l 1 anatomy endo
1/5
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
6 Terms
Q1: Mention the anatomical relations of the pituitary gland.
Answer:
Anterior relation: Tuberculum sellae and Anterior intercavernous sinus.
Posterior relation: Dorsum sellae and Posterior intercavernous sinus.
Superior relation: Diaphragma sellae and Optic chiasma.
Inferior relation: Hypophyseal fossa (Sella turcica) and Sphenoid air sinus within the body of sphenoid bone.
Lateral relation (on each side): Cavernous sinus and its contents (Internal carotid artery, Abducent nerve CN VI, Oculomotor nerve CN III, Trochlear nerve CN IV, Ophthalmic nerve V1, and Maxillary nerve V2)
Describe the subdivisions of the pituitary gland.
The pituitary gland is divided into:
1. Anterior Lobe (Adenohypophysis)
It is a true gland that secretes hormones.
It consists of:
Pars distalis:
Pars intermedia:
Pars tuberalis:
2. Posterior Lobe (Neurohypophysis)
It stores hormones .
It consists of:
Pars nervosa
Infundibulum
Q3: Describe the embryological development and dual origin of the pituitary gland.
Answer:
The pituitary gland develops during the 3rd week from two different ectodermal origins:
1. Anterior Lobe (Adenohypophysis):
It develops from Rathke's pouch, which is an upward ectodermal growth from the roof of the stomodeum (primitive mouth).
The stalk of Rathke's pouch normally degenerates and loses connection with the stomodeum.
2. Posterior Lobe (Neurohypophysis):
It develops from a downward neuroectodermal growth from the floor of the Diencephalon (primitive brain).
This connecting stalk persists to form the infundibulum (pituitary stalk).
Q4: Explain the clinical complications and applied anatomy related to pituitary gland tumors.
1. Optic Chiasma Compression: Pituitary adenomas/tumors grow upwards and compress the optic chiasma, leading to visual field defects (like bitemporal hemianopia).
2. Cavernous Sinus Compression: Tumors tend to expand laterally, occluding the Internal Carotid Artery and pressing the Abducent nerve (CN VI) before affecting any other cranial nerves inside the cavernous sinus.
3. Surgical Approach: Due to its inferior relation to the sphenoid air sinus, the preferred surgical approach for removing pituitary tumors is trans-sphenoidal (performed through the nose).
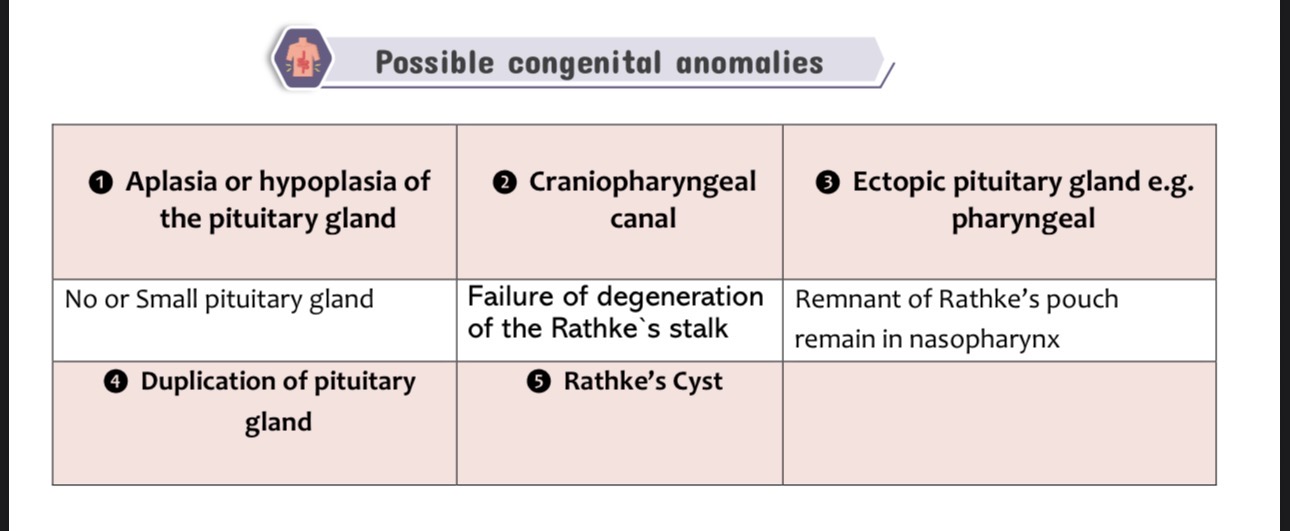
Discuss the congenital anomalies of the pituitary gland.
The congenital anomalies of the pituitary gland include:
Aplasia or hypoplasia of the pituitary gland
Due to defective development of the pituitary gland.
Results in absence (aplasia) or small size (hypoplasia) of the gland.
Craniopharyngeal canal
Occurs due to failure of degeneration of Rathke’s stalk.
Ectopic (pharyngeal) pituitary gland
Caused by persistence of remnants of Rathke’s pouch in the nasopharynx.
Duplication of the pituitary gland
A rare congenital anomaly characterized by the presence of two pituitary glands.
Rathke’s cyst
Results from persistence and cystic enlargement of remnants of Rathke’s pouch.