Psy 332 Ch 8 Interactions in Long term memory
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
43 Terms
Schema:
an organized, structured set of information about a concept, theme or person.
Schemas involves categorization of any type of information in the world (hospital, shopping mall, mother, conflict, acceptance, secure, abuse, failure).

Scripts (Schank & Abelson, 1977):
Schemas for events in the world/routines (allow us to create inferences). (ex. Restaurant script, Grocery shopping script, Daily routine script, TV watching script)
Inference
The process by which a person draws connections between concepts, determines referents and derives conclusions. (assumption, fill-in-the gaps. E.g How did the fishbowl fell?)
Evidence for Schemas (Brewer & Treyens, 1981)
•Subjects were asked to wait in an office and they were later asked to recall the various objects from the room.
•Subjects showed good memory for objects consistent with an office (ex. A stapler), but they had poor memory for objects inconsistent with an office (ex. A toy top) and showed false memory for objects consistent with an office (ex. paper clips)
Evidence for Scripts (Bower, Black & Turner, 1979)
-Participants were asked to read stories based on common themes (Ex. Going to the doctors office, eating at a restaurant).
Afterwards, participants were asked to recall the events in the story. Participants were better recalling script-inconsistent actions (talking with the chef) than the script-consistent actions (paying the bill)
-Participants also showed that they falsely recalled and recognized script-consistent actions that were never explicitly stated in the stories

