High-Risk Newborn Care: Gestational Age & Development Terms CH. 29
1/56
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
57 Terms
Which infant is a likely candidate for receiving exogenous surfactant?
a. An infant with hypoglycemia born to a diabetic mother
b. A preterm infant with respiratory distress syndrome at birth
c. A preterm infant with a soft cranium who is at risk for cranial molding
d. An infant at risk for inborn errors of metabolism, such as galactosemia
b. A preterm infant with respiratory distress syndrome at birth
Exogenous surfactant helps maintain lung expansion in infants with respiratiory distress. Oral glucose is used for an infant with hypoglycemia at birth. A preterm infant is placed on a waterbed or a gel mattress to minimize the risk for cranial molding. Galascosemia is managed by eliminating lactose-containing food and milk from the infant’s diet. Pg 640
Necrotizing enterocolitis (NEC) is an inflammatory disease of the gastrointestinal mucosa. The signs of NEC are nonspecific. What are some generalized signs the nurse might see?
a. Hypertonic, tachycardia, and metabolic alkalosis
b. Hypertension, absence of apnea, and ruddy skin color
c. Abdominal distension, temperature instability, and grossly bloody stools
d. Scaphoid abdomen, no residual with feedings, and increased urinary output
c. Abdominal distension, temperature instability, and grossly bloody stools
Generalized signs of NEC include: decreased activity, hypotonia, pallor, recurrent apnea and bradycardia, decreased O2 sat values, respiratory distress, metabolic acidosis, oliguria, hypotension, decreased perfusion, temperature instability, cyanosis, abdominal distinction, residual gastric aspirates, vomiting, grossly bloody stools, abdominal tenderness, and erythema of the abdominal wall. The infant may display hypotonia, bradycardia, and metabolic acidosis. Hypotension, apnea, and pallor are signs of NEC. Abdominal distinction, residual gastric aspirates, and oliguria are sings of NEC. Pg 641
An infant weighing 4.1 kg was born 2 hours ago at 37 weeks of gestation. The infant appears chubby with a flushed complexion and is very tremulous. What are the tremors most likely the result of?
a. Seizures
b. Birth injury
c. Hypocalcemia
d. Hypoglycemia
d. Hypoglycemia
This infant is macroscopic and at risk for hypoglycemia. The tremors are jitteriness that is associated with hypoglycemia. Signs of hypoglycemia include jitteriness, apnea, tachypnea, and cyanosis. Tremors are not associated with seizures, birth injury, or hypocalcemia. Pg 643
Which vital sign will the nurse plan to assess frequently to decrease the risk for retinopathy of prematurity (ROP) for a preterm infant receiving oxygen?
a. Heart rate
b. Blood pressure
c. Pulse oximetry
d. Respiratory rate
c. Pulse oximetry
Retinopathy of prematurity (ROP) is an eye problem that can cause blindness and is caused by abnormal growth of blood vessels in the retina in premature infants. When a baby is born prematurely, the retinal blood vessels are not full grown and can grow abnormally. When ROP is severe, it can cause the retina to pull away or detach from the wall of the eye and possibly cause blindness. Babies born at a weight of 1500 grams or less and born before 31 weeks gestation are at highest risk.
Fluctuating blood oxygen levels are associated with ROP; therefore the nurse will frequently assess the infant’s pulse oximetry readings for all infants receiving oxygen. Pg 641
A preterm infant is on a respirator with intravenous lines and much equipment around her when her parents come to visit for the first time. What action by the nurse is most important?
a. Suggest that the parents visit for only a short time to reduce their anxieties.
b. Reassure the parents that the baby is progressing well.
c. Encourage the parents to touch her.
d. Discuss the care they will give her when she goes home.
c. Encourage the parents to touch her.
Physical contact with the infant is important to establish early bonding. The nurse as the support person and teacher is responsible for shaping the environment and making the care giving responsive to the needs of both the parents and the infant. The nurse should encourage the parents to touch their baby and show them how to do so safely. Bonding needs to occur, and this can be fostered by encouraging the parents to spend time with the infant. It is important to keep the parents informed about the infant‘s progression, but the nurse needs to be honest with the explanations. Discussing home care needs to wait until the parents are ready and discharge is closer with known needs.
Which cue describes the risk factor associated with the delivery of an infant large for gestational age? Select all that apply.
a.Precipitous labor
b. Cesarean section
c. Shoulder dystocia
d. Cephalohematoma
e. Instrumental delivery
b. Cesarean section
c. Shoulder dystocia
d. Cephalohematoma
e. Instrumental delivery
Large for gestational age infants weigh above the 90th percentile for gestational age on the intrauterine growth charts. Infants who are large for gestational age have an increased risk for cesarean delivery, shoulder dystopia, cephalohematoma, and instrumental delivery. The large for gestational age infant is more likely to go through a long labor. Pg 643
Which cue is associated with the asymmetric growth of an infant small for gestational age?
a. Small head
b. Short length
c. Sunken abdomen
d. Underdeveloped appearance
c. Sunken abdomen
A sunken abdomen is a clinical finding associated with the infant who is small for gestational age and asymmetrical. An infant small for gestational age with asymmetric growth has a normal head size that seems large for the rest of the body. The length is normal, and the appearance is not underdeveloped. The appearance is one of think wasted, dry, loose skin; a thin cord; and a facial appearance of being elderly. Pg 642-643
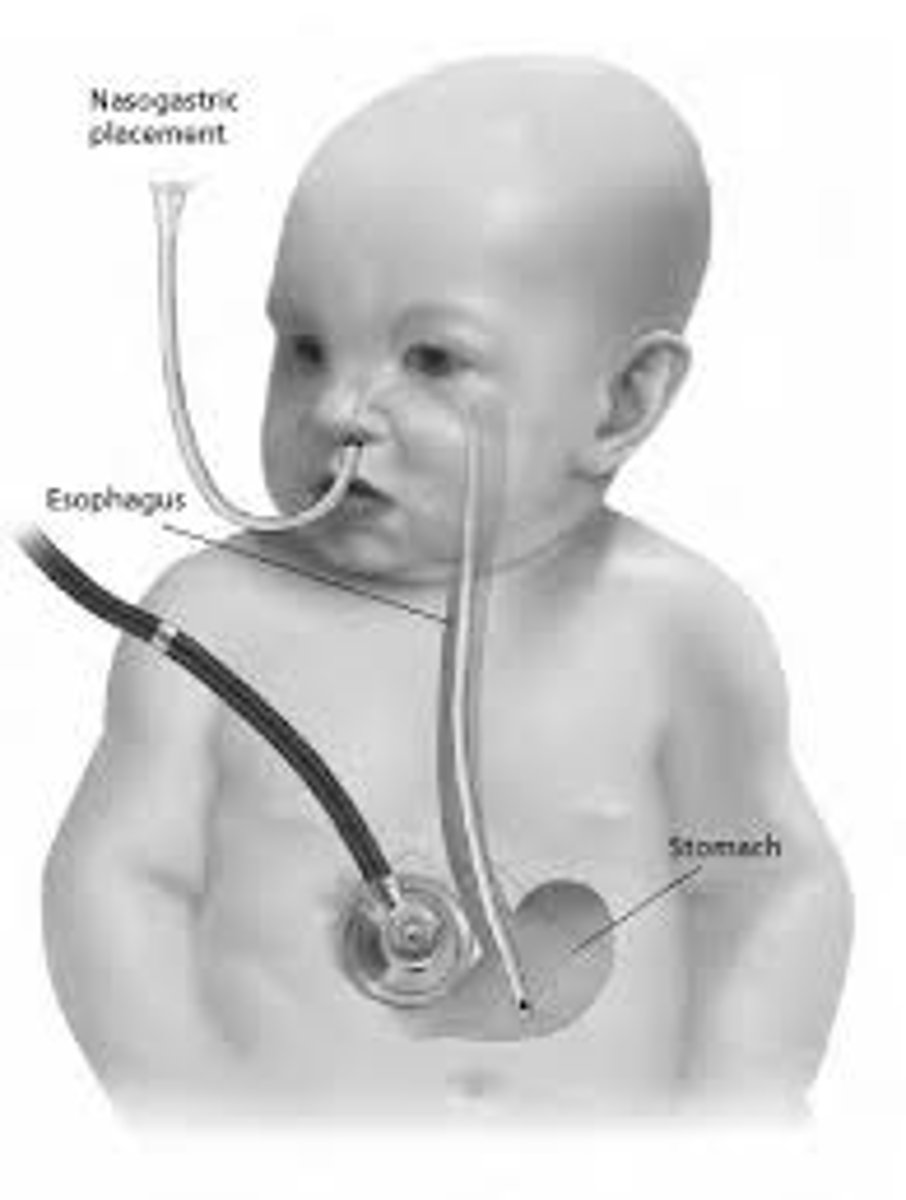
Which preterm infant should receive gavage feedings instead of a bottle?
