UMP
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
BRONCHOSCOPY EXPLANATION
Explain what the procedure is
Explain the reason for the procedure
Before
Oral intake
6 hours before – clear fluids (sips) only
2 hours before – NBM
Also if high-risk (e.g. transbronchial biopsy) depending on risk/benefit
- Stop clopidogrel 1 week before (unless high risk, e.g. drug-eluting stent)
- Stop warfarin 5 days before (± give LMWH)
- Stop DOAC 48 hours before
During
- Midazolam sedative (→amnesia)
- Lidocaine spray/gel to the nose, throat and windpipe
After
- No eating/drinking 2 hours after as throat still numb
- No driving, alcohol, operating machinery, or signing legal documents for 24 hours
- Keep someone with you for 24 hours
- Arrange follow-up
Risks
Lung damage/collapse
Infection
Bleeding (haemoptysis)
Sore nose/throat
Sedation side effects
Pneumothorax
OGD EXPLANATION
Explain what the procedure is
Explain the reason for the procedure
Before
Oral intake
6 hours before – sips of water only (sips)
2 hours before – completely NBM
Also
Stop acid suppressive medications 2 weeks before e.g PPI
During
Option of non-sedated or sedated
Lidocaine throat spray or midazolam sedative (→amnesia)
Continuous suction
Air passed through scope (→fullness, belching)
After
Arrange follow-up
If had throat spray: No eating/drinking 2 hours after as throat still numb
If had sedation: No driving, alcohol, operating machinery or signing legal documents for 24 hours
Keep someone with you for 24 hours
Risks
Perforation (<0.1%)
Bleeding
Infection (aspiration pneumonia)
Sore throat
Dental damage
Sedation side effects
COLONOSCOPY EXPLANATION
Explain what the procedure is
Explain the reason for the procedure
Before
Oral intake
2 days before – low fibre diet
1 day before – clear fluids only after light breakfast
2 hours before – NBM
Also
Sodium picosulfate sachet afternoon before and morning of the procedure (bowel prep_
Stop iron tablets 1 week before, and constipating agents 4 days before (e.g. codeine)
During
- Midazolam sedative (→amnesia)
- Digital rectal examination prior to scope insertion
- Air passed through scope (→bloating, you may feel like you need to go to the toilet)
After
No driving, alcohol, operating machinery, or signing legal documents for 24 hours
Keep someone with you for 24 hours
Arrange follow-up
Risks
Perforation (0.1%)
Bleeding
Infection
Abdominal discomfort
Sedation side effect
FLEXIBLE SIGMOIDOSCOPY explanation
Explain what the procedure is
Explain the reason for the procedure
Before
Oral intake
2 hours before – NBM
Also
Phosphate enema 2 hours before (can be self-administered at home)
During
Digital rectal examination prior to scope insertion
No sedation required
After
Arrange follow-up
Risks
Perforation
Bleeding
Infection
Abdominal discomfort
ERCP counselling
explain:
Camera test through mouth to check/treat bile & pancreas ducts (e.g. stones, blockages).
Before
* NBM 6 hrs.
* IV line for sedation ± antibiotics.
* Bloods, stop blood thinners if needed.
* Consent after risks/benefits explained.
During
* Sedation (relaxed but awake).
* Camera through mouth to small bowel.
* Dye + X-rays to see ducts.
* May remove stones, place stent, take sample.
* ~30–60 mins.
---
After
* Monitored in recovery.
* No food/drink until swallowing safe.
* Mild sore throat/bloating common.
* Report pain, fever, vomiting.
* Follow-up appointment
---
benefits
* Diagnose + treat in one test.
* Avoids surgery.
risks
* **Common**: infection, bleeding.
* **Rare**: Perforation, aspiration, death (<0.5%).
---
alternatives
* MRCP (scan only).
* Surgery** if ERCP not possible.
---
doing nothing
* Ongoing blockage → worsening of symptoms
RRT counselling
1. haemodialysis
- 4 hours 3 times a week come into hospital (significant impact on quality of life)
- fistula (unsightly)
side effects: itchy skin, fatigue, swelling
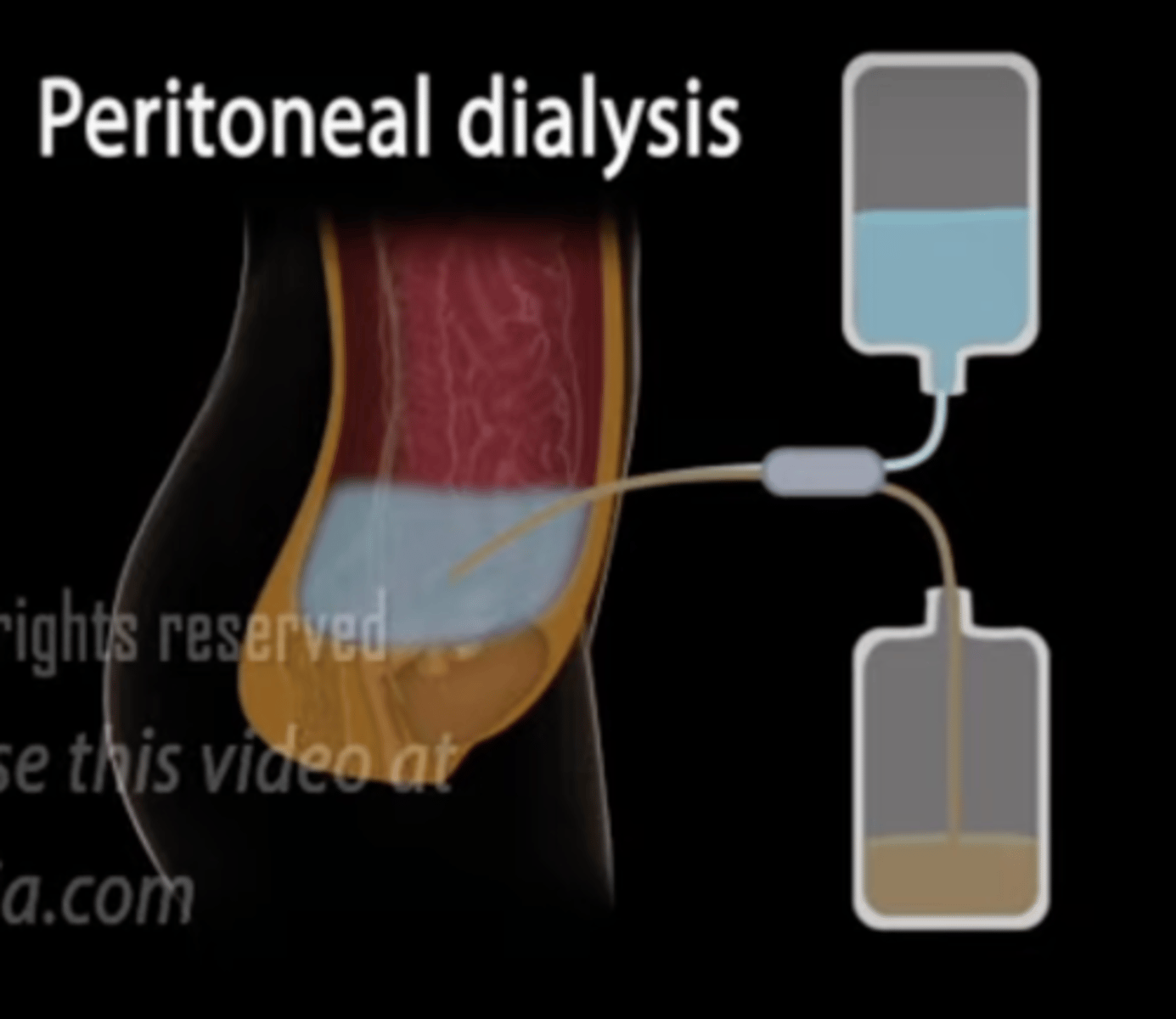
2. peritoneal dialysis
how it works: give fluid into tummy. There is a lining around your organs called the peritoneum. Blood gets filtered through the lining of the peritoneum and into the fluid. The waste fluid is then drained. The cycle is repeated.
