Hemoglobin Synthesis
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
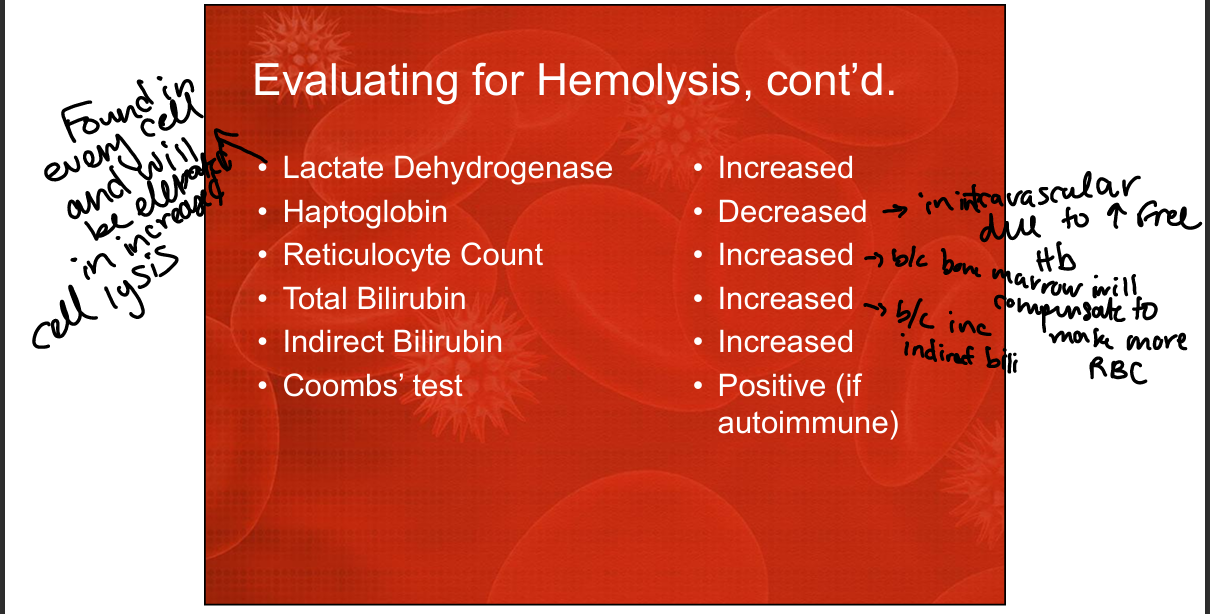
What are three laboratory abnormalities commonly associated with hemolytic anemia?
Increased LDH, decreased haptoglobin, increased indirect bilirubin, increased reticulocyte, postiive Coombs if autoimmune
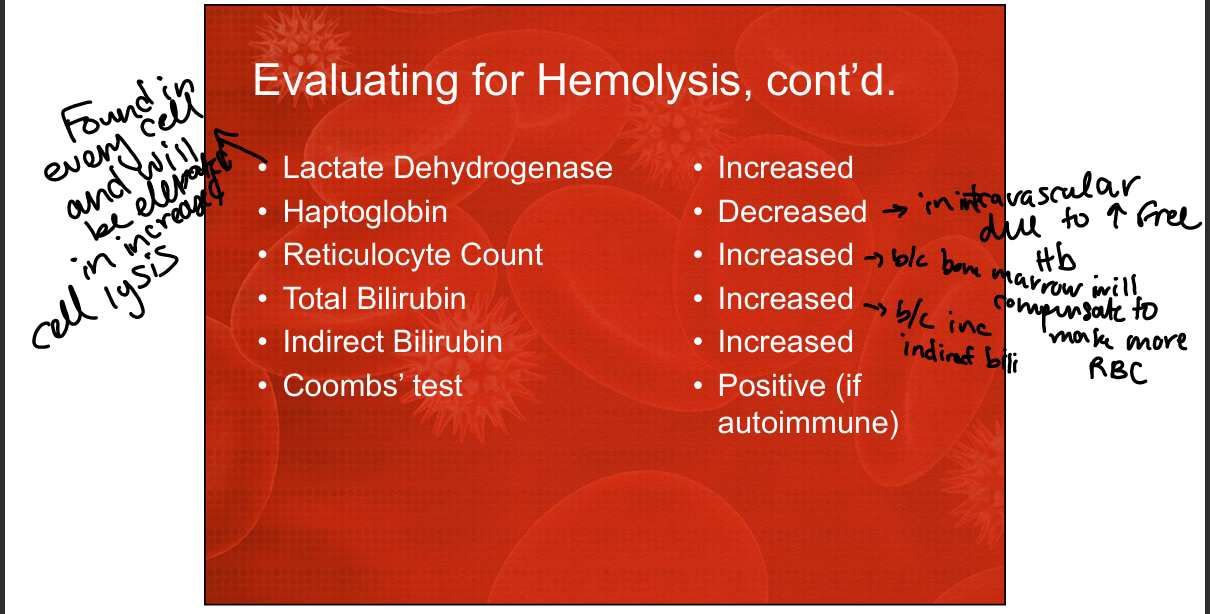
Why does LDH increase in hemolytic anemia?
LDH is released from lysed RBCs during hemolysis, increasing serum levels.
Why does indirect bilirubin increase in hemolytic anemia?
