wk 2- class V restorations/subging CORD isolation
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
39 Terms
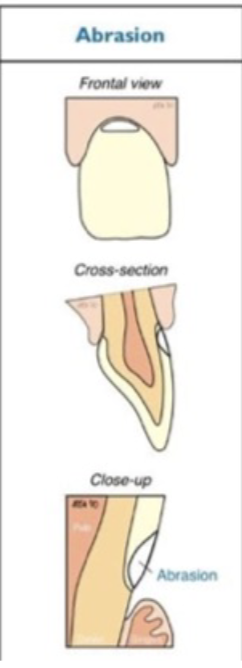
abrasion cause
mechanical wear- like toothbrush habit
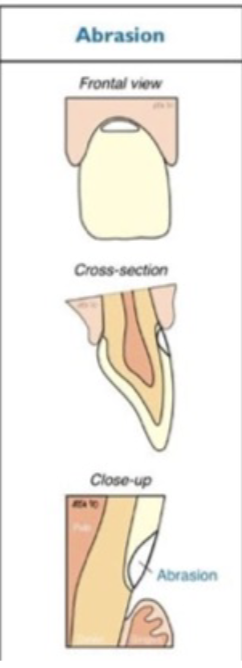
abrasion affect
teeth in groups- often unilateral
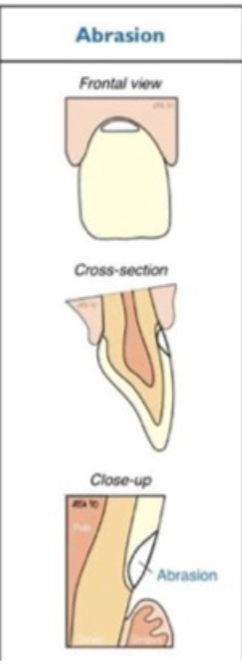
abrasion tx
comosite- hybrid or flowable
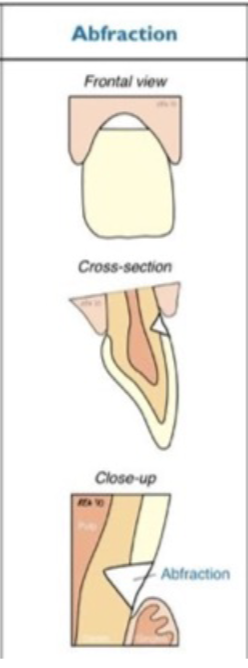
abfraction cause
stress corrosion- occlusion related
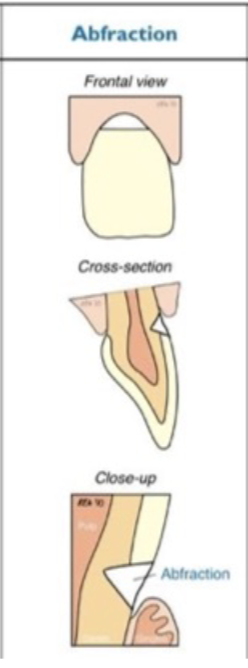
abfraction affects
single tooth- often upper premolars first
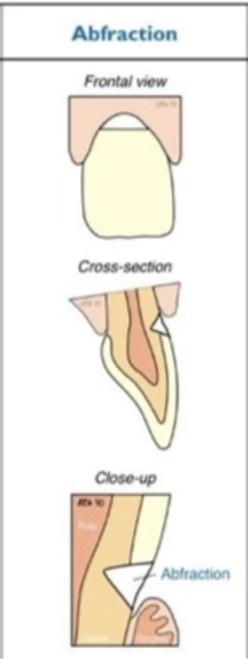
abfraction tx
composite- hybrid or flowable, light cured GIC
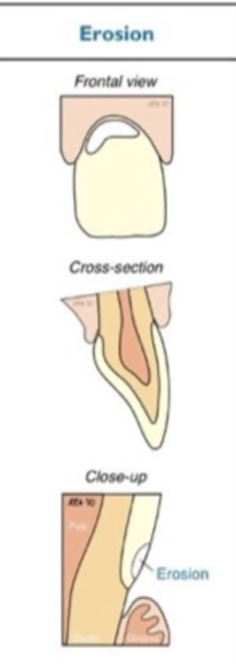
erosion cause
chemical erosion- gastric causes

erosion affects
teeth in groups- lingual on upper and buccal on lowers
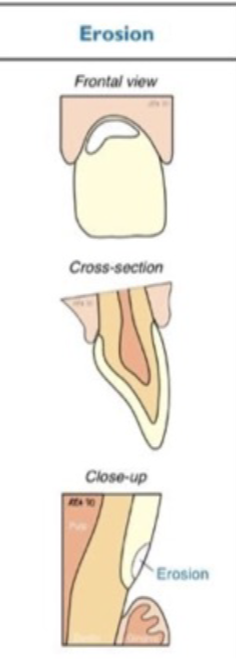
erosion tx
composite- hybrid or flowable
what is the basic erosive wear examination
