Psychopathology Quiz 2
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
72 Terms
Histrionic Personality Disorder
· Histrionic Core Features: A pattern of excessive emotionality & attention seeking
o Primary impairment is interpersonal
Narcissistic Personality Disorder
A pervasive pattern of grandiosity (in fantasy or behavior), need for admiration, and lack of empathy,
Conduct Disorder
· CD Core Features: A pattern in which the basic rights of others or major age-appropriate societal norms or rules are violated. Areas include:
o Aggression to people or animals (bullies, physically cruel, stolen)
o Destruction of property (fire setting, destroyed property)
o Deceitfulness or theft (broken into place, lies to get goods, stolen)
o Serious violation of rules (stays out, run away, truant from school)
· Note: ODD often precedes CD
Oppositional Defiant Disorder
· ODD Core Features: A pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness (not w/ sibling). Areas include:
o Angry/irritable mood (angry, annoyed, lose temper)
o Argumentative/defiant behavior (argues, deliberate annoyance, defies)
o Vindictiveness (spiteful)
Antisocial Personality Disorder (ASPD)
· ASPD Core Features: Pattern of disregard for and violation of the rights of others. MUST be 18 and have evidence of Conduct Disorder before age 15.
· Characteristics:
o Failure to conform to social norms
o Deceitful
o Impulsive
o Irritable & aggressive
o Lack of remorse
· Note: In AMPD, ASPD contains Antagonism traits & Disinhibition traits
Intermittent Explosive Disorder (IED)
· IED Core Features: Recurrent behavioral outburst representing a failure to control aggressive impulses. Must be either:
o Verbal aggression or physical aggression toward property, animals, or individuals that happens 2x weekly for 3 months (NOTE: the physical aggression doesn’t result in damage, injury, or destruction)
o 3 behavioral outbursts involving damage to property and/or physical assault involving injury against individuals or people within 1 yr period
Attention-Deficit/Hyperactivity Disorder (ADHD)
· ADHD Core Features: Pattern of inattention and/or hyperactivity-impulsivity that interferes w/ functioning or development (Note: Symptoms MUST be present before age 12 & occur in 2+ settings)
Substance-Related Disorders
o Core feature is a cluster of cognitive, behavioral, and physiological symptoms indicating that the individual continues using the substance despite significant substance-related problems
§ Applies to all except caffeine
§ 11 criteria across 4 major categories:
· Impaired control over substance use (criterion 1-4)
· Social impairment (5-7)
· Risky substance use (8-9)
· Pharmacological criteria (10-11)
· Severity is determined on # of symptoms
o Potential Gender Paradox where women are more effected by alcohol than men - women can experience greater health harm from alcohol use and develop AUD-related problems faster than men, even with lower consumption levels
Caffeine is NOT considered a substance disorder
Alcohol Use Disorder (AUD)
· Alcohol Use Disorder Core Features: A pattern of alcohol use leading to significant impairment or distress. Areas include:
o Tolerance – Increased amount needed OR diminished effects w/ same amount
o Withdrawal – Symptoms of withdrawal syndrome OR alcohol taken to relieve withdrawal symptoms
Obsessive-Compulsive Personality Disorder (OCPD)
· OCPD Core Symptoms: A pattern of preoccupation w/ orderliness, perfectionism, and mental and personal control, at the expense of flexibility, openness, and efficiency..
AMPD
a. AMPD is more dimensional
i. Criteria A: (Personality functioning)
1. Identity
2. Self-direction
3. Empathy
4. Intimacy
ii. Criteria B: (Personality Traits)
Gore wrote that Histrionic should be considered…
a. Histrionic PD must be understood via antagonism and extraversion
Histrionic AMPD
i. Criteria A: (Personality functioning)
1. Identity
2. Self-direction
3. Empathy
4. Intimacy
ii. Criteria B: (Personality Traits)
1. Psychological Traits – MUST have both grandiosity & attention-seeking
Miller - NP Factor Model
Factor Models:
a. One Factor: General Narcissism dimension
b. Two Factor: Grandiose & vulnerable
c. Three Factor: Antagonism & Agentic & Narcissistic neuroticism
Miller - NP Two Factor Model Findings
a. There is a fluctuation between grandiosity vs vulnerability
One Factor: General Narcissism dimension
Two Factor: Grandiose & vulnerable
Three Factor: Antagonism & Agentic & Narcissistic neuroticism
Miller - NP - AMPD Criteria B vs. A
A. a. Overall: Criteria B explains NP more than Criteria A. DSM-5 AMPD provides a reasonable framework for assessing NPD, especially grandiose narcissism. Vulnerable narcissism is harder to capture, requiring specifiers (e.g., depressivity, anxiousness).