a. Sometimes gags when a feeding tube is inserted
b. Is unable to coordinate sucking and swallowing
c. Sucks on a pacifier during gavage feedings
d. Has an axillary temperature of 98.4° F, an apical pulse of 149 beats/min, and
respirations of 54 breaths/min
b. Is unable to coordinate sucking and swallowing
An infant who cannot coordinate sucking, swallowing, and breathing should receive gavage feedings. The other infants are ready for bottle feedings.
Which factors describe the etiology associated with a small for gestational age infant? Select all that apply.
a. Smoking
b. Maternal age
c. Placenta previa
d. Nutritional status
e. Maternal hypertension
a. Smoking
c. Placenta previa
d. Nutritional status
e. Maternal hypertension
Smoking, placenta previa, and maternal hypertension all interfere with the placenta’s function. The poor placental function increases the risk for SGA. The maternal nutritional status affects the growth of the fetus. Severe maternal malnutrition can impair fetal growth resulting in an infant that is SGA. Pg 642-643
Which complication will the nurse prepare to address for an infant of 39 weeks of gestation in the 8th percentile on the growth chart? Select all that apply.
a. Hypothermia
b. Hypoglycemia
c. Hyperbilirubinemia
d. Immature suck reflex
e. Respiratory distress syndrome
a. Hypothermia
b. Hypoglycemia
Infants below the 10th percentile on the growth chart are considered SGA (small for gestational age). Hypothermia is a risk because the white and brown fat stores have been used to survive in utero. Hypoglycemia occurs because of inadequate storage of glycogen in the liver. Pg. 642- 643
Which action will the nurse include in the plan of care during the first 24 hours after birth for an infant with postmaturity syndrome? Select all that apply.
a. Early feeding
b. Skin to skin contact
c. Increased frequency in feeding
d. Decreased environmental stimuli
e. Supplementation with formula
a. Early feeding
b. Skin to skin contact
c. Increased frequency in feeding
The normal length of pregnancy is 37 to 41 weeks. Early term is from 37 weeks to 38 weeks and 6 days. Full term is 39 weeks to 40 weeks and 6 days. Late term is 41 weeks to 41 weeks and 6 days. Postmaturity (dysmaturity) describes babies born after 42 weeks.
Early and increase frequency of feeding prevents hypoglycemia. Skin to skin contact will help regulate the infants temp and promote bonding. Pg. 641- 642
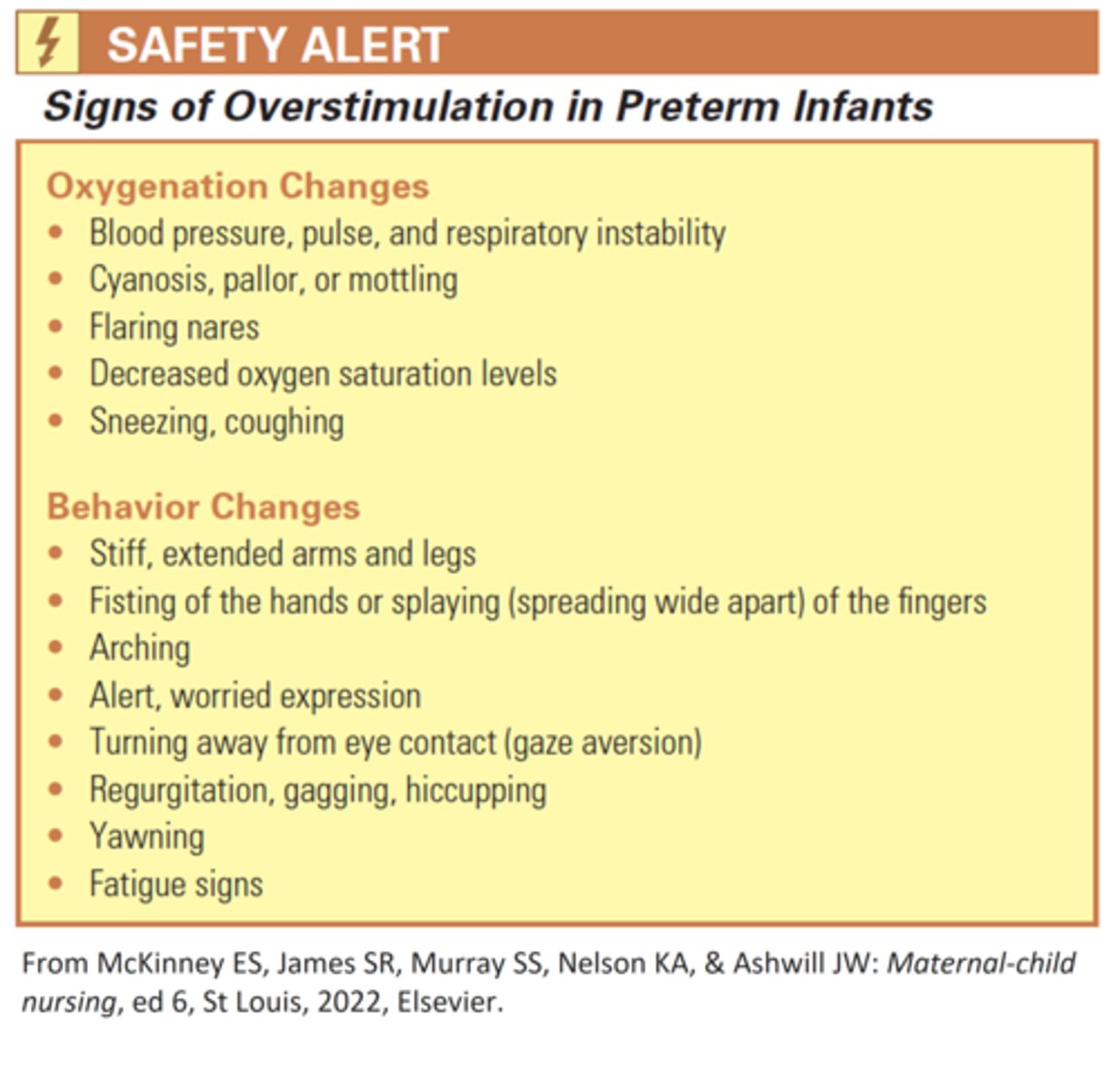
Overstimulation may cause increased oxygen use in a preterm infant. Which nursing intervention helps to avoid this problem?
a. Group all care activities together to provide long periods of rest.
b. While giving your report to the next nurse, stand in front of the incubator and talk softly about how the infant responds to stimulation.
c. Teach the parents signs of overstimulation, such as turning the face away or stiffening and extending the extremities and fingers
d. Keep charts on top of the incubator so the nurses can write on them there.
c. Teach the parents signs of overstimulation, such as turning the face away or stiffening and extending the extremities and fingers
Parents should be taught these signs of overstimulation so they will learn to adapt their care to the needs of their infant. This may understimulate the infant during those long periods and overtire the infant during the procedures. Talking in front of the incubator could overstimulate the baby. Placing objects on top of the incubator or using it as a writing surface increases the noise inside.
