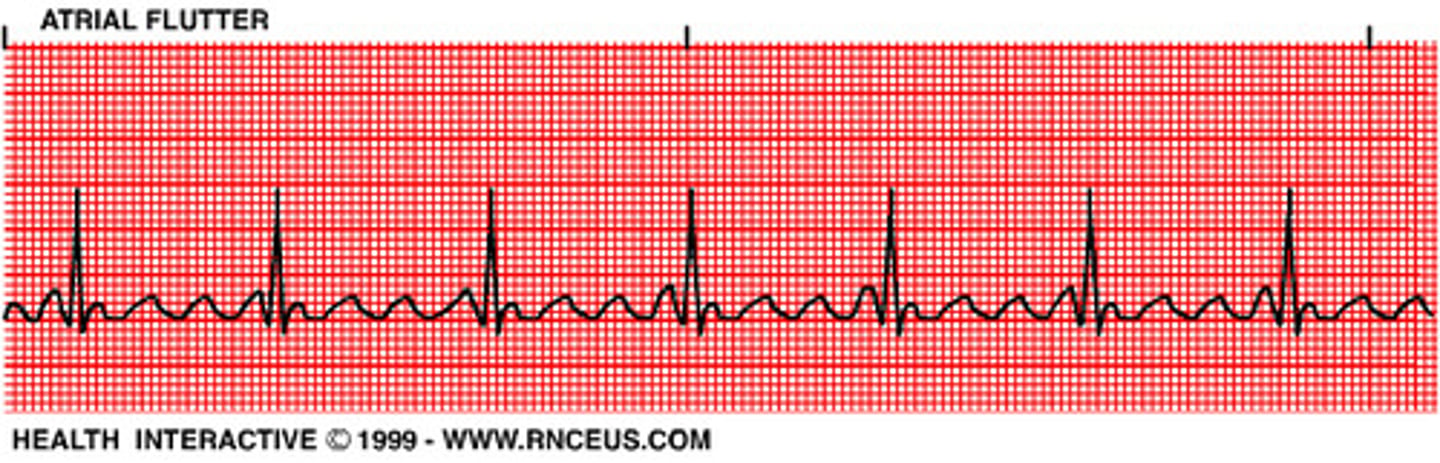
How to treat A-flutter?
Stable: BB
Unstable: Cardiovert
How to treat A-fib?
Depends, but make sure to anti-coag for stroke prevention (DOAC preferred)
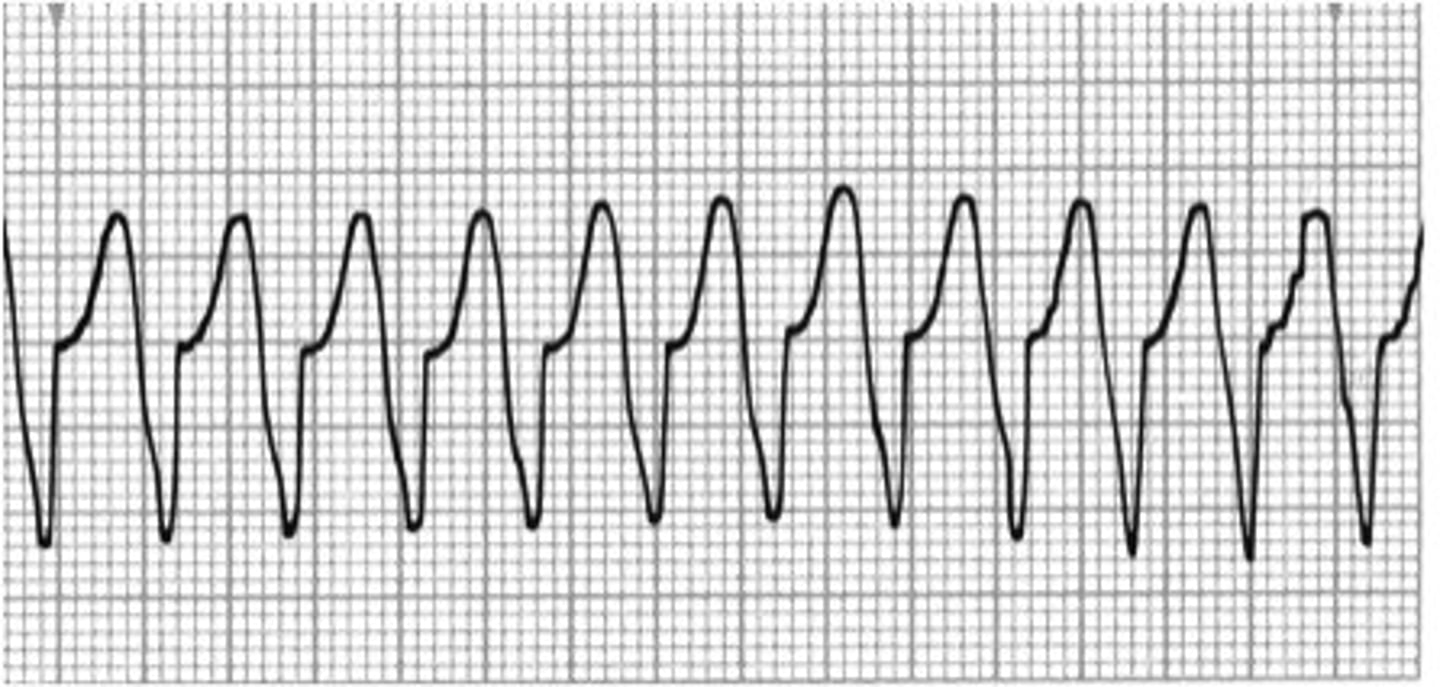
How to treat ventricular tachycardia?
Pulse: Synchronized cardioversion
Pulseless: Chest compression + defibrillate
**+/- pulse
How to treat Torsades de Pointes?