A. Experts rated grandiosity as most central to NPD, followed by manipulativeness, callousness, risk-taking, attention seeking, and hostility
a. DSM-5 AMPD Criterion B traits capture grandiose narcissism well but leave much variance unexplained for vulnerable narcissism.
Beauchaine & McNulty - CD & ODD - overall point
a. Overall: Externalizing disorders are not separate entities but developmental expressions of shared vulnerabilities. Trait impulsivity, shaped by dopamine dysfunction and environmental risks, drives continuity from ADHD in childhood to antisociality in adulthood.
Beauchaine & McNulty - CD & ODD - Multilevel Developmental Model = model of early-onset externalizing behavior
i. The model of early-onset externalizing behavior in which comorbidities and continuities are viewed as ontogenic processes: products of complex longitudinal transactions between interdependent individual-level vulnerabilities and equally interdependent contextual risk factors. Through interactions across levels of analysis, some individuals traverse along the externalizing spectrum, beginning with heritable trait impulsivity in preschool and ending in antisociality in adulthood.
i. Externalizing disorders share common higher-order vulnerability heritable trait impulsivity
ii. Trait comes from genetic factors mesolimbic dopamine dysfunction (dopamine is lower so engage in more extreme behaviors)
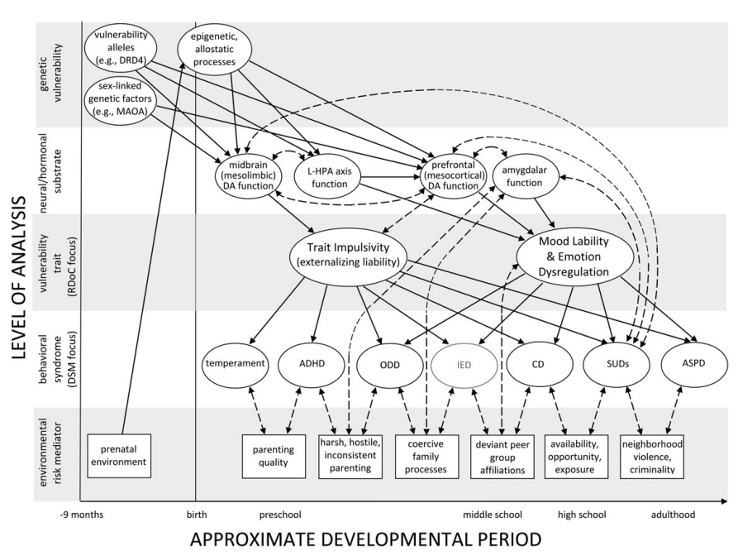
Beauchaine - ODD & CD morst heritable trait
i. Trait impulsivity is highly heritable genetic vulnerability that predisposes kids to ADHD and CD
Beauchaine - ODD & CD Vulnerability X Environmental Context Model
a. Vulnerability X Environmental Context Model:
i. Inherited impulsivity interacts w/ environmental experiences (and is met w/ weak or strong emotion reg skills)
ii. Inherited Impulsivity - High-risk environment - weak emotion reg - ADHD + ODD - deviant peers - ADHD + CD - Antisocial personality traits
iii. Inherited Impulsivity - Protective environment - strong emotion reg - healthy peers - ADHD only Socialized, regulated impulsivity
Frick - ODD & CD Traits finding
a. Purpose: Research on the use of callous and unemotional (CU) traits for designating an important subgroup of children and adolescents with severe conduct problems.