Which complication will the nurse plan to monitor carefully in a post term infant? Select all that apply.
a. Sepsis
b. Hypothermia
c. Hypoglycemia
d. Transient tachypnea
e. Respiratory distress syndrome
b. Hypothermia
c. Hypoglycemia
A post term infant is at risk for hypothermia because of a loss of subcutaneous tissue.
Pg 641- 642
Which cue would the nurse be concerned about when initiating a feeding for an infant during the immediate recovery period from necrotizing enterocolitis?
a. Water stools
b. Fluid imbalance
c. Feeding intolerance
d. Electrolyte imbalance
e. Decreased abdominal girth
a. Water stools
b. Fluid imbalance
c. Feeding intolerance
d. Electrolyte imbalance
During the recovery period from NEC, the nurse must manage pain and observe for feeding intolerance. I and O are essential, as third space fluid loss occurs when fluid moves from the intravascular space to the extra vascular space. The third spacing can create a fluid and electolyte imbalance. A feeding intolerance indicates the NEC is not resolved. Pg. 641
What action describes the therapeutic management of NEC? Select all that apply.
a. Administer antibiotics
b. Initiate gastric suction
c. Provide parenteral nutrition
d. Prepare the infant for an ostomy
e. Decrease volume of enteral feedings
a. Administer antibiotics
b. Initiate gastric suction
c. Provide parenteral nutrition
Therapeutic management of NEC includes the administration of antibiotics, gastric suction, and parenteral nutrition. An ostomy is performed if necrotic bowel is present. Parenteral feedings will be initiated to allow the gastrointestinal tract to recover. Pg 641
A nurse is caring for a preterm baby who weighs 4.8 pounds. What assessment finding indicates the baby is dehydrated?
a. Urine output of 3.3 mL/hour
b. Urine specific gravity of 1.001
c. Low serum sodium
d. Weight gain of 43 g in one day
a. Urine output of 3.3 mL/hour
This baby weighs 2.18 kg (4.8lbs/2.2 = 2.18kg)
Dehydration is noted with a urine output of <2 mL/kg/hour.
A urine output of 3.3 mL is 1.5 mL/kg/hour and so indicates dehydration. (3.3ml output/ 2.18kg= 1.5 ml output per kg per hour).
The dilute urine specific gravity indicates overhydration as does the low serum sodium. The weight gain is normal (15 to 20 g/kg/day).
The nurse is observing a parent holding a preterm infant. The infant is sneezing, yawning, and extending the arms and legs. What action by the nurse is best?
a. Cover the infant with a warmed blanket.
b. Encourage the parent to do kangaroo care.
c. Encourage the parent to place the infant back in the warmer
d. Have the parent fold the infant's arms across the chest.
c. Encourage the parent to place the infant back in the warmer
