grondslagen vd kp hc 3
1/15
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
16 Terms
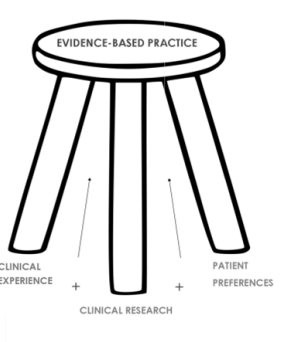
evidence-based practice (EBP)
an approach to clinical decision making which comprises the thoughtful integration of the best available scientific evidence concerning psychotherapy with clinical expertise and client preferences/values.
first leg
best available research evidence (whether and why a treatment works)
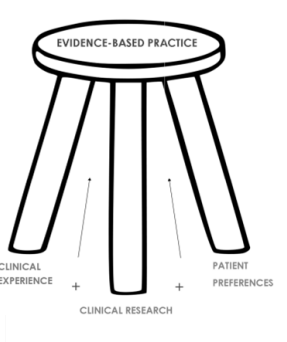
second leg
clinical expertise (clinical judgement and clinical experience)
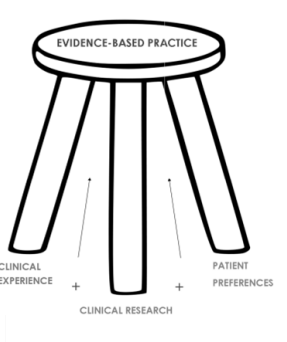
third leg
client preferences and values
empirically supported therapies (ESTs)
specific psychological treatments that have been shown to be effective in controlled research for specific conditions.
- Scientific literature e.g. meta-analyses published in peer reviewed journals.
- Online published guidelines.
- Treatment manuals.
CBT
an example of an EST
- In general, the evidence-base of CBT is very strong.
- The strongest support exists for CBT of anxiety disorders, somatoform disorders, bulimia, anger control problems, and general stress.
- CBT techniques = cognitive restructuring, activity scheduling and behavior activation, behavioral experiments, role playing and relaxation exercises.
strengths of evidence-based working
- Clients receive therapies that are safe, consistent, and cost-effective.
- Evidence improves patient outcomes. IAT example = results:
o Depression = no difference in the recovery rates associated with CBT and counselling. Guideline = CBT & counselling.
o GAD = CBT was associated with a higher recovery rate than counselling. Guideline = CBT, no counselling.
- Evidence reduces effects of therapist bias.
o Anchoring bias = first point of information influences later decisions.
o Confirmation bias = seek out information that confirms beliefs.
o Recency bias = greater importance given to recent event.
o Sunk Cost Effect = commitment to a course of action in which we have made a substantial prior investment of resources.
Challenges to evidence-based working
- Generalizability of findings = comorbidity and minority populations.
- Differences in processes = symptom alleviation versus coping and search for meaning.
- Limitations of scientific research.
- Rigid use can ignore other tools.
- Burden of time and money.
- Sometimes there are no (relevant) guidelines available = scientific literature or expert opinion.
Resistances to evidence-based working
= ESTs are often not implemented in clinical practice.
- Less than 5% of adults with depression or anxiety disorders were receiving an empirically supported psychological therapy in 2007 in the UK.
- Practitioners find other sources more relevant e.g. colleagues, intuition, how-to books, workshops.
. Naïve realism (sources of resistance ebt)
= the world is exactly how we see it. “The patient got better therefore the treatment was effective”. But don’t forget causes of spurious therapeutic effectiveness (CSTEs).
CSTEs = placebo effects, spontaneous remission, regression to the mean, effort justification, multiple treatment interference.
Myths and misconceptions regarding human nature (sources of resistance)
Myths about memory and memory recovery.
Myths regarding the primacy or early experience.
Myths regarding effective interventions.
The application of group probabilities to individuals (sources of resistance)
= “Every individual is unique, results from RCTs won’t apply to my patient.”
But statistical prediction is virtually always equivalent, if not superior, to clinical prediction.
Reversal of the onus of proof (sources of resistance)
= “EBP is unfair because certain excluded treatments have not yet been studied sufficiently and therefore may be effective.”
But the burden of proof rests on the proponents rather than the sceptics of assertions.
Pragmatic, educational, and attitudinal obstacles (sources of resistance)
= time, training manuals, steep learning curve, statistical complexity, ivory tower mentality.
How to “fight” resistances to EBP = recommendations
- Improvements of educational training of future psychologists.
- Improvement of methods of information dissemination.
Scientific evidence should be the only factor that a therapist takes into consideration when making clinical decisions.
- Working in an evidence-based way means that the client is treated in a safe and effective way.
- Research should therefore form the basis of our clinical decisions.
- As a field we should work to fight misconceptions and resistance to evidence- based working. But evidence-based working is not without challenges. We therefore also need to
- Practice “flexibility within fidelity”. - Bridge the science-practitioner gap.