Quiz 4 + Midterm 2 (Lectures 8-11) - 231 Lecture
1/77
Earn XP
Description and Tags
Make sure to study Lecture 7 Slides
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
78 Terms
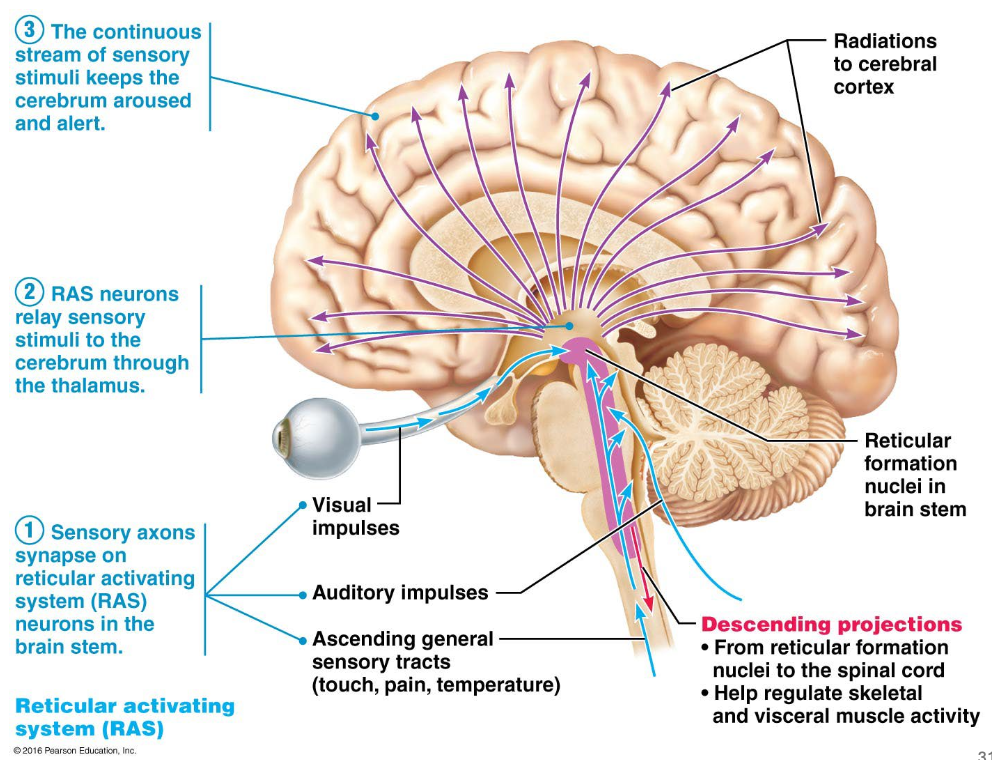
Reticular Formation (L7)
Sensory neurons carry information up the spinal cord to the brain stem
Retricular Activating System (RAS) neurons in the brain stem are stimulated by the incoming sensory information
RAS neurons projects these signals to the thalamus
Thalamus selectively sorts and filters the information, passing vital sensory messages to specific areas of the cerebral cortex for conscious perception
Continuous strea, of sensory information keeps the cerebrum aroused and alert
Caffeine (L7)
Caffiene is an antagonist
Similar structure to Adenosine
Caffiene can fit into the same receptors as Adenosine, essentially blocking Adenosine from binding
Adenosine is prevented from inducing drowsiness
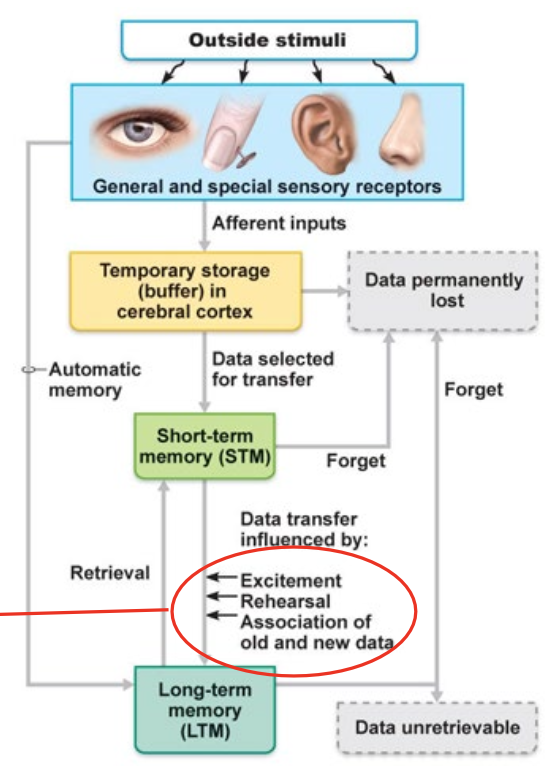
Learning and Memory (L7)
Outside Stimuli
→ General and special sensory receptors
→ Temporary storage
→ (Data Permanently Lost)
→ Short-Term Memory (STM)
→ Excitement, Rehearsal, Association of old and new data
→ Long-Term Memory (LTM)
Consolidation = process of stabilizing and transforming short-term memories into long-term memories
Done through:
Excitement
Rehearsal
Association of old and new data
Declarative and Procedural Memory (L7)
Declarative Memory = the conscious recall of facts and events (“knowing what”)
Loop:
Sensory Input →
raw input processed in primary sensory cortices then passed on to high-level processing in association cortex
Association cortex →
brain gives meaning to the raw input - ex: recognizing a song or face
Medial temporal lobe →
receives processed information from association cortex and associated sights, sounds, etc. into a single memory
Thalamus →
routes information from the medial temporal lobe to other regions
Prefrontal cortex
during encoding, PFC helps select, organize, and evaluate incoming information based on relevance to the individual’s goals
can send signals back to the thalamus or MTL to reconstruct memory
Procedural (Skills) Memory = unconscious execution of motor and cognitive skills (“knowing how”)
Loop:
Sensory and motor inputs
raw input → primary sensory cortex → association cortex
Association cortex
integrate sensory data with context, spatial awareness, and memory
Basal nuclei
project information to specific nuclei in the motor thalamus
Thalamus
send excitatory signals to excite the cortical motor areas
Premotor cortex
receives information from thalamus
map out muscle sequences and prepare the body to execute
Cerebellus acts in the background to refine motor sequences
balance and coordination
motor memory
How to improve formation of long-term memories (L7)
Re-study and re-test mastered terms
Why are there enlargements? Where does the spinal cord end?