People can implicitly use prior knowledge to interpret ambiguous events and the corresponding bias is revealed during the time of memory recall.
Pitchert and Anderson (1977) instructed participants to read through a scenario describing a floor-plan of a house from the perspective of a home-buyer vs. burglar.
Researchers found that participants instructed to have a home-buyer perspective recalled information related to the features of the house that make it a good investment. In contrast, participants given the burglar perspective recalled information related to being able to steal from the house.
Source Misattribution:
The inability to distinguish whether the original event or some later event was the source of the information (E.g: Elizabeth Loftus "Car Crash" Memory Study)
Elizabeth Loftus "Car Crash" Memory Study
Subjects saw a film of a car accident
Later, different subjects were asked:
How fast were the cars going when they:
smashed?, collided?, bumped?, contacted? (leading questions)
Subjects estimates of speed varied with the verb they got in the question phase of the experiment.
(smashed > collided > bumped > contacted) fastest estimate slowest estimate
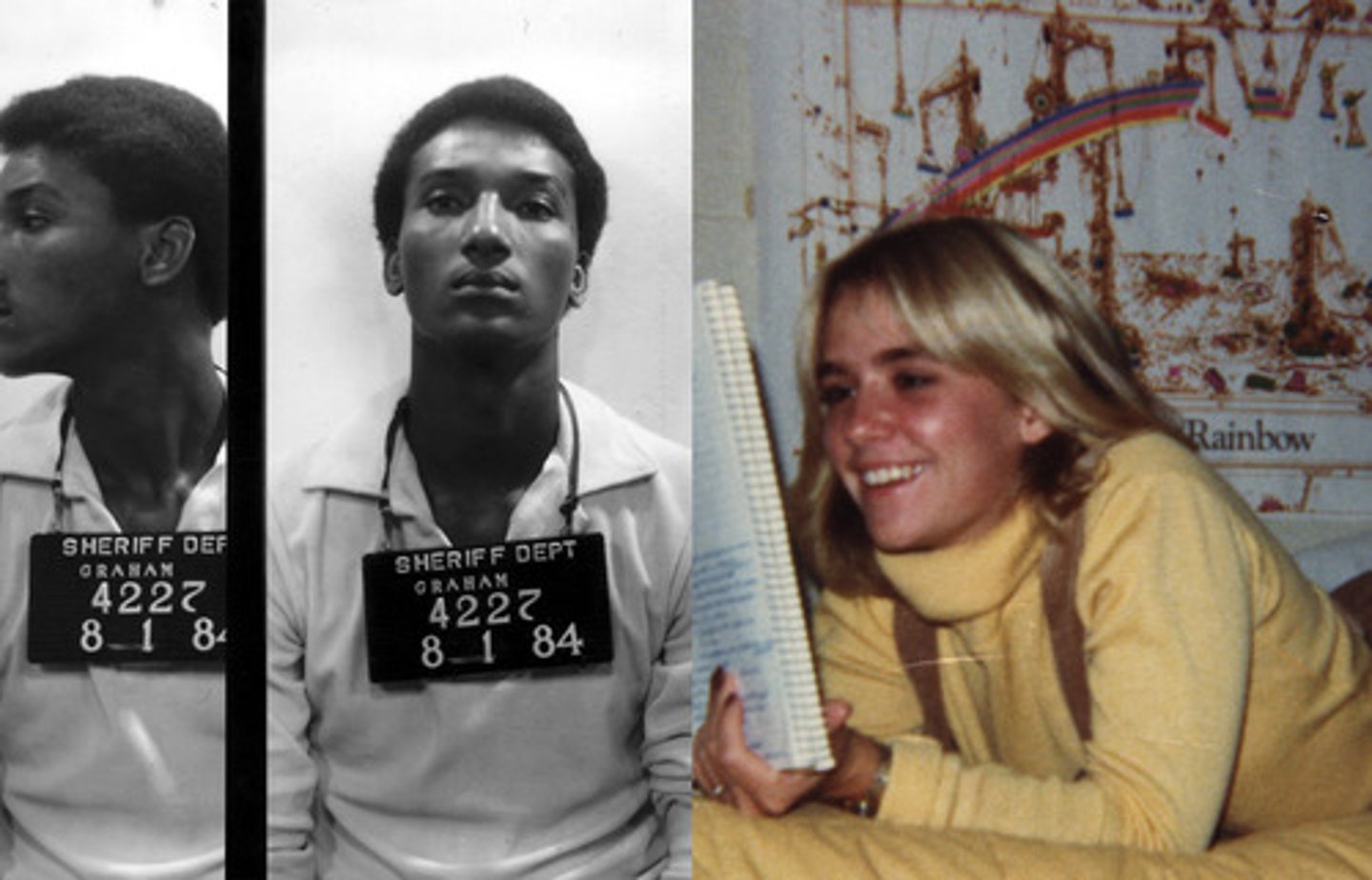
Factors involved in the overconfidence in eyewitness memory
Increased exposure to the associated information to the incident or event.
Post-identification reinforcement (by other people, police etc)
Repeated questioning of the eyewitness.
EX:(Jennifer Thompson accused the wrong guy (Ronald Cotton) and he was sent to jail for rape, the right guy (Bobby Poole) was found guilty many years later)
Emotions and False Memories
Storbeck and Clore (2005) used a Deese-Roediger-McDermott false memory task to examine how emotional states influence processing styles.
Researchers primed a positive (uplifting classical music) or negative mood (downtrodden classical music) or no mood at all (control group) among the participants before the false memory task was presented.
In the first part of the study (Experiment 1), the researchers demonstrated that the negative mood group recalled fewer critical lures compared to both the positive and control groups. (depressive realism)
A follow-up experiment asked whether the effect observed in Experiment 1 was due to encoding processes or strategies.
To examine this question, the researchers asked participants to write down both words they recalled as having been presented and words that came to mind but that had not been presented.
Overall, the sad mood group recorded fewer total critical lures compared to the positive mood group.
Positive emotions increased false memory and negative emotions decreased false memory
Reproductive memory
Autobiographical Memory and Flashbulb Memories
Autobiographical Memory:
The study of one's lifetime collection of personal memories. (remember those
memories accurately strong moments that happen to you in life )
Flashbulb Memories:
Extremely vivid recollections of emotional memories of particular events, especially when the events were surprising or highly unusual.
(Note: Flashbulb memories may also be vulnerable to Source Misattribution and forgetting, but people still report being confident about the accuracy of the memory.) E.g: Aug 7 knowing that landed on a Saturday because is your wedding date and you remember all the details. Doesn't have to be positive memory