Heme breakdown produces unconjugated bilirubin
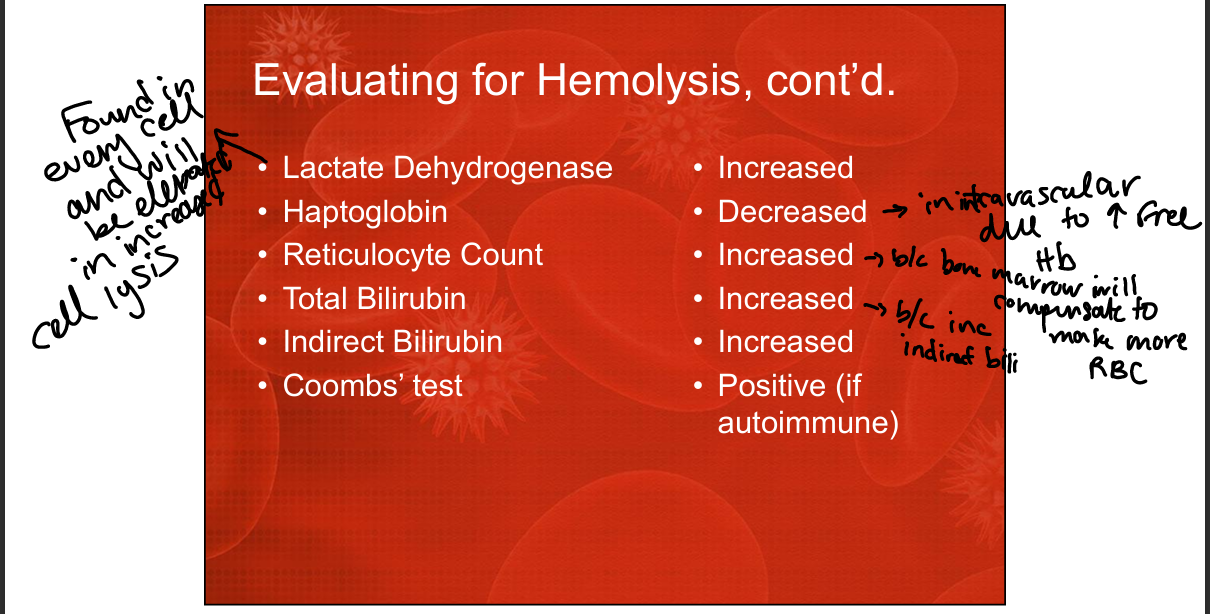
Why does haptoglobin decrease in hemolytic anemia?
Free hemoglobin released from lysed RBCs binds haptoglobin, forming complexes cleared by the liver, lowering serum haptoglobin.
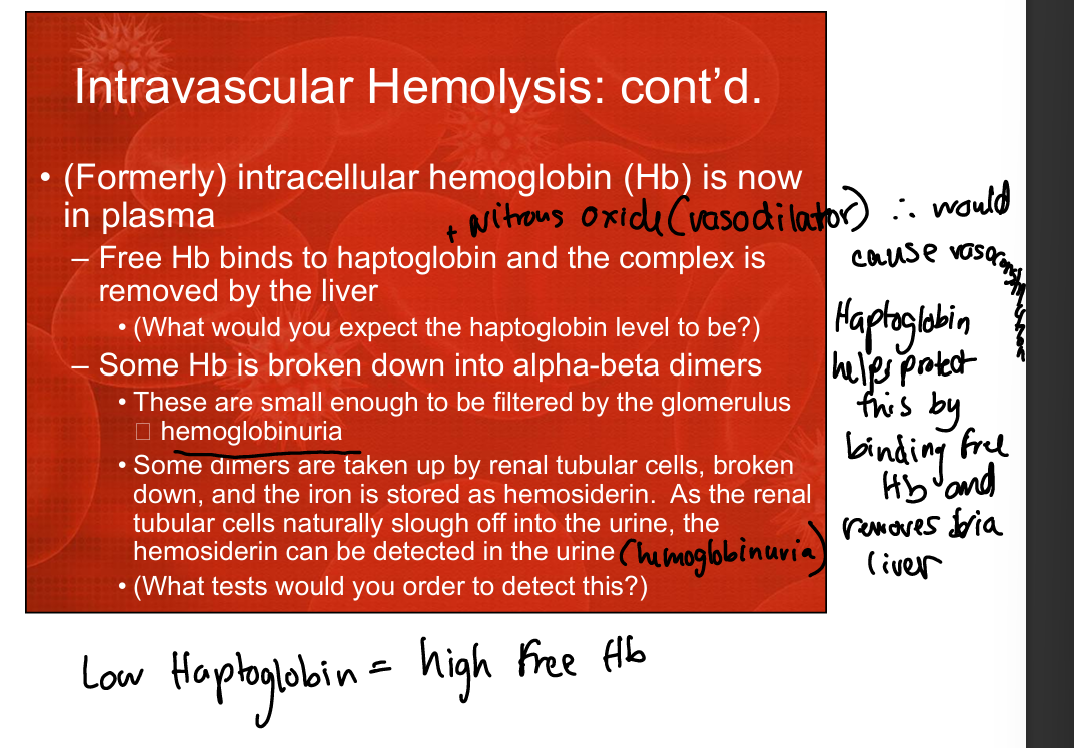
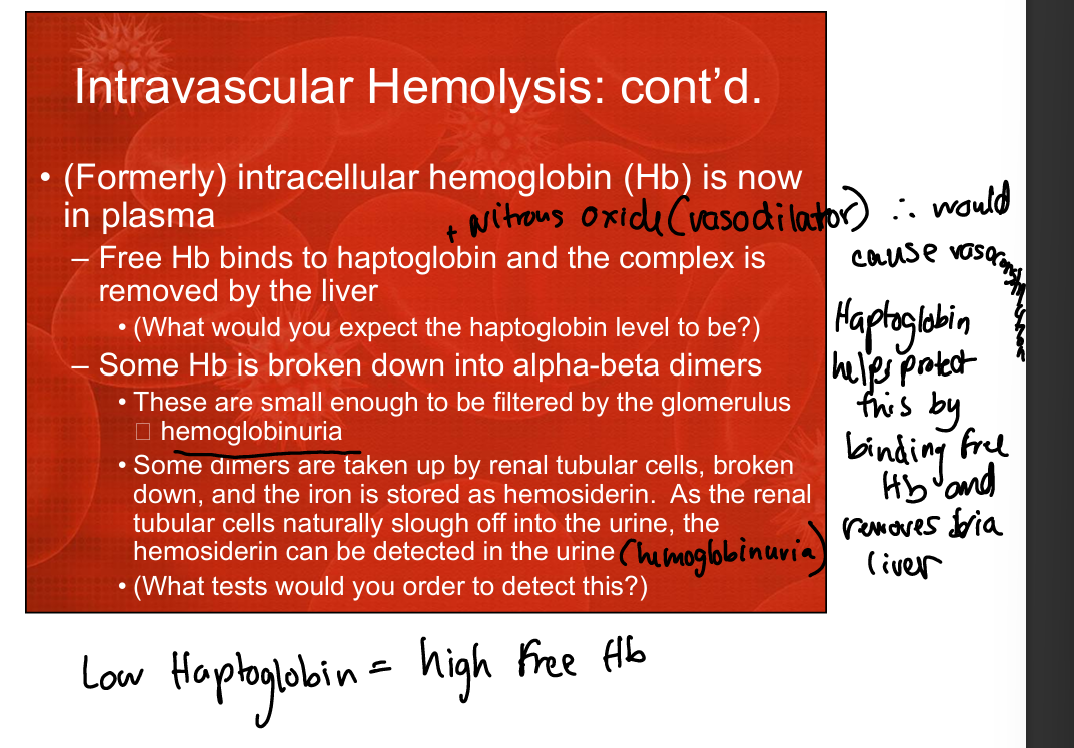