Cervial and Lumbar Enlargements =
More gray matter due to higher amount of innervation to these regions
Spinal cord ends near L1 vertebrae
PNS
Peripheral Nervous System =
cranial nerves and spinal nerves
Communication between the CNS and the rest of the body
Lumbar Puncture
Retracts CSF from subarachnoid space
In the lumbar area, past the spinal cord
For example, to identify infenction of menigies/meningitis
Spinal Cord
Dorsal root = sensory neurons
Dorsal root ganglion = holds sensory unipolared neurons
Ventral root = motor neurons
Spinal nerve = where sensory and motor neurons meet
Gray Matter vs White Matter
Gray Matter =
Horns
Nuclei
White Matter =
Columns (tracts)
Ascending tracts = carry sensory information to the brain
Descending tracts = carry commands to motor neurons
Sensory (Ascending) Pathways
DECUSSATION occurs in the BRAINSTEM or SPINAL CORD
3 neuron circuits from receptor to Primary Somatosensory Cortex
Motor (Descending) Pathways
DECUSSATION occurs in the BRAINSTEM or SPINAL CORD
Two or Three neuron circuits from Primary Motor Cortex to the muscle
Spinal Cord Injuries
Deficits = any loss or impairment of sensory, motor, cognitive, or bodily function caused by damage to the nerve pathways within the spinal cord
Deficits inferior to the site of damage:
loss of sensation
loss of motor function
Paralysis due to spinal cord injury
How far down the spinal injury is in the spine is relevant to the extent of the paralysis
You don’t kill the neurons, unless you crush the cell bodies, you just tear the axons
After effects of the spinal cord injury can cause cell bodies to die
You are able to regrow axons, but it is hard to due to scar tissue
Regeneration of axons in spinal cord in fish is better than in mammals
Mammals = axons get stuck in scar tissue
Fish = able to regenerate spinal columns
Treatments for spinal cord injury
Stem cell therapy
Optimal time is before the scar formation, and after the inflammatory reaction
Electrical Stimulators
Can recover some function by stimulating neurons
Peripheral Nervous System: Visceral vs Somatic
Visceral = internal organs
organ stretch, nausea, hunger, changes in chemical composition
largely unconscious
Somatic = external, body-wall structures
touch, pain, temperature, etc
highly conscious
Gray Matter vs White Matter (spinal cord)
Gray Matter:
Ganglia
White Matter:
Nerves/Roots/Rami
Sympathetic trunk ganglion:
along sides of the vertebral column in two vertical chains
efferent pathway
have a synapse
Nerve Structure
Nerve →
Epineuirm surrounds bundles of perineurium
Perineurium surround buncles of endoneurium
Endoneurium surrounds myelin sheath
Myelin shealth surround axons
Nerve = bundles of axons
Cranial Nerves
Can be sensory, motor, or both
Most connect to the brainstem
Most are involved with structures in the head and neck
Spinal Nerves
All spinal nerves are mixed nerves
Contain both sensory and motor fibers
Cranial Nerves = nerves connected to the brain
Nerve Plexuses
A complex, web-like network of intersecting nerves in the peripheral nervous system. Functioning like an electrical junction box, it sorts, combines, and redistributes nerve fibers from multiple spinal segments so that fibers traveling to a specific body part are grouped together
Innervation of Specific body regions
Dermatome = The regions of the body that are associated with a specific type of spinal nerve
Innervation of specific body region
Ex: Sciatica = radiating sciatic pain and sensory symptoms will follow distinct dermatomal patterns on the leg, depending on exactly which nerve root is affected
Shingles
After an infection, the virus can retreat to the nervous system and remain dormant in the dorsal-root ganglion
When reactivated, the virus travels down the specific sensory nerve fibers to the skin, causing a painful, blistering rash that is typically restricted to a single dermatome
Sensory System Signaling Summary
Perception =
The interpretation of the signals from those receptors
Circuits =
Connect sensory receptors to the CNS for perception
Receptors =
Detect sensory input and send signals to the CNS
Sensory Systems - levels of perception
Perceptual detection (something happened)
Magnitude estimation (how intense was it?)
Stimulus discrimination (where was it located?)
Quality discrimination (what color is it)
Feature abstraction (identify complexity)
Pattern recognition (do I know what this is?)
Sensory Systems - classification based on the location of the receptors
General senses = found all over the entire body, including the skin, muscles, internal organs, joints, etc
AKA Somatosensory System, monitor touch, pressure, temperature, pain, body position, etc
Special Senses = concentrated exclusively in specialized organs within the head
eyes, ears, nose, mouth
dedicated to procesing specific, complex, environmental stimuli (vision, hearing, balance, taste, small)
require localized structures before sending this refined data directly to the brain
Sensory Systems - classification based on where the stimulus is coming from
Exteroceptors = external stimuli
sight, taste, hearing
Interoceptors = internal environment
inside (heart, lungs, stomach)
Proprioceptos = body position and movement
at joints, muscles, tendons
Primary Sensory Coding - what do receptors tell the brain and how does it interpret that information?
Receptors tell the brain:
Stimulus type
Stimulus location
Stimulus intensity
Stimulus duration
Primary Sensory Coding - Stimulus Type (MODALITY)
Receptors have graded potentials (receptor potentials) in response to a particular type of stimulus
Mechanoreceptors - TOUCH
Convert physical forces (touch, pressure, stretching, and sound waves) into electrical signals
Examples: Pacinian corpuscles, Merkel Cells, and hair cells in the ear
Mechanical force distorts the mechanoreceptor’s membrane, pulling open the mechanically-gated ion channels and causing a local change/receptor potential
GRADED POTENTIAL = light touch opens fewer ion channels, resulting in a weak potential; a heavy press opens up more channels, leading to a larger potential
Chemoreceptors - TASTE and SMELL
Specialized sensory cells that detect chemicals in the environment and convert them into electrical signals that the brain interprets as taste and smell
Thermoreceptors - TEMPERATURE
Detect temperature and changes in temperature and translate it to electrical signals
Free nerve endings
Nocioceptors - PAIN
specialized sensory nerve endings that detect extreme stimuli and convert them into electrical signals
Photoreceptora - VISION
When light hits the rods or cones in retina, they convert the light waves into electrical signals
Primary Sensory Coding: Location
Size of Receptive Fields
Smaller receptive fields = better determination
Receptive fields that overlap can help determine which part of the skin is stimulated
Primary Sensory Coding: Modality and Location
Specific Ascending Pathways
Modality = specific type of stimulus being detected (ex: light, sound, temp, smell)
Each modality has a pathway that goes through the thalamus to a specific primary sensory cortex (in a specifc lobe) then to a specific association cortex for higher level understanding and integration of that sensation
Within the cortex, there are maps that correspond to specific parts of the body or receptive fields
Primary Sensory Coding: Stimulus Intensity
Stronger sitmuli cause MORE action potentials in receptor
More APs, cause release of more neurotransmitter in the synapse to cause a stronger post-synaptic potential
Intensity coded by number of action potentials
Primary Sensory Coding: Stimulus duration
Adaption = decrease in AP frequency in presence of constant stimulus
Phasic receptors = adapt quickly - stop sending signals
Tonic receptors = don’t adapt or adapt slowly - continue sending signals
Ex:
Smell = quick, bad sell = not quick
Taste = somewhat fast
Touch = quick adaptor (clothes)
Summary of Sensory and Receptors and Principles of Sensory Systems
Receptors are sensitive to specific modalities
Ascending pathways/circuits go through thalamus before relayed to cortex
Processing in association areas can affect perception and memory
Primay coding involves receptors transmitting info about stimulus type, location, intensity, and duration
General (somatic) senses - Types of receptors
Somatosensory:
free nerve endings - uncapsulated, can penetrate into epidermis
can be phasic or tonic
can detect mechanical stimuli, temperature, pain, etc
ONE free nerve ending responds to ONE stimulus
Merkel cells -
in strantum basale
send signals to free nerve endings
receptive field = small
very light touch
Hair follicle receptor -
free nerve ending that is wrapped around the hair sheath
Meissner corpuscle -
found in papillary layer, medium receptive field, encapsulated
Pacinian corpuscle -
reticular dermis, large receptive field
Proprioception:
muscle spindles -
inside skeletal muscle
send sensory (afferent) signals regarding state of muscle
golgi tendon organs
send sensory (afferent) signals regarding state of muscle
Somatic Sensation and Proprioception
Receptors (afferent neurons) are unipolar neurons neurons with cells bodies in the DRG
General senses - Circuits Ascending Pathways
Specifc Ascending Pathways:
Affect neuron sends signal to spinal cord or brainstem
Ascending neuron decussates in the SPINAL CORD or MEDULLA
Projection neuron sends signal from THALAMUS to PRIMARY SOMATOSENSORY CORTEX
Contralateral = opposite side
Ipsilateral = same side
Primary Somatosensory Cortex
PARIETAL LOBE
each hemisphere receives general sensory information from skin and joints/muscles from opposite side of the body
Touch
Temperature
Pain
Itch
Body position (proprioceptors)
The General Senses: Nocioceptors - how could you stop pain?