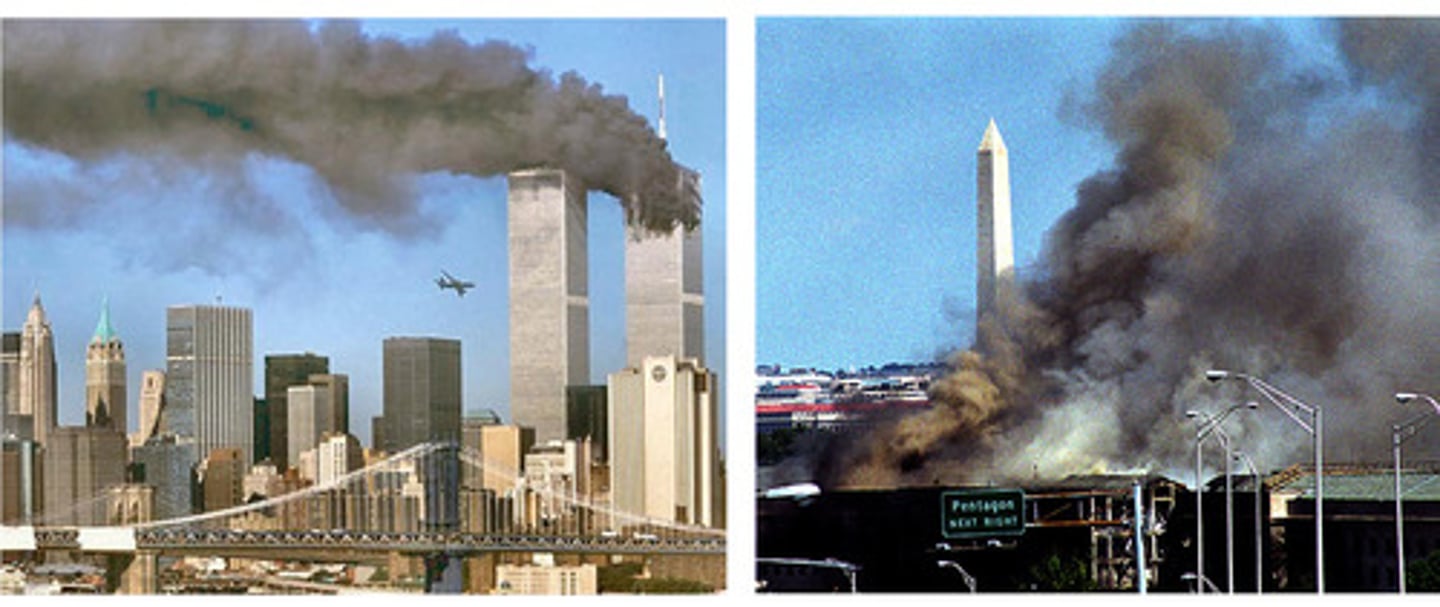
Hirstetal(2009) report an extensive study for the memory of 9/11 events involving 3000 individuals from 7 American cities.
Surveys were conducted 1 week after the attack, 11 months later, and 35 months later.
The researchers found significant evidence for forgetting, but inconsistent with the amount of normal forgetting that people experience in their daily lives.
A detailed analysis of the type of the factual details remembered shows variations in the accuracy of flashbulb memories. For example, people's memory for the crash sites was significantly higher than the names of the airlines.
Memory for Negative words
Ochsner & Schacter (2000) found that normal people tend to remember negative words (ex. sad, die, gun) from a free recall list due the detailed, specific emotional recollections they felt during the time the negative words were encountered.
Mineka & Nugent (1995) found that depressed individuals tend to remember more negative words than positive words from a free recall list and this fits in with their negative-self schema.
• When recalling autobiographical events, people in positive moods, compared with those in negative moods, describe such events using more abstract, global representations.
Which part of the brain contributes to declarative memory?
The Hippocampus
The Hippocampus
is necessary for the formation of new explicit (Semantic and Episodic) long- term memories. It helps organize the distributed representation regarding a memory from the different areas of the brain (vision, smell, hearing, touch, taste, emotion)
Damage of the hippocampus
causes an inability to form new explicit declarative (semantic and episodic) memories; Anterograde Amnesia (ex. Patient EP and HM)

