Case 4: Nabil Assad - Strep Pharyngitis
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
Virus
Small infectious particle relying on host cell to reproduce
Cannot reproduce without host cell
Virus Structure
Capsid: Protein shell around nucleic acid
Nucleocapsid: Capsid + nucleic acid
Envelope: Lipid membrane around capsid
Matrix Proteins: Connect envelope to capsid
No Envelope = Nonenveloped
Shape:
Helical: Capsid proteins around nucleic acid in spiral rod
Icosahedral: 20-sided shell surrounding capsid
Complex: Abnormal shapes
Virus Classifications
Baltimore Classification System: By genome and replication strategy
Class I: dsDNA
Class II: ssDNA
Class III: dsRNA
Class IV: + sense ssRNA
Class V: - sense ssRNA
Class VI: Reverse transcription RNA
Class VII: Reverse transcription DNA
Bacteria
Unicellular prokaryotes
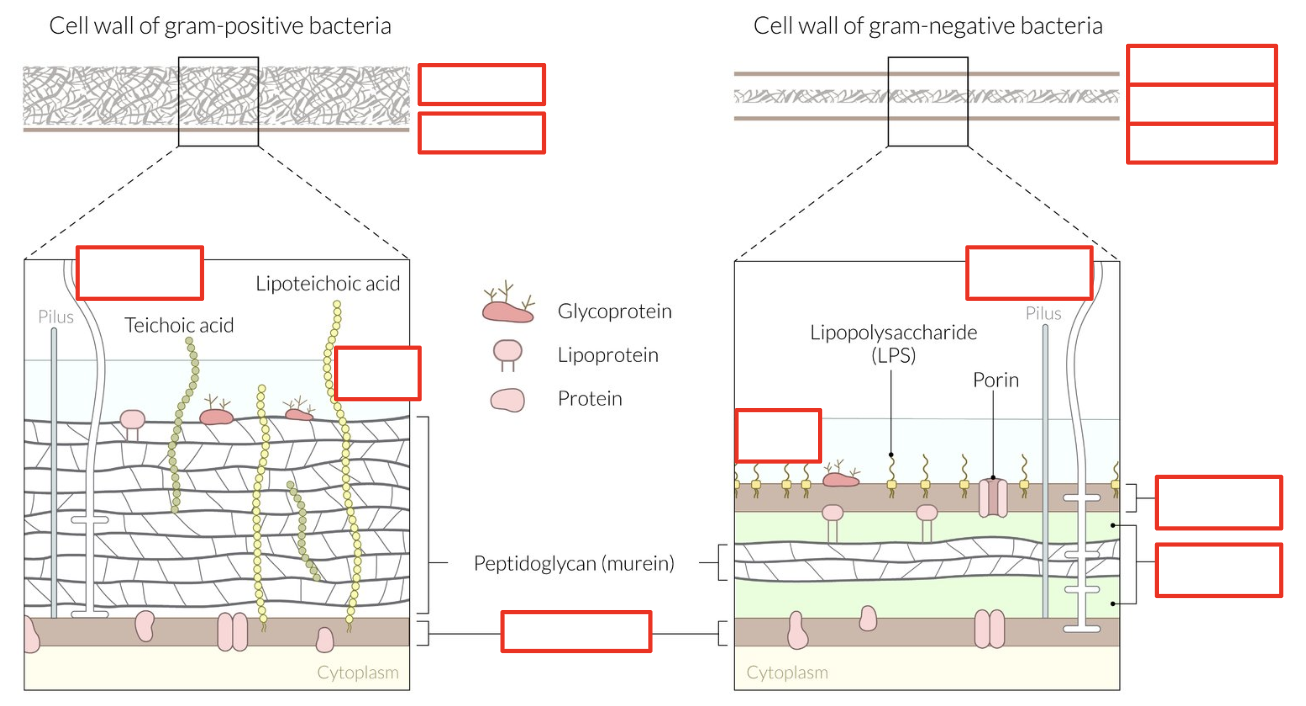
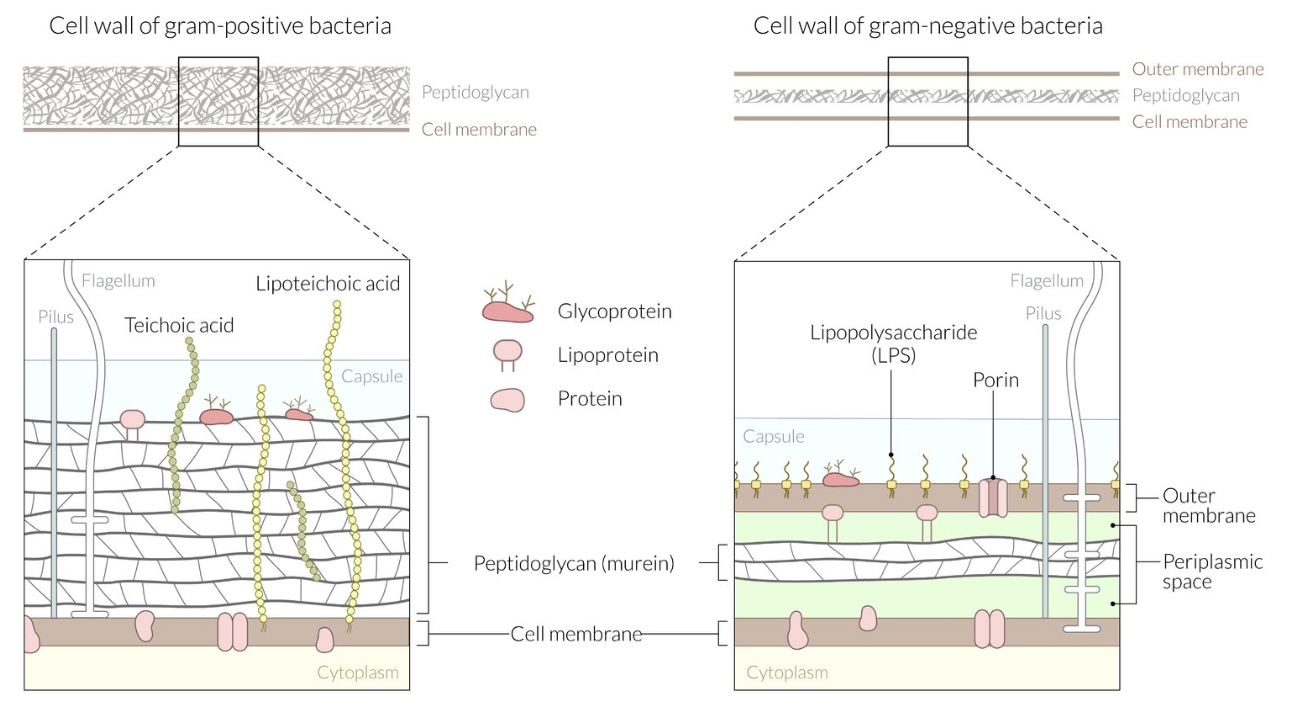
Bacteria Structure
Cell Wall: Peptidoglycan
Gram+ only
Outer Membrane: Endotoxins and phospholipids
Gram- only
Cytoplasmic Membrane: Phospholipid bilayer
Capsule: Polysaccharide layers
Glycocalyx: Polysaccharide slime layers
Periplasm: Space between outer and cytoplasmic membranes
Contain peptidoglycan and beta-lactamase
Gram- only
Flagellum: Protein tail
Pilum/Fimbria: Glycoprotein appendage
Endospores: Form spores
Gram+ only
Bacteria Classification
Gram staining
Shape
O2 requirements
Spore formation
Bacteria Classification: Gram Staining
Identifying cell wall
Gram+: Purple
Cell wall trap iodine/crystal violet stain
Gram-: Pink
No cell wall trap crystal violet stain (eluted with alcohol)
Bacteria Classification: Shape
Cocci: Sphere
Most gram+
Bacilli: Rod
Most gram-
Vibro: Curved
Spirilla: Spiral
Bacteria Classification: O2 Requirements
Obligate Aerobes: Require O2
Facultative Anaerobes: Can use O2 or not
Obligate Anaerobes: Harmed by O2
Aerotolerant Anaerobes: Tolerate O2 but cannot use
Microaerophiles: Require low conc O2
Bacteria Classification: Spore Formation
Endopores: Spores produced inside cell
Exospores: Spores produced outside cell
Non-Sporing: No spore production
Antibiotics
Treat bacterial infections
Indications:
Clear bacterial etiology
NOT for acute cough, bronchitis, sore throat
Overprescription increase MDR risk
Innate Immune System
Broad, non-specific response
Innate: Granulocytes
Neutrophils: WBC
Eosinophils: WBC
Basophils
Granulocytes: Neutrophils
Recognize antigens
Phagocytic
Produce bactericides (AMPs) → Cytotoxic
Granulocytes: Eosinophils
Secrete proinflammatory cytokines
Activate mast cells
Secrete anti-pathogen proteins (AMPs)
