Tibiafemoral Joint, ACL, PCL, MCL, LCL and Meniscus
1/77
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
78 Terms
ACL Anatomy (Bundles)
Anteromedial bundle: taut in flexion. Most often injured in same position
Posterolateral bundle: taut in extension. Most often injured in same position
During examination for possible ACL tear, what do you check?
ACL, MCL, LCL and PCL
Test at multiple angles, at 0-30 deg and 80-90 deg
Post-injury of ACL tear, what structure guards at 90 deg of flexion?
Hamstrings due to helping resist anterior tibia translation
Primary Function of the ACL?
Primary restraint of anterior translation of tibia and IR
Secondary function of the ACL?
Secondary restraint to varus and valgus stresses at the knee
What else does the ACL do?
Guides the screw-home mechanism
Terminal Extension Screw Home
During terminal extension, the lateral femoral condyle finishes rolling/gliding before the medial side → causes tibial ER in open chain ("locking" the knee).
Flexion Screw Home
During flexion, ACL tension helps initiate the “unlocking” by guiding posterior femoral glide and internal tibial rotation.
Highest ACL Strain Activities
Isometric Quad Contraction at 15 deg (30Nm): 4.4% strain
Squatting with Sport Cord (anterior attachment): 4.0% strain
Active flexion-extension with 45N boot: 3.7% strain
Lachman Test (150N anterior shear): 3.0% strain
Squatting (knees over toes): 2.8% strain
Lowest ACL strain Activities
Isometric HS at 30,60 and 90 deg: 0%
Isometric Quads at 60 or 90 deg: 0%
Stationary Biking: 0.6%
Passive flexion-extension: 0.1%
Simultaneous quad + HS at 60/90: 0%
PCL Anatomy (Bundles)
Anterolateral bundle: taut in flexion. 2x as thick as Posteromedial band, allows higher failure load to occur.
Posteromedial bundle: taut in extension.
Primary Function of PCL
Resist restraint of tidal posterior translation and tibial ER
Secondary Function of PCL
Secondary restraint to varus and valgus stresses
Does the PCL Endure More Stress Than the ACL?
Anatomically larger and stronger than the ACL (almost 2× thicker). Also endures more force
Does the PCL Have a Tendency to Heal (Scar Down)?
Yes, it has a higher healing potential than the ACL
Are Isolated PCL Injuries Typically Repaired Surgically?
No
PCL MOI
