Chronic Kidney Disease
1/150
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
151 Terms
How is chronic kidney disease defined?
Abnormalities of kidney structure or function present for at least 3 months with health implications
What are some markers of CKD?
- albuminuria (Albumin:Cr ratio ≥30)
- urine sediment abnormalities
- persistent hematuria
- electrolyte and other abnormalities due to tubular disorders
- abnormalities detected by histology
- structural abnormalities detected by imaging
- history of kidney transplant
- GFR < 60
What are some common comorbidities associated with CKD?
1. HTN
2. DM
3. Cardiovascular disease
4. Previous AKI/AKD
What are some other risk factors of CKD?
1. GU disorders - recurrent kidney calculi
2. Chronic inflammatory conditions - lupus, vasculitis, HIV
3. Exposure to nephrotoxins or radiation
4. Family history/genetics - polycystic kidney disease, APOL-1, Alport syndrome
5. Eclampsia
6. Preterm birth
7. Environmental exposures/toxins
Describe the recommendations for CKD screening
No current recommendations for at-risk patients except for patients with diabetes (annual)
How does CKD usually present?
Often asymptomatic, especially in early stages. Symptoms don't usually develop until G4-5
What are some symptoms/signs of CKD?
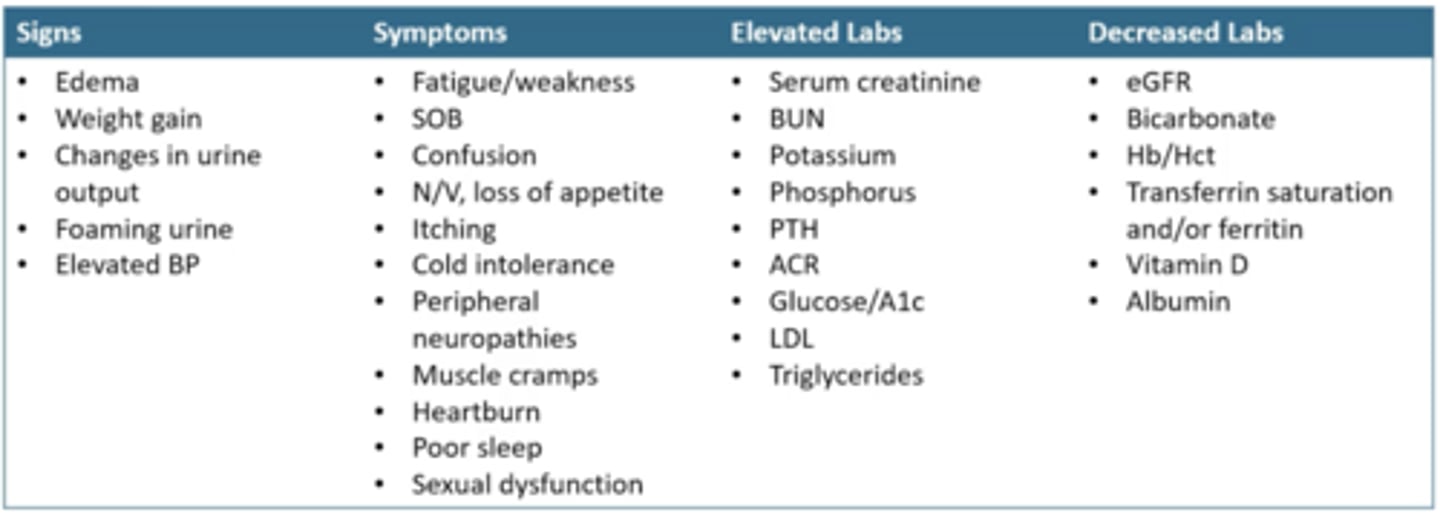
What 3 things do we look at when classifying CKD?
1. Cause
2. GFR
3. Albuminuria
What 3 things are considered when looking at the cause of CKD?
1. Primary
2. Congenital/genetic
3. Secondary to systemic disease
How is CKD classified based on GFR?