Nocioceptors = respond to extreme mechanical deformation, excessive heat and many chemicals
Decrease stimulus
Ibuprofen
decreases activation of pathway
Stop voltage-gated channels = block action potentials
Increae uptake at synapses = decrease amount of NT in the synaptic space
Non-pain stimulus = Inhibits afferent neuron
Referred Pain
Convergence of two receptors on one ascending pathway
General Sensory Systems Summary
Receptors
can be free-nerve endings or encapsulated
Most are unipolar neurons with cells bodies in DRG
Receptor potentials in response to stimuli that trigger APs
Circuits
Synapses in spinal cord and thalamus before related to cortex
Can cause reflexes before stimulus perception occurs
Decussation in spinal cord or medulla
Perception
Somato-sensory cortex in parietal lobe
Gustation Chemoreceptors
Remember: special senses have a specific organ
Gustation Chemoreceptors
Papilla = projections
Taste buds located on the side of papilla
Activation of Gustatory (Taste) Receptors:
Taste sensations:
Sweet, sour, salty, bitter, umami
Tate Buds:
Gustatory receptor cells
can be damaged easily bc they are more susceptible to the taste pore
Supporting cells
basal cell = makes more cells
Free nerve endings of afferent neurons
sent to cranial nerve
Signal Transduction in gustatory receptors
Chemicals enter cells through channels
Sodium can diffuse straght into the receptors through channels
Bigger chemicals need recetors to bind to and act through a secondary messenger system
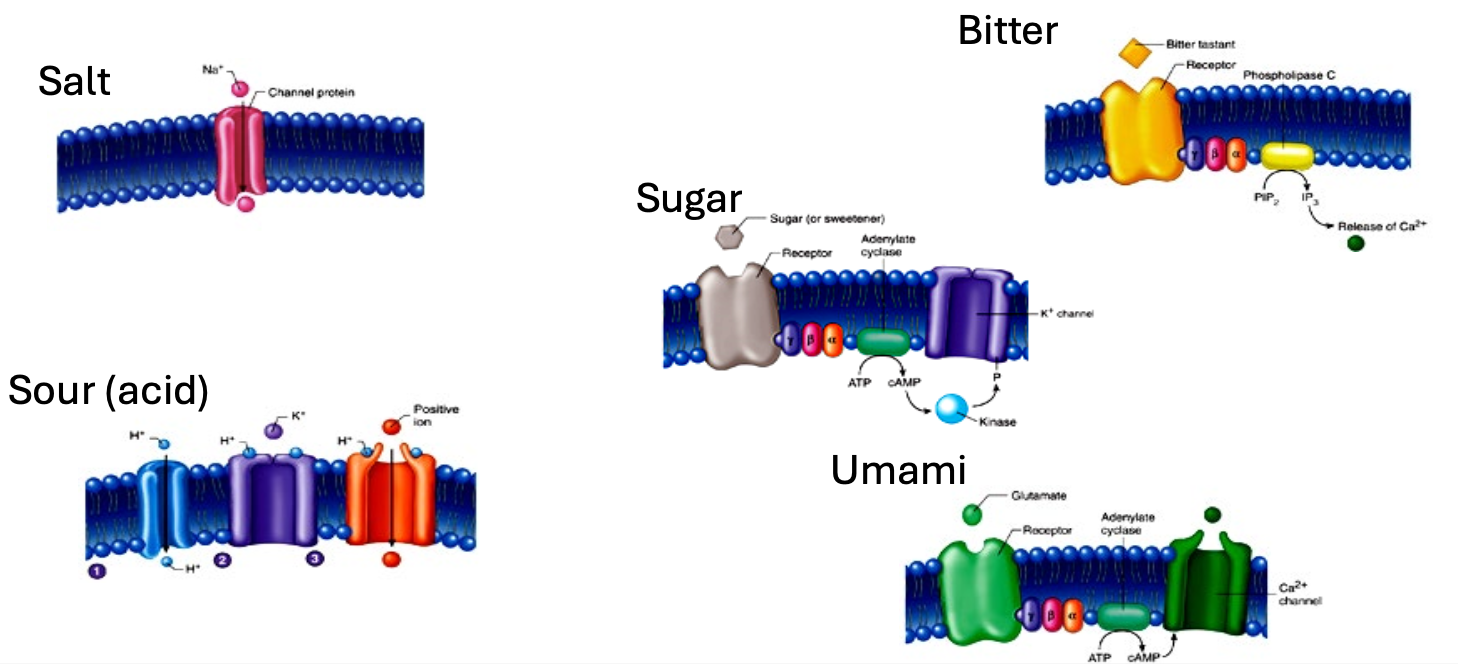
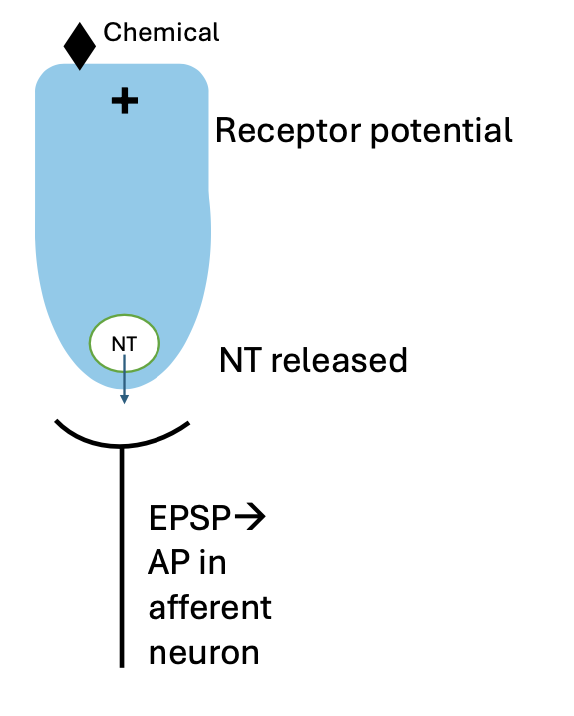
Signal transduction in gustatory receptors