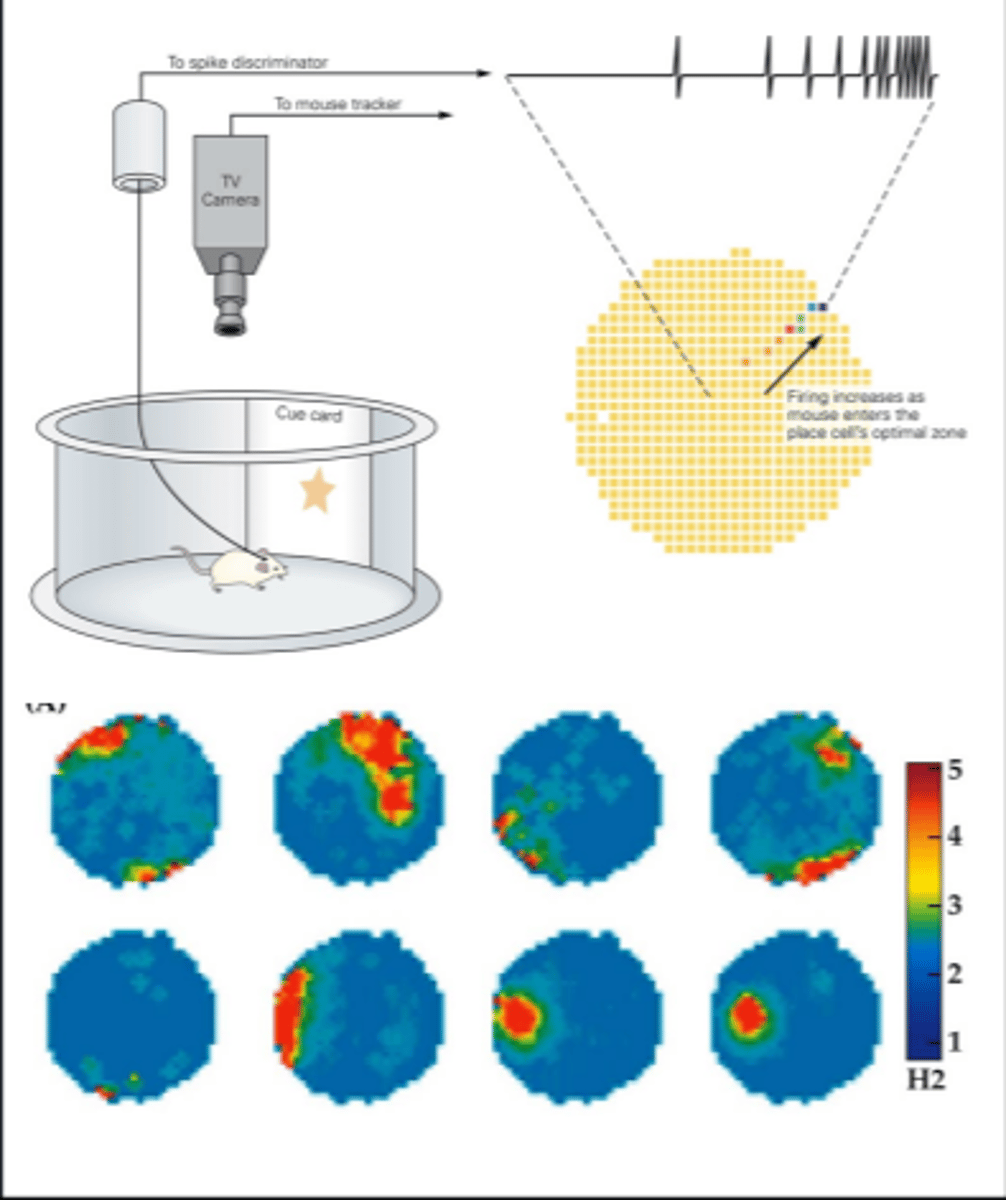
Cognitive map theory:
The hippocampus constructs maps of external world based on the relationships between external landmarks and objects
Evidence: Place cells
Place cells in rat hippocampus were activated when a rat is placed in a specific location, but only after the rat becomes familiar with that location.
Configural association theory
the hippocampus organizes and retains the behavioral significance of combinations of stimuli and the context that they are presented in, but not the individual stimuli themselves.
Long-Term Potentiation (LTP)
Long-term increase in the excitability of a postsynaptic neuron to a particular presynaptic input caused by repeated, intense, high frequency activity from that presynaptic input. In other words, neurons that fire together, connect together.
This is a mechanism for synaptogenesis (forming new synapses)
Long term potentiation (weak input and strong input)
Forming episodic memories requires
an intact Prefrontal cortex and Hippocampus.
Post-traumaticstress disorder (PTSD):
An anxiety disorder in which a person who has experienced a traumatic or life-threatening event has symptoms such as psychic numbing, reliving of the trauma, and increased physiological arousal. (Amygdala and Hippocampus)