G1 = ≥90, normal/high
G2 = 60-89, mildly decreased
G3a = 45-59, mildly/moderately decreased
G3b = 30-44, moderately/severely decreased
G4 = 15-29, severely decreased
G5 = <15, kidney failure
In which populations/conditions might we see an increase in creatinine production?
1. Extreme sports/body builders
2. Class III obesity
3. High protein diet/creatinine supplementation
In which populations/conditions might we see a decrease in creatinine production?
1. EDs
2. Above knee amputation
3. Spinal cord injury
4. Low protein diet
5. Malnutrition
6. Elderly
Which medications can lead to an inaccurate reading of Cr based GFR?
1. Anabolic steroids
2. Cimetidine
3. Trimethoprim
4. Rilpivirine
5. Dolutegravir
6. Cobicistat
7. Pyrimethamine
8. Amiodarone
Which chronic conditions can lead to an inaccurate reading of Cr based GFR?
1. Cancer
2. HF
3. Cirrhosis
4. Catabolic consuming diseases
5. Muscle wasting diseases
When is cystatin C used to estimate GFR?
When the patient has a condition/medication that might impact the accuracy of creatinine measurement
What is cystain C?
A protease inhibitor produced by all nucleated cells
How is cystatin C different from creatinine?
It's production is not affected by muscle mass
How/why do concentrations of cystatin C vary person to person?
Concentrations can be altered by age, nutritional status, gender, weight, height, smoking, CRP levels, steroids, and rheumatoid arthritis
When is eGFRcys considered?
- Eating disorders
- Extreme exercise
- Medications that decrease tubular secretion (cimetidine, trimethoprim)
- Broad spectrum antibiotics that decrease extra-renal elimination
When is eGFRcr-cys considered?
- Above knee amputation
- Spinal cord injury
- Class III obesity
- Chronic illness (HF, cirrhosis, cancer)
- Anabolic steroid use
What conditions impact BOTH creatinine and cystatin C?
- Smoking
- Very low muscle mass
- Hypo- and hyperthyroidism
- Glucocorticoid excess (high catabolic states like in serious infection or inflammation, high dose steroid use)
- Chronic inflammation (insulin resistance, elevated CRP/TNK, low albumin)
When is a measured GFR considered?
When their are possible inaccuracies/conditions that impact BOTH creatinine and cystatin C
Describe the benefits to mGFR
- Best index of kidney function
- Accurate in all situations
- Identifies early changes in GFR
- Less impacted by non-GFR determinants
How is mGFR determined?
Administration of exogenous marker (inulin, iothalamate, iohexol, EDTA, or DTPA) with measure of plasma and urinary clearance
What are 4 limitations to mGFR?
1. Expensive
2. Time consuming
3. Invasive
4. Not routinely available
What are the main non-GFR determinants of creatinine and cystatin C that are considered before using mGFR?
1. Catabolic states (serious infection or inflammatory states)
2. High cell turnover (cancer)
3. Advanced cirrhosis or HF
4. High dose steroids
5. Very frail
When is mGFR used?
When non-GFR determinants of creatinine and cystatin C are present AND there is a need for greater accuracy (transplant evaluation, donor candidacy, drug dosing is narrow therapeutic index with serious toxicity like chemo)
How is CKD classified using albuminuria (Albumin to Creatinine ratio or ACR)
A1 = <30, normal-mildly increased
A2 = 30-300, moderately increased
A3 = >300, severely increased
What is the KDIGO recommended A1c goal for preventing CKD in diabetes?
<6.5-8% (depends on risk factors, higher risk, higher A1c goal)
What is the KDIGO recommended BP goal for preventing CKD in HTN?
SBP <120 mmHg (at least <130/80)
Besides diabetic and HTN risk factors, what other ways can we prevent CKD?