- infection (peritonitis)
- need to do it your self
- weight gain
- blood sugar variation
3. renal replacement therapy
- risk of rejection
- need to find a donor, average wait is 3y
- average lifespan of a kidney is 10-15 years
general prescribing tips
- write mg out in full i.e micrograms
- with fluids - write out 0.9% sodium chloride instead of 0.9% NaCl or 0.9% saline
- if cancelling a medication, do a squiggly line and sign and date
Things to consider in prescribing patients with renal impairment
1. if there is reduced renal excretion, drugs stay in the body for longer -> need to decrease dose
2. whether the drugs cause further renal impairment
3. drugs which rely on the normal processes of the kidney to get them to their site of action become less effective
Things to consider in prescribing patients with hepatic impairment
1. whether the drugs cause further hepatic impairment
2. drugs which rely on being metabolised by the liver to active/inactive/toxic metabolites may not be metabolised as much with hepatic impairment
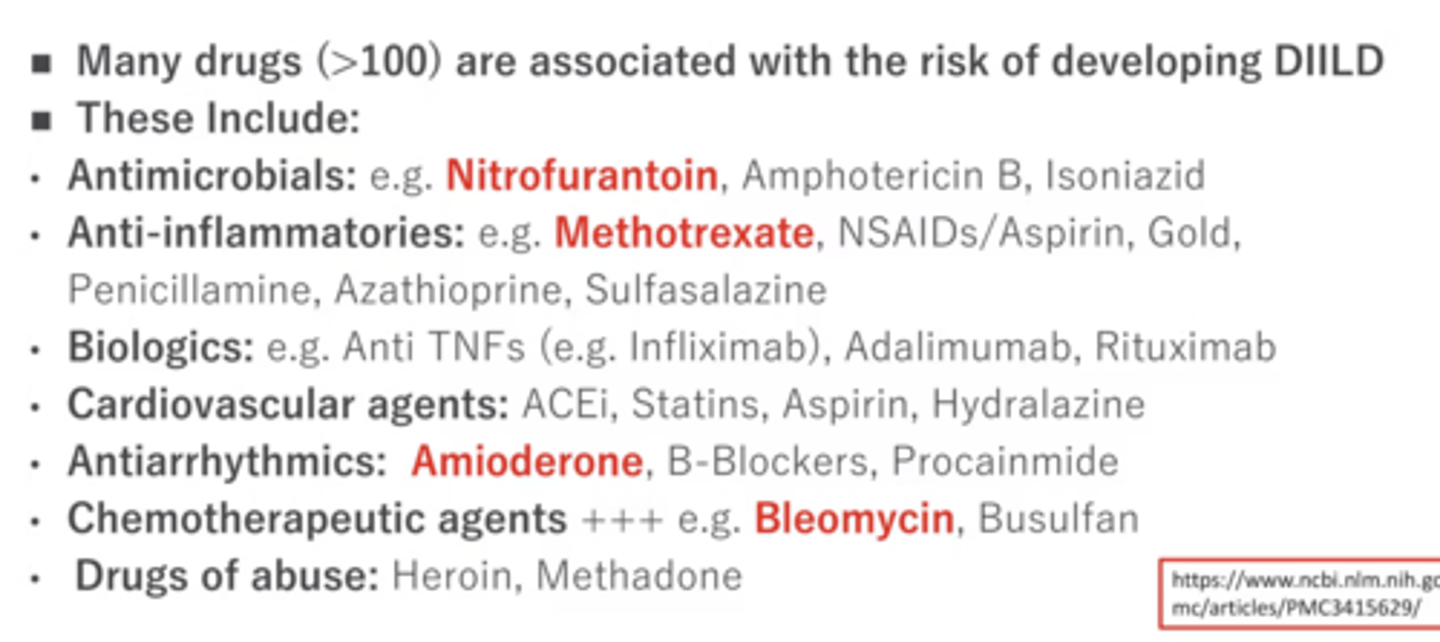
which drugs can common;y cause DIILD (drug induced interstitial lung disease?)
a lot but commonly:
1. nitrofurantoin
2. methotrexate
3. amiodarone
4. bleomycin
what happens if you take metronidazole and alcohol
also common side effect of metro
Metronidazole and alcohol can produce a disulfiram-like reaction
(cant drink alcohol on the metro
side effect: metallic taste in mouth
spironolactone side effect
gynaecomastia (bc it has anti-androgenic propreties)
importantly, NOT galactorrhea
metoclopramide and domperidone side effect
galactorrhea
(me=rhea)
what medications can cause sore gums
ciclosporin, amlodipine, phenytoin
phenytoin side effect
can cause acquired factor VIII deficiency as a side effect, leading to bleeding tendencies.