Granulocytes: Basophils
Produce histamine and heparin (prevent blood clot)
Innate: Natural Killer (NK) Cells
Lymphocyte detecting MHC class I (pathogenic host cells)
Cytotoxic: Release cytokines for cell lysis
Innate: Mast Cells
In interstitial connective tissue
Receptors for Fc portion of IgE antibodies
Allergen contact = IgE degranulate cell for histamine secretion and inflammation
Innate: Antigen-Presenting Cells (APCs)
Present surface peptides via MHC class I and II
APC: Monocytes
Differentiate into macrophages
Activate adaptive immune system
APC: Macrophages
Phagocytic
APC: Dendritic Cells
Express MHC class I and II + Fc receptors
Activate adaptive immune system
Phagocytic
Adaptive Immune System
Delayed, specific response
Adaptive: T-Cells
Cell-mediated response
Express antigen-specific T-cell receptors (TCR) to recognize antigen fragment presented on MHC on APCs
Cytotoxic T-cell (MHC I) → Detect intracellular (viruses)
Helper T-cell (MHC II) → Detect extracellular (bacteria)
Adaptive: B-Cells
Humoural response
Produce antigen-specific antibodies
URT Defense Mechanisms
Physical barriers
Chemical barriers
Biological/cellular barriers
Physical Barriers: Epithelial Cells
Prevent pathogen entry into submucosa
Smoking disrupts cell barrier
Physical Barrier: Mucus
Secreted by epithelial cells
Trap and remove pathogens via mucociliary escalator
Winter/smoking = More dry = Less efficient
Cilia sweep mucus towards pharynx and mouth for swallowing/expectorating
Chemical Barriers: Antimicrobial Peptides (AMPs)
Secreted by neutrophils and epithelial cells
Defensins: Chemotactic
Lactoferrin: Modulate inflammatory cytokine production
Biological Barriers: Respiratory Tract Microbiota
Resident symbiotic organisms in resp tract
Prevent pathogen entry
Smoking/drugs = Dysbiosis = Increase infections
Biological Barrier: Innate Immune Cells
Inflammation
Phagocytosis
Lymphatic System: Transport antigens and APCs from mucosa to lymph nodes for adaptive immune activation
Swelling from immune cell proliferation
URT Viral Infections: Manifestation
More common
Signs:
Nasal congestion
Cough
Sneezing
Sore throat
Low-grade fever
URT Viral Infections: Transmission
Droplets: Large particles, short-range
Aerosols: Fine particles, long and short-range
Direct Contact: Short-range
Indirect Contact: Fomites, long and short-range
URT Viral Infections: Pathogenesis
Rhinovirus:
Replicate in posterior nasopharynx epithelial cells
Short incubation
Influenza:
Replicate in tracheobronchial epithelial cells
More damage
URT Viral Infections: Treatment/Management