1. Albuminuria - strong predictor of accelerated progression
2. Smoking - reduces GFR and increases albuminuria
3. Obesity - BMI ≥25 at 20 years increases risk x3
In all patients with CKD, Albumin:Cr ratio should be monitored...
at least annually, more frequent if higher risk for progression
When is Albumin:Cr ratio monitored more frequently than annually?
G3a-b = every 6 months
G4 = every 3 months
G5 = every 6 weeks
What non-pharm lifestyle modifications are recommended for CKD?
1. Healthy diet (DASH, mediterranean) with Na restriction <2 g/day, protein intake 0.8 g/kg/day if CKD G3-5
2. Physical activity - mod intensity 150 min/week
3. Stopping tobacco and limiting alcohol to <2 drinks/day for men, <1 for women
4. Weight management - weight loss if BMI >25
What are the protein recommendations if a patient has CKD stage G3-5?
0.8 g/kg/day
What are the 1st line pharm therapy options for CKD?
1. SGLT2i
2. +/- RAS inhibitor for HTN
3. Mod/high intensity statin
When is a RAAS inhibitor recommended?
- CKD G1-4 with A2-3 with or without diabetes
- CKD + compelling indication (HTN, HF)
What is the benefit of a RAAS inhibitor in CKD?
- Delayed progression to kidney failure
- Reduced proteinuria
- Reduction in adverse renal and CV events
When is a RAAS inhibitor not usually recommended?
CKD G5 - kidney failure
What are 2 RAAS inhibitors?
ACEi and ARB
What is the MOA of ACEi and ARB, respecitively?
ACEi - blocks conversion of AT-I to AT-II in RAAS pathway and blocks degradation of bradykinin
ARB - blocks AT-I receptor, inhibiting AT-II from all pathways
What are the effects of angiotensin II?
Potent vasoconstrictor that stimulates aldosterone secretion, increases Na and H2O reabsorption, and increases potassium loss
Blocking AT-II leads to...
- vasodilation of efferent arteriole
- decreased glomerular hyperfiltration
- decreased intraglomerular pressure
What are the recommended dosing strategies for ACEi/ARBs?
- Start at lowest recommended dose
- Titrate to max tolerated
What are the therapeutic goals for ACEi/ARBs?
- SBP <120 mmHg
- 30-50% reduction in albuminuria
What are 4 contraindications of ACEi/ARBs?
1. Pregnancy
2. Bilateral renal artery stenosis
3. History of angioedema (mainly with ACEi)
4. Concomitant ACEi/ARB or direct renin inhibitor
What are 5 AEs for ACEi/ARBs?
1. Acute kidney injury - Cr increase 20-30% from baseline
2. Angioedema - typically within first week
3. Bradykinin cough - switch to ARB
4. Hyperkalemia
5. Hypotension - reduce dose or D/C
How should the ACEi/ARB dose be adjusted with normokalemia and a <30% decrease in eGFR?
This is fine, increase dose of ACEi/ARB or continue on max tolerated
How should the ACEi/ARB dose be adjusted with hyperkalemia?
Review concurrent drugs, moderate dietary intake, and consider diuretics, sodium bicarbonate, and potassium binders. Reduce or stop ACEi/ARB if mitigation strategies are ineffective
How should the ACEi/ARB dose be adjusted with a ≥30% decrease in eGFR?
Review for causes of AKI, correct volume depletion, reasesses concomitant meds (diuretics, NSAIDs), consider renal artery stenosis. Reduce or stop ACEi/ARB if mitigation strategies are ineffective
SGLT2-inhibitors are often continued until...
Dialysis or kidney transplant
Describe the place in therapy for SGLT2is?
- CKD + T2DM + eGFR ≥20
- CKD + eGFR ≥20 + urine ACR ≥200
- CKD + HF
- CKD + eGFR 20-45 + albuminuria
What are the benefits of SGLT2i in CKD?
- slow progression of kidney disease - equivalent to 15 years freedom from kidney failure in T2DM
- reduce need for dialysis or transplant
- decrease risk of AKI in CKD
- reduced risk of CV mortality or HF hospitalization
What is the MOA of SGLT-2i?