opioid overdose antidote
Naloxone
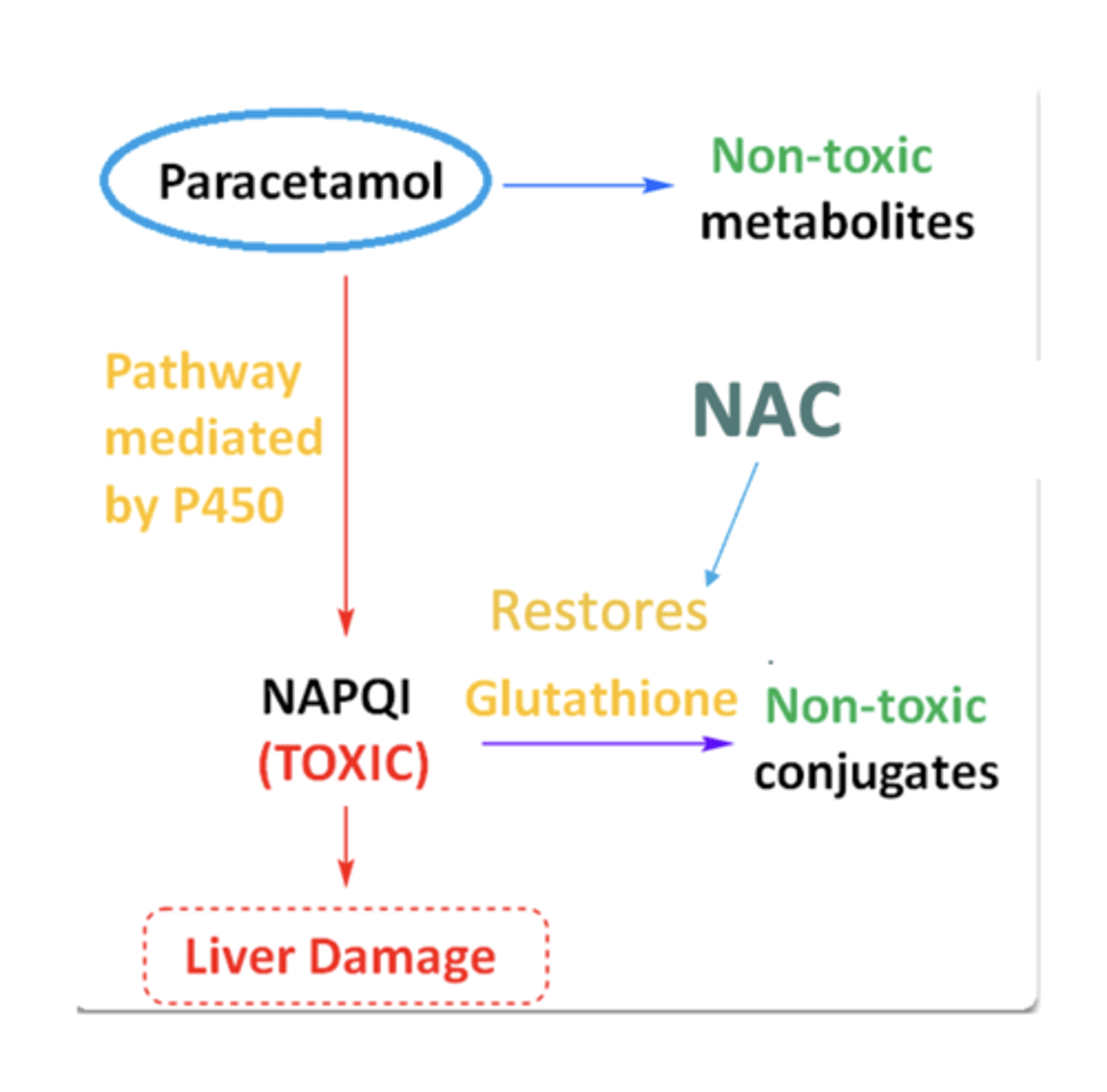
paracetamol overdose antidote
acute overdose (ingested in < 1 hour)
- if <1 hour since last ingestion
- consider activated charcoal if ingested >150 mg/kg
- 1-8 hours ingestion
- take bloods after 4 hours
- plot levels of paracetamol on nomogram
- if above line of concern: treat with NAC
- 8+ hours
- take bloods immediately
- if >150 mg/kg ingested or level of paracetamol is above nomogram,: start NAC
- 24 hours
- if presence of liver derangement (RUQ pain, deranged LFTs, jaundice, encephalopathy) - treat with NAC
staggered overdose (ingested in > 1 hour)
- start NAC immediately
- do bloods after 4 hours
- if results are unremarkable, NAC can be stopped. (senior review needed)
therapeutic excess - i.e an overdose without the intention of self harm
- start NAC if symptomatic
(NAC is not indicated if below nomogram UNLESS: uncertainty over timing of overdose, staggered overdose, unconscious patient)