What is the difference between intravascular and extravascular hemolysis?
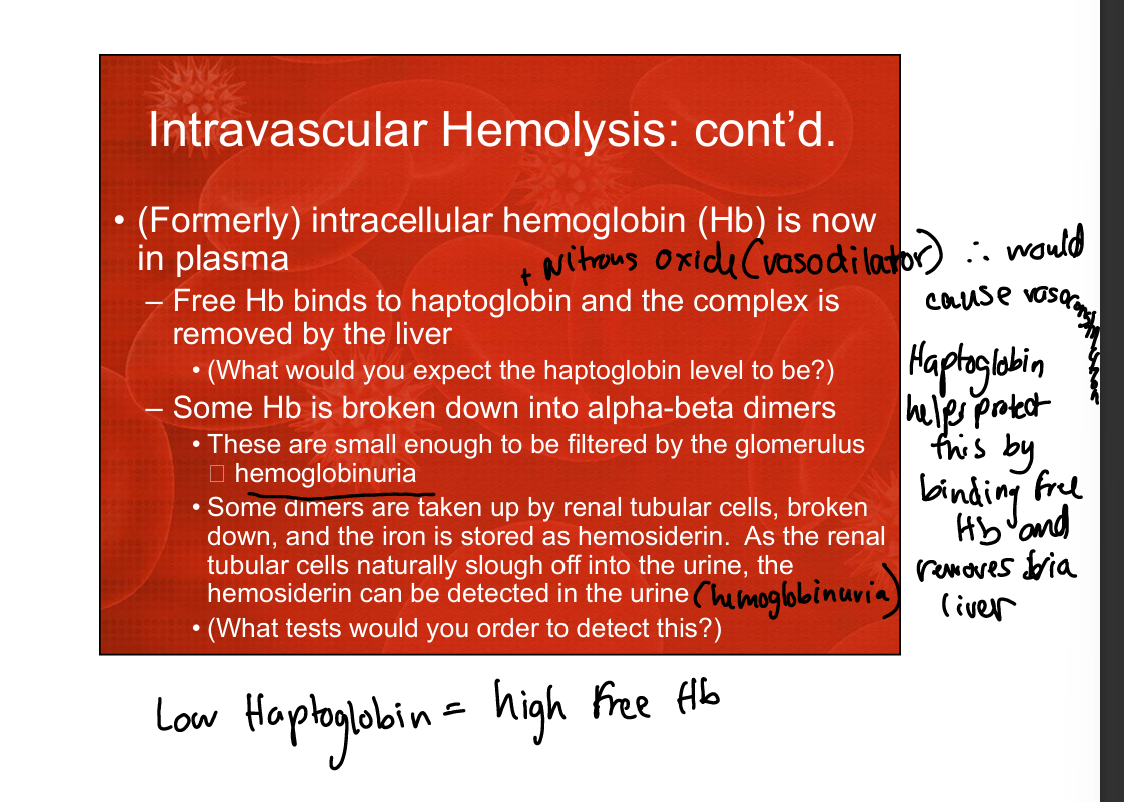
Intravascular hemolysis occurs inside blood vessels with free Hb in plasma; Extravascular occurs outside of vascular space (in liver or spleen)
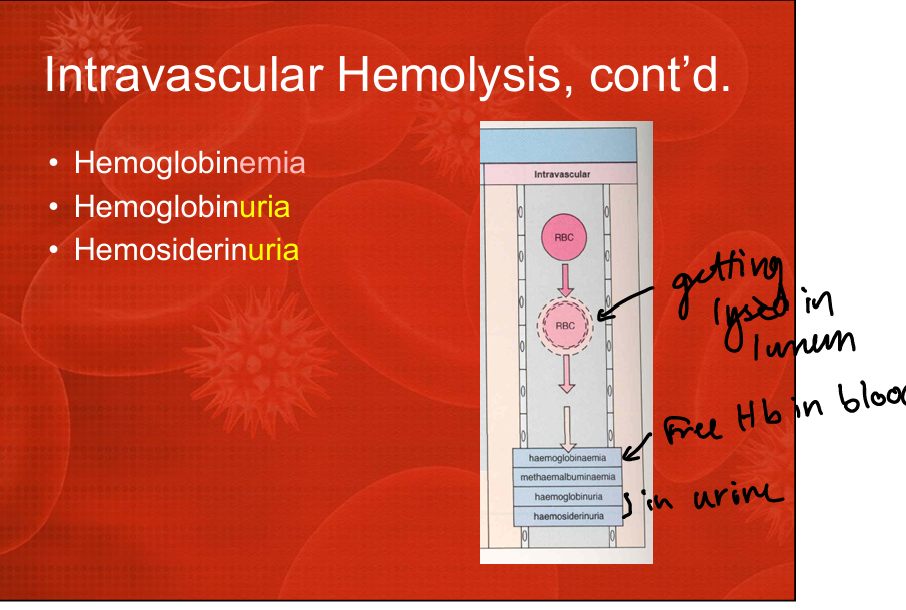
List key features of intravascular hemolysis.