These are signs that the preterm infant is overstimulated. The parent should place the infant back in her warmer, and the nurse can turn down the lights and limit noise. The other suggestions will not help decrease stimulation.
Which effect describes the benefit of trophic feedings for an infant of 34 weeks of gestation?
a. Accelerates weight gain
b. Prevents excessive fluid loss
c. Decreases feeding intolerance
d. Facilitates the absorption of electrolytes
c. Decreases feeding intolerance
Trophic feeding is the practice of feeding minute volumes of enteral feeds in order to stimulate the development of the immature gastrointestinal tract of the preterm infant.
Trophic feedings decrease feeding intolerance, promote maturation of the intestinal tract and motility, and aid gastric hormone production. Overall, feeding tolerance and weight gain are improved, and infants achieve full enteral feedings earlier if given Trophic feedings. Pg 632
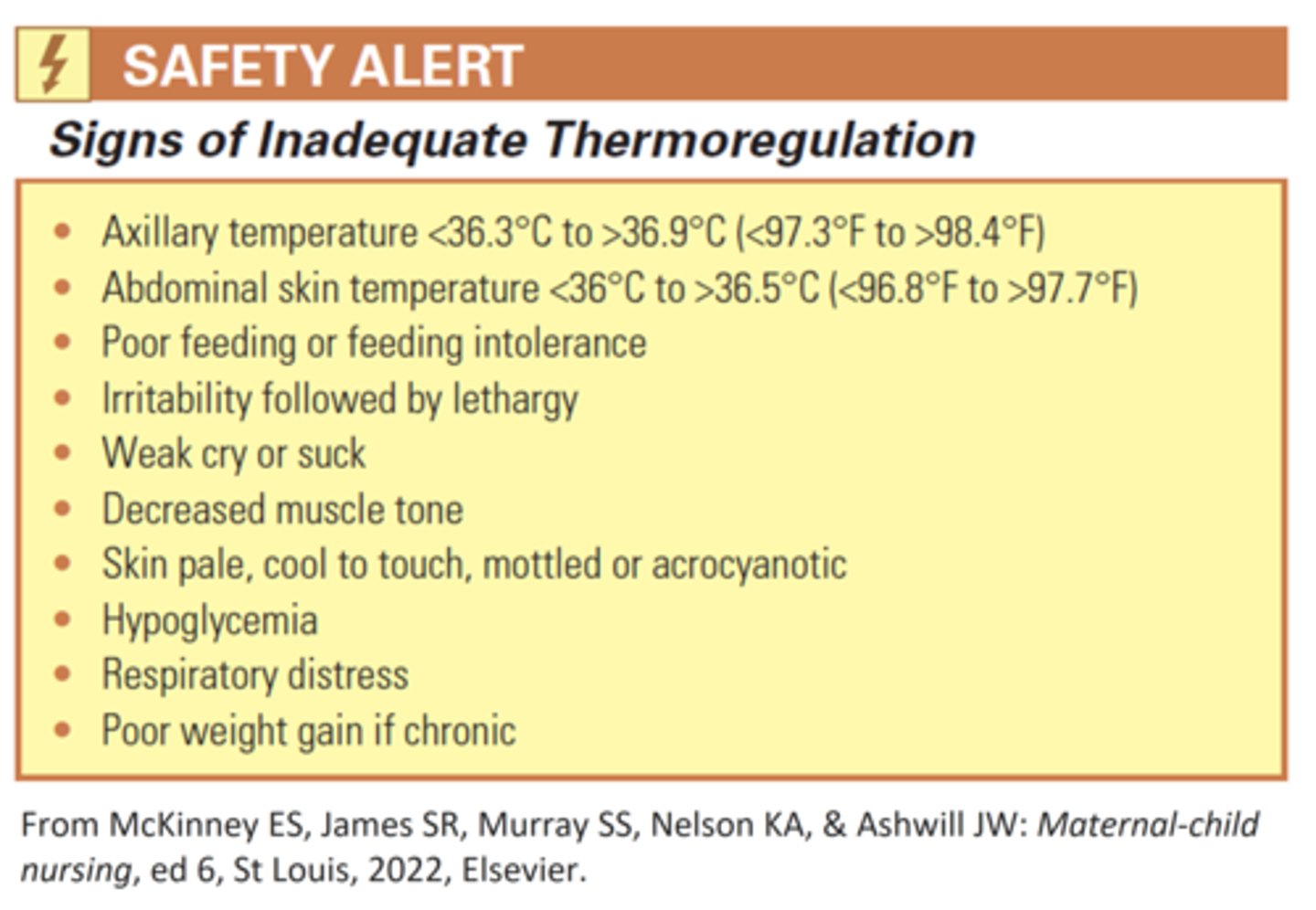
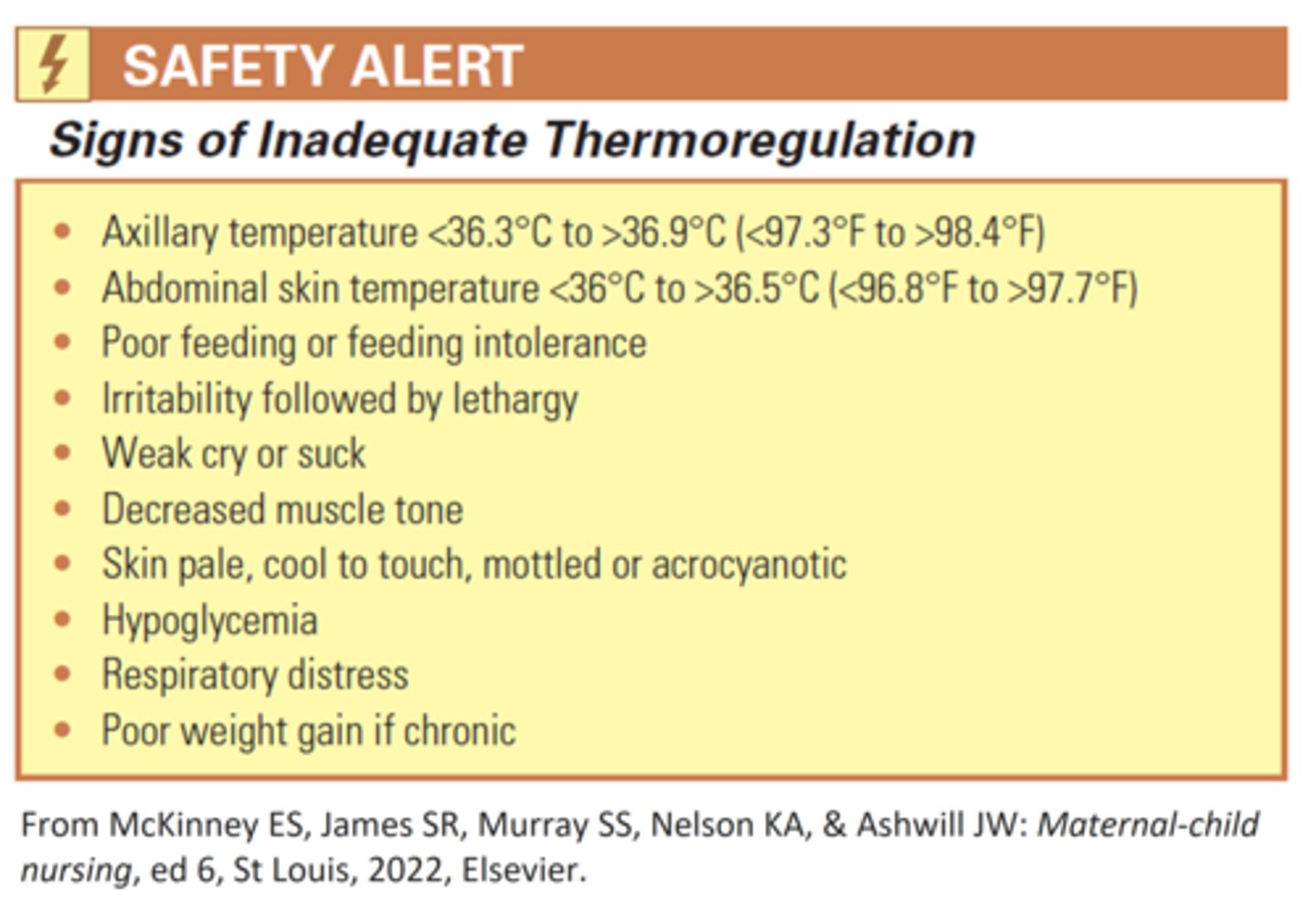
A nurse is caring for a preterm infant who has a weak cry and is irritable. What action by the nurse is best?
a. Assess the infant for pain.
b. Take the infant's temperature.
c. Obtain a bedside glucose reading.
d. Reduce stimulation in the environment.
b. Take the infant's temperature.
These are signs of inadequate thermoregulation. The nurse should assess the infant's temperature first. The other actions do not address thermoregulation.
The nurse tells the nursing student that late preterm infants are at increased risk for which of the following problems? (Select all that apply.)
a. Problems with thermoregulation
b. Cardiac distress
c. Hyperbilirubinemia
d. Sepsis
e. Hyperglycemia
a. Problems with thermoregulation
c. Hyperbilirubinemia
d. Sepsis
Problems with thermoregulation, hyperbilirubinemia, and sepsis are common with late preterm infants. They typically have respiratory distress and hypoglycemia.
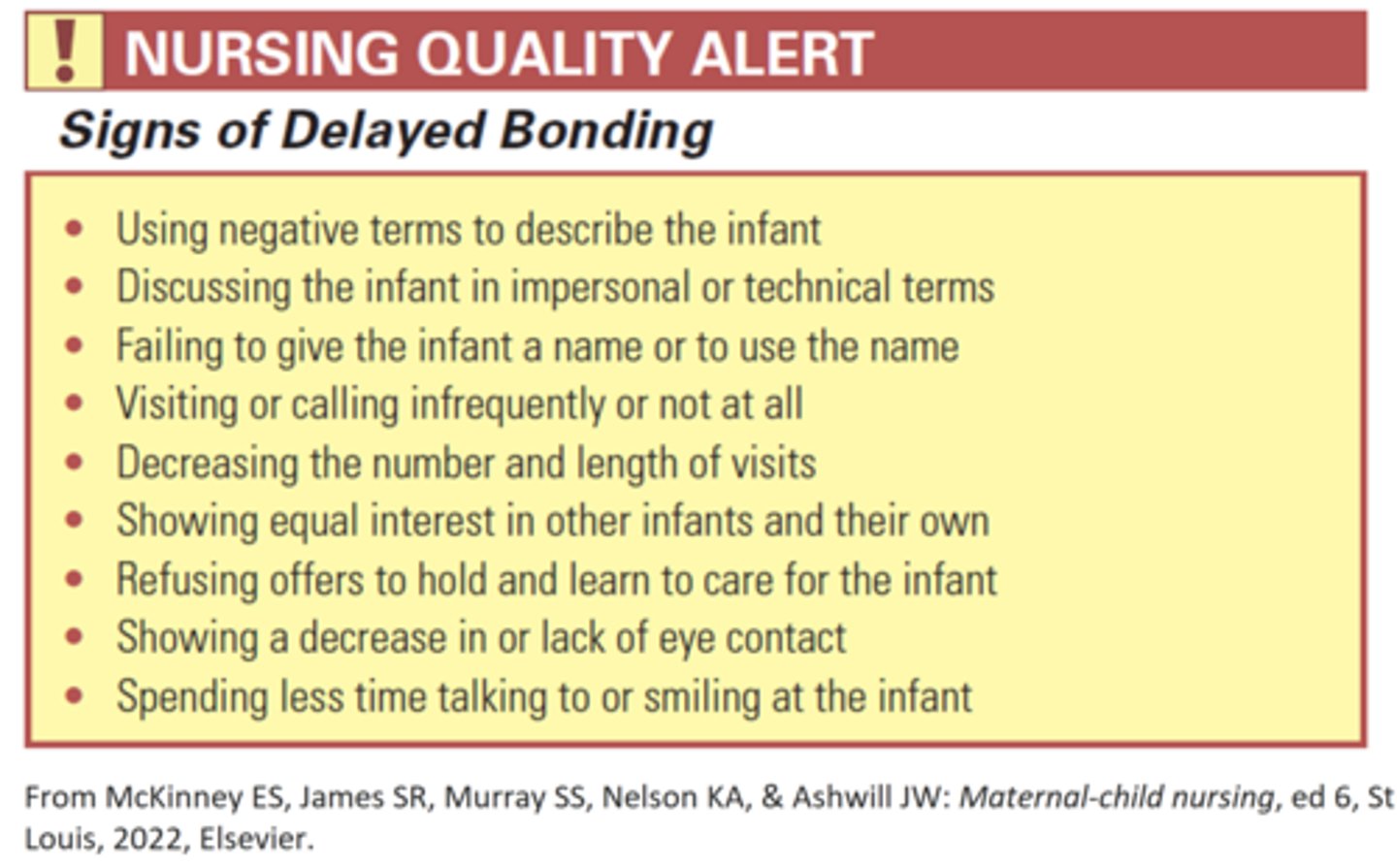
Which cue will the nurse look for to indicate delayed bonding when monitoring the parents of a preterm infant? Select all that apply.
a. Frequency of visits
b. Interest in the neonatal care unit
c. Receptivity to learning infant care
d. Verbal communication with the infant
e. Nonverbal interaction with the infant
a. Frequency of visits
c. Receptivity to learning infant care
d. Verbal communication with the infant
e. Nonverbal interaction with the infant
Pg 636
For which cue of intraventricular hemorrhage would the nurse monitor in a preterm infant?
a. Lethargy
b. Tachypnea
c. Hypertonicity
d. High pitched cry
e. Elevated pain score
a. Lethargy
d. High pitched cry
Intraventricular hemorrhage, also known as intraventricular bleeding, is a bleeding into the brain's ventricular system, where the cerebrospinal fluid is produced and circulates the rough towards the subarachnoid space.