how does NAC work
salicylate poisoning antidote
there is no antidote! so should be managed supportively
can consider:
1. IV fluids
2. activated charcoal
3. potassium replacement
4. sodium bicarb
what happens in an aspirin overdose
initially a respiratory alkalosis followed by a metabolic acidosis. Tinnitius can also be a feature
TCA overdose therapy
IV sodium bicarbonate
ethylene glycol toxicity management =
fomeprizole
DOAC reversal (e.g apixaban, rivaroxaban)
andexanet-alfa
dabigatran reversal
Idarucizumab
dapagliflozin - what is a side effect in diabetics
can cause euglycaemic hyperosmolar ketoacidosis
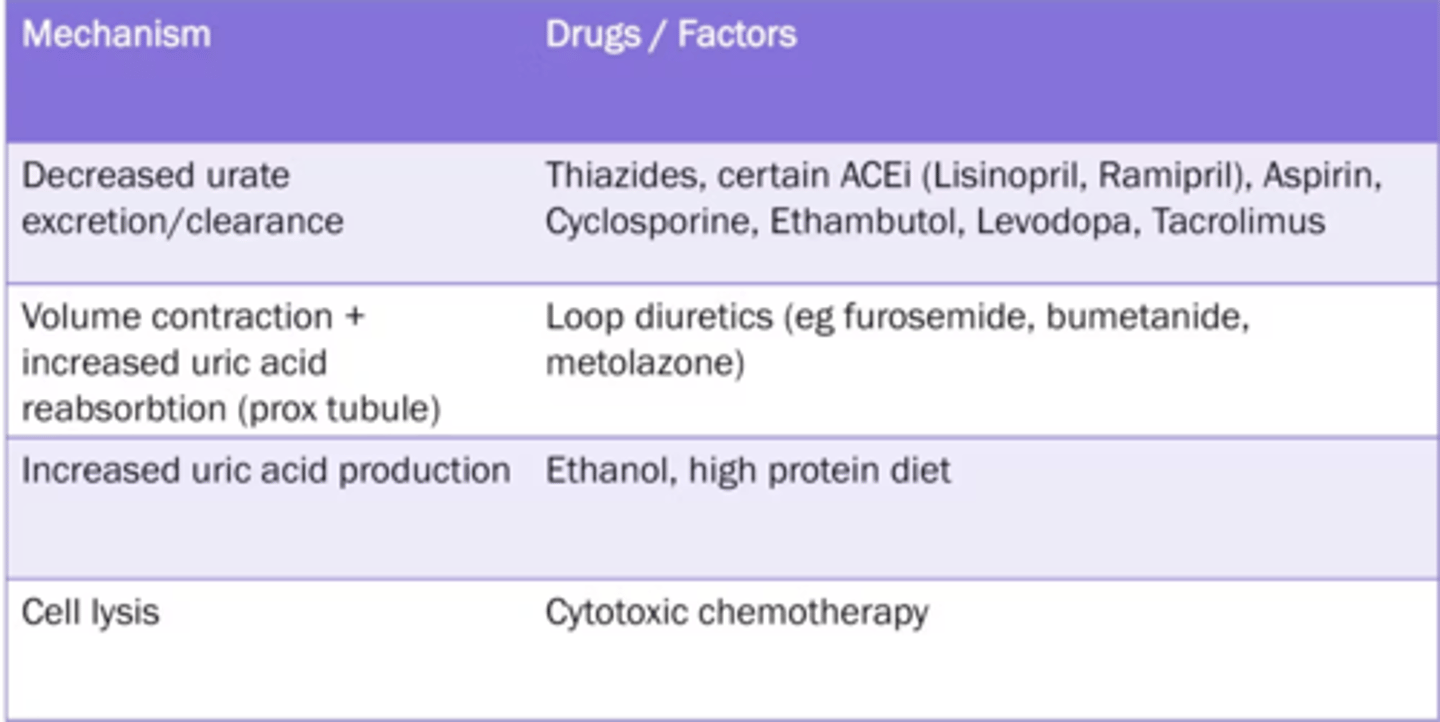
drugs that predispose to gout
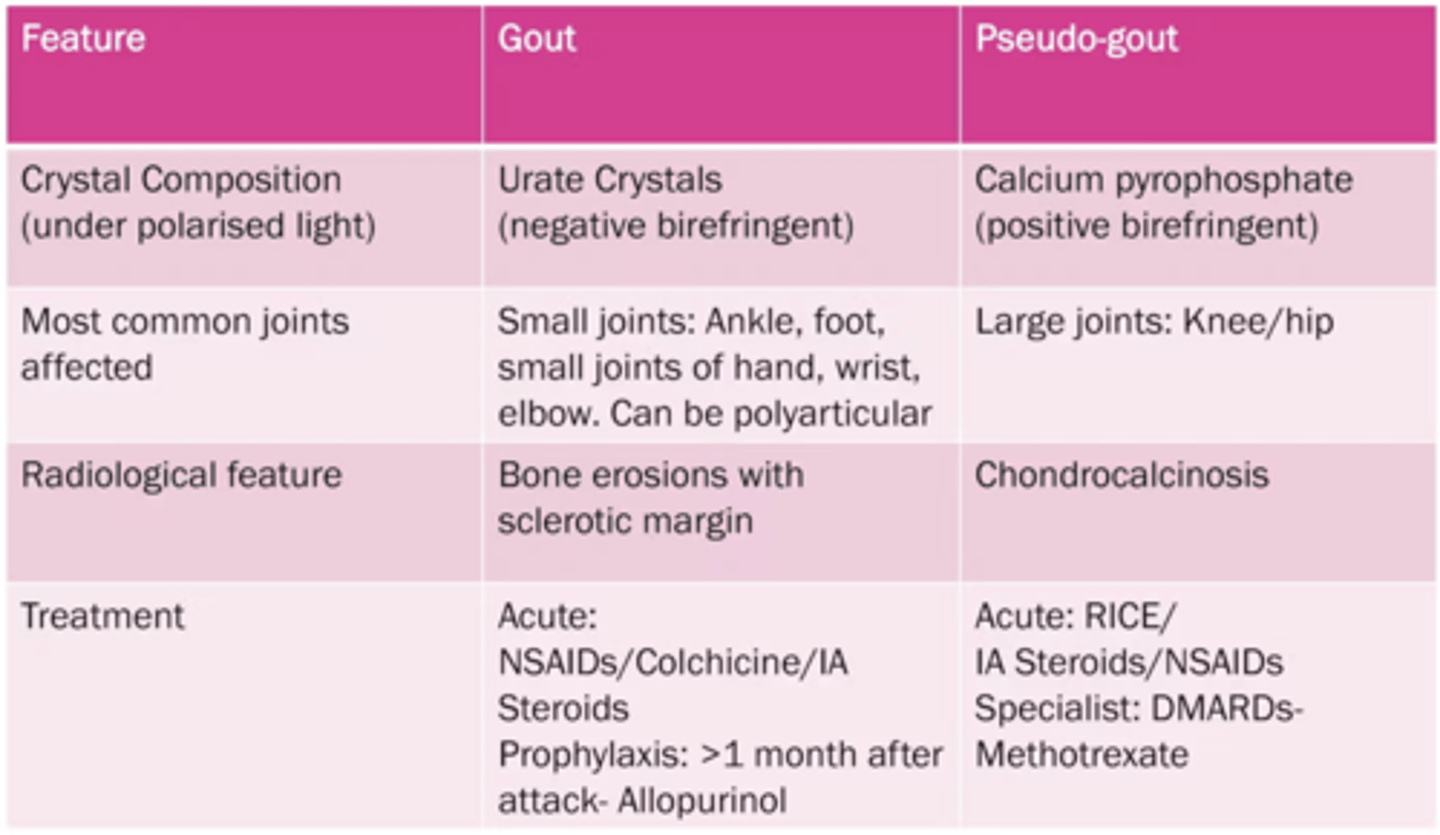
gout vs pseudo gout
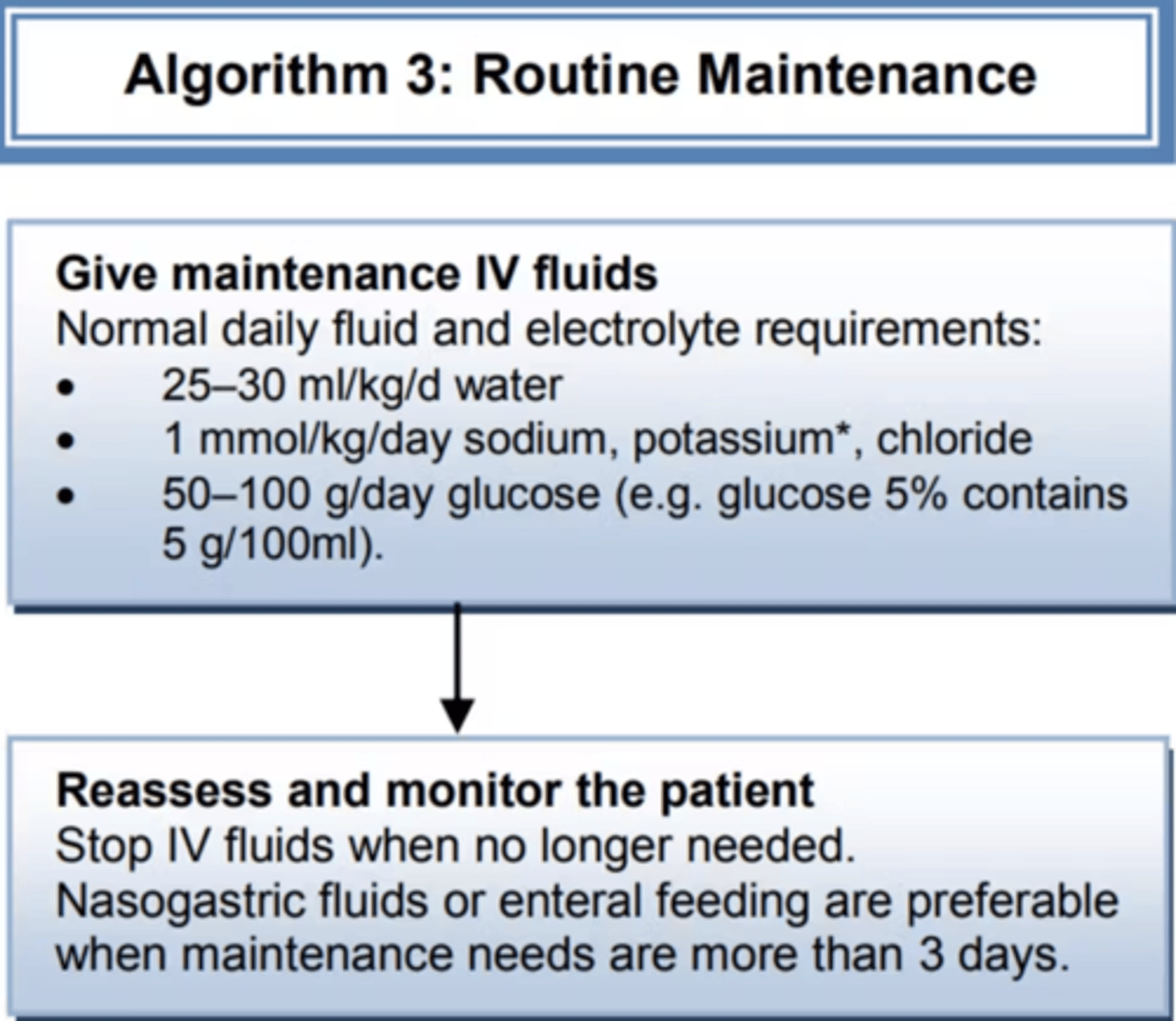
what fluids do you give to someone who is nil by mouth (NBM
THIAZIDE DIURETICS effects, also what can it worsen?