NO antibiotics
Self-limiting
Supportive Measures:
Rest, hydrate
NSAIDS/acetaminophen for pain
Antihistamines/decongestants
URT Bacterial Infections: Manifestations
Similar to viral
Differences:
Persistent symptoms (> 10 days)
Severe onset (high fever, prolonged nasal discharge)
Worsening symptoms after improving (double-sickening)
URT Bacterial Infections: Transmission
Opportunistic → Dysbiosis
URT Bacterial Infections: Pathogenesis
Secondary infection after viral infection
Inflammation
Decrease tissue O2
Bacteria colonize mucosal surfaces to impair microbiota
URT Bacterial Infections: Treatment/Management
Antibiotics
Symptom management same as viral
Common Cold Viruses
Rhinovirus (most common)
Influenza
Parainfluenza
Coronavirus
Adenovirus
Respiratory syncytial virus
Common Cold: Rhinovirus
Inactivated by gastric acid
Infection limited to nasopharynx + resp epithelium
Group A Streptococcal (GAS) Pharyngitis: Description
Sore throat from pharynx inflammation (strep throat)
Fever
Enlarged tonsils + exudate
GAS Pharyngitis: Epidemiology
Most common strep throat cause (in children)
GAS Pharyngitis: Etiology
Group A beta-hemolytic Streptococcus
Streptococcus pyogenes
GAS Pharyngitis: Pathogenesis
Evade immune system with:
Virulence factors (prevent phagocytosis)
Toxin production
Adaptive mechanisms: Pili adhere to pharyngeal epithelium, antibiotic resistance
GAS Pharyngitis: Investigation
Not needed unless high risk
Rapid antigen detection test
Throat culture
Nucleic acid amplification test (ex: PCR)
GAS Pharyngitis: Clinical Presentation
Differentiate viral and bacterial pharyngitis
Centor Score:
+1 for each criteria
Fever
Tonsil exudate
Lymph node swelling
No cough
+1 point for < 15 years
-1 point for > 45 years
0-1 Points: Low risk
3-4 Points: Increased risk
GAS Pharyngitis: Treatment/Management
Usually self-limiting
Supportive Care:
Fluid
Analgesics
Antibiotics if lab confirmed
Penicillin
Amoxicillin
GAS Pharyngitis: Complication of Not Treating
Acute rheumatic fever
Autoimmune reaction causing carditis (heart inflammation) and arthritis
Infection Causing Airway Obstruction
Mostly from self-limiting viral laryngotracheobronchitis
Edema
Pus in abscess (dead + alive immune cells) → Must drain
Infection Causing Airway Obstruction: In Children
Common
Narrow subglottic + epiglottic regions
Soft cartilage
Infection Causing Airway Obstruction: In Adults
Glottic region
Cough Indication of Location
URT/Extrathoracic:
Barky/hoarse cough
Stridor
Voice hoarseness
LRT/Intrathoracic
Dry or productive cough
Wheezing
More persistent