Hemoglobinemia, hemoglobinuria, hemosiderinuria, decreased haptoglobin, free Hb in plasma, RBC destruction within vessels.
List key features of extravascular hemolysis.
RBC destruction by macrophages in spleen/liver, increased bilirubin, normal or mildly decreased haptoglobin, no hemoglobinuria.
Why does hemoglobinuria occur in intravascular hemolysis?
Free Hb dimers are small enough to be filtered by the glomerulus, appearing in urine.
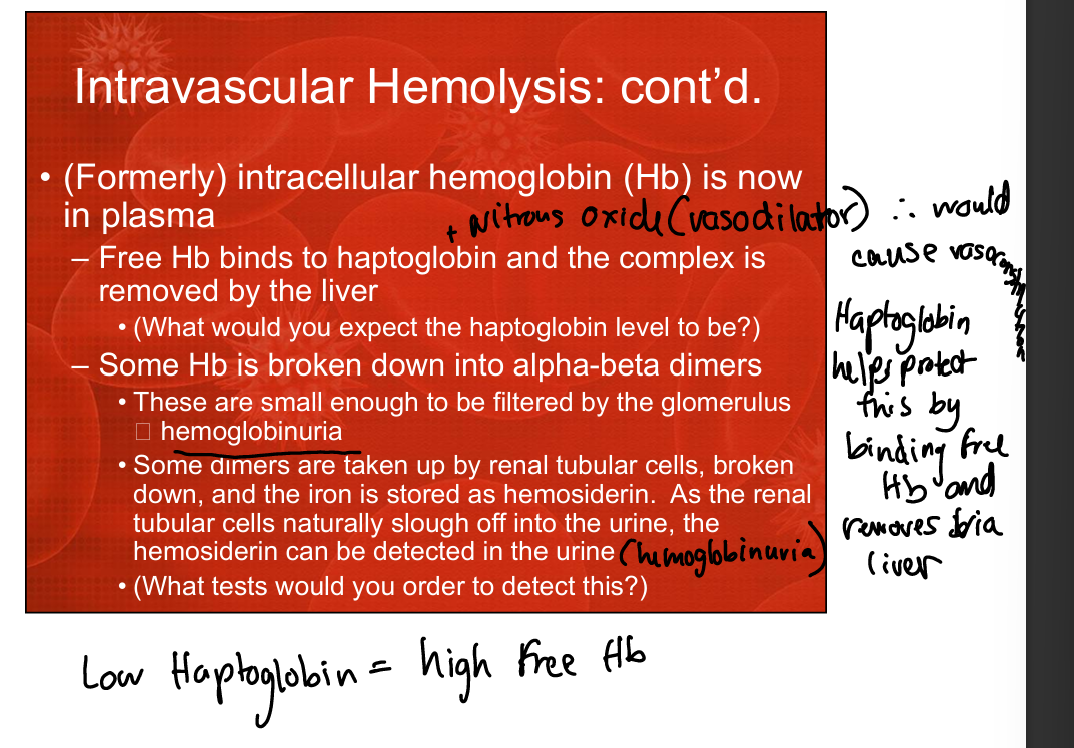
Why does hemosiderinuria occur in intravascular hemolysis?
Renal tubular cells take up Hb dimers, convert iron to hemosiderin, and slough into urine.
Why does extravascular hemolysis not produce hemoglobinuria?
RBCs are phagocytosed intact by macrophages, preventing free Hb release into plasma.