Receptor potentials occur when gustatory receptor is exposed to chemical
Action potentials occur in afferent neuron
Gustatory cells depolarize and release NT
Sensitivity of Different taste receptors
Smaller threshold for action potential = more sensitive
can be a warning sign to not eat
bitter is most sensitive
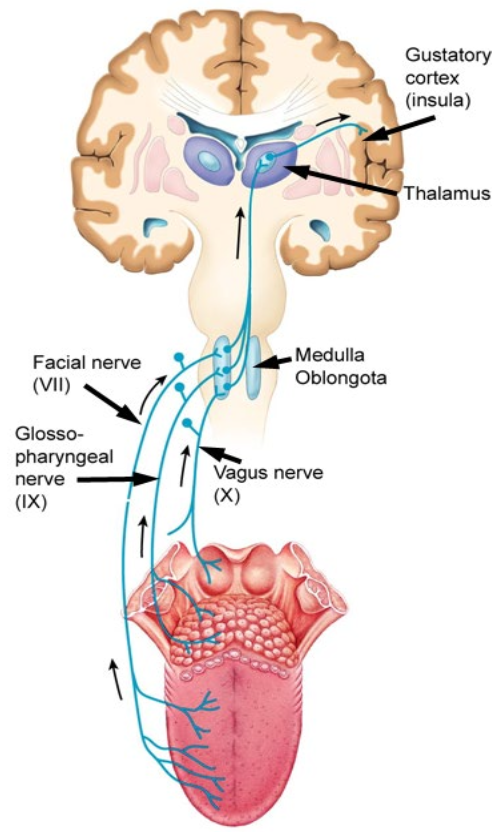
Gustatory Pathway
Afferent neurons in cranial nerves
→ Medulla oblongota
→ Thalamus
→ Gustatory cortex
Olfaction (smell) - Chemorecptors
Chemical binds dentrite of the olfactory receptor cell in cilia
Axons group together to form olfactory nerve
olfactory nerve goes through ethmoid bone
olfactory nerve goes into the olfactory bulb
GLOMERULI = bundle of nerves specific to odor molecule
mitral cells connects to glomeruli and form the olfactory tract
OLFACTORY PATHWAY DOES NOT GO THROUGH THE THALAMUS
Signal transduction in olfactory receptors
Receptor potentials occur when neuron is exposed to odorant molecules
Action potentials occur if receptor potential is above threshold
Around 400 different types of receptors
Processing of olfactory information
Axons of olfactory neruons are found in olfactory nerves that go to the olfactory bulb
Synapses occur in balls called GLOMERULI
Each glomerulus processes info about one chemical
Olfactory Pathway
Olfactory receptor (afferent neuron)
→ Olfactory bulb
→ Olfactory cortex (perception of odors)
→ Hypothalamus and Limbic regions (Physiological and emotional responses to odors)
DOES NOT GO THROUGH THALAMUS
Chemosensory Systems Summary
Olfactory
Receptors =
Receptor potentials in response to stimuli that trigger APs
Circuits =