Findings:
a. Callous and unemotional traits are moderators for CD
B. Kids with both severe conduct problems and elevated CU traits are at risk for more severe and persistent antisocial outcomes
Beauchaine - ASPD shared etiology w/ BP
a. Purpose: ASPD and BPD may share common etiology rooted in trait impulsivity and emotion dysregulation
a. Main neurotransmitters: Dopamine & serotonin dysfunction serves as principle vulnerability for both ASPD & BPD
a. Double Vulnerability: Relationship between two neurotransmitters. High impulsivity w/ high dopamine and high trait anxiety from serotonin will make individual more vulnerable
b. High comorbidity
Beauchaine - ASPD & BPD - Sex moderated outcomes
i. Males: Impulsivity + aggression = ASPD
ii. Females: Impulsivity + self-injury = BPD
Beauchaine - ASPD & BPD - Developmental Model
a. Developmental Model:
i. Model 1: Inherited impulsivity - High risk environment - impulsivity w/ weak emotion regulation - ODD & mood dysreg - Deviant peers - Boys (CD or ASPD) OR girls (CD or BPD)
i. Model 2: Inherited impulsivity - Protective environment - impulsivity w/ strong emotion regulation - healthy peers - neighborhood cohesion - socialized/regulated impulsivity
ii. ADHD - ODD - Early-onset CD - SUDs - ASPD
iii. Biological vulnerability: Heritable impulsivity from dopamine and serotonin dysfunction
iv. Environmental reinforcement: Adverse family environments shape emotion dysregulation
b. Overall: In short: ASPD and BPD are multifinal outcomes of a shared vulnerability (impulsivity + emotion dysregulation), shaped by sex differences and adverse environments.
Wright - ASPD - Purpose
States criteria A & B overlap and that DSM doesn’t adequately represent the interpersonal side of disorders.
a. Overall: Personality disorders should be reconceptualized as interpersonal disorders, since chronic relational dysfunction is their defining feature
a. Interpersonal dysfunction is more distinct feature of PDs
Wright - ASPD - why reframe PDs as Interpersonal Disorders
i. Reduce stigma (focus on relational dysfunction)
ii. Provide clearer diagnostic boundaries, improving validity and utility of diagnosis
iii. Align diagnosis with treatments, improving effective treatments
Wright - ASPD - Contemporary Integrative Interpersonal Theory (CIIT):
i. Key features:
1. Interpersonal functioning is made of two dimensions: Agency (dominance vs submission) and Communion (warmth vs coldness)
2. Adaptive functioning = ability to flexibly balance you own needs and the needs of others across social situations
i. Agency - pursuit of your goals, how does it balance with communal goals)
Wright - ASPD - 4 Interpenetrating System
i. Behavior – Observable interactions or overt behaviors between people (varies around dominance & affiliation)
ii. Self System – Internal motives or goals related to getting ahead and getting along with others
iii. Affect System – Structures by arousal and valence, that provide information regarding satisfaction & frustration of motives
iv. Perception – Each person perceives the other and themselves, the assumption is that the interpersonally salient perceptions and their impact on the individual can be similarly organized by dominance and affiliation
Muris - ASPD - Dark Triad
a. The Dark Triad refers to three overlapping personality traits:
i. Narcissism
ii. Machiavellianism
iii. Psychopathy.
Muris - ASPD - Dark Triad traits linked to?
a. These traits are linked to malevolent, norm-violating behaviors (e.g., lying, cheating, manipulation, aggression).
a. Big 5:
i. Agreeableness was negatively associated with all 3 traits
ii. HEXACO – All 3 traits are negatively associated w/ honesty & humility
Muris - ASPD - Dark Triad trait w/ strongest link to each other?
a. Strongest link: Machiavellianism & Psychopathy
Muris - ASPD - Dark Triad trait “Super Trait”
a. Super Trait: “Malevolence” supertrait rather than 3 distinct constructs
Muris - ASPD - Dark Triad overall findings
a. Overall: The Dark Triad traits are closely related, malevolent personality features that predict a wide range of antisocial outcomes. Psychopathy may be the central driver, while narcissism is somewhat distinct/unique.