The Impact of PTSD on the brain (Van Der Kolk, 2003)
Increased activity of the amygdala, right hemisphere, insula and medial temporal lobe
Decreased activation of prefrontal cortex
Decreased activation of the hippocampus (lack of integration of the traumatic event)
Decreased activation of Broca's area
(ability to have grammar in language, if you have trauma in this area of the brain a person can have problems
Edna Foa’s theory of PTSD (1986, 1989, 1998)
focuses on a semantic fear network in long term memory that requires assimilation.
Foa states that resolution of trauma occurs by integrating information in the fear network with existing memory structures. This assimilation process requires the activation of the fear network so that it becomes accessible for modification and also the availability of information that is incompatible with the fear network so that the overall memory structure can be modified. (victim mentally vs survivor mentality) Ex: video of senator being accused of raped years ago.

Theories of Forgetting
Lack of attention during Storage (encoding failure), Decay theory,
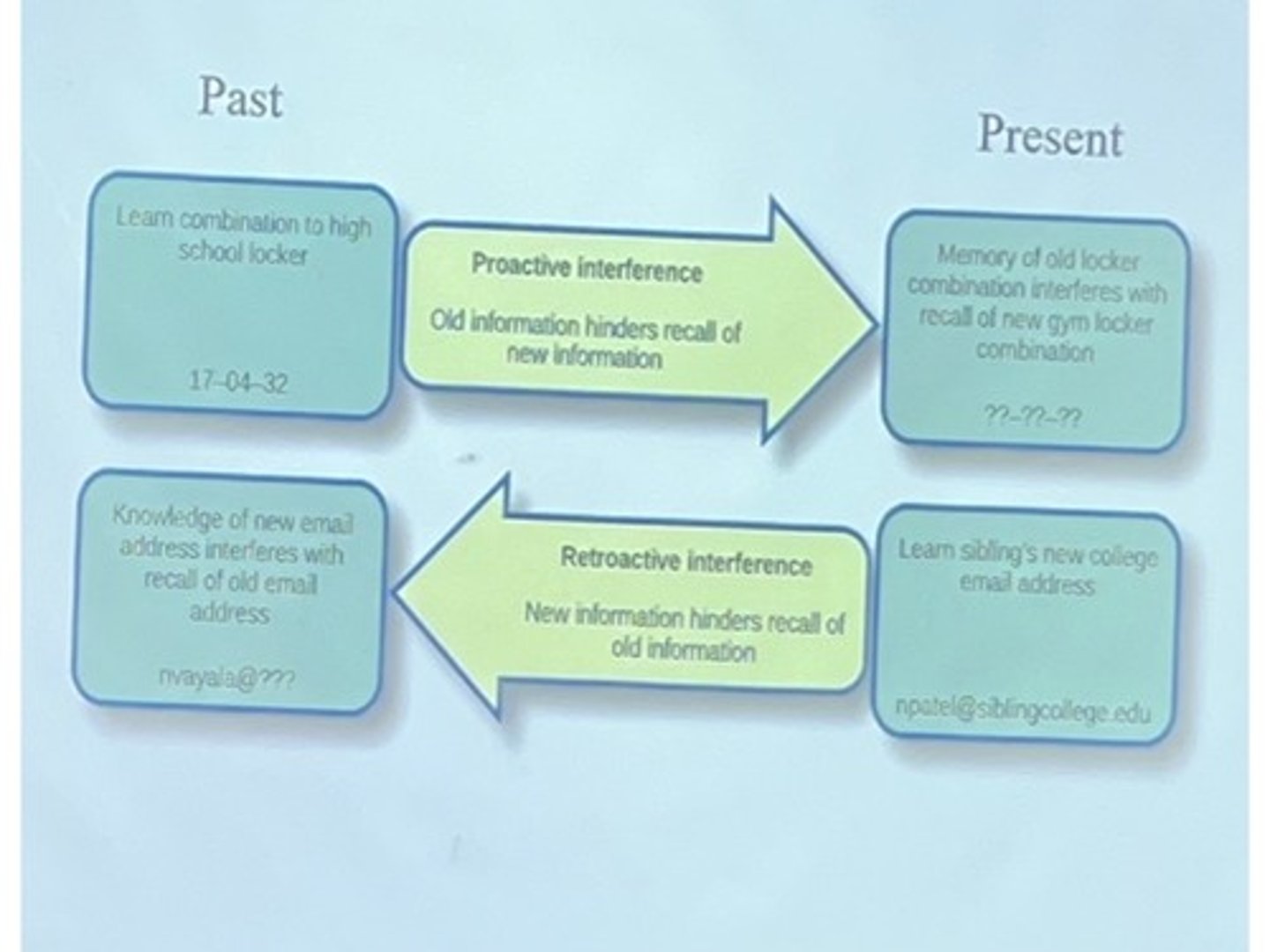
Retroactive interference:
Proactive interference