Olfactory nerves synapse in olfactory bulb - goes directly to cortex
Each glomerulus processes a specific odor
Perception =
Olfactory corte in temporal lobe connects to limbic system
Gustation
Receptors =
Receptor potentials that cause graded release of NT to afferent neuron
Circuits =
Gustatory receptors synapse on afferent neuron - goes through brainstem and thalamus
Decussation in medulla
Perception =
Gustatory cortex in insula
Hearing and Equilibrium
Mechanoreceptors sense vibration
Found in the inner ear
Hearing = Cochlea
Equilibrium = Vestibule & Semicircular Canals
Pathways of sound wave-amplification
Amplification in middle ear as it goes through malleus, incus, stapes
Air filled cavity
Sound Transduction
Tympanic membrane deflects
Middle ear bones move
Membrane in oval window moves
Basilar membrane moves
Membrane in round window moves
Cochlea - houses sensory receptors for hearing
Scala vestibuli - filled with perilymph
Cochlear duct - filled endolymph
Scala tympani - filled with perilymph
Bailar membrane lines cochlear duct
Increases increases in thickness →
Thinner part detects high pitch, thick detects low
Hair cells on basilar membrane attached to tectorial membrane
When basilar membrane moves, the tectorial membrane forces the hair cells to intake potassium, causing a depolarization of the cells
Action potential sent to brain
Resonance
Different parts of the basilar membrane are sensitive to different frequencies
How sound energy is transduced to AP
Bending of the sterocilia opens ion channels - causes graded potentials
Auditory Pathway
Vestibulocochlear Nerve
→ Medulla (decusates)
→ Midbrain (reflexes)
→ Thalamus