Magnesium IV
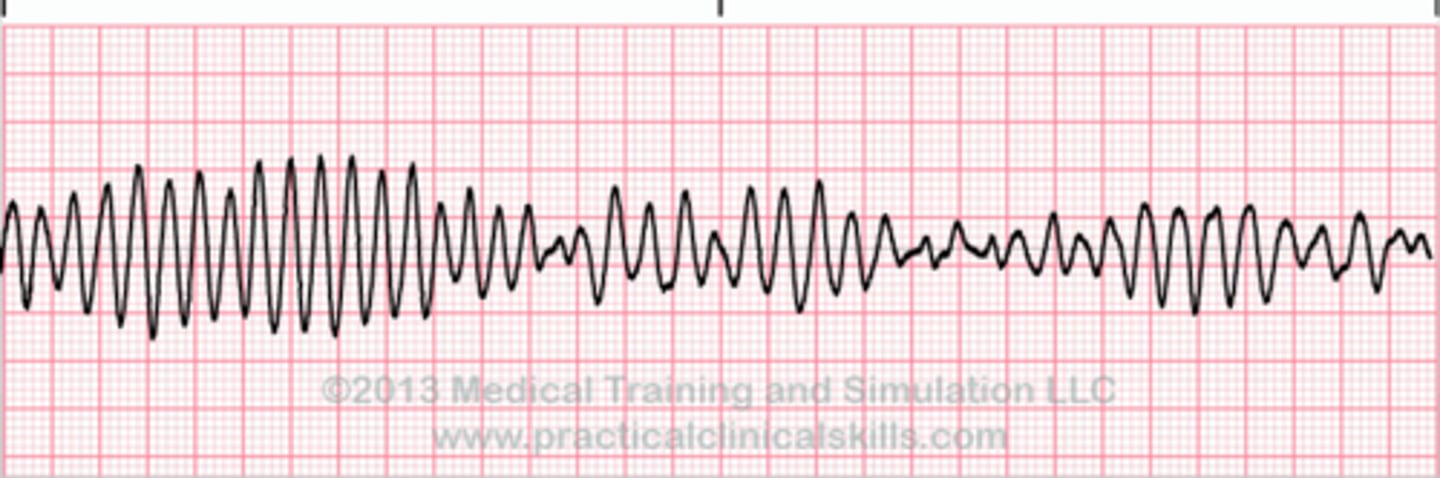
How to treat Ventricular Fibrillation?
Chest compression + Defibrillate
How to treat pulseless electrical activity (PEA)?
Chest compression
**DO NOT SHOCK!!
How to treat Asystole?
Chest compression
**DO NOT SHOCK!!
How to treat a 3rd degree heart/complete heart block?
Pacemaker
**Transcutaneous pacing until they can get pacemaker