Lethargy and a high-pitched cry are clinical findings associated with IVH. The symptoms occur as a result of increased cranial pressure. Apnea is a symptom associated with IVH. Pain and stress contribute to the increased risk for IVH but are not clinical symptoms resulting from IVH.
Pg 640- 641
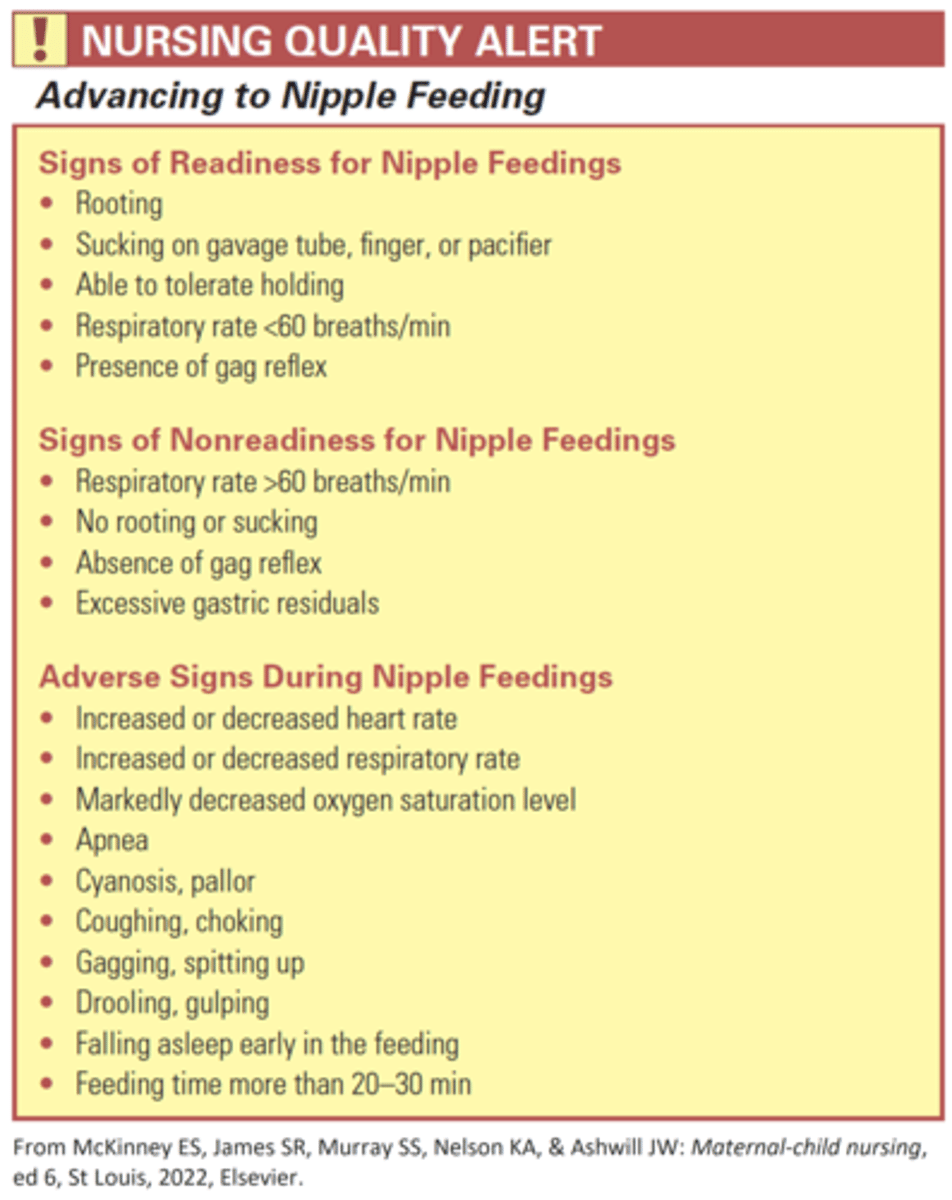
For which cue would the nurse stop the oral feeding of a 16 hour old late preterm infant? Select all that apply.
a. Acrocyanosis
b. Heart rate of 156
c. Respiratory rate of 62
d. Periodic cessation of sucking
e. Cessation of breathing for 23 seconds
c. Respiratory rate of 62
e. Cessation of breathing for 23 seconds
The nurse will stop the feeding if tachypnea or apnea is present.
Normal RR 40- 60.
A RR above 60 is considered tachypnea. 23 seconds of cessation of breathing is considered apnea. Acrocyanosis is a common finding for an infant under 24 hours of age.
Normal HR is 120- 160.
A HR of 156 is an acceptable finding. Pg. 632- 634
Which action will the nurse take when attempting to feed a sleepy preterm infant orally?
a. Stimulate the rooting reflex
b. Initiate nonnutritive sucking
c. Position the infant at a 60 degree angle
d. Hold the bottle so the infant can suck slowly
b. Initiate nonnutritive sucking
Initiation of nonnutritive sucking helps alert the infant to prepare for feeding. Stimulating the rooting reflex is a neurological assessment and part of an evaluation for the readiness for an infant to advance to nipple feeding. Positioning at 60 degrees is an intervention to help control flow of formula. Holding the bottle so the infant can suck slowly allows the infant to regulate breathing.
Pg 632
For which complications will the nurse monitor a preterm infant receiving continuous gavage feedings?
a. Infection
b. Aspiration
c. Weight loss
d. Feeding intolerance
e. Uncoordinated suck reflex
a. Infection
b. Aspiration
c. Weight loss
d. Feeding intolerance
Infection because bacterial counts in milk may become too high. Aspiration because they may be left unattended at times during a feeding. Weight loss because fats tend to adhere to the tubing during the continuous feeding. Pg 632
Which action would the nurse take after observing a feeding preterm infant pull away from the breast and begin arching and yawning?
a. Garage feed the infant
b. Provide a period of rest
c. Rewrap the infant before reintroducing to the breast
d. Implement the use of a supplemental nursing system
b. Provide a period of rest
Arching and yawning are signs of overstimulation. Pg 630- 632
Which cue provides the most accurate information when evaluating the nutritional intake of a late preterm infant?
a. Weight
b. Vital signs
c. Elimination output
d. Observed feedings
c. Elimination output
Late preterm infants can have an immature suck and swallow reflex, shorter awake periods, and a tendency to fall asleep through or during feedings. Therefore, urine and stool output are monitored as indications of adequate intake. Pg. 628
Which action will the nurse take after reviewing the EHR (below) for a preterm infant?
History
Female infant, 31 weeks of gestation with respiratory distress syndrome. Surfactant replacement therapy and CPAP by mask initiated after birth.
Umbilical Artery Blood Gas
pH 7.37
PaCO, 36
Pa0, 56
Base excess -1
A. Prepare to intubate
B. Discontinue the continuous positive airway pressure (CPAP)
C. Continue with the plan of care
D. Notify the HCP
C. Continue with the plan of care
The umbilical artery blood gas results are within acceptable parameters; therefore the nurse will anticipate continuing with the plan of care. The CPAP is providing adequate respiratory support for the infant with respiratory distress syndrome and will not be abruptly discontinued. Pg 626
The nurse is preparing discharge information for the parents of an infant born at 32 weeks of gestation. Based on the gestational age of birth, calculate developmental age the nurse will provide education for.