the mouth is divided into 6 distinct areas for evaluation, using the criteria for sextant scores from 0 to 3 and the surfaces w the highest score is recorded for each sextant
the scores are summed to obtain a cumulative score that is the basis for determining interventions
management challenges for erosive tooth wear
early dx of erosive lesion
initiation of preventative strategies and behavioral changes
early intervention w minimally-invasive restorative procedures
early dx of erosive tooth wear should include
charting of erosive lesions
sensitive teeth
staining
making note of areas of exposed dentin
preventative habits that reduce the risk fo erosive tooth wear
staying hydrated
rinsing w water before brushing
brushing w fluoride toothpaste
not brushing for at least 1-2 hours after an acid challenge
erosive tooth wear score 0
no erosive tooth wear
erosive tooth wear score 1
initial loss of surface texture

erosive tooth wear score 2 (dentin)
distinct defect; hard tissue loss involving <50% of the surface area (only molar)

erosive tooth wear score 3 (dentin)
hard tissue loss involving >/= 50% of the surface area

if the cumulative score for erosive tooth wear is 0-2 (not rlly any ETW), what are the general guidelines for management
routine maintenance for observation
repeat at 3-yr intervals
if the cumulative score for erosive tooth wear is 3-8 (low), what are the general guidelines for management
oral hygiene, dietary assessment
routine maintenance and observation
repeat at 2-yr intervals
if the cumulative score for erosive tooth wear is 9-13 (medium), what are the general guidelines for management
oral hygiene, dietary assessment
routine maintenance
fluoride measures
avoid restorations requiring tissue removal
repeat at 6-12 month intervals
if the cumulative score for erosive tooth wear is >/= 14 (high), what are the general guidelines for management
oral hygiene, dietary assessment
routine maintenance
fluoride measures
repeat at 6-12 month intervals
consider restoration
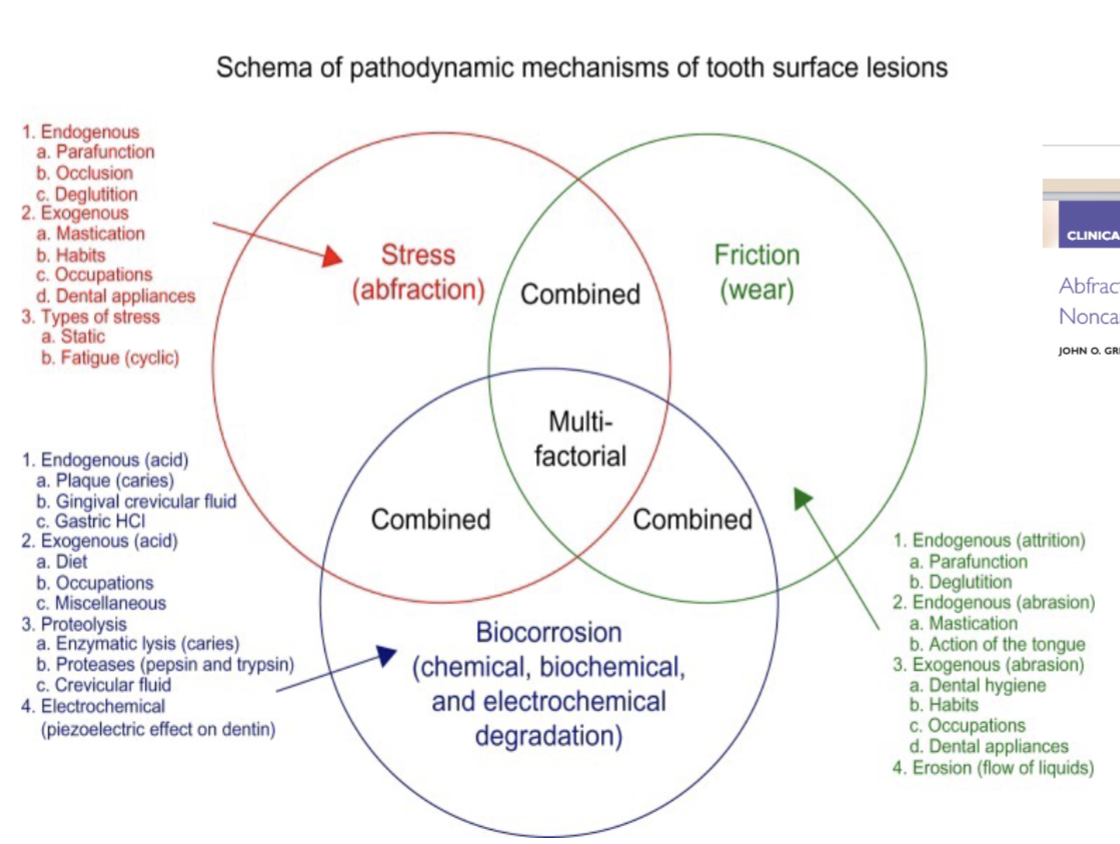