Direct blow to Proximal Tibia (High energy via MVA)
Fall on the knee with the foot in a PF position
Fall with hyper flexion of the knee
What would be injured if you fall on a flexed knee while DF?
Patella Fx
Tibia is always more anterior compared to?
Femur, opposite in PCL tears, If tibia is sitting posteriorly at rest, suspect PCL injury.
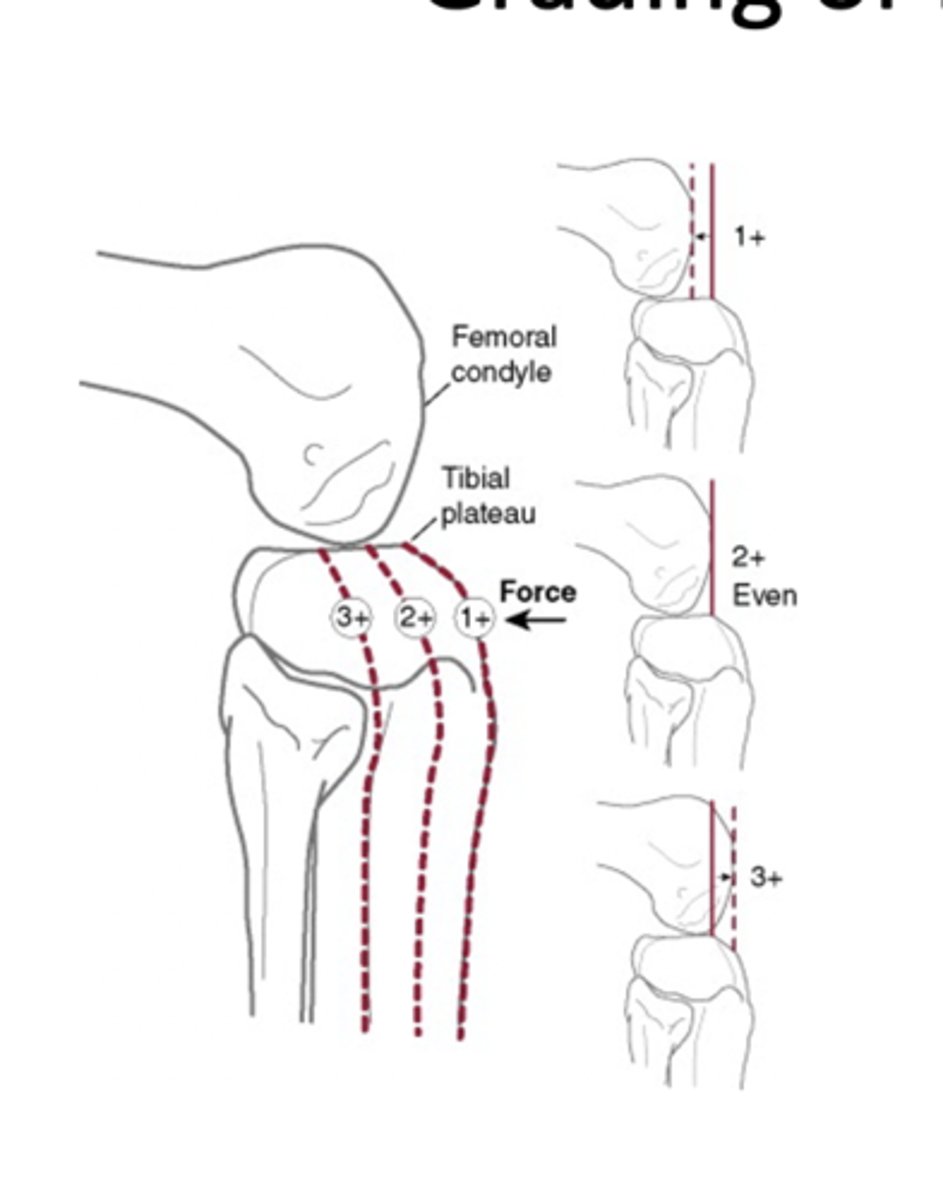
Grading of PCL Injuries
1+: Tibia plateau is slightly posterior to femoral condyles
2+: Tibia plateau is even with femoral condyles
3+: Tibia plateau is posterior to femoral condyles
ACL Injuries - Epidemiology & Risk Factors
11–90% develop tibiofemoral OA within 10 years
Females: 2.4–9.7× more likely than males in same sport
Most common in ages 15–25
70% are non-contact injuries
Greatest predictor of future OA?
Meniscal injury w/ ACL tear due to loss of shock absorption
Does ACL reconstruction help reduce risk of OA?
ACL reconstruction does NOT reduce the risk of OA development. It more prolongs the development
ACL-Deficient Knee - Meniscal Injury Risk
Year 1: 40% risk of meniscal damage
Year 5: 60%
Year 10: 80%
60-80% is degenerative not macro trauma
ACL Injury - Intrinsic Risk Factors
1. Intercondylar Notch Size (Smaller intercondylar notch width = ↑ ACL injury risk)
2. Generalized Ligamentous Laxity (2.7× more likely to tear their ACL)
3. Hormonal Influences (Ovulatory and luteal phases = ↑ estrogen. Estrogen affects: Ligament laxity (collagen remodeling) and Neuromuscular timing
ACL Injury - Extrinsic Risk Factors
1. Shoe-to-Surface Interaction (High friction between cleats and turf increases torsional forces on the knee)
2. Inadequate neuromuscular control allows dangerous combinations of movement, especially during: Deceleration, landing from jumps, cutting or pivoting
Neuromuscular Risk Factors
Ligament Dominance (Valgus and foot placement not width apart)
Quadriceps dominance (Excessive landing contact noise, more stiff, rigid, upright landing)
Leg dominance or Residual Injury Deficits (Thighs not equal side to side during flight, foot contact timing not equal due to being off centered)
Trunk Dominance (Core Dysfunction, thighs do not reach parallel, pause between jumps and does not land in the same footprint
You can only see quadriceps dominance in what view?