_____ months
2 months
It is important to help the parents understand the developmental or corrected age of their infant. Understanding the corrected age will help form realistic expectations of the infants developmental tasks, such as crawling and walking later than full term infants. Therefore the nurse will reinforce with the parents the allowance for the extra weeks for the infant to obtain developmental milestones.
To calculate the corrected age, the nurse uses the following formula:
Chronologic age- weeks or months of prematurity= corrected age.
40- 32= 8 weeks= 2 months. Pg 625
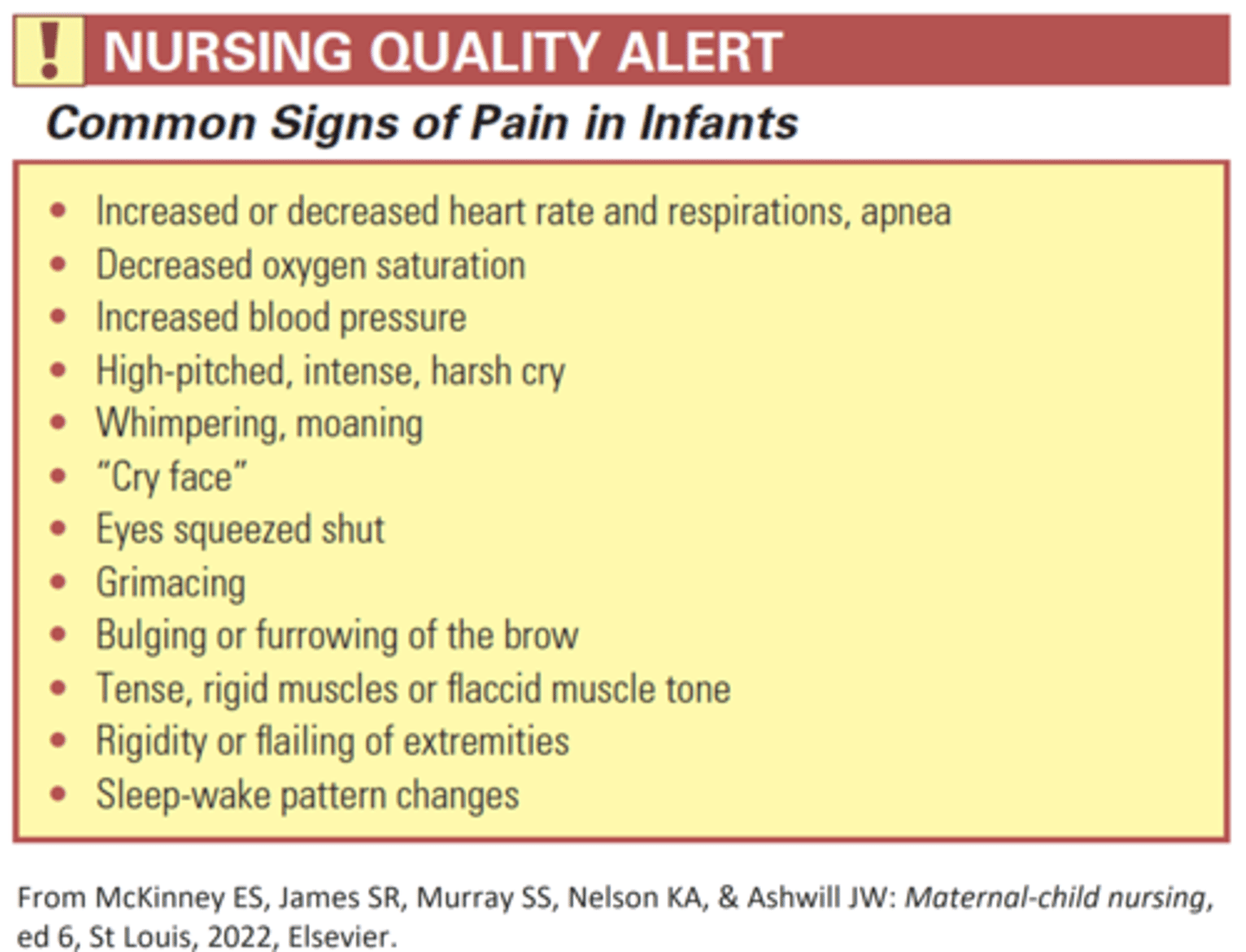
Which cue for an infant of 32 weeks of gestation will the nurse determine requires intervention for pain management?
a. Limp extremities
b. BP 62/44 mm Hg
c. Predictably SpO2 sat 90%
d. Cessation of breathing for 10 seconds
b. BP 62/44 mm Hg
A BP of 62/44 is a BP anticipated for a term infant, not a preterm infant. An elevated BP is a common sign of pain in infants.
Blood pressure rises as the baby grows. The average blood pressure in a newborn is 64/41. The average blood pressure in a child 1 month through 2 years old is 95/58.
Which action will the nurse take when caring for an infant at 30 weeks of gestation mechanically ventilated with a grade 3 intraventricular hemorrhage?
a. Monitor arterial blood gases
b. Position the infant's head midline
c. Prepare the infant for a spinal tap
d. Decrease the pressure of suctioning
e. Prepare the infant for placement of a shunt
a. Monitor arterial blood gases
b. Position the infant's head midline
Careful management of an infant with IVH includes ensuring that the ventilation is managed correctly to avoid hypocapnia. Hypocapnia and hypoxia can cause further neurological injury. The nurse will ensure the infants head is midline to promote neurocirculation and reduce the risk of increasing the cranial pressure. Pg 640- 641
Based on a review of the EHR, which action would the nurse take?
History
Male infant, 29 weeks of gestation delivered by emergency cesarean section because of a placental abruption. The infant is currently mechanically ventilated. After receiving a red blood cell transfusion, the nurse notes the hematocrit level remains unchanged.
A. Continue the plan of care
b. Increase intravenous infusion
c. Notify the HCP
d. Prepare for an additional transfusion of RBCs
c. Notify the HCP
The infant is at risk for IVH. IVH results from the rupture of the fragile blood vessels in the germinal matrix, located around the brain’s ventricles. IVH is associated with decreased BP and respiratory distress requiring mechanical ventilation. Rapid blood volume expansion is also associated with a risk for IVH. Because the infant’s risk factors and the failure of Hct to increase after the RBC transfusion, the infant may be experiencing a low grade IVH. Because a grade 1 IVH may be asymptomatic, the infant requires further evaluation by ultrasound. Pg. 640- 641
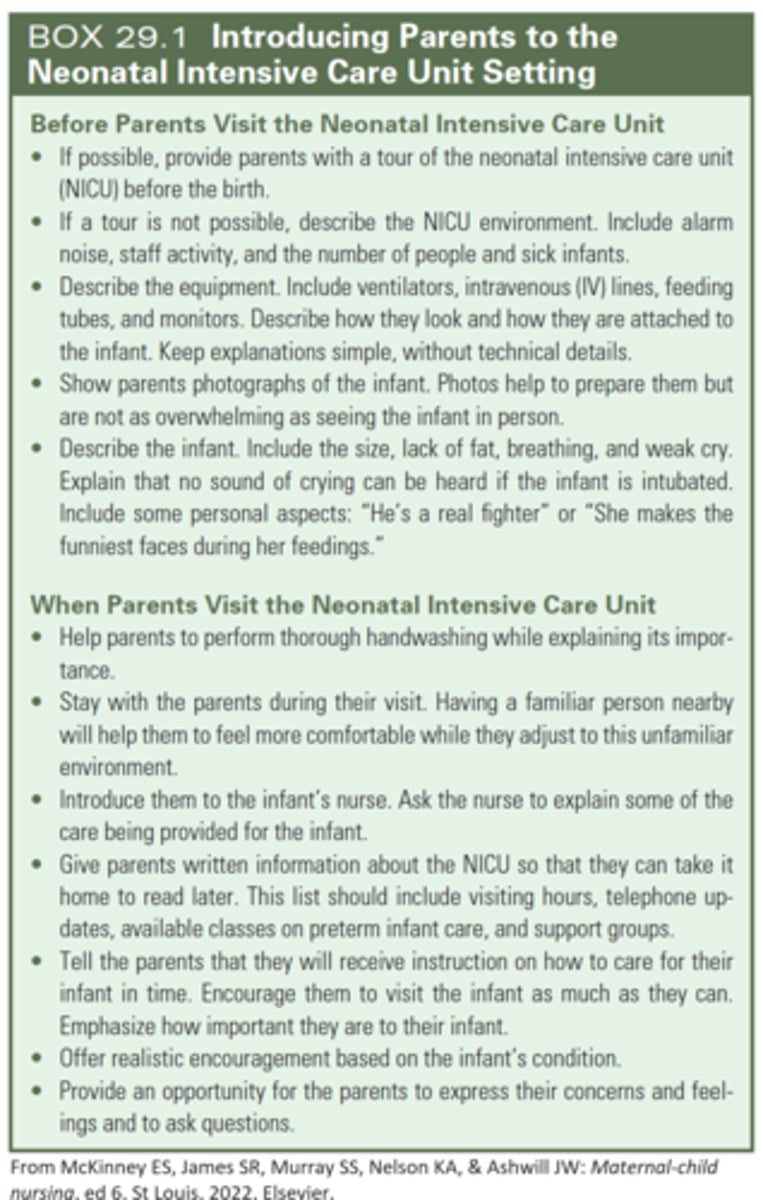
Introducing Parents to the NICU setting
Which action will the nurse take after assessing the infant for readiness for nipple feeding?