→ Primary auditory cortex (perception) - temporal lobe
Threshold of Hearing
Threshold for hearing is higher at lower frequencies
Over 120 threshold of pain - can damage hair cells
Deafness
Conduction deafness = conduction of sound wave from air → basement membrane
Something happens to hamper sound conduction of sound wave to fluid of inner ear
Sensorineural deafness = damage from hair cells → afferent neurons
damage to neural structures in auditory pathway
Cochlear implant
Electrically stimulates afferent neurons, allowing signals to go to the brain
Hearing Summary
Receptors
Receptor potentials that cause graded release of NT to afferent neuron
The basilar membrane resonates at different frequencies to maximmaly stimulate particular hair cells
Circuits
Synapses occur in the medulla, midbrain, and thalamus
Can cause reflexes before stimulus perception occurs
Decussation in medulla
Perception
Auditory cortex in temporal lobe
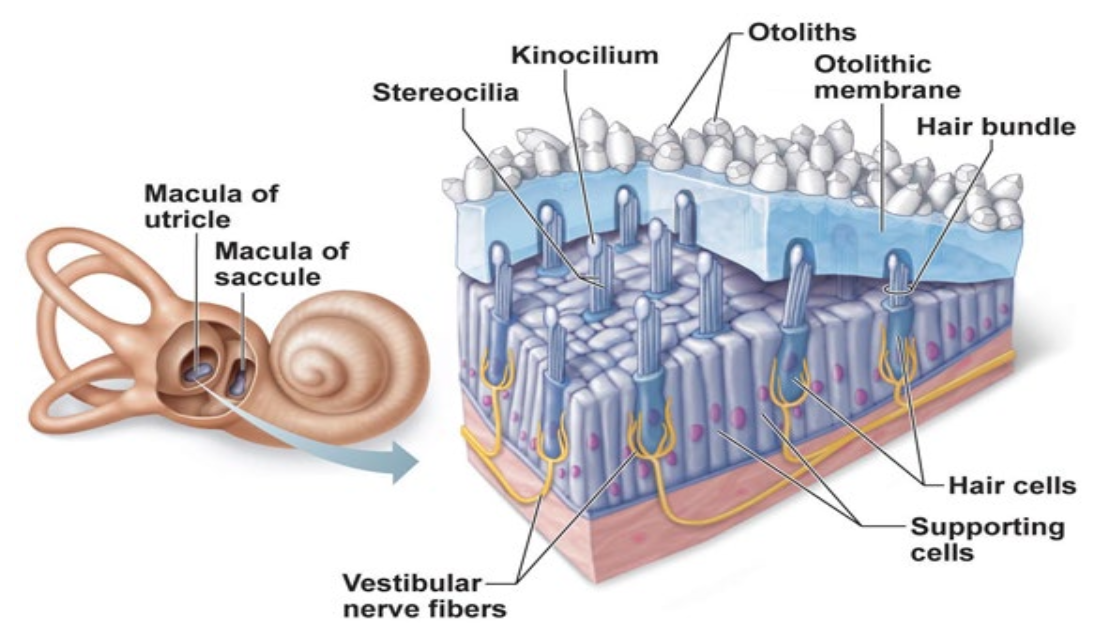
Static Equilibrium
In the Vestibule:
Macula of utricle
Macula of saccule
Both situated perpendicular to each other
Otoliths =
Stones that give density to membrane
Otolitic Membrane =
Gelatenous
Will “pull” on hairs when not flat
Static = still
Nerve fibers send signals of position
Used to understand position of head in relation to gravity
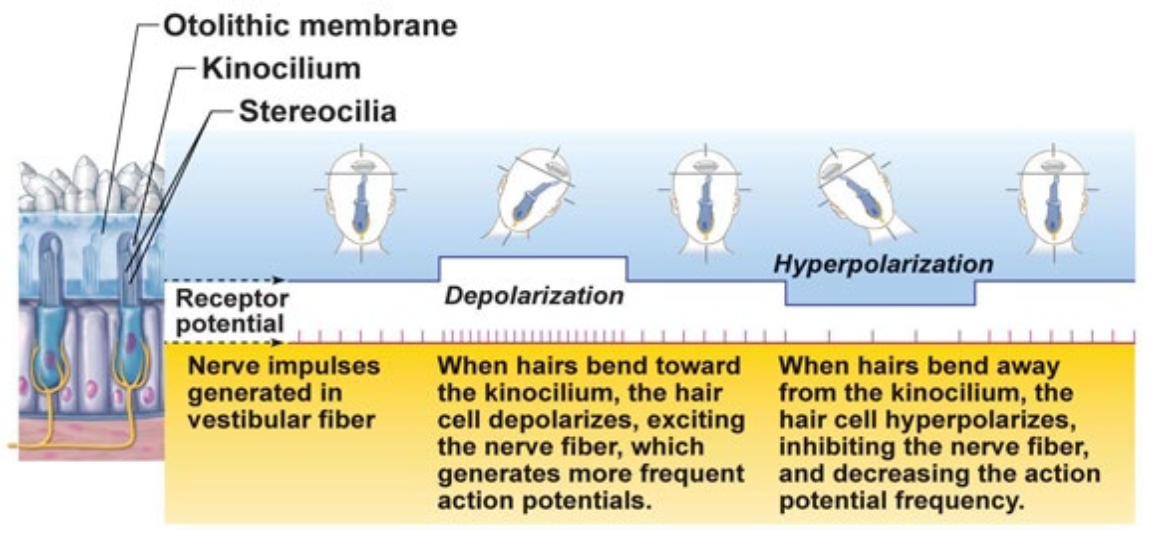
Static Equilibrium - Explanation
Nerve impulses generated in vestibular fiber (nerve)
When hairs bend toward the Kinocilium, the hair cell depolarizes, exciting the nerve fiber, which generates more frequent action potentials