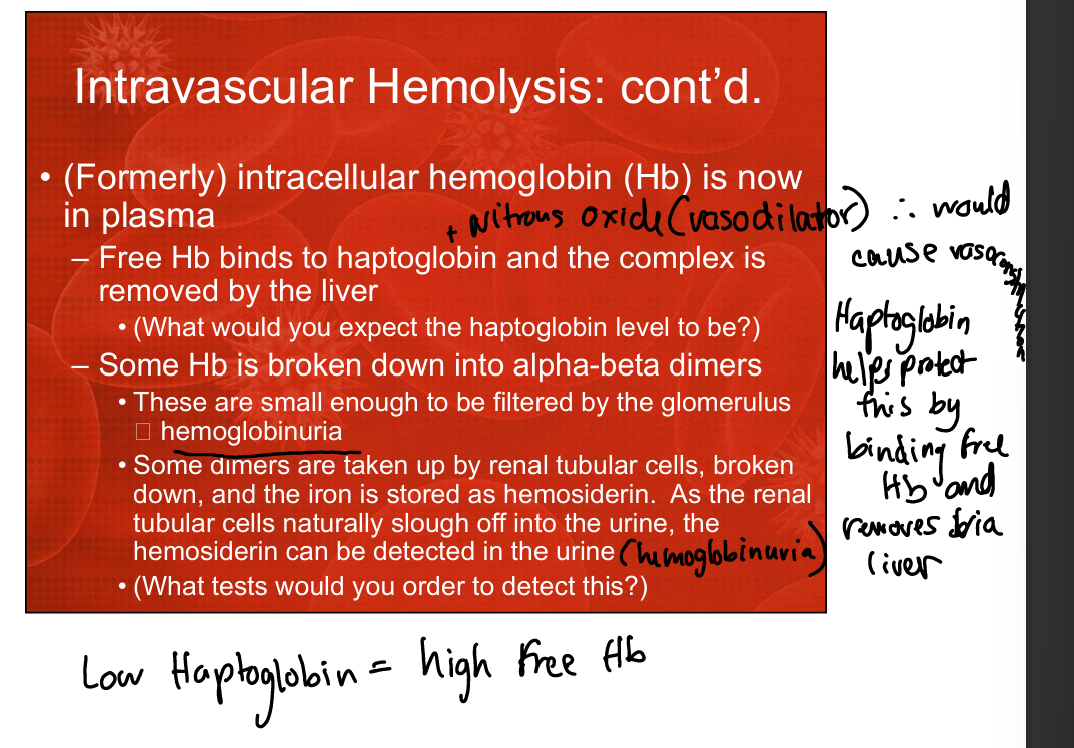
What happens to haptoglobin in intravascular hemolysis?
It decreases because free Hb binds haptoglobin and the complex is cleared by the liver.
What happens to haptoglobin in extravascular hemolysis?
It is normal or mildly decreased because RBCs are destroyed inside macrophages, not releasing large amounts of free Hb.
What test is used to determine if hemolysis is autoimmune?
The Coombs test.
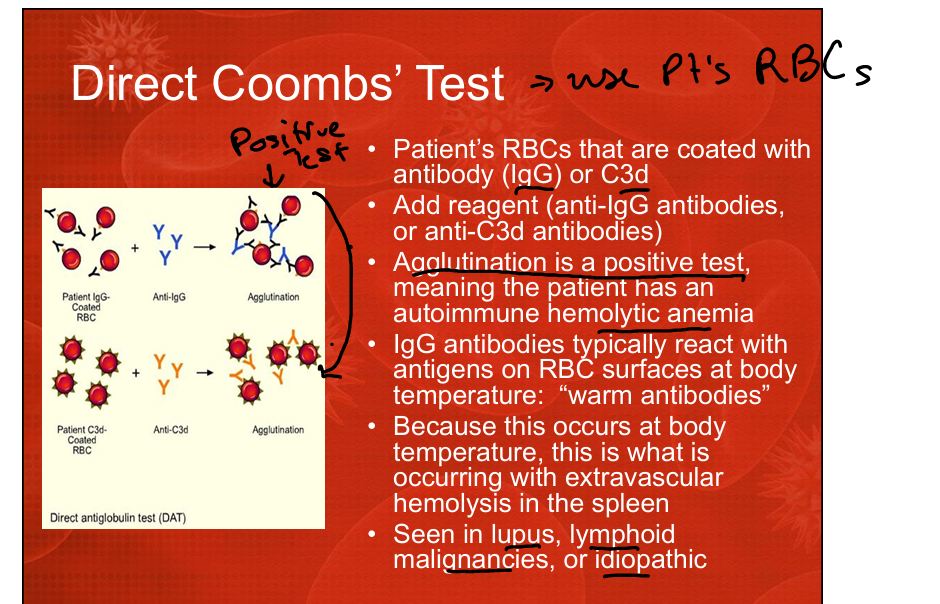
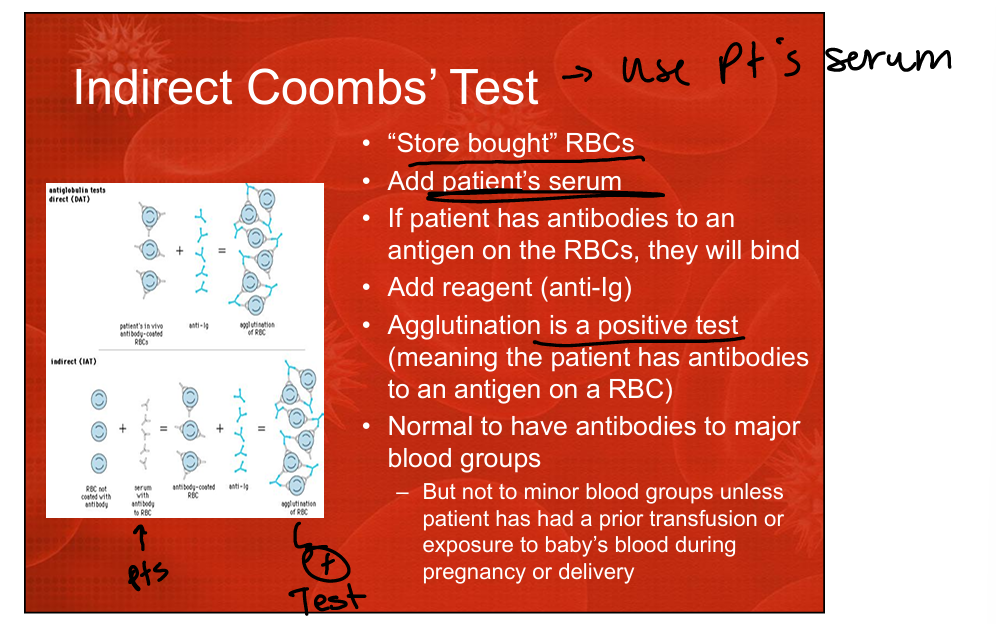
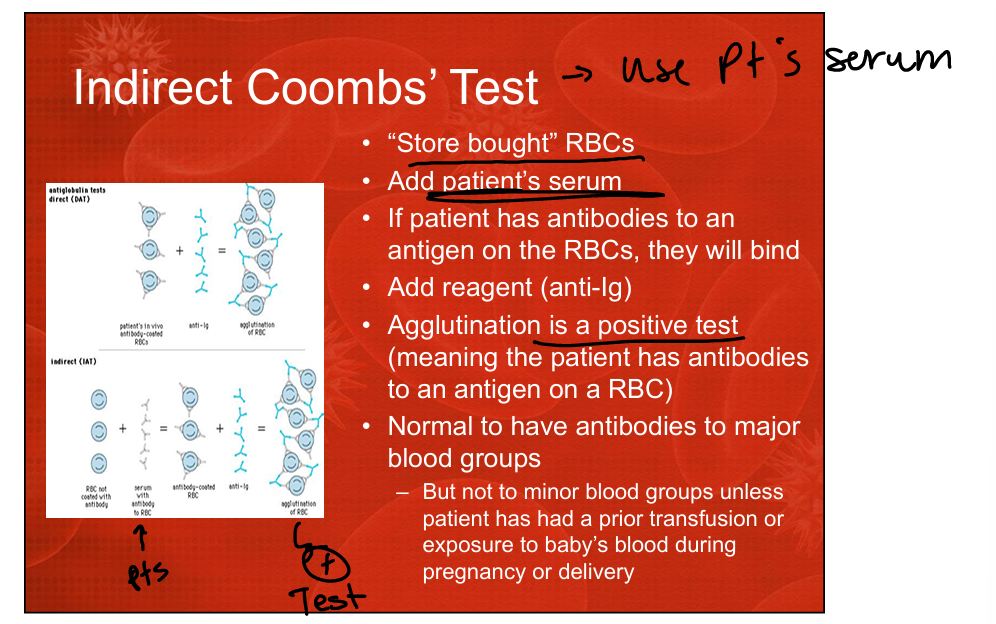
What does the Direct Coombs Test detect?
IgG or C3d bound directly to the patient’s RBC surface.
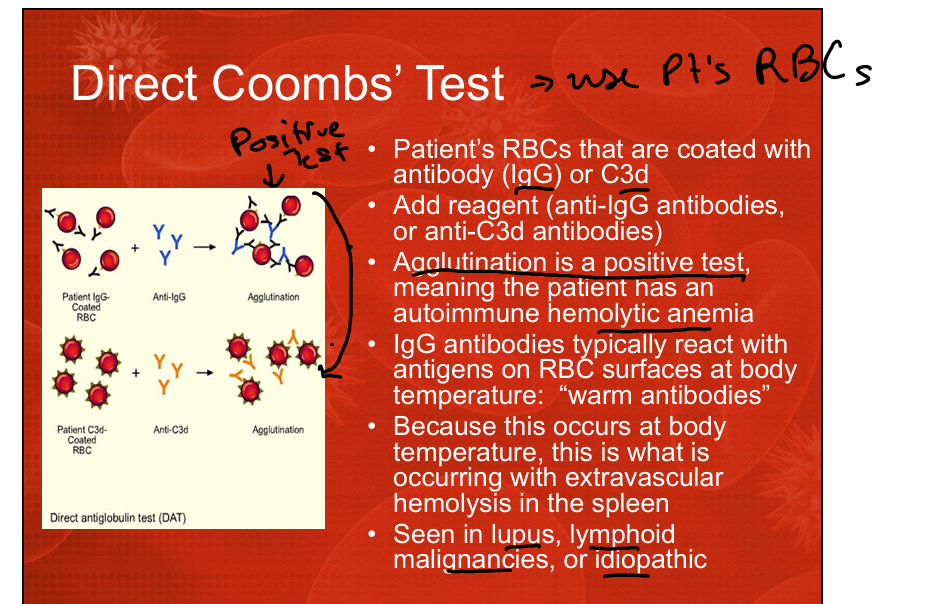
What does a positive Direct Coombs Test indicate?
Autoimmune hemolytic anemia (warm IgG antibodies or complement coating RBCs).
What does the Indirect Coombs Test detect?
Antibodies present in the patient’s serum that bind to “store‑bought” RBCs.
What does a positive Indirect Coombs Test indicate?
Circulating antibodies against RBC antigens (alloantibodies from transfusion or pregnancy).
List four categories of non-autoimmune hemolytic anemia.
RBC membrane disorders (hereditary spherocytosis, hereditary elliptocytosis),
RBC enzyme disorders (G6PD deficiency, pyruvate kinase deficiency),
Hemoglobin disorders (unstable Hbs, methemoglobinemia, thalassemia, sickle cell disease),
Extrinsic mechanical/traumatic causes (prosthetic valves, DIC fibrin strands, march hemoglobinuria).