Decrease glucose and Na reabsorption in the proximal tubule of the kidney thereby decreasing glomerular hyperfiltration and reducing glomerular hypertension
Describe dosing of SGLT-2is
- Different from in diabetes
- Canagliflozin 100 mg PO qd
- Dapagliflozin 10 mg PO qd
- Empagliflozin 10 mg PO qd
Which patients were excluded from Canagliflozin trails? Do NOT give when...
eGFR <30
Which patients were excluded from Dapagliflozin trials? Do NOT give when...
eGFR <25
Which patients were excluded from Empagliflozin trials? Do NOT give when...
eGFR <20
If a patient starts on a SGLT2-i and THEN their eGFR drops below that medications specific studied threshold, what should be done?
2024 KDIGO recommendation: continue once started until no longer tolerated or initiation of RRT
SGLT2-is be avoided in patients with...
- T1DM
- Increased risk for volume depletion
- Mycotic genital infections (chronic yeast infections, history of Fournier's gangrene)
- Indwelling Foley catheters
When should SGLT2-is be held/paused?
- Hold 3 days prior to surgery/procedures requiring 1+ days in hospital
- Hold during illness, excessive exercise, or alcohol intake
What are some AEs of SGLT2-i?
1. Euglycemic DKA
2. Acute kidney injury
3. GU fungal infections and UTI
4. Hypotension/hypovolemia
5. Lower limb amputations (canagliflozin)
Describe euglycemic DKA
- BG <250
- Higher risk if on insulin
- Precipitating events: dehydration, infection, surgery, changes in insulin dose
- Symptoms = N/V, abdominal pain
Describe acute kidney injury changes seen with SGLT2-i
- Due to osmotic diuresis caused by Na and glucose excretion
- Early decrease in eGFR which stabilizes in about 4 weeks, no need to D/C
- Lower incidence of AKI than placebo
- Risk factors = hypovolemia, HF, concomitant nephrotoxins
What GU infection is cause to D/C a SGLT2-i?
Fournier's Gangrene. Required surgical intervention and IV antibiotics. Notify provider if pain, tenderness, erythema, swelling in genital or perineal area with fever and/or malaise
What should be monitored when on a SGLT2-i?
- Routine monitoring schedule for CKD
- Blood glucose
- Volume status
- Signs/symptoms of diabetic foot infection
- Signs/symptoms of GU infection
Who are statins indicated for in CKD?
- Age ≥50 with ANY stage CKD (G1-5) not treated with dialysis or kidney transplant
- Age 18-49 with CKD and no dialysis or transplant PLUS 1+ of the following: known coronary disease, DM, prior ischemic stroke, estimated 10 year incidence of coronary death or nonfatal MI >10% using PREVENT calculator
- Follow AHA guidelines
Finerenone is a _____ line treatment for CKD
second
What type of drug is Finerenone?
Nonsteroidal Mineralocorticoid Receptor Antagonist (nsMRA)
Describe the place in therapy for Finerenone
Add-on treatment for T2DM + eGFR >25 with normal K + ACR >30 despite max tolerate dose of ACEi/ARB
What are the benefits of Finerenone?
Reduced risk of CKD progression and CV events (FIDELIO)
What is the MOA of Finerenone?
Blocks Na+ reabsorption and mineralocorticoid receptor (MR) overactivation, preventing fibrosis and inflammation responsible for end organ damage. It has a high potency and selectivity with no affinity for androgen, progesterone, estrogen, and glucocorticoid receptors
Dosing for Finerenone is based on what 2 things?
eGFR and K+
How should Finerenone be dosed if K+ ≤4.8?
- 10 mg qd if eGFR 25-59
- 20 mg qd if eGFR ≥60
- Restart K+ (10 mg) if previously held for hyperkalemia
How often should K+ levels be checked when starting Finerenone?
1 month after start and then every 4 months
How should Finerenone be dosed if K+ 4.9-5.5?