hyponatremia, hypokalaemia, hypercalcemia,
Thiazide Takes back calcium (into the blood)
Loop diuretic Loses calcium (into the urine)
TZDs can worsen glucose tolerance
CALCIUM CHANNEL BLOCKERS side effect
gingival hyperplasia
P450 INDUCERS
"CRAPGPS"
Carbamazepine
Rifampicin
Alcohol (chronic use)
Phenytoin
Griseofulvin
Phenobarbital
Sulfonylureas
INDUCE RAGE
P450 INHIBITORS
"SICKFACES.COM"
Sodium valproate
Isoniazid
Cimetidine
Ketoconazole
Fluconazole
Alcohol (acute use)
Chloramphenicol
Erythromycin (and macrolides)
Sulfonamides
Ciprofloxacin
Omeprazole
Metronidazole
ACE inhibitor side effect
angioedema! can present even after a year.
tetracyclines side effect
black hairy tongue
risk of taking DAPT and NSAIDs
peptic ulcers and then GI bleed
types of antiemetics
5-HT3 antagonists: ondansetron
D2 antagonists: metoclopramide, prochlorperazine
H1 antihistamines: promethazine, cyclizine
complication of taking antiemetic
with metoclopramide and prochlorazine
a complication can be an oculogyric crisis
- eyes roll upwards
- mouth opens
- tongue protrudes
treated with procyclidine
amiodarone complication
thyrotoxicosis
drug counselling tips
first ask about condition
lifestyle factors
STATINS side effect, when to take
- musculoskeletal: rhabdomyolysis, myalgia
- Gastrointestinal: nausea, vomiting, elevate liver enzymees
take at night to maximise effect!
- contraindicated in pregnancy?
when should steroid be withdrawn gradually?
the BNF suggests gradual withdrawal (i.e over weeks) of systemic corticosteroids if patients have:
- received more than 40mg prednisolone daily for more than one week
- received more than 3 weeks of treatment
- recently received repeated courses
METHOTREXATE antidote to overdose
folinic acid
ACE INHIBITOR drug counselling
ACTION
works to relax and widen blood vessels
TIMING
taken once a day, usually in the morning
HOW TO TAKE IT
tablet taken with water
LENGTH OF TREATMENT
usually long-term
EFFECTS
preserves kidney function
reduces blood pressure
helps with management after a heart attack or stroke
TESTS
check kidney function
regular home BP monitoring
IMPORTANT SIDE EFFECTS
can initially cause some dizziness
nausea, vomiting
CONTRAINDICATIONS
history of angioedema
pregnancy
try to limit nsaid use
SUMMARISE, SAFETY NET AND LEAFLET
lifestyle factors cmon
BISPHOSPHONATE drug counselling
ACTION
prevents bone from breaking down, and also rebuilds new bone
TIMING and HOW TO TAKE IT
- take as a tablet with water weekly (for alendronate and risedronate). for zoledronate its an annual infusion
- 30 mins before eating
- sit up straight for the 30 minutes
LENGTH OF TREATMENT
long-term
can have drug holiday after 5 years after doing DEXA
EFFECTS
will help to reduce risk of osteoporotic fractures
TESTS
regular dental check ups required (for osteonecrosis of the jaw), renal function tests
IMPORTANT SIDE EFFECTS
- oesophagitis
- osteonecrosis of the jaw
- Gi (nausea, vomiting, constipation)
- atypical stress fractures
CONTRAINDICATIONS
- pregnancy
- unable to sit upright for 30 minutes
- renal impairment
SUPPLEMENTARY INFO
lifestyle factors also important!
DOAC drug counselling
A
works to thin blood
T
tablet taken once daily
H
- take with glass of water
- sit upright
L
for VTE - 3/6 months. For AF - lifeliong
E
prevents clot formation
T
before starting renal function tests. And then renal function tests annually
I
- GI disturbance
- bleeding (safety net: if severe bruising, head injury, prolonged epistaxis then seek medical advice)
C
- current bleeding
- risk of major bleeding
- renal impairment
- pregnancy?
S
none
INSULIN drug counselling
ACTION
works by replacing normal insulin which helps glucose be absorbed from the bloodstream into cells
TIMING
HOW TO TAKE IT
there are different insulin regimens e.g injection into thigh
LENGTH OF TREATMENT
long-term
EFFECTS
TESTS
CBG should be done before each meal
IMPORTANT SIDE EFFECTS
- weight gain
- sharps injuries
- hypoglycaemic / hyperglycaemic episode (safety net for symptoms such as confusion)
CONTRAINDICATIONS
none
SUPPLEMENTARY INFO
none
IRON TABLETS counselling
ACTION
works by replacing iron levels, helps body make RBC
TIMING
works best if taken before food, however most people take with food due to GI irritation
HOW TO TAKE IT
taken as a tablet or syrup- dose can vary from 1-3 times a day, or on alternate days
LENGTH OF TREATMENT
long-term
EFFECTS
will help with iron deficiency symptoms
TESTS
Hb 3-4 weeks after starting tablets to assess response
IMPORTANT SIDE EFFECTS
GI irritation
metallic taste
black/green stools
CONTRAINDICATIONS
none
SUPPLEMENTARY INFO
none
LEVODOPA drug counselling
ACTION
- increases dopamine
TIMING AND HOW TO TAKE IT
- take as a tablet 3-4 times daily with food
- given with carbidopa
LENGTH OF TREATMENT
- long term
EFFECTS
TESTS
IMPORTANT SIDE EFFECTS
- nausea
CONTRAINDICATIONS
SIDE EFFECTS
- nausea
- postural hypotension
LEVOTHYROXINE drug counselling
ACTION
works by replacing normal thyroid hormone
TIMING
every day before breakfast on an empty stomach
HOW TO TAKE IT
LENGTH OF TREATMENT
long-term
EFFECTS
will help with hypothyroid symptoms
TESTS
TSH testing every 2-3 months until stable. Once stable, TSH testing annually
IMPORTANT SIDE EFFECTS
if dose too high: hyperthyroid symptoms
if dose too low: hypothyroid symptoms
CONTRAINDICATIONS
none
SUPPLEMENTARY INFO
METHOTREXATE drug counselling
ACTION
disease modifying drug, helps to suppress immune system
TIMING
HOW TO TAKE IT
- once weekly tablet. Take folic acid on another day
- take on same day each week
LENGTH OF TREATMENT
long-term if effective
EFFECTS
TESTS
- Bloods before starting
- Bloods every 2 weeks until therapy stabilised
- Once stabilised, bloods every 2 months
IMPORTANT SIDE EFFECTS
- alopecia
- GI disturbance
- headaches
- liver and lung toxicity
CONTRAINDICATIONS
- pregnancy - should stop 6 months before conception (so should men)
- breast feeding
- liver impairment
SUPPLEMENTARY INFO
STATINS drug counselling
A – Action
Lowers cholesterol → reduces risk of heart attack/stroke.
T – Timing
Take once daily, usually at night. If miss a dose take straight away. Don't double
H – How to take it
Swallow with water, with or without food.
L – Length of treatment
Long-term (usually lifelong).
E – Effects
Lowers cholesterol, reduces cardiovascular risk.
T – Tests
Monitor liver function and cholesterol via blood tests.
I – Important side effects
Muscle pain, fatigue, GI disturbance, rhabdo, liver dysfunction (rare).
C – Contraindications/Complications
Avoid excess alcohol; beware of drug interactions.
S – Supplementary advice
Lifestyle changes (diet, exercise) enhance effect.