Psychopathy linked in men more
Coccaro - IED is a disorder of ___ and therefore suggests____.
a. Argues recognition of IED and emphasizes it’s a disorder of impulsive aggression
a. Suggests refinement of DSM criteria:
i. Differentiating between high-frequency/low-intensity and low-frequency/high-intensity aggression.
ii. Requiring aggression to be impulsive, not premeditated.
Coccaro - IED - Taxometric analyses suggests?
a. Taxometric analyses suggest IED has a categorical (not dimensional) structure
Coccaro - IED - Narrow vs. Broad
a. Narrow vs Broad IED:
i. Narrow = higher frequency & less severe outbursts
ii. Broad = Lower frequency & more severe outbursts
Wakefield - IED DSM changes
a. DSM-5 added verbal aggression & nondestructive property destruction
Wakefield - “False Positive Epidemic” IED
a. “False positive epidemic” – Healthy people labeled as mentally ill
b. DSM criticism as having diagnostic overreach – it over-pathologizes which leads to diagnostic inflation
i. EX: Verbal aggression as IED
ii. Under DSM criteria there would be widespread diagnosis bc severe anger attacks and verbal aggression aren’t uncommon
iii. Conceptually challenges normal distress vs. dysfunction
Hinshaw - ADHD - No Child Left Behind (NCLB)
a. schools may have been incentivized to give ADHD diagnoses to remove underperforming students from data to prevent losing funding
Hinshaw - ADHD Mechanisms
a. Mechanisms:
i. Deficits in Executive Functioning (i.e., working memory & response inhibition)
ii. Low intrinsic motivation (excessive delay aversion - unable to delay gratification)
iii. Dysregulated attentional capacity (Inability to inhibit distracting information)
Hinshaw - ADHD - Motivation & impulsivity
a. Intrinsic motivation: Insufficient arousal, related to hypodopaminergic functioning, leading to a constant need for stimulation, an aversion to delayed rewards, and a need for high levels of reinforcement to motivate performance
b. Impulsivity is core factor
Hinshaw - ADHD - Gender Paradox
a. ender Paradox: The contention of this paradox is that, for the sex or gender with lower prevalence of a given condition—such as males in regards to major depression—the disorder, when it exists, will be more severe, requiring a greater genetic vulnerability or accumulation of other risk factors to lead to its onset
i. Berkley Girls study – Found executive Functioning deficits, risk for self-harm is intensified by early maltreatment, deficits in response inhibition, maladaptive peer relationships, unplanned pregnancy, and persisting academic struggles
Faraone - ADHD Facts
a. Multifinality - is when the same vulnerability leads to multiple different outcomes
b. Environmental correlates – toxic exposure, prenatal factors, birth complications, psychosocial stressors
Nigg - ADHD Self-Regulation Purpose & key argument
a. Self-regulation encompasses cognitive control, emotion regulation, and top-down and bottom-up processes that alter emotion, behavior, or cognition to attempt to enhance adaptation (or to achieve an explicit or implicit goal or goal state).