When hairs bend away from the kinocilium, the hair cell hyper polarizes, inhibiting the nerve fiber, and decreasing the action potential frequency
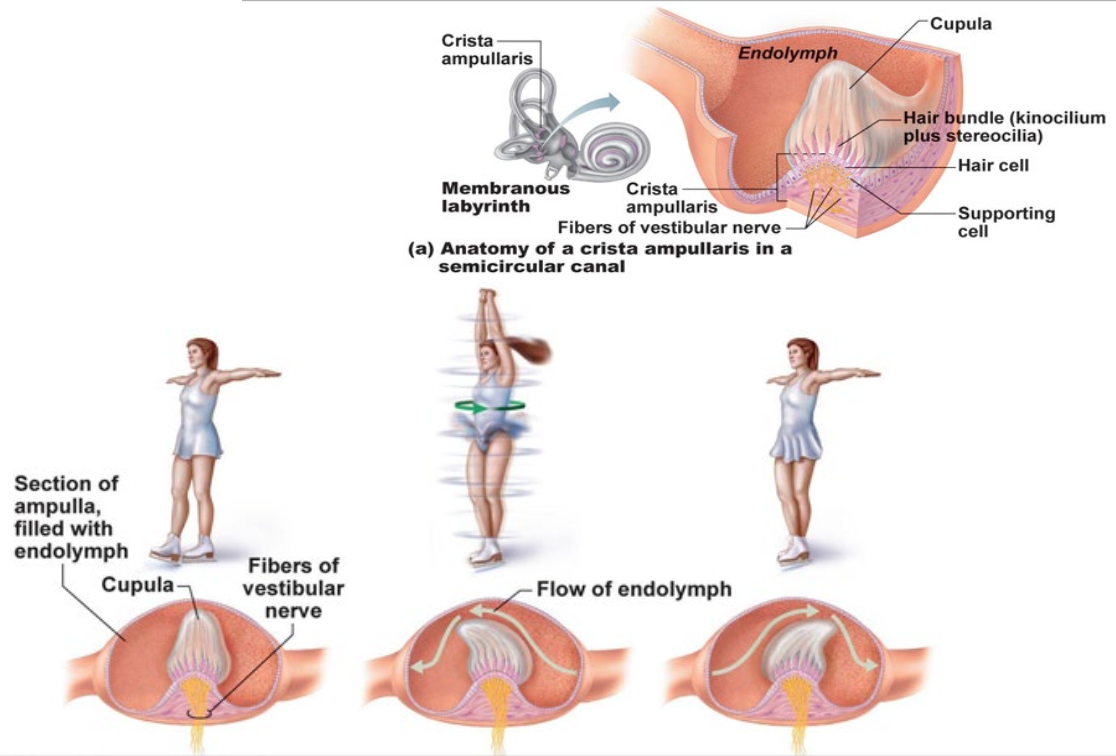
Dynamic Equilibrium
Inside Semicircular Canal
Bone moves, fluid still
Fluid catches up with bone
Bone stops, fluid keeps going
When the fluid moves, it pushes the Cupula
Cupula is bent and ion channels are opened, altering electrical signals sent to the vestibular nerve
Cupula will continue to be stimulated when fluid is slowing down after the bone stop moving due to inertia or fluid
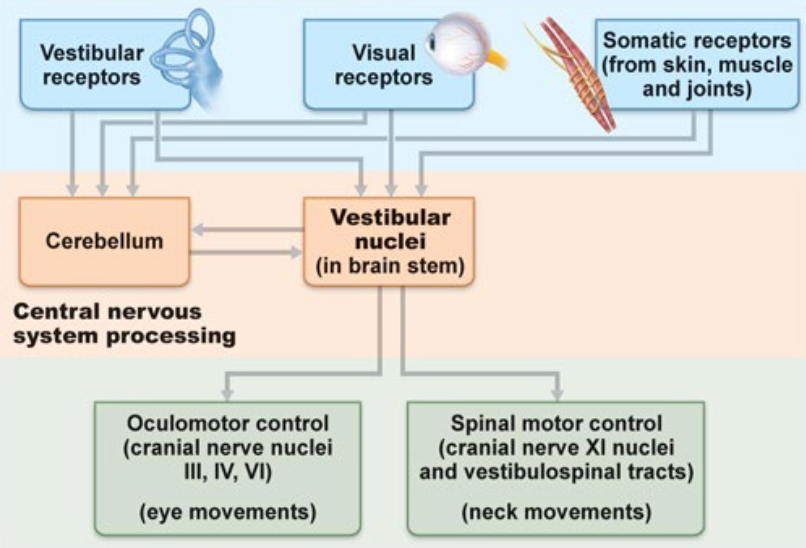
Balance and Equilibrium
Information about the body’s position in space comes from three main sources and is fed into two major processing areas in the central nervous system
Three main sources:
Vestibular Receptors
Visual Receptors
Somatic Receptors (skin, muscle, joints)
Two major processing areas:
Cerebellum → CNS
VESTIBULAR NUCLEI (in brain stem)
→ cranial nerves (PNS) for eye and neck movements
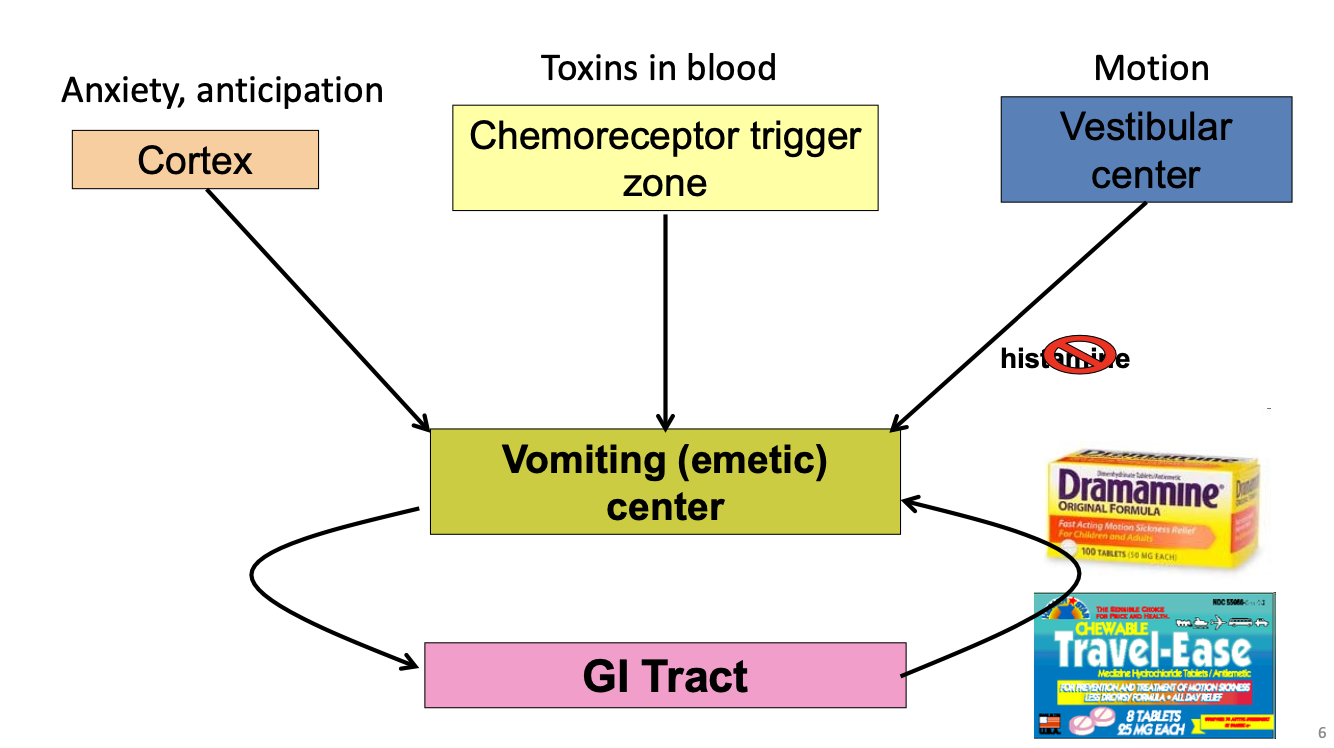
Activation of Vomiting (emetic) center
3 Sources Activate Vomit Center:
Cortex (anxiety, anticipation) →
Chemoreceptor trigger zone (toxins in blood) →
Vestibular Center (motion) →
Histamine is the primary neurotransmitter in the brainstem that drives nausea and vomiting
Histamine attatches to Histamine receptors in the vestibular nuclei
VOMITING CENTER
Sends signals to GI Tract
GI Tract can also send signals to Vomiting Center
*No conscious perception in equilibrium
Equilibrium Summary
Receptors
Hair cells in vestibule (static equilibrium) or semi-circular canals (dynamic equilibrium)
Circuits
Synapses in brainstem for balance to vestibular center