when thinking of the scema of pathodynamic mechanism of tooth surface lesion, what are the 3 factors
stress- abfraction
friction- wear
biocorrosioin- chemical, biochemical, electrochemical degradation
what are the 7 situation when you would restore non-carious cervical lesions (NCCLs)
active, cavitated carious lesions associated w the lesion- CRA must be conducted (carious or complex cervical lesion)
cervical margins are subgingival precluding plaque control inc caries- biocorrosion and periodontal disease risk
extensive tooth structure loss, which compromises the integrity of the tooth
defect is in close proximity to the pulp, or the pulp has been exposed
persistent dentinal hypersensitivity, in which noninvasive therapeutic options have failed
prosthetic abutment
esthetic demand- by pt request
funx of B4 clamp
aids in isolation by retracting tissue without harming surrounding gingival tissue

which clamos are used to provide access if rubber dam is used
#212
#B4
besides clamps, what is another way you can get isolation
retraction cords

response from astringents
contraction-retraction of the tissues
response to hemostatic agents
constrict blood flow through coagulation
common compounds of astringents/hemostatic agents
ferric sulfate 15-20%: viscostat
aluminum potassium sulfate
aluminum sulfate
aluminum chloride 20-25%
racemic epinephrine 4-8%
when to place cord
before preparation or before restorative material placement
steps of cord placement
eval the health of gingiva and the depth of the sulcus to select the proper cord- single or double
soak the cord in astringent/hemostat, avoid axcess solution
loop cord around tooth, depending ont he preparation area; adjust length to cover mesial and distal
repeat process for a second cord if needed
when time to remove- wet cord w water so it won’t grab and tear the tissues when removed and create more bleeding
after removal, you have about 30 sec until gingiva goes back, use this time to further subgingival finish if needed