History
2-day old male infant 35 1/7 weeks of gestation, weight 2580 g
Assessment
Residual from gavage feeding 13 mL
Respirations: 42 breaths per minute
Heart rate: 136 bpm
Preductal SpO2 saturation 90%
A. Evaluate the gag reflex
b. Initiate a nipple feeding
c. Continue garage feedings
d. Notify the HCP
d. Notify the HCP
The residual measures more than 2 to 4 mL/kg. Because of the excessive gastric residual, the infant is not ready for a nipple feeding, and the information would be reported to the HCP.
2580g= 2.580kg; 2.580kg X 4mL= 10mL
Excessive residuals indicate that the formula amount, type, or flow rate needs to be changed or that complications may have occurred; therefore the nurse would not continue gavage feedings. Pg 632- 633
Calculate the maximum amount of residual feeding for a preterm infant weighing 2018g receiving intermittent gavage feedings. Record as a whole number in mL.
8mL
2018g= 2.018kg
2.018kg X 4mL= 8.072
rounded to nearest whole= 8mL
EVOLVE Questions
A preterm infant with respiratory difficulties should be placed in what position to facilitate drainage?
a. Fowler's
b. Trendelenburg
c. Supine
d. Prone
d. Prone
The prone position and side-lying position for a preterm infant can facilitate drainage of respiratory secretions and regurgitated feedings. Prone position also increases oxygenation and lung compliance and reduces energy expenditure.
The most important reason to protect the preterm infant from cold stress is that:
a. it could make respiratory distress syndrome worse.
b. shivering to produce heat may use up too many calories
c. hyperglycemia may develop
d. polycythemia may develop
a. it could make respiratory distress syndrome worse.
Cold stress may interfere with the production of surfactant, making respiratory distress syndrome worse. Other complications of heat loss include hypoglycemia, metabolic acidosis, pulmonary vasoconstriction, impaired surfactant production, and hyperbilirubinemia. Preterm infants do not shiver to produce heat. Polycythemia, can develop from hypoxia before birth, not cold stress.
Which is true about newborns classified as small for gestational age (SGA)?
a. They are below the 10th percentile on gestational growth charts.
b. They weigh less than 2,500 grams.
c. Placental malfunction is the only recognized cause of this condition
d. They are born before 38 weeks of gestation
a. They are below the 10th percentile on gestational growth charts.
SGA infants are defined as below the 10th percentile in growth compared with other infants of the same gestational age. Many risk factors may cause an infant to be SGA.
What nursing action is especially important for a small for gestational age (SGA) newborn?
a. observe for and prevent dehydration
b. observe for respiratory distress syndrome
c. promote bonding
d. prevent hypoglycemia with early and frequent feedings.
d. prevent hypoglycemia with early and frequent feedings.
SGA infants have inadequate glycogen storage in the liver and are subject to hypoglycemia. Respiratory distress syndrome is seen in preterm infants. Dehydration and promoting bonding are a concern for all infants and not specific for SGA.
What are appropriate nursing measures to help relieve a preterm infant’s pain during a painful procedure (Select all that apply.)
a. keeping a hand near the face to be used for sucking
b. administering a prescribed sedative
c. use of a pacifier dipped in sucrose
d. swaddling the infant
a. keeping a hand near the face to be used for sucking
c. use of a pacifier dipped in sucrose
d. swaddling the infant
Comfort measures such as swaddling, using a pacifier dipped in sucrose, and keeping a hand near the face to be used for sucking help the infant cope with short-term, mild pain and reduce agitation. Comfort measures alone are not enough for moderate to severe pain. The nurse should discuss the infant's pain with the primary care provider to ensure that medications are available when necessary. Sedatives do not help with pain relief.
What is most helpful in preventing premature birth?
a. High socioeconomic status
b. Adequate prenatal care
c. Transitional Assistance to Needy Families
d. Women, Infants, and Children nutritional program
ANS: B. Adequate prenatal care
Prenatal care is vital in identifying possible problems. Women from higher economic status
are more likely to seek adequate prenatal care, but it is the care that is most helpful.
Government programs help with specific needs of the pregnant woman, but adequate care
is more important.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 620 OBJ: Nursing Process: Assessment
MSC: Client Needs: Health Promotion and Maintenan
Compared to the term infant, the preterm infant has
a. few blood vessels visible though the skin.
b. more subcutaneous fat.
c. well-developed flexor muscles.
d. greater surface area in proportion to weight
ANS: D. greater surface area in proportion to weight
Preterm infants have greater surface area in proportion to their weight. They often have
visible blood vessels because their skin is thin and they have less fat. More fat and
well-developed flexor muscles are characteristic of a more mature infant.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 623 OBJ: Nursing Process: Assessment
MSC: Client Needs: Physiologic Integrit
Decreased surfactant production in the preterm lung is a problem because surfactant
A. causes increased permeability of the alveoli.
B. provides transportation for oxygen to enter the blood supply.
C. keeps the alveoli open during expiration.
D. dilates the bronchioles, decreasing airway resistance.
C. keeps the alveoli open during expiration.
Surfactant prevents the alveoli from collapsing each time the infant exhales, thus
reducing the work of breathing. It does not cause increased permeability, provide
transportation of oxygen or dilate the bronchioles.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 635 OBJ: Nursing Process: Assessment
A nurse is caring for a late preterm infant. What action by the nurse is inconsistent with best
practice to prevent cold stress?
a. Wean the infant directly to an open crib.
b. Check temperature every 3 to 4 hours.
c. Encourage kangaroo care.
d. Place infant on a radiant warmer.
ANS: A. Wean the infant directly to an open crib.
Weaning to an open crib takes many steps and is not done directly because of the risk of
cold stress. The other actions help prevent cold stress.
PTS: 1 DIF: Cognitive Level: Application/Applying
REF: pp. 622-623 OBJ: Nursing Process: Implementation
MSC: Client Needs: Physiologic Integrity
A premature infant never seems to sleep longer than an hour at a time. Each time a light
is turned on, an incubator closes, or people talk near her crib, she wakes up and cries
inconsolably until held. The correct nursing diagnosis is ineffective coping related to
a. severe immaturity.
b. environmental stress.
c. physiologic distress.
d. behavioral responses.
ANS: B. environmental stress.
This nursing diagnosis is the most appropriate for this infant. Light and sound are known
adverse stimuli that add to an already stressed premature infant. The nurse must monitor
the environment closely for sources of overstimulation. The other diagnoses do not
recognize that fact.