Sagittal view
Neuromuscular Control – Additional Risk Factors
1. Mental Fatigue (Cognitive Load)
2. Physical Fatigue
"Glitch in the system"
Are you more likely tear ACL in game or practice?
Games due to higher intensity and unpredictability
Sex Differences in ACL Injury Risk (Female vs. Male Athletes)
1. Decreased Knee Flexion Angle (Stiffer landing with increased peak vertical GRF)
2. Hip Muscle Weakness (Increased dynamic valgus= Femoral IR, tibia ER, foot pronation and hip adduction)
3. Quadriceps Dominance relative to HS (hamstrings not adequately resisting anterior tibial translation, leading to it being increased)
4. Increased Anterior Tibial Translation and Knee valgus (external abduction)
Drop Vertical Jump (DVJ) + LESS Overview
Athlete stands on a 30 cm (12 in) box.
Steps forward off the box (no jumping).
Lands both feet on the ground, then immediately jumps vertically as high as possible.
Video capture is used from frontal and sagittal views for movement analysis. Good for screening and RTS
LESS is scored based on?
17 items but most notably:
Knee flexion angle at initial contact (IC)
Shallow flexion = stiff landing → ↑ ACL load
Stance width
Too wide or too narrow = poor control
Symmetric foot contact at IC
Asymmetry = ↑ unilateral load, potential compensations
Knee valgus displacement
Medial collapse during landing = major ACL injury mechanism
Higher LESS score =?
more errors = higher ACL risk
LESS Score Breakdown
Excellent (0-3)
Good (4-5)
Moderate (6)
Poor (>7)
86% sens
64% spec
Interrater: 84% ICC
Intrarater: 91% ICC
Validation Findings - Poor LESS Scores Are Associated With?
Decreased hip and knee flexion (stiff landings), increased knee vagus, hip adduction angle (medial collapse), increased hip extension moment (ACL strain), and increased internal knee vagus, and hip adduction moment
ACL Injury Prevention - Key Components
Identification of Extrinsic Risk Factors (Neuromuscular) like valgus collapse, asymmetry, poor shock absorption
Strengthening at an appropriate load, neuromuscular training for knee, hip, trunk on stable and unstable surfaces with sports specific drills that emphasize proper alignment and mechanics
2x per week, 30 min a sesh
External or Internal focus will give the best results?
External
Prophylactic ACL Bracing
Used for prevent ACL injury, great for preventing anterior shear forces, but not good at rotary instability
DonJoy Full force is braced is used for?
Post-op ACL
ALL Ligament
Important to limit IR to limit ACL
Medial Ligament Complex is a ?
3-Layer concept, consisting of superficial, middle and deep layers
Superficial Layer of MCL complex
Fascia involving sartorius
Resists Tibia valgus (Abd) + Tibia ER
Middle Layer of MCL Complex
Includes superficial MCL, with structures of the Posteromedial corner (POL and Semimembranosus tendon insertion)
Posteromedial Corner resists?
Valgus + Posterior translation of tibia
Deep Layer of MCL complex
Represents true capsule of joint (deep MCL and includes meniscotbial and meniscofemoral ligaments
Resists valgus force
Tear of the medial ligament complex is usually from?
Deep to superficial around the joint line or femoral insertion
Contact MOI of MCL
Blow or force outside of knee/thigh that creates valgus
Non-Contact MOI of MCL
Tibia ER + Abduction stretching the medial ligament complex
Grade 1 of MCL Sprain
Microtrauma with no elongation
Exam Findings: Tender Ligament + Normal Valgus Laxity. May have pain at end ranges of motion
Laxity: 0-5mm
Grade 2 of MCL Sprain
Elongated but intact
Exam Findings: Increased valgus laxity with firm endpoint on valgus stress at 20 deg of knee flexion
Laxity: 5-10mm
Grade 3 of MCL Sprain
Complete disruption
Exam findings: Increased valgus laxity with soft endpoint on vagus stress at 30 deg of knee flexion. May be painful early on
Laxity: >10mm
Grade 1 and 2 MCL sprains are usually treated?