Inputs from vestibular center to other regions (like vomiting center)
Perception
No direct cortical (cortex) region involved with perception
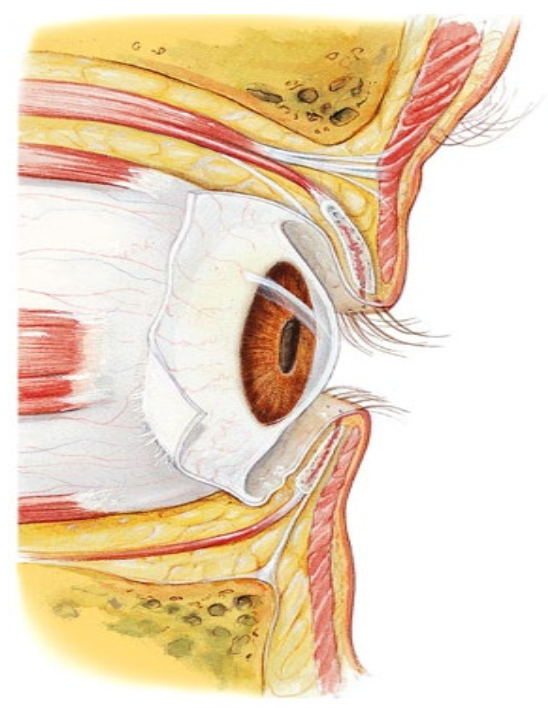
Accessory organs around the eye
Eyebrows and eyelashes
Eyelids (palpebrae)
External eye muscles
Conjunctiva = thin membrane over the sclera
Prevents debris from migrating to the back of the eye
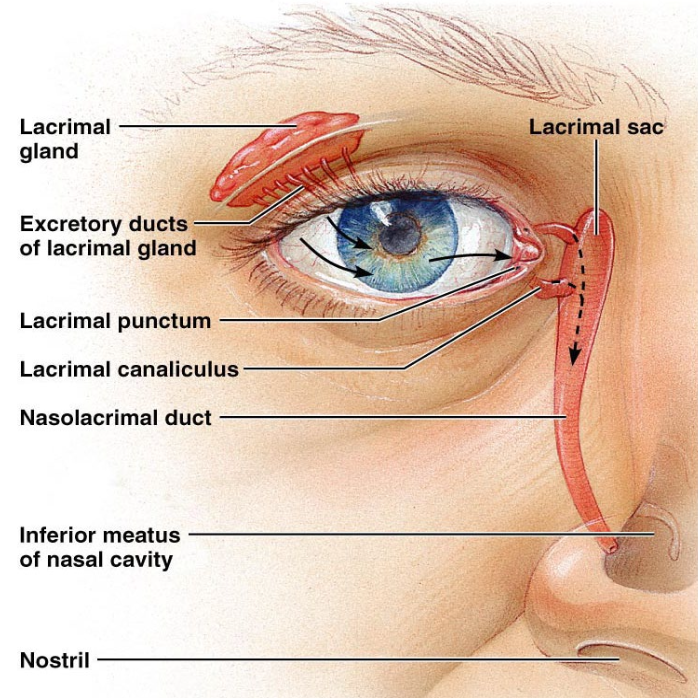
Lacrimal apparatus
Lacrimal Apparatus
Tears = Lacrimal Fluid
Cleans and lubricates the eye
Contains mucus, antibodies, and lysozyme
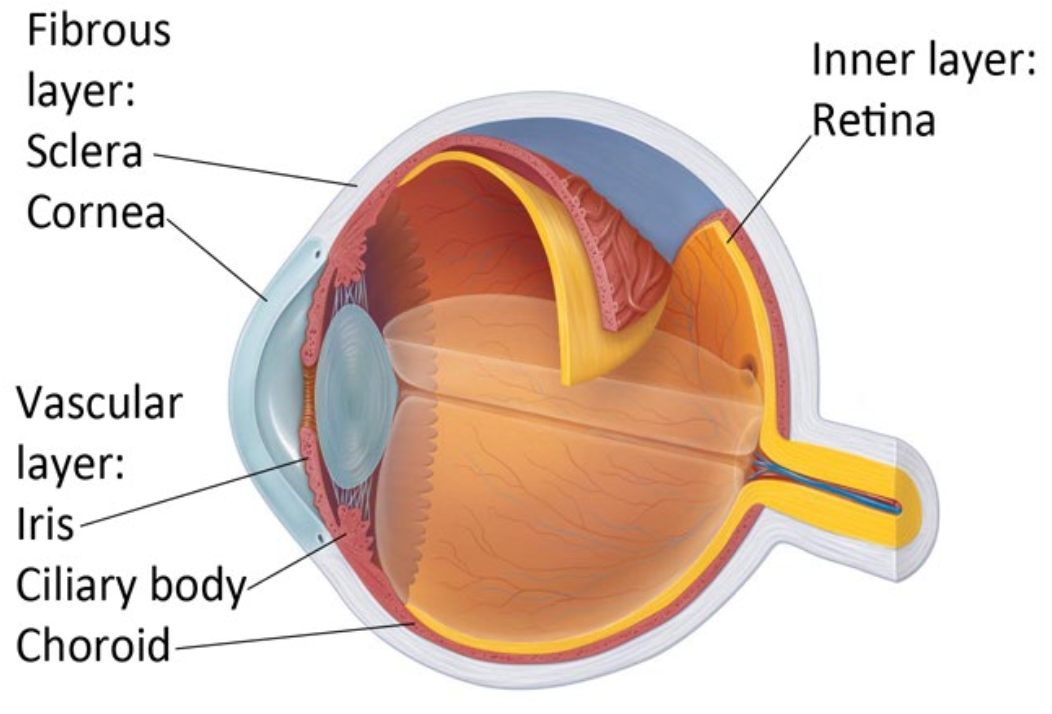
Structure of the eyeball
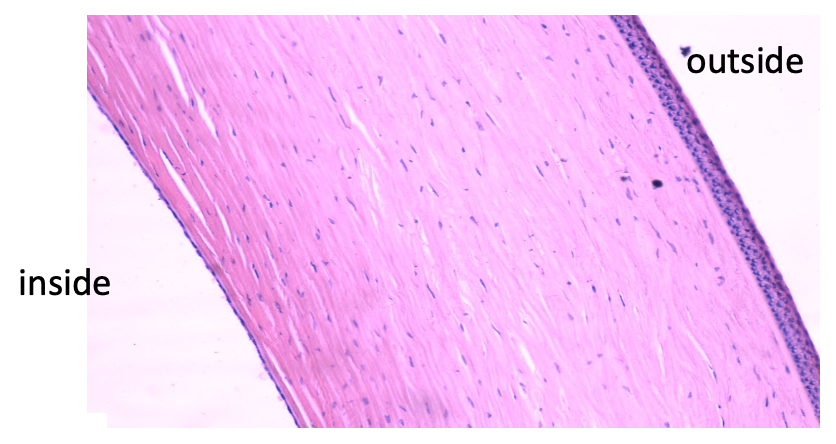
Fibrous Layer:
Sclera
thick, white part of the eye
Cornea
works with the lens to bend the light that hits the retina
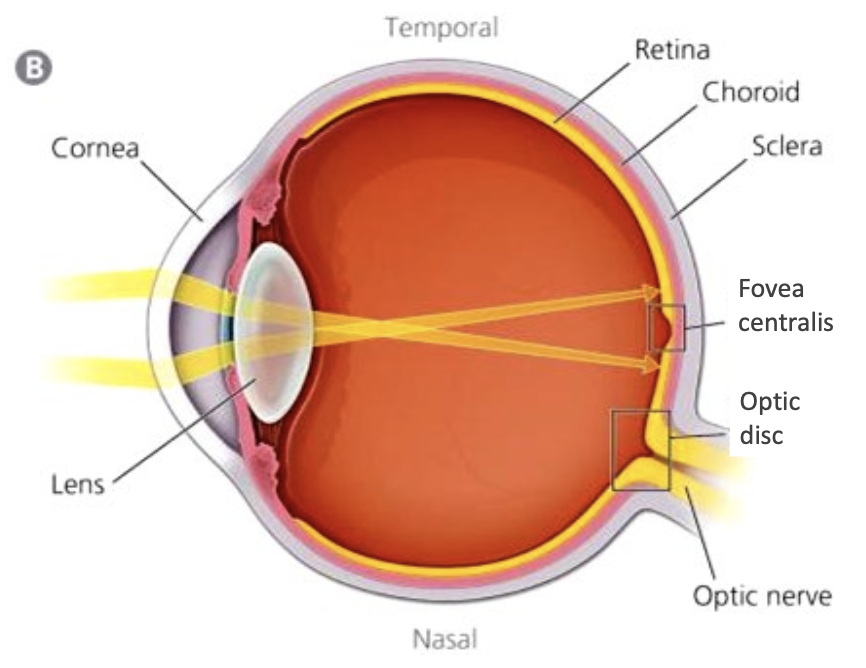
Inner Layer:
Retina
Composed of photoreceptors (rods and cones), Neurons, and Glial cells
Fovea = where light is focused
Vascular Layer:
Iris
Ciliary Body
produces aqueous humor
Choroid
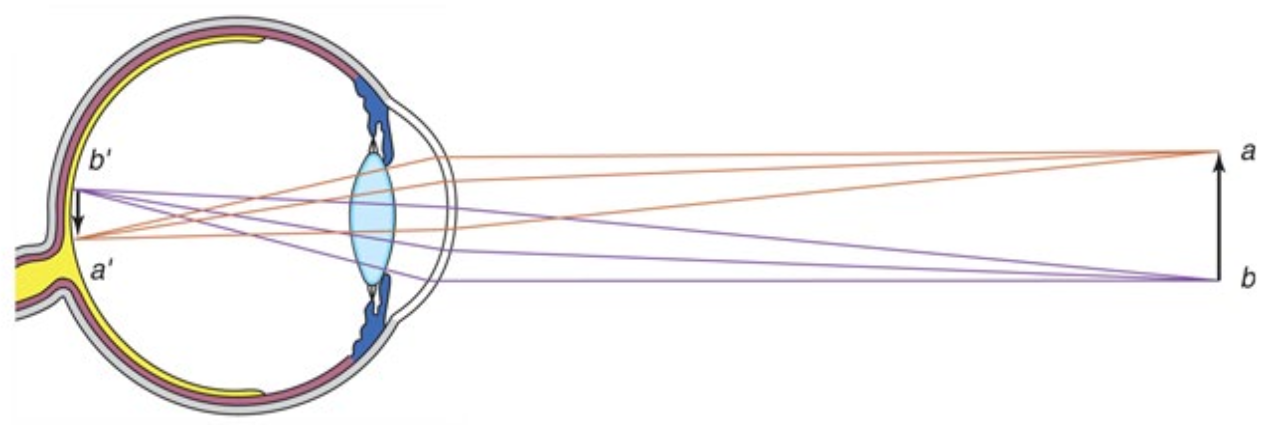
Vision
Optical Component
focuses light onto receptor cells
Neuron Component
transforms light stimulus to graded potentials and action potentials
Optics of vision
Refraction of light by cornea and lens
Regulation of the amount of light entering the eye by the iris
Cornea
Transparent tissue that bends (refracts) light into the eye
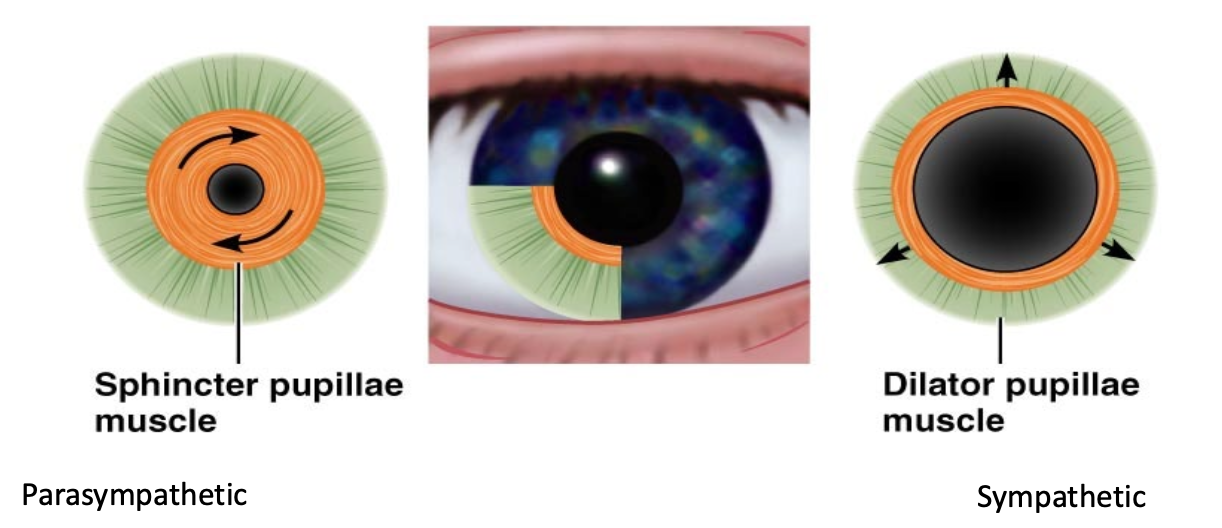
Iris
Two separate muscles to control diameter of the pupil
Sphincter pupillae muscle
Parasympathetic
Less light
Dilator pupillae muscle
Sympathetic
More light
Lens
The lens can change shape
ACCOMODATION = tauting or slac