i. The field needs a domain-general construct of SR that encompasses SR of action, emotion, and cognition and involves both top-down and bottom-up regulatory processes
i. Impulsivity, risk-taking, and disinhibition are distinct although overlapping
Nigg - ADHD SR Bottom Up
a. Bottom up (automatic/type1) – Automatic response to sensory input
i. Stimulus driven, rapid, and do not require mental capacity
ii. They are elicited by sensory (external) stimuli
1. Ex: Identifying new objects, tasting familiar food
iii. Bottom-up aspects of SR:
1. Impulsivity
2. Risk-taking
3. Disinhibition
Nigg - ADHD SR Top Down
a. Top Down (deliberate/type2) – Regulatory processes
i. Slow, sequential, require working memory, and capacity limited
ii. Used to address problem, resolve conflict or coactivation, or to prepare for anticipated goal or challenge
1. Ex: Stroop effect, can read with typos
iii. Top-down aspects of SR:
1. Executive Functioning
2. Cognitive Control
3. Effortful Control
SUDs Gender Paradox
o Potential Gender Paradox where women are more effected by alcohol than men - women can experience greater health harm from alcohol use and develop AUD-related problems faster than men, even with lower consumption levels
Bones - AUD - Etiologic, Theory-based, ontogenetic Hierarchical Framework (ETOH Model)
a. Etiologic, Theory-based, Ontogenetic Hierarchical Framework (ETOH Model):
i. Dimensional
ii. Improves construct validity
iii. Outlines domains of cognitive control, reward, and neg valence & emotionality
iv. Includes key moderators of AUD mechanisms opponent processes & self-awareness
v. Increased conceptual role for neg valence & compulsions in AUD
vi. Reduce heterogeneity & comorbidity
vii. Helps identify mechanisms
viii. Give symptoms more meaning (DSM is symptom level; this explains HOW you got symptoms
ix. Help w/ treatment matching
a. Critique of DSM
i. Inadequate construct validity
ii. Heterogeneity
iii. Substantial comorbidity
iv. Failure to consider etiology
Bones - AUD - 3 Super Domains
i. Cognitive Control – Compulsivity & impulsivity
ii. Reward – Pos expectations, reward sensitivity, pos emotionality, incentive salience, discounting, habit
iii. Negative Valence/Emotionality – Punishment sensitivity, coping, neg emotionality, neg expectations
Watts - AUD - Purpose & Findings
a. Purpose: Crude measurement practices—especially using too few indicators per construct—can obscure meaningful multidimensionality. Challenges assumption that disorders like AUD are unidimentional
b. Findings:
i. A simple 11-item AUD model (one item per DSM-5 criterion) showed good fit, suggesting unidimensionality. But when all 87 items were included, the model fit worsened significantly, revealing poor unidimensional structure.
ii. Multidimensionality outperformed unidimensionality
iii. Tolerance is NOT a strong marker of severity or dependence after controlling for heavy consumption
iv. Tolerance is independent but encourages other aspects of dependence by facilitating repeated high-dose exposure
Watts - AUD - Higher-Order Dimensions of AUD
i. Tolerance
ii. Withdrawal
iii. Loss of control
Watts - AUD linked strongest to Internalizing
a. AUD criteria most strongly linked to internalizing:
i. Withdrawal
ii. Giving up activities to drink
Watts - AUD linked strongest to Externalizing
a. AUD criteria most strongly linked to externalizing:
i. Role interference
ii. Social/interpersonal problems
iii. Time spent drinking
Watts - AUD weakly linked to internalizing/externalizing
a. AUD criteria most weakly linked to internalizing/externalizing:
i. Tolerance
ii. Drinking larger amounts/longer than intended
iii. Trying to cut down
Grant - SUDs & Behavioral Addictions
a. Behavioral addictions:
i. Involve diminished control over rewarding behaviors despite neg consequences
ii. Behaviors are ego-syntonic (initially pleasurable) but can become habitual or compulsive w/ time
b. Essential feature of behavioral additions is failure to resist an impulse, drive, or temptation to perform an act that is harmful to themselves or others
Grant - SUDs & Behavioral Addictions - Examples
a. Examples: (high co-occurrence with SUDs)
i. Gambling (Most supported)
ii. Kleptomania
iii. Intern/gaming/sex/shopping
Grant - SUDs & Behavioral Addictions - common features
i. Natural history – Begin in adolescence & can be chronic, relapsing course
ii. Phenomenology – Cravings, mood elevation, withdrawal symptoms
iii. Tolerance
iv. Comorbidity – High overlap with SUDs, depression, ADHD
v. Genetic contributions - Shared family vulnerability – twin studies
vi. Neurobiological mechanisms - dysfunction with dopamine & serotonin
vii. Response to treatment – CBT & meds
Grant - SUDs & Behavioral Addictions - Results/Findings
a. Only Pathological Gambling was officially recognized by DSM-5
b. Evidence to consider pathological gambling as a non-substance or behavioral addiction. DSM has proposed moving its classification from impulse control disorder to an addition and related disorders
Grant - SUDs & Behavioral Addictions - Telescoping Phenomenon
a. Telescoping phenomenon - Higher rates of pathological gambling are observed in men, with a telescoping phenomenon observed in females (i.e., women have a later initial engagement in the addictive behavior, but foreshortened time period from initial engagement to addiction
Samuel - DSM AMPD doesnt capture OCPD - they suggest
a. They suggest –
i. Adding workaholism
ii. Subdivide rigid perfectionism
iii. Consider adding traits like excessive deliberation & moral scrupulousness
b. Key feature missing from AMPD — Workaholism, excessive deliberation, and moral scrupulousness
c. Rigid perfectionism consistently strongly correlates to OCPD
Limburg - Disorders highly associated w/ perfectionism
i. Anxiety Disorders (6.2%)
ii. Eating disorders (4.6%)
iii. OCD (3.9%)
iv. Depression (1.6%)
Limburg - Perfectionistic concerns vs perfectionistic strivings
a. Perfectionistic concerns – Self-criticism, concern over mistakes, doubts about actions, socially prescribed perfectionism.