Decay theory:
memory fades with time if they are not retrieved every now and then. Use it or lose it

Retroactive interference:
recently learned material interferes with remembering a similar previously stored material. (E.g a waiter taking guest orders)

Proactive interference:
previously learned material interferes with remembering a similar new material. (Old phone number vs. new phone number)
Amnesia
Can be caused by Electro Convulsive Therapy, Hypothermia, Concussion, Infection, Tumor, Lesion

Anterograde Amnesia:
the inability to store new long- term memories that occurs after an amnesia inducing event.
Retrograde amnesia:
the loss of memory for events that occurred prior to the amnesia inducing event

What can damage to the amygdala cause?
Causes impairments in fear conditioning or startle responses. (fear is important to sense danger and get yourself hurt)
What can damage to the Cerebellum cause?
causes distruption of eye-blink conditioning, while damage to the Striatum (Caudate nucleus, Putamen) causes a disruption of habit learning such as procedural memories.
Korsakoff’s syndrome
Anterograde amnesia caused by thiamine (vitamin B1) deficiency (often associated with alcoholism🍺)
Damage to the dorsomedial nucleus of thalamus and mammillary bodies
Intact implicit, procedural memory and short term/ working memory
Inability to form new explicit memories

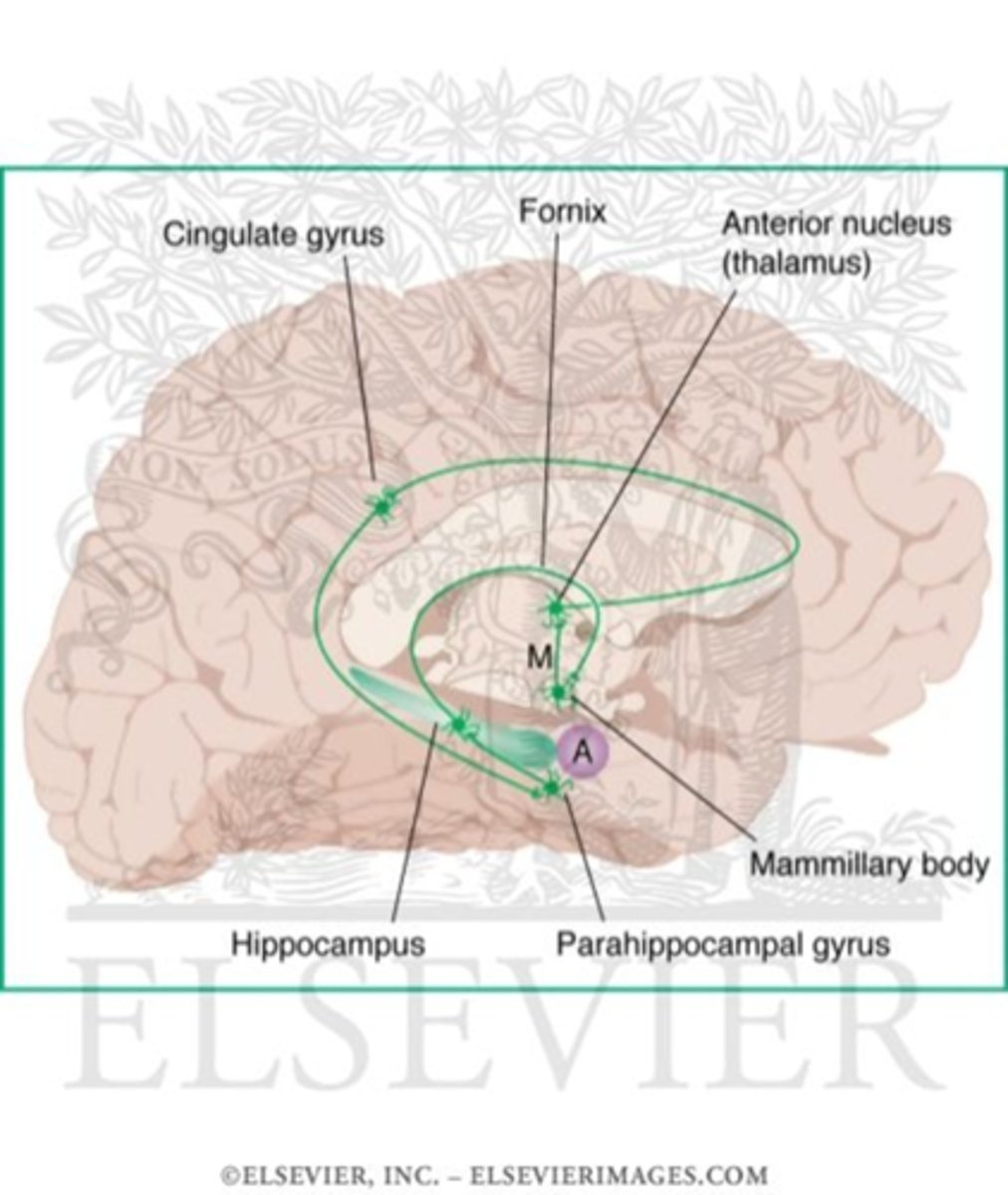
Papez Circuit (James Papez, 1937)
-A series of interconnected brain regions that have key roles in the formation of explicit memories
-Hippocampus, Parahippocampal gyrus, Mammilary body, Anterior Nucleus of the Thalamus, Fornix and Cingulate Gyrus
Acetylcholine pathways starting from the basal forebrain nuclei regulate the activity of the hippocampus. (disruption of these pathways leads to disruption of memory and learning)
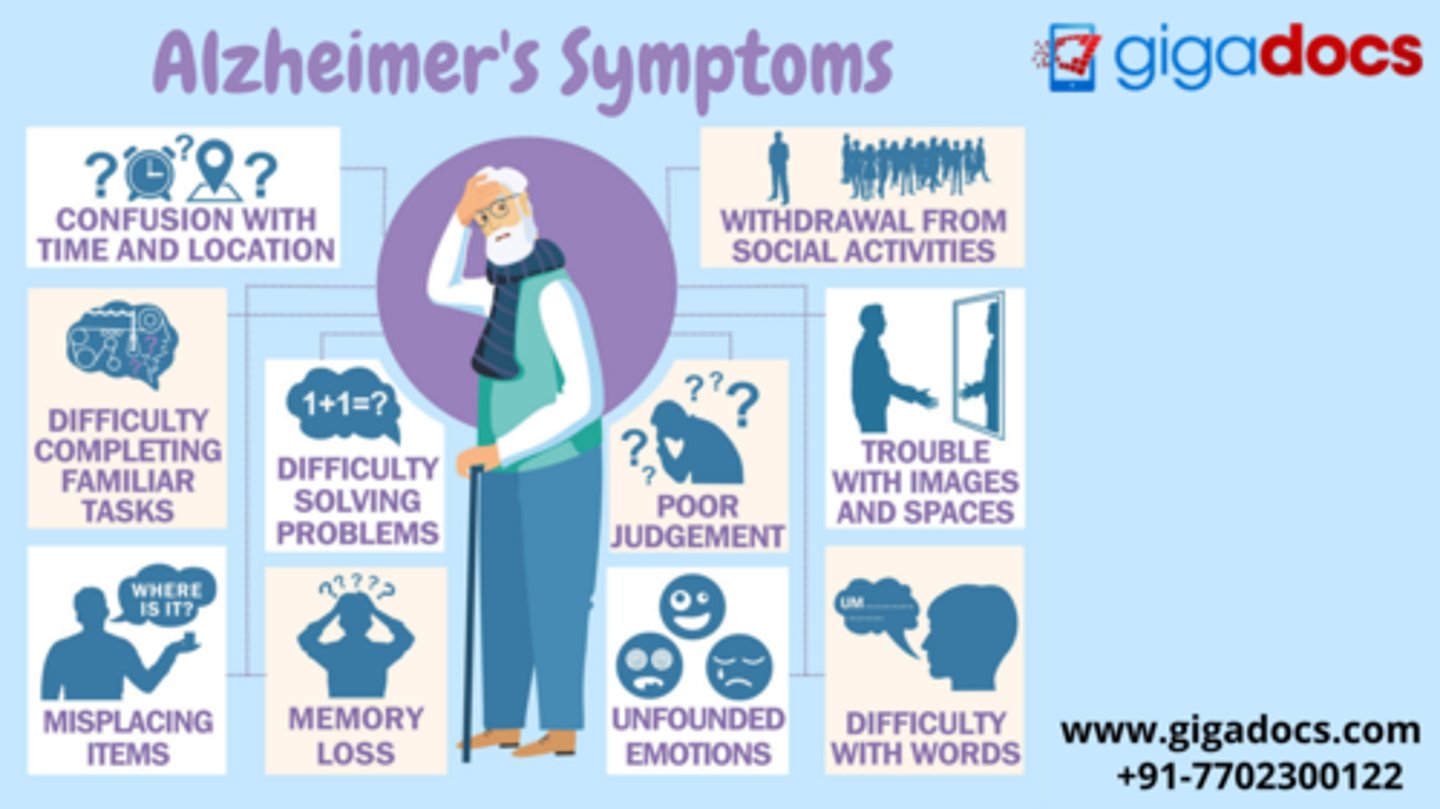
Alzheimer’s disease:
Symptoms include widespread disturbances in working, semantic, episodic and procedural memory in individuals aged 65 and above. Other symptoms include confusion, irritability, aggression, mood swings, language breakdown, and the general social withdrawal of the patient as his or her senses decline.
• The average life expectancy following diagnosis is approximately seven years. Fewer than 3% of patients live more than fourteen years.