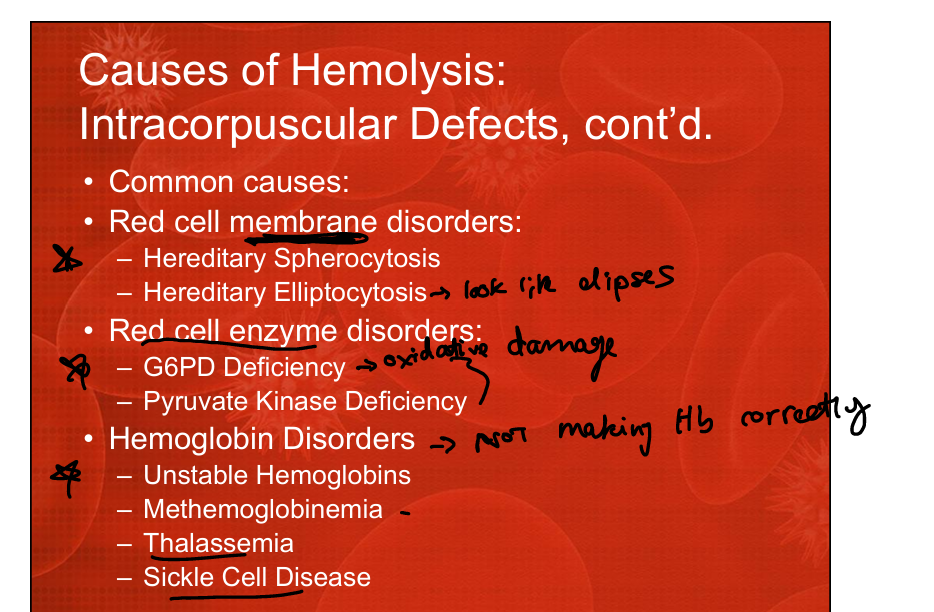
What are intracorpuscular causes of hemolysis?
Defects within the RBC itself: membrane disorders, enzyme deficiencies, hemoglobin abnormalities.
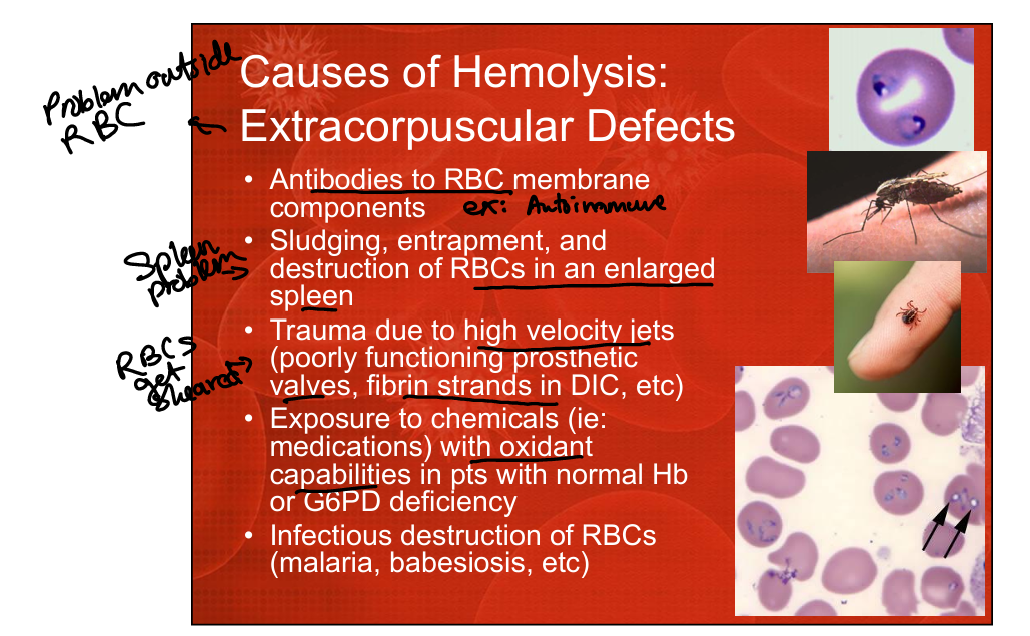
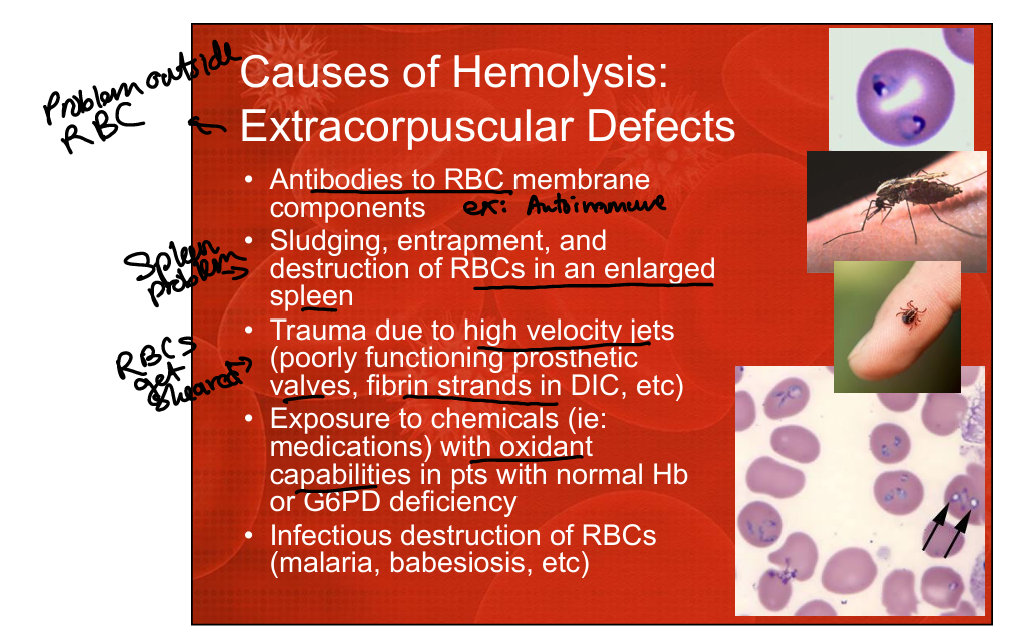
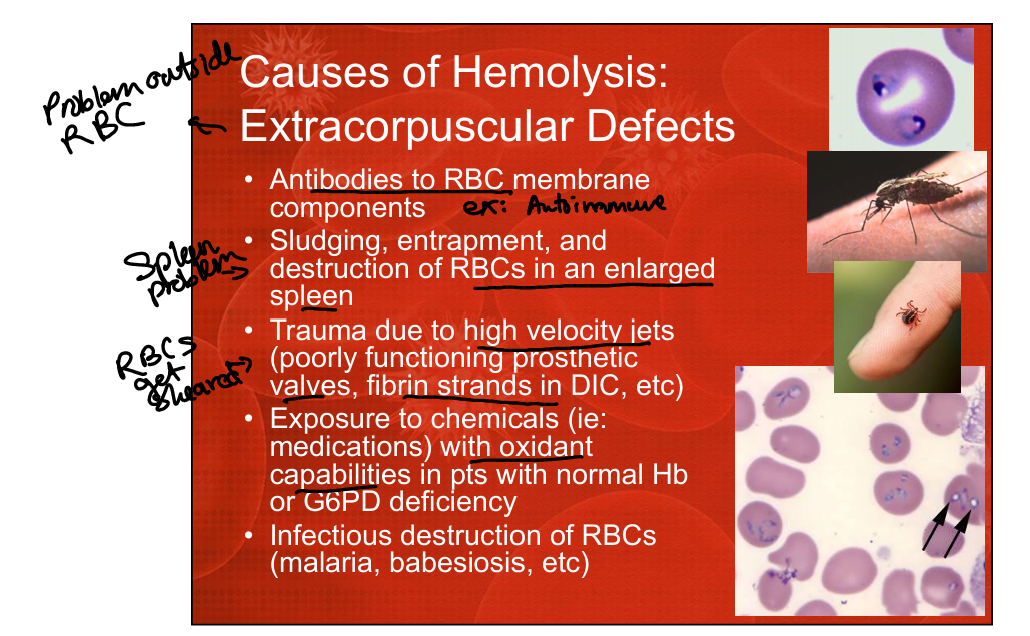
What are extracorpuscular causes of hemolysis?
External factors damaging RBCs: antibodies, splenic sequestration, mechanical trauma, oxidant drugs, infections (malaria, babesiosis).
What RBC membrane disorders cause hemolysis?