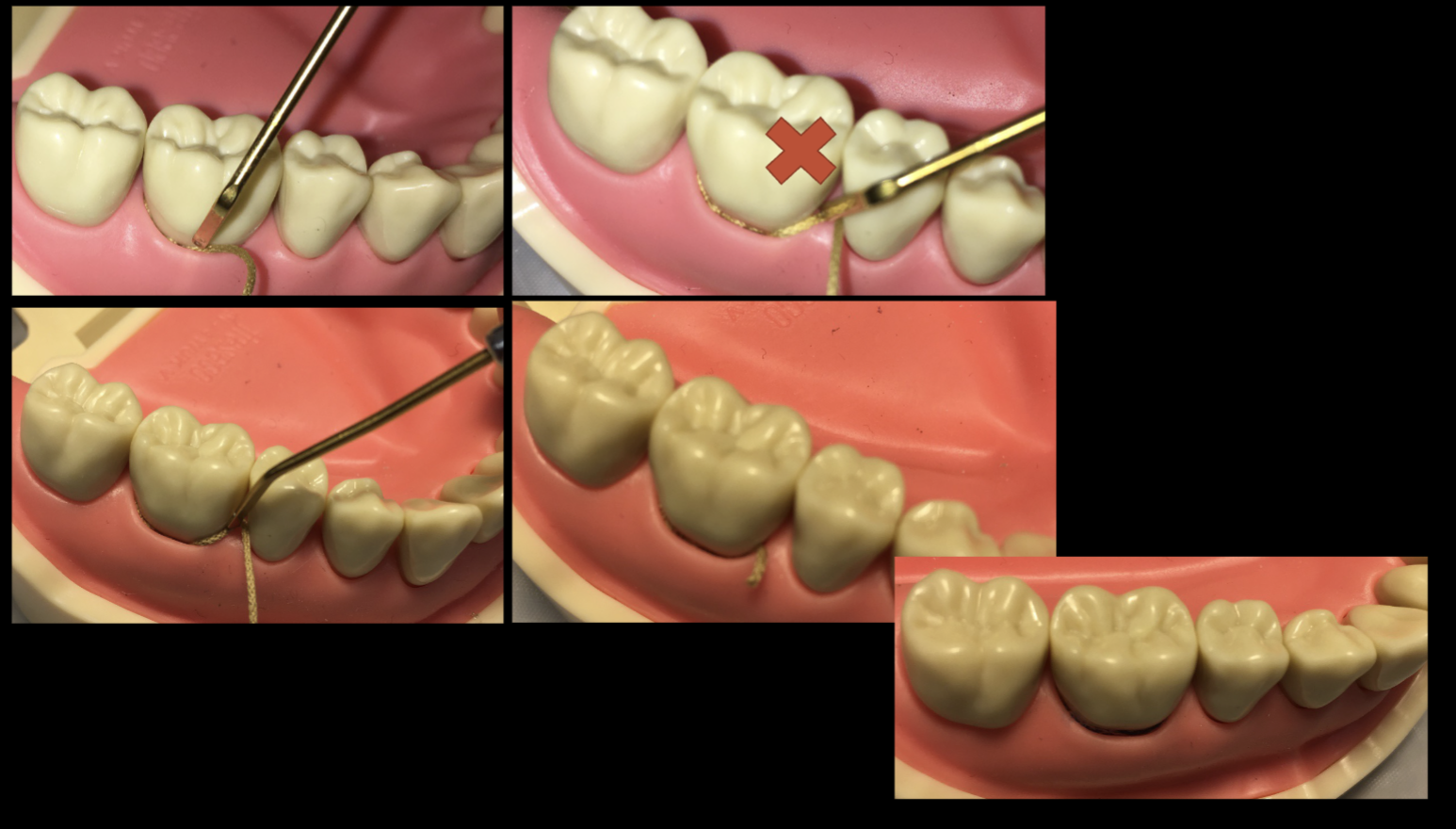
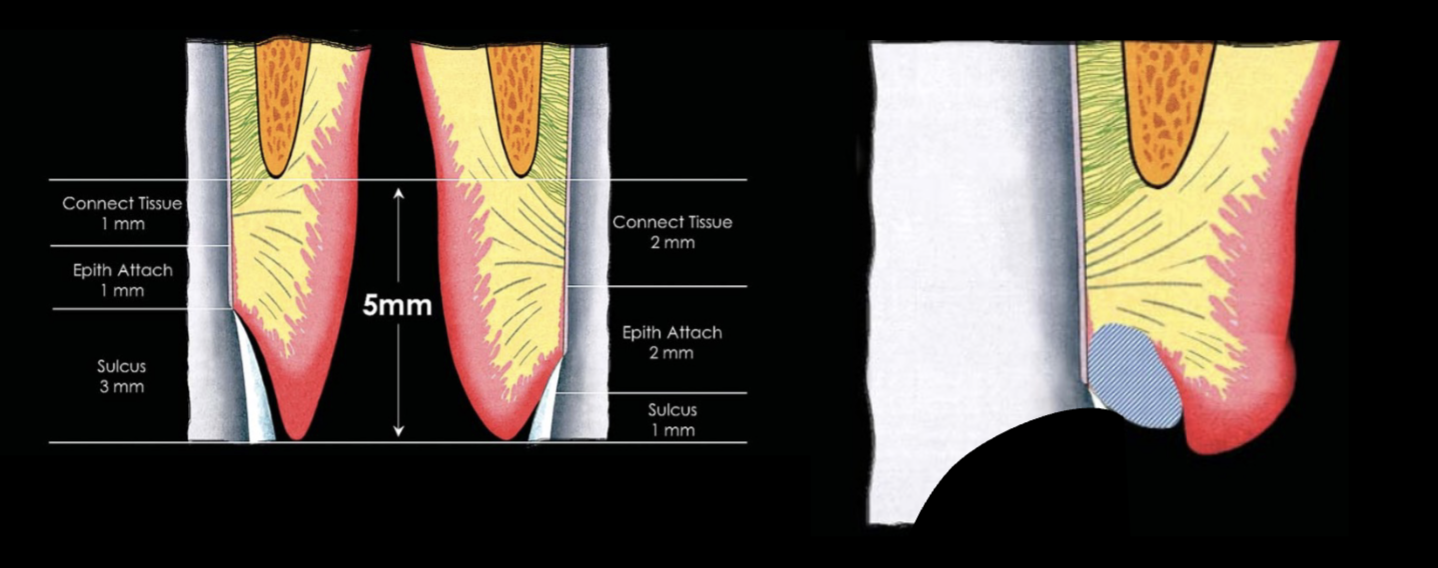
where is the cord actually packed
in the sulcus, ~1-3 mm; so don’t be aggressive
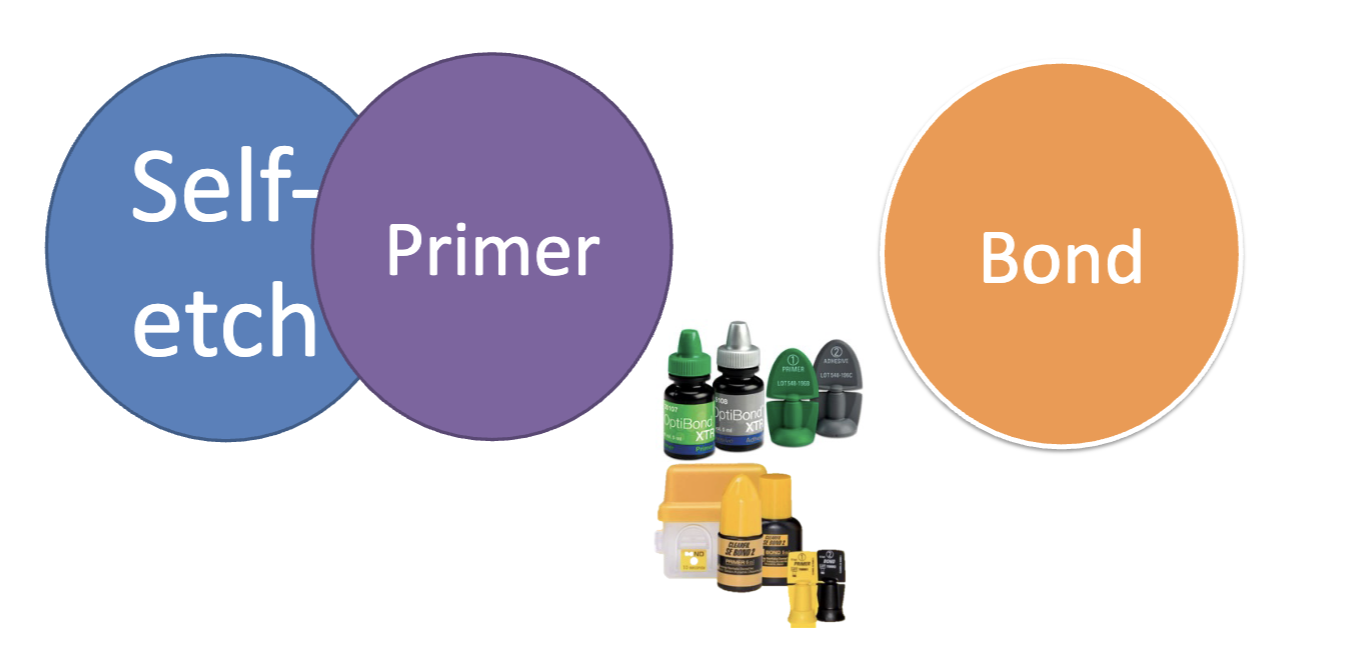
4th gen adhesive
three-step bonding- total etch and rinse (go-to)
PA etch, rinse
primer, dry
bond

5th gen adhesive
2-step total etch and rinse (stay away??)
PA etch, rinse/dry
primer + bond, dry

6th gen adhesive
2-step self-etch (go-to??)
self etch + primer, dry
bond
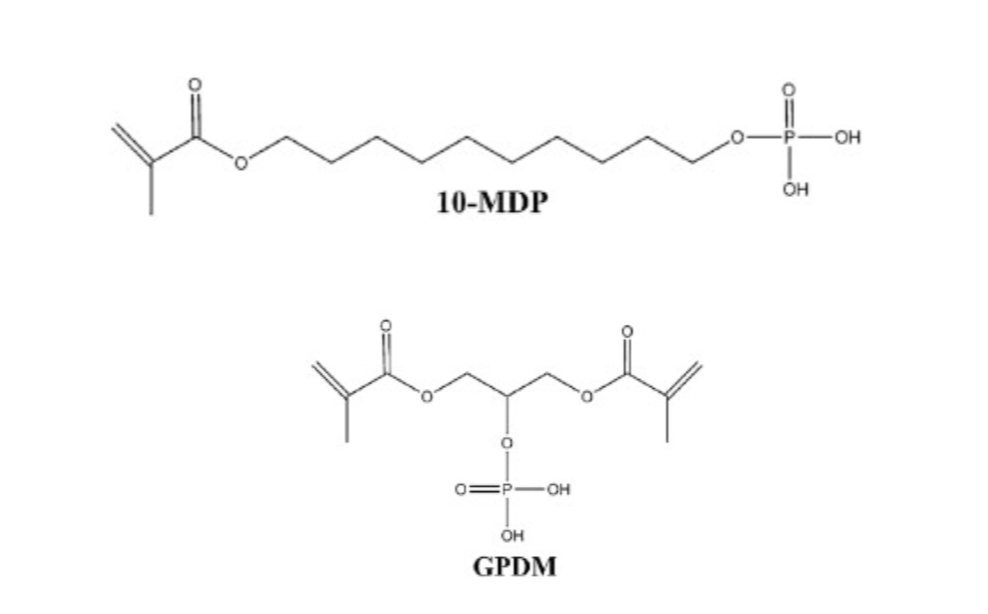
types of adhesive monomers
10-MDP
GPDM
7th gen universal all-in-one
one step self etch→ universal
self etch + primer (then dry) + bond
when you want to protect adjacent teeth from etching, what can you use
teflon tape (but don’t like at school)
why use teflon tape to protect adjacent teeth from etching
thin, non-sticky and chemically inert
smooth surface and very low friction w surface
resistant to water and etchant
soft, easy to manipulate and shape on/between surfaces
cheap and safe