Continue 10 mg or 20 mg
How should Finerenone be dosed if K+ >5.5?
- Hold Finerenone
- Consider diet/med adjustments to mitigate hyperkalemia
- Consider reinitiation if/when K+ ≤5.0
What are 3 contraindications to Finerenone?
1. Concomitant strong CYP3A4 inhibitors (azoles, protease inhibitors, grapefruit juice)
2. Adrenal insufficiency
3. Serum potassium >5.5
What are some AEs to Finerenone?
1. Hyperkalemia
2. Increased creatinine
How is resistant HTN managed in CKD?
- Maximize diuretic therapy
- Add spironolactone
- Per AHA guidelines
GLP-1s are ________ line therapy for CKD
second
Describe the place in therapy for GLP-1 agonists in CKD
Add-on treatment for CKD + T2DM not meeting glycemic targets despite metformin + SGLT2-i
What are the benefits of GLP-1 agonists?
- Reduce CV morbidity and mortality in T2DM + pre-existing CV disease
- Reduced new onset albuminuria
Which GLP-1 agonists are recommended in CKD? No renal dose adjustments
1. Dulaglutide 0.75 mg and 1.5 mg once weekly
2. Liraglutide 1.2 mg and 1.8 mg once daily
3. Semaglutide 0.5 mg and 1 mg once weekly
What are 8 AEs of GLP-1 agonists?
1. N/V/D - slow and low
2. injection site reactions
3. Antibody formation
4. Hypersensitivity
5. Retinopathy
6. Cholecystitis/cholelithiasis
7. Medullary thyroid carcinoma
8. Pancreaitis
Why is metabolic acidosis a common complication of CKD?
As GFR decreases below 60, the kidneys ability to excrete hydrogen ions and generate bicarbonate decreases
What is a normal serum bicarbonate range?
22-29 mEq/L
How is metabolic acidosis treated?
Oral sodium bicarbonate, but no evidence of improved outcomes with CKD
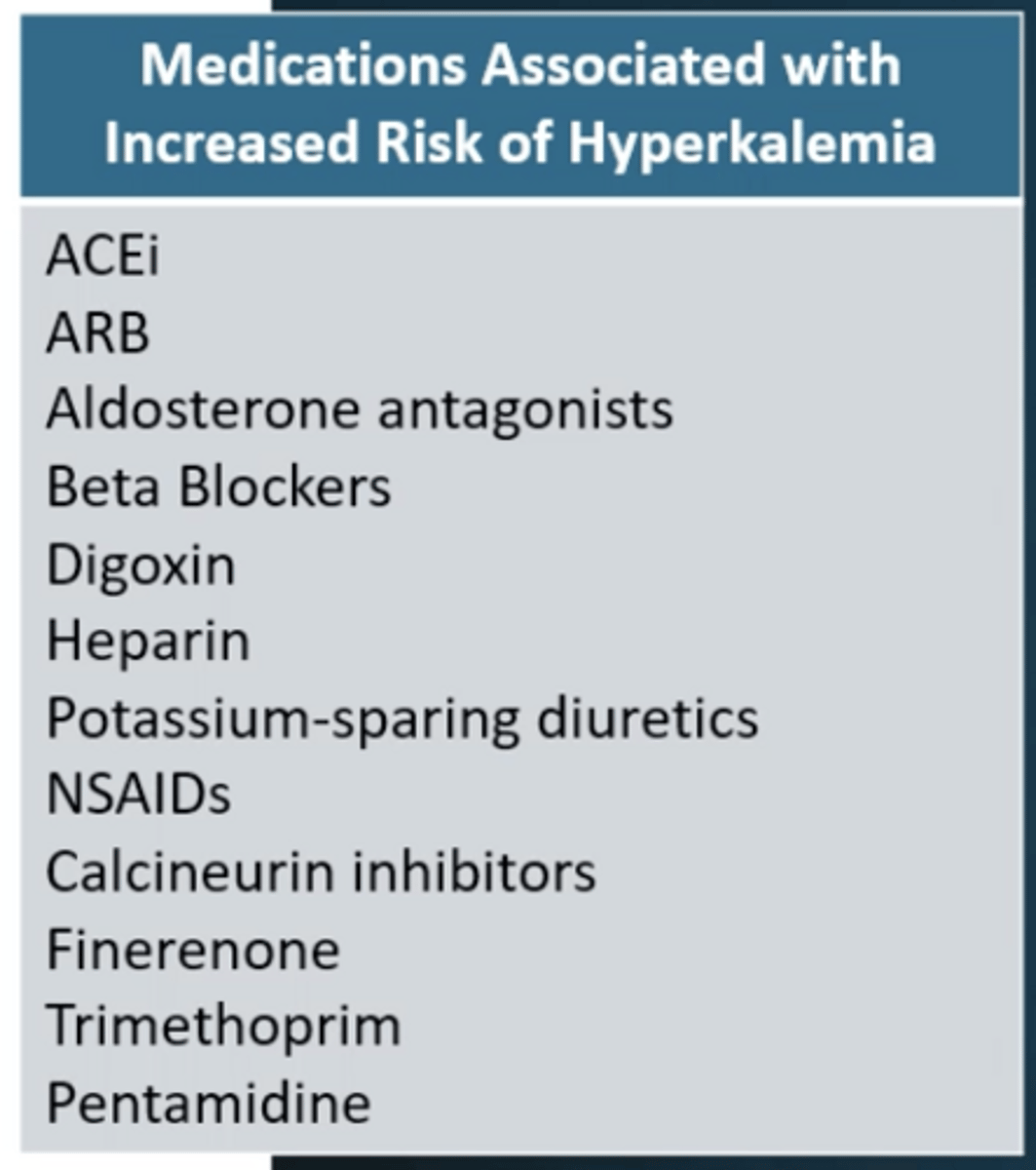
What are some meds that increase the risk of hyperkalemia?