Conservative
Posteromedial Corner (PMC) Anatomic Components
Semimembranosus Insertion ("Semimembranosus Corner")
Posterior Oblique Ligament (POL)
Oblique Popliteal Ligament (OPL)
Posterior One-Third of the Medial Meniscus
Injury to the PMC can result in?
Anteromedial rotary instability (involving the MCL and POL)
Posteromedial rotary instability (due to damage to the posteromedial capsule, including semimembranosus, OPL
Valgus instability, accompanied by ACL injury 73/93 times
Grade lll POL typical require?
Surgical Reconstruction
Anteromedial Rotary Instability + test would show?
Anterior translation of the medial tibial plateau + Tibia ER
Posteromedial Rotary instability + test would show?
Posterior translation of the medial tibial plateau + Tibia IR
How would you test Anteromedial Rotary Instability?
1. (Anteromedial drawer variant)
Patient: Supine, knee flexed to 90°
Tibia is placed in 15° external rotation
Examiner applies an anterior drawer force to the tibia+ Test: Excessive anterior displacement of the medial tibial plateau
➡️ Indicates MCL + POL + possibly ACL injury
How would you test posteormedial rotary instability?
Posterior Drawer with Tibial Internal Rotation
Patient: Supine, knee flexed to 90°
Examiner applies a posterior drawer force while keeping tibia in internal rotation (30 deg)
+ Test: Excessive posterior translation of the medial tibial plateau relative to lateral side
➡️ May produce a "medial sag"
Post-operative rehab is based on associated ligament reconstruction of?
ACL/PCL injuries
Posterolateral Corner (PLC) Anatomical Component
Fibular Collateral Ligament (LCL)
Arcuate Ligament Complex (Popliteofibular Ligament, Fabellofibular Ligament, Popliteus Tendon)
Posterolateral corner can be injured in?
Isolation
PLC primary functions
Resists varus stress and controls external rotation of the tibia
Provides posterolateral rotational stability
PLC works with PLC due to?
Both resist posterior tibial translation, especially under varus and external rotation stress
Dial Test for PLC Rotary Instability
Purpose: Detects increased external rotation of the tibia — sensitive for PLC and/or PCL injury.
Procedure:
Patient is prone (can also be done supine), knees flexed to 30° and 90°
Stabilize the thigh, and externally rotate the lower legs
Interpretation:
Increased external rotation (>10–15°) on one side:
At 30° only: PLC injury
At both 30° and 90°: PLC + PCL injury
At 90° only: More suggestive of isolated PCL injury
If Varus test + tests at 0 deg and 20-30 deg?
0 deg: More structures involved (PLC + Cruciates)
20-30 deg: LCL Isolated
Straight Anterior Instability
Anteromedial bundle of ACL is lax
Anterolateral instability
Involves ACL, ITB, arcuate ligament complex and ALL
Posteromedial Instability
PMC, PCL and POL
Posterolateral Instability
Involves PCL, LCL and PLC
AnteroMedial Instability
Involves ACL, MCL, POL and PMC
Anterior Transition Restraints
Primary: ACL
Secondary: MCL, LCL, Middle and posterior 1/3 of medial/lateral capsule, PMC, and IT band
Posterior Translation Restraints
Primary: PCL
Secondary: MCL, LCL, posterior 1/3 of medial/lateral capsule, polities tendon, and A/P meniscofemoral ligaments
Valgus Restraints
Primary: MCL
Secondary: ACL, PCL, middle 1/3 of medial capsule, posterior oblique ligament
Varus Restraints
Primary: LCL
Secondary: ACL, PCL, ITB, Middle 1/3 of lateral capsule, posteorlateral corner (arcuate complex)
Lateral Rotation Restraints
Primary: MCL/LCL
Secondary: PLC (arcuate complex)
Medial Rotation Restraints
Primary: ACL
Secondary: PMC + Meniscofemoral ligaments