PTS: 1 DIF: Cognitive Level: Application/Applying
REF: p. 626 OBJ: Nursing Process: Diagnosis
MSC: Client Needs: Safe and Effective Care Environme
In caring for the preterm infant, what complication is thought to be a result of high
arterial blood oxygen level?
a. Necrotizing enterocolitis (NEC)
b. Retinopathy of prematurity (ROP)
c. Bronchopulmonary dysplasia (BPD)
d. Intraventricular hemorrhage (IVH)
ANS: B. Retinopathy of prematurity (ROP)
ROP is thought to occur as a result of high levels of oxygen in the blood. NEC is due to the
interference of blood supply to the intestinal mucosa. Necrotic lesions occur at that site.
BPD is caused by the use of positive pressure ventilation against the immature lung tissue.
IVH is due to rupture of the fragile blood vessels in the ventricles of the brain. It is most
often associated with hypoxic injury, increased blood pressure, and fluctuating cerebral
blood flow.
PTS: 1 DIF: Cognitive Level: Comprehension/Understanding
With regard to eventual discharge of the high-risk newborn or transfer to a different facility,
nurses and families should be aware that
a. b. infants will stay in the NICU until they are ready to go home.
once discharged to home, the high-risk infant should be treated like any healthy
term newborn.
c. d. parents of high-risk infants need special support and detailed contact information.
if a high-risk infant and mother need transfer to a specialized regional center, it
is better to wait until after birth and the infant is stabilized.
ANS: C. parents of high-risk infants need special support and detailed contact information.
High-risk infants can cause profound parental stress and emotional turmoil. Parents need
support, special teaching, and quick access to various resources available to help them care
for their baby. Parents and their high-risk infant should get to spend a night or two in a
predischarge room, where care for the infant is provided away from the NICU. Just because
high-risk infants are discharged does not mean they are normal, healthy babies. Follow-up
by specialized practitioners is essential. Ideally, the mother and baby are transported with
the fetus in utero; this reduces neonatal morbidity and mortality.
PTS:
OBJ:
1 DIF: Cognitive Level: Comprehension REF: p. 634
Nursing Process: Planning MSC: Client Needs: Psychosocial Integrit
Which combination of expressing pain could be demonstrated in a neonate?
A. Low-pitched crying, tachycardia, eyelids open wide
B. Cry face, flaccid limbs, closed mouth
C. High-pitched, shrill cry, withdrawal, change in heart rate
D. Cry face, eye squeeze, increase in blood pressure
ANS: D. Cry face, eye squeeze, increase in blood pressure
Cry face, eye squeeze, and an increase in blood pressure indicate pain. The other
manifestations are not those of pain in the neonate.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 624 OBJ: Nursing Process: Assessment
MSC: Client Needs: Health Promotion and Maintenance
A nurse is assessing an SGA infant with asymmetric intrauterine growth restriction. What
assessment finding correlates with this condition?
A. One side of the body appears slightly smaller than the other.
B. All body parts appear proportionate.
C. The head seems large compared with the rest of the body.
D. The extremities are disproportionate to the trunk.
ANS: C. The head seems large compared with the rest of the body.
In asymmetric intrauterine growth restriction, the head is normal in size but appears large
because the infant's body is long and thin due to lack of subcutaneous fat. The left and right
side growth should be symmetric. With asymmetric intrauterine growth restrictions, the
body appears smaller than normal compared to the head. The body parts are out of
proportion, with the body looking smaller than expected due to the lack of subcutaneous
fat. The body, arms, and legs have lost subcutaneous fat so they will look small compared
to the head.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 637 OBJ: Nursing Process: Assessment
MSC: Client Needs: Physiologic Inte
Which statement is true about large for gestational age (LGA) infants?
A. They weigh more than 3500 g.
B. They are above the 80th percentile on gestational growth charts.
C. They are prone to hypoglycemia, polycythemia, and birth injuries.
D. Postmaturity syndrome and fractured clavicles are the most
common complications.
ANS: C. They are prone to hypoglycemia, polycythemia, and birth injuries.
Hypoglycemia, polycythemia, and birth injuries are common in LGA infants. LGA infants
are determined by their weight compared to their age. They are above the 90th percentile
on the gestational growth charts. Birth injuries are a problem, but postmaturity syndrome is
not an expected complication with LGA infants.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 638 OBJ: Nursing Process: Assessment
MSC: Client Needs: Physiologic Integri
Of all the signs seen in infants with respiratory distress syndrome, which sign is
especially indicative of the syndrome?
a. Pulse more than 160 beats/min
b. Circumoral cyanosis
c. Grunting
d. Substernal retractions
ANS: C. Grunting
Grunting increases the pressure inside the alveoli to keep them open when surfactant is
insufficient. This is a characteristic and often early sign of RDS. The other assessments are
not specific to RDS.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 621 OBJ: Nursing Process: Assessment
MSC: Client Needs: Physiologic Integrity
While caring for the postterm infant, the nurse recognizes that the fetus may have
passed meconium prior to birth as a result of
a. hypoxia in utero.
b. NEC.
c. placental insufficiency.
d. rapid use of glycogen stor
ANS: A. hypoxia in utero.
When labor begins, poor oxygen reserves may cause fetal compromise. The fetus may pass
meconium as a result of hypoxia before or during labor, increasing the risk of meconium
aspiration. Meconium is not passed as a result of NEC, placental insufficiency, or rapid use
of glycogen stores.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 636 OBJ: Nursing Process: Assessment
MSC: Client Needs: Physiologic Integ
Which data should alert the nurse that the neonate is postmature?
a. Cracked, peeling skin
b. Short, chubby arms and legs
c. Presence of vernix caseosa
d. Presence of lanugo
ANS: A. Cracked, peeling skin
Loss of vernix caseosa, which protects the fetal skin in utero, may leave the skin
macerated and appearing cracked and peeling. Postmature infants usually have long, thin
arms and legs. Vernix caseosa decreases in the postmature infant. Absence of lanugo is
common in postmature infants.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering
REF: p. 637 OBJ: Nursing Process: Assessment
MSC: Client Needs: Health Promotion and Mainten
Because of the premature infant's decreased immune functioning, what nursing diagnosis
should the nurse include in a plan of care for a premature infant?
a. Delayed growth and development
b. Ineffective thermoregulation
c. Ineffective infant feeding pattern
d. Risk for infection
ANS: D. Risk for infection
The nurse needs to know that decreased immune functioning increases the risk for
infection. The other diagnoses are appropriate for the premature infant but not related
directly to immune function.
PTS: 1 DIF: Cognitive Level: Comprehension/Understanding
REF: p. 624 OBJ: Nursing Process: Planning
MSC: Client Needs: Physiologic Integrity
To maintain optimal thermoregulation for the premature infant, what action by the nurse is
most appropriate?
A. Bathe the infant once a day.
B. Put an undershirt on the infant in the incubator.
C. Assess the infant's hydration status.
D. Lightly clothe the infant under the radiant warmer.
ANS: B. Put an undershirt on the infant in the incubator.
Air currents around an unclothed infant will result in heat loss. Bathing causes
evaporative heat loss. Assessing hydration will not maintain thermoregulation. Clothing is
not worn when the infant is under a radiant warmer.
PTS: 1 DIF: Cognitive Level: Application/Applying
REF: p. 623 OBJ: Nursing Process: Implementation
MSC: Client Needs: Health Promotion and Maintenan
An important nursing factor during the care of the infant in the NICU is assessment for
signs of adequate parental attachment. The nurse must observe for signs that bonding is not
occurring as expected. These include (Select all that apply.)
a. using positive terms to describe the infant.
b. showing interest in other infants equal to that of their own.
c. naming the infant.
d. decreasing the number and length of visits.
e. refusing offers to hold and care for the infant.
ANS: B, D, E
b. showing interest in other infants equal to that of their own.'
d. decreasing the number and length of visits.
e. refusing offers to hold and care for the infant.
Bonding is not progressing as expected when parents show interest in other babies equal to
that of their own, decreasing the number and length of visits, and refusing to hold and help
care for the infant. Using positive terms to describe the baby and naming the infant are
signs that bonding is occurring.
PTS: 1 DIF: Cognitive Level: Knowledge/Remembering