What is 1st line treatment for hyperkalemia?
Address correctable factors by reviewing non-RASi meds (NSAIDs, trimethoprim) and assess/change dietary intake
What are some 2nd line treatment options for hyperkalemia?
- Diuretics
- Optimize serum bicarbonate levels
- Potassium exchange agents
What are some last line treatment options for hyperkalemia?
Reduce dose or D/C RASi/MRA
What are some agents used to treat chronic hyperkalemia?
1. Sodium polystyrene sulfonate (Kayexalate) - Na/K exchange resin. Rectal enema possible, intestinal necrosis is AE, separate by 3 hr
2. Patiromer (Veltassa) - Ca/K exchange polymer, separate by 3 hr
3. Sodium zirconium cyclosilicate (Lokelma) - Traps K+ in exchange for H+/Na+ - more predictable, reliable, and quick, separate by 2 hr
What are some agents used to treat acute hyperkalemia?
Calcium gluconate
Albuterol
Bicarbonate
Insulin/Glucose
Kayexalate/Lokelma
Diuretic
Incidence of what blood condition increases in CKD?
Anemia
Why is anemia a complication of CKD?
In CKD, kidney oxygen consumption decreases. EPO-producing cells are tricked into thinking the body has enough O2, despite systemic hypoxia. Iron deficiency, resistance to EPO signaling, and shortened RBC lifespan also contributes
What are some consequences of anemia from CKD?
- Left ventricular hypertrophy
- Transfusions
- Hospitalizations
What kind of iron supplementation is preferred in hemodialysis?
IV, 1 g in divided doses
What are some AE of iron supplementation?
- Hypersensitivity/anaphylaxis (iron dextran)
- Hypotension
- Dizziness
- Nausea
- Dyspnea
- HA
- Lower back pain
- Arthralgia
- Syncope
- Arthritis
When should iron supplementation be held?
- Ferritin ≥700 ng/mL
- TSAT ≥40%