STEROIDS drug counselling
A – Action
Anti-inflammatory & immunosuppressive.
Replaces steroids called cortisol which we normally produce.
L – Timing
Take once in the morning. If missed, take ASAP. Don’t double.
T – How to take it
With/after food. Swallow with water.
H – Length of treatment
Short or long-term. Taper if long-term.
E – Effects
Reduces symptoms & flare-ups.
T – Tests
Monitor BP, glucose, weight, bone, adrenal function.
I – Important side effects
Short-term: insomnia, mood changes, increased appetite, indigestion.
Long-term: osteoporosis, diabetes, Cushingoid features, infection risk, adrenal suppression
C – Contraindications/Complications
Caution in DM, HTN, ulcers, infections. No live vaccines.
S – Supplementary advice
Carry steroid card. Don’t stop abruptly. Follow sick day rules. Bone protection if long-term.
SICK DAY RULES
- must increase steroid dose (to mirror normal physiological increase in steroids when ill)
WARFARIN drug counselling
A - Action
Vitamin K antagonist. Vitamin K part of clotting cascade. Prevents clotting
T - Timing
Oral tablet once daily
initially given with heparin for 3-5 days
H - How to take it
In evening
L - Length of treatment
Can be lifelong
E - Effects (benefits)
Prevention of clotting
T - Tests
INR -
once a day for a week,
then once a week
once stable - once every 3 months
I - Important side effects
- N/V
- bleeding, bruising, dark stools
C - Complications/Contraindications
- keep a warfarin yellow book
- avoid eating leafy greens, cranberry juice
- if miss a dose, take another within 24 hours. Dont double dose on a day
- If you miss for more than 2-3 doses, contact doctor
- tell doctor you are on warfarin before having a procedure
S - Summary
- summarise
- leaflet
- safety net.
ANAPHYLAXIS prescribing
0.5 mg OR 0.5 mL 1:1000 IM STAT
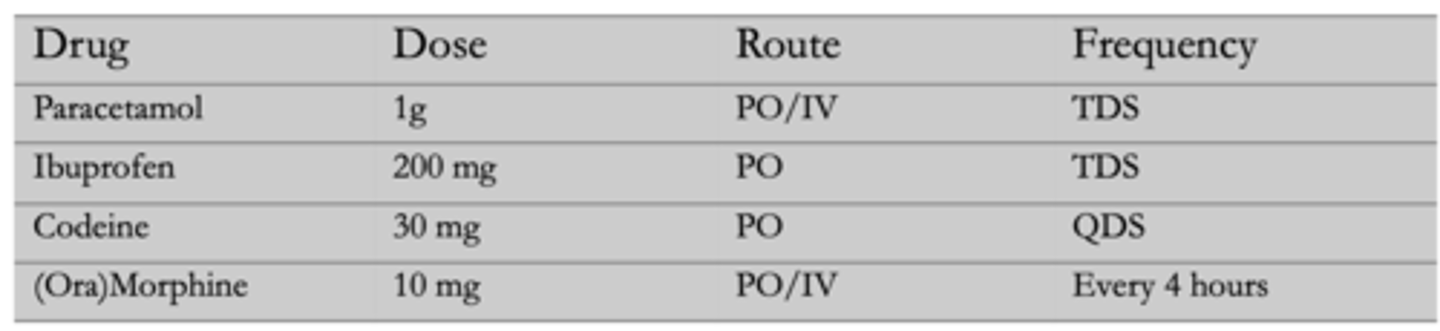
ANALGESIA prescribing
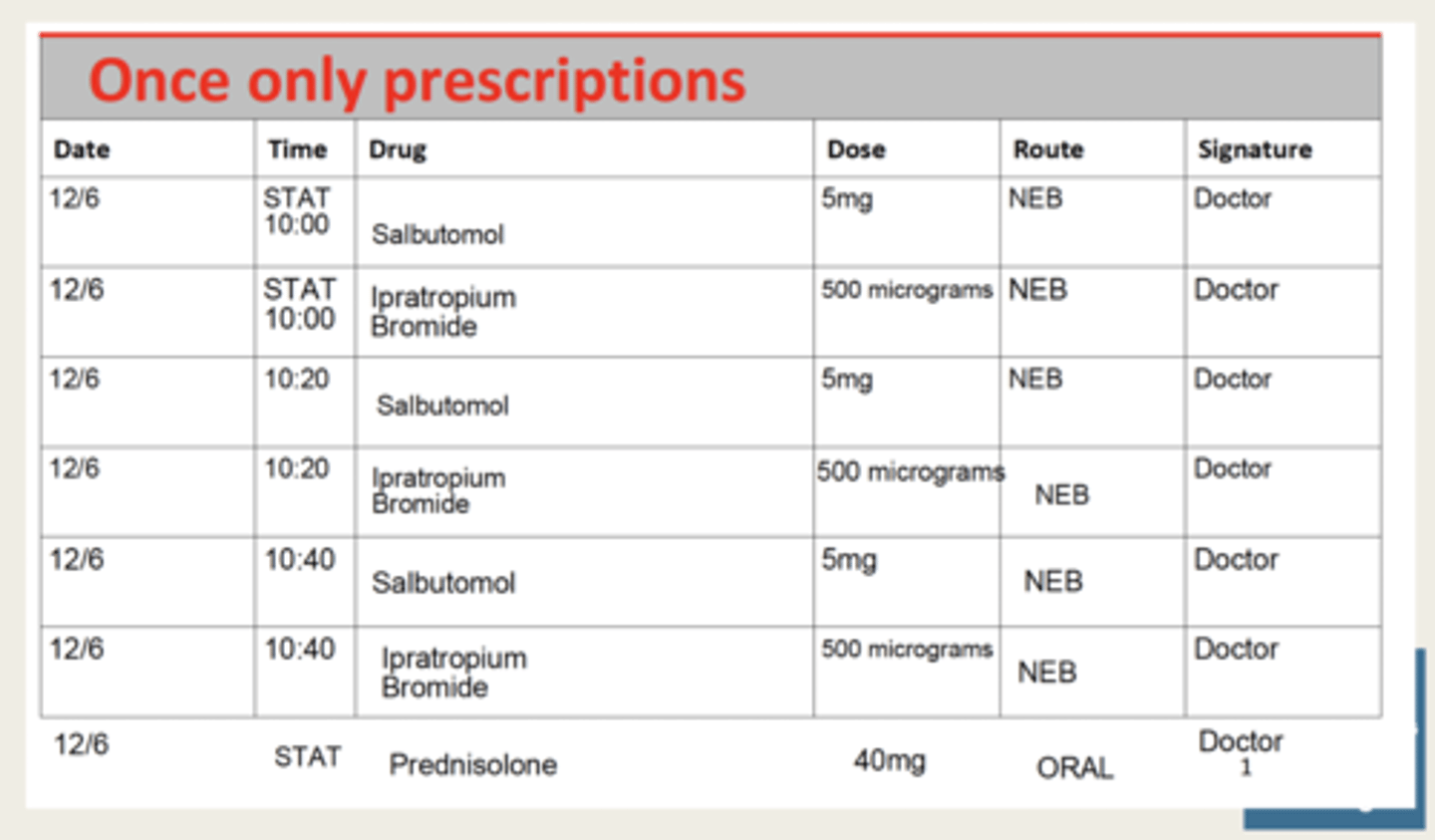
ASTHMA prescribing
STAT
- salbutamol 5mg NEB