Hereditary spherocytosis and hereditary elliptocytosis.
What RBC enzyme disorders cause hemolysis?
G6PD deficiency and pyruvate kinase deficiency.
What hemoglobin disorders cause hemolysis?
Unstable hemoglobins, methemoglobinemia, thalassemia, sickle cell disease.
What infectious organisms can cause hemolysis?
Malaria, babesiosis, Bartonella (listed under smear abnormalities).
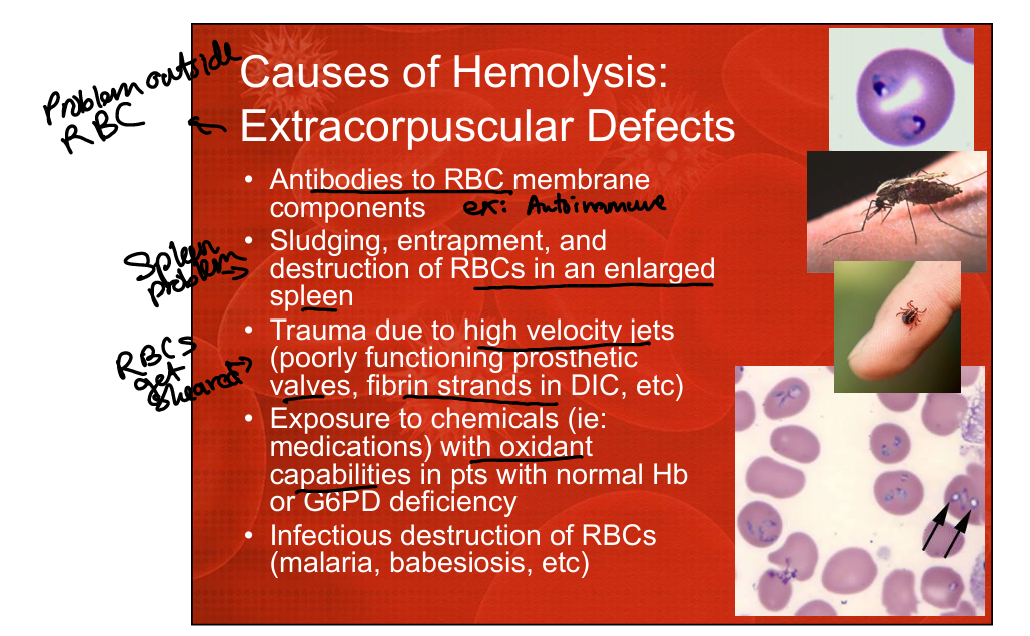
What mechanical processes can cause hemolysis?
Defective prosthetic valves, high‑velocity jets, fibrin strands in DIC, march hemoglobinuria.