Predementia stage of Alzheimer’s Disease
The most noticeable symptom is memory loss, which involves a difficulty to remember recently learned facts and an inability to acquire new information.
Slight problems with the executive functions of attentiveness, planning, mental flexibility, and abstract thinking or with impairments in semantic memory and concept relationships can also be symptomatic of the early stages of Alzheimer's Disease.
Apathy can begun to be observed at this stage.

Early dementia stage of Alzheimer’s Disease
Language problems mainly involve a shrinking vocabulary and decreased word fluency, which lead to a general limitations of oral and written language. In contrast, people are usually capable of adequately communicating basic ideas.
While performing fine motor tasks such as writing, drawing or dressing, certain movement coordination difficulties may be present, which may appear as clumsiness.
Moderate dementia stage of Alzheimer’s Disease
Reading and writing skills are progressively lost.
Complex motor sequences become less coordinated as time passes, reducing the ability to perform most normal daily living activities.
Short-term memory problems worsen and Long-term memory problems occur
The person may not recognize close relatives.
Wandering, irritability, crying, outbursts of unprovoked aggression or resistance to care-giving occur.
Approximately 30% of the patients also develop illusionary misidentifications and other delusional symptoms.
Lack of control over urination can develop.

Advanced dementia stage of Alzheimer’s Disease
The patient is completely dependent upon caregivers.
Language is reduced to simple phrases or even single words, eventually leading to complete loss of speech. (They can still receive and return emotional signals via facial expressions.)
Patients will ultimately not be able to perform even the most simple tasks without assistance.
Muscle mass and mobility will deteriorate to the point where they are bedridden, and they will also lose the ability to feed themselves.
Death occurs from some external factor such as pressure ulcers or pneumonia, and not from the disease itself.
Causes of Alzheimer’s Disease
Cytoskeletal (within the cell structure) abnormalities
Formation of Neurofibrillary tangles.
Thetanglesdisrupt intracellular transport of proteins causing cell death.
Neurofibrillary tangles are left behind.
Senileplaques
Accumulation of protein fragments (amyloid beta) between cells
Under normal conditions protein fragments are broken down and eliminated
In Alzheimer disease, they build up to form hard, insoluble plaques
Neurotransmitterchanges
Degeneration acetylcholine neurons of basal forebrain that regulate the activity of the hippocampus.