- prednisolone 40mg PO (40 = asthma dose, 30 = COPD dose)
- ipratropium bromide (500 micrograms) NEB (if severe)
dont think you can give: (magnesium sulfate 2g IV (if severe))
PRN - always give indication here
- salbutamol 5mg NEB every 15-30 mins
- ipratropium bromide (500 micrograms) NEB (if severe)
QDS max frequency is 6 times daily
REGULAR
- Prednisolone 40mg PO for 5 days
if severe:
- oxygen
ASTHMA BURST therapy prescribing
COPD prescribing
STAT
- salbutamol 5mg NEB
- prednisolone 30mg PO (40 = asthma dose, 30 = COPD dose)
- Ipratropium 250micrograms or 500micrograms NEB
PRN - always give indication here
- salbutamol 5mg NEB
REGULAR
- Prednisolone 30mg PO
ANTI-INFECTIVES
500mg amoxillin TDS
if severe:
- oxygen via venturi mask. target range - 88-92 if co2 retainers
RENAL COLIC prescribing
1. diclofenac sodium - STAT, 75mg, IM
2. metoclopramide - PRN, 10mg, PO, TDS
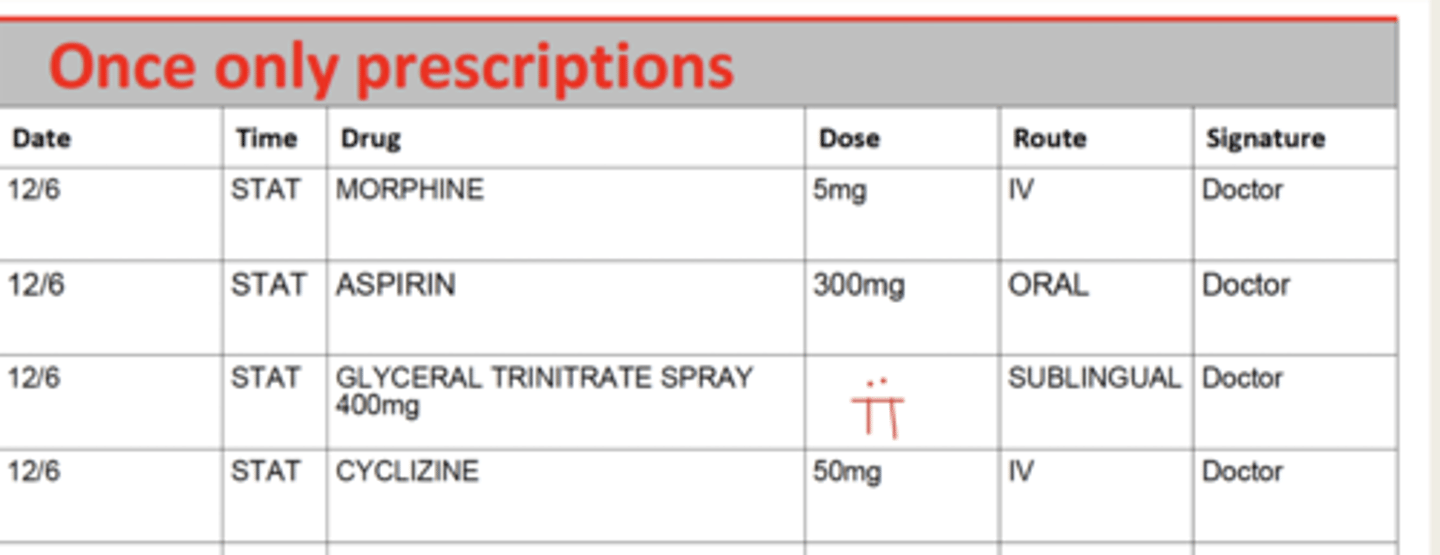
NSTEMI prescribing
STAT
1. morphine 10mg PO or 5mg IV
2. metoclopramide (for morphine) - 10mg IV
2. oxygen if sats < or equal to 94%
3. Glyceryl trinitrate: 2 puffs, sublingual
4. aspirin 300mg PO
5.
- clopidogrel 300mg PO
- prasugrel 60mg PO
- ticagrelor 180mg PO
REGULAR
fondaparinux 2.5mg PO OD
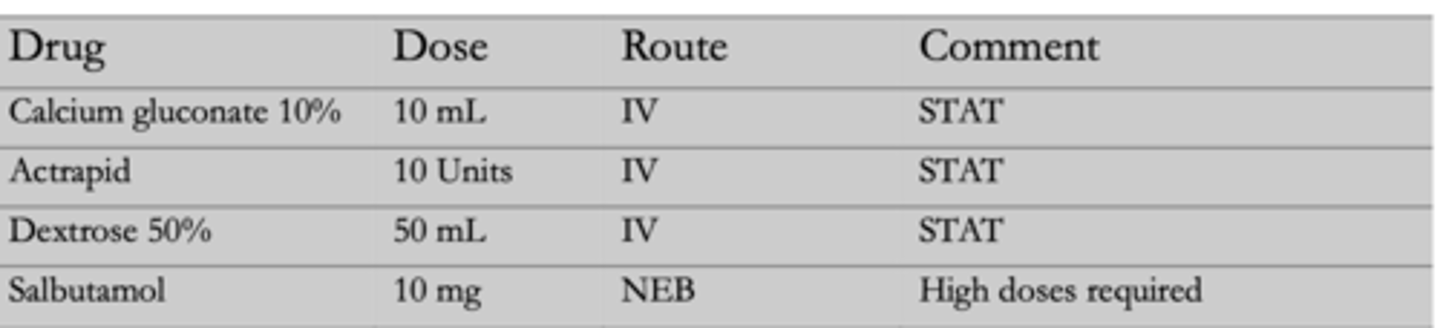
HYPERKALAEMIA prescribing
STAT
Calcium Gluconate 10% 10 mL (stabilises cardiac membranes)
Salbutamol 10mg NEB (moves K+ into cells)
INFUSIONS
Dextrose 50% 50mL with inulin (actrapid) 10 units
PULMONARY OEDEMA prescribing
Furosemide 40mg PO OD
Morphine
N - GTN
O - oxygen
Position sit up straigh
DKA prescribing
the actrapid should be within 50mL sodium chloride
it should be given at 0.1 units/kg/hour and you alwasy give 50 units

HHS prescribing
IL 0.9% sodium chloride over 1 hour
also VTE prophylaxis due to hypervisvosity
STEMI prescribing
STAT
1. morphine 10mg PO or 5mg IV
2. metoclopramide (for morphine) - 10mg IV
2. oxygen if sats < or eual to 94%
3. Glyceryl trinitrate: 2 puffs, sublingual
4. aspirin 300mg PO
5.