b. Perfectionistic strivings - Setting high personal standards, organization, self-oriented perfectionism.
c. Results:
i. Perfectionistic concerns had largest effect for most disorders
ii. However, perfectionistic concerns & strivings are equal in variance for eating disorders
OCPD AMPD
a. Alternative model:
i. Criteria A: Identity, self-direction, empathy, & intimacy
ii. Criteria B: Requires rigid perfectionism & 2+ of perseveration, intimacy, avoidance, restricted affectivity, impairment in functioning
Diedrich & Voderholzer - AMPD stricter w/ OCPD
a. Hoarding & miserliness was in original DSM and not Alternative
i. Alternative model is stricter and leading to less frequent diagnosis & has increased heterogeneity of OCPD
Diedrich & Voderholzer - OCPD vs OCD
a. OCPD vs. OCD:
i. OCPD: Egosyntonic, compulsions, & lack of obsessions
ii. OCD: Egodystonic, compulsions, & contains obsessions
iii. Shared features – Symmetry, hoarding-related symptoms, compulsions (23-45% comorbidity)
iv. Differences –
1. OCD is contamination & cleaning-obsessions.
2. OCPD is rigidity & self-control
Diedrich & Voderholzer - OCPD predictors of good outcomes
i. Strong early therapeutic alliance
ii. Self-esteem variability
iii. Distress levels (State Anxiety)
Diedrich & Voderholzer - OCPD etiology
i. Psychoanalytic etiological models – Attribute obsessive character formation to parental dominance, over-control and intrusiveness
ii. Attachment theory – Lack of secure attachment, less care, overprotection
Diedrich & Voderholzer - OCPD co-occurs w/
i. Anxiety Disorders
ii. Mood Disorders (unipolar & bipolar)
iii. SUD
iv. Cluster A PDs (Paranoid & schizotypical)
v. Medical conditions
Diedrich & Voderholzer - OCPD stability
i. Less stable than thought. Some studies show remission and others show persistence/worsening with age.
ii. Trait stability: Rigidity, hoarding, problems delegating
Miller - NP Mask Model
Mask Model - Inner insecurity or fragility as a driving force of grandiose narcissistic behavior
Argues that this is incorrect and lacking because there is no evidence for high explicit self-esteem co-occurring with low implicit self-esteem
Miller - NP Status-pursuit-in-narcissim Model
Status-pursuit-in-narcissism Model - Narcissism is related to selection of situations that afford status, increased attention to status-related cues, and increased behavioral activation following evaluations of these cues and appraisals of whether they signal an opportunity to elevate one’s status (agentic reactions following positive appraisals and antagonistic reactions following negative appraisals).
Miller - NP Dual Pathway Approach
Dual-pathway approach to the social consequences of grandiose narcissism - narcissism can be expressed in agentic behaviors (acting expressive and self-assured) as well as antagonistic behaviors (acting aggressive and derogating other people); the former typically evoke positive social impressions, and the latter typically evoke negative social impressions.