- clopidogrel 300mg PO
- prasugrel 60mg PO
- ticagrelor 180mg PO
PNEUMONIA (community acquired) prescribing
depends on CURB 65 score
1. mild (0.1)
Amoxicillin 500mg, PO, TDS for 5 days
2. moderate (2)
Amoxicillin 500mg, PO TDS for 5 days
if pen allergic: Clarithromycin 500mg, PO BD for 5 days
if atypical suspected:
Amoxicillin 500mg, PO TDS for 5 days
+ Clarithromycin 500mg, PO BD for 5 days
3. severe (3 or more)
- Co-amoxiclav 1.2g IV TDS (every 8 hours) WITH clarithromycin 500mg PO BD
NEUTROPENIC SEPSIS prescribing
ANTI-INFECTIVE: piperacillin with tazobactam 4.5g IV every 6 hours for 48 hours
after that change to vancomycin or meropenem
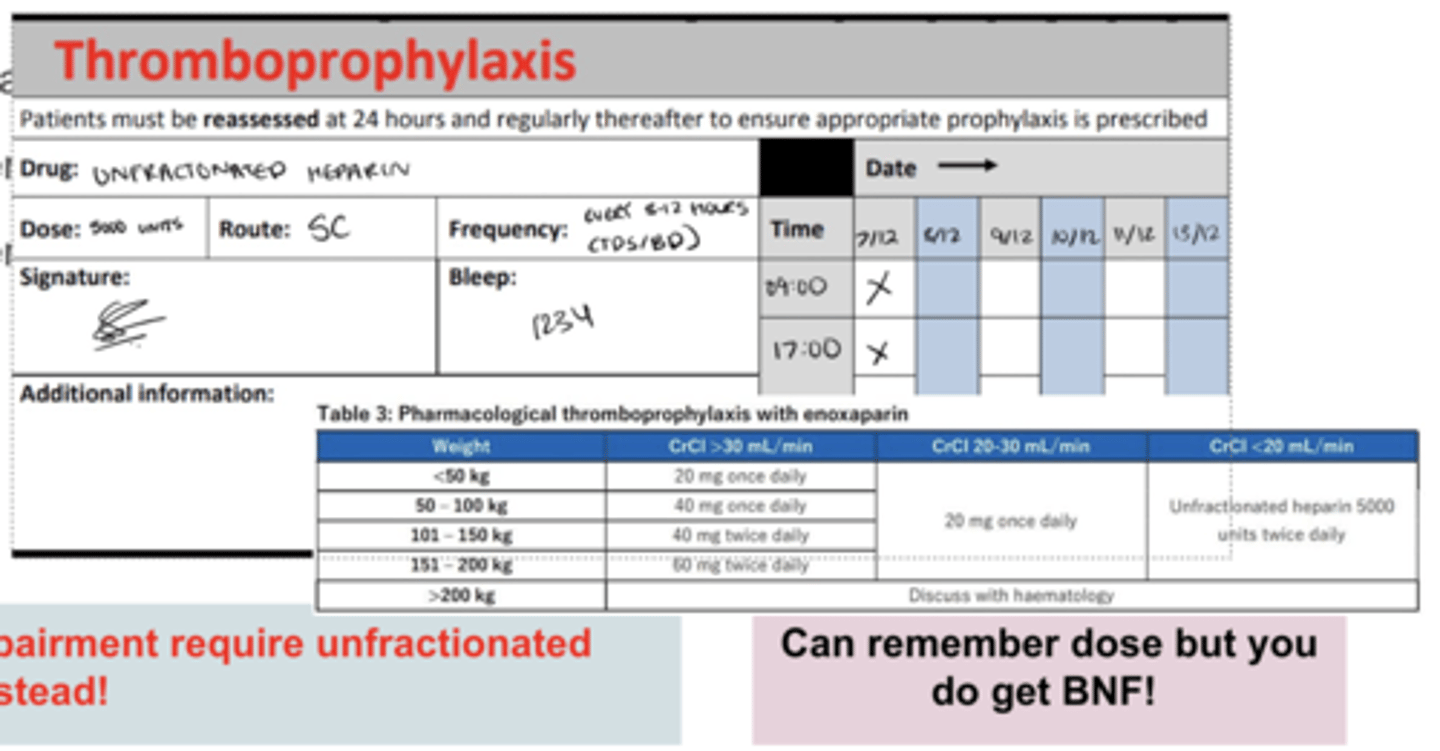
VTE PROPHYLAXIS prescribing
enoxaparin SC 40mg OD
in thromboprophylaxis section!!
OR
in renal impairment
5000 units unfractionated heparin BD (every 8-12 hours)
PERI-OP prescribing
FLUIDS - maintenance]
2 sweet 1 salty
5% dextrose 500mL with 20mmol potassium chloride 8h
5% dextrose 1000mL with 40mmol potassium chloride 8h
0.9% sodium chloride 500mL with 20 mmol potassium chloride 8h
THROMBOPROPHYLAXIS
ENOXAPARIN 40MG SUBCUT OD
REGULAR
Senna
15mg, PO ON
Omeprazole
20mg, PO OD
Paracetamol
1 gram, PO, QDS, max 4g a day
Cyclizine
50mg, PO, max 3 times a day
PRN - always put reason why
Morphine
10mg, PO, max dose every 4 hours
FT SOP MC
FLUIDS prescribing
daily requirement
Na+/K+ = 1 mmol/kg/day
water = 25-30 mL/kg/day
Glucose = 50-100g/day
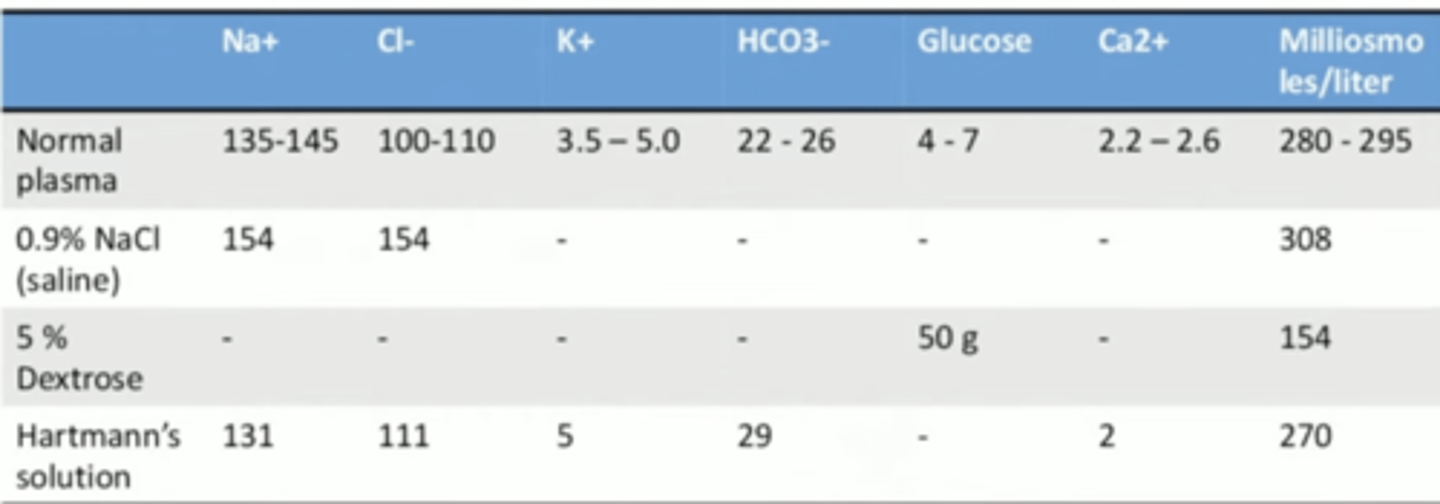
in 1L of 0.9% NaCl - 154 mmol of Na and Cl
In 1L of Dextrose 5% - 50g of glucose
dont give more than 10 mmol per hour for K+
POST STROKE
1. atorvastatin
2. ramipiril
3. bisoprolol
4. aspirin
5. clopidogrel
how to stop a medication
1. put a clear line
2. name
3. signature
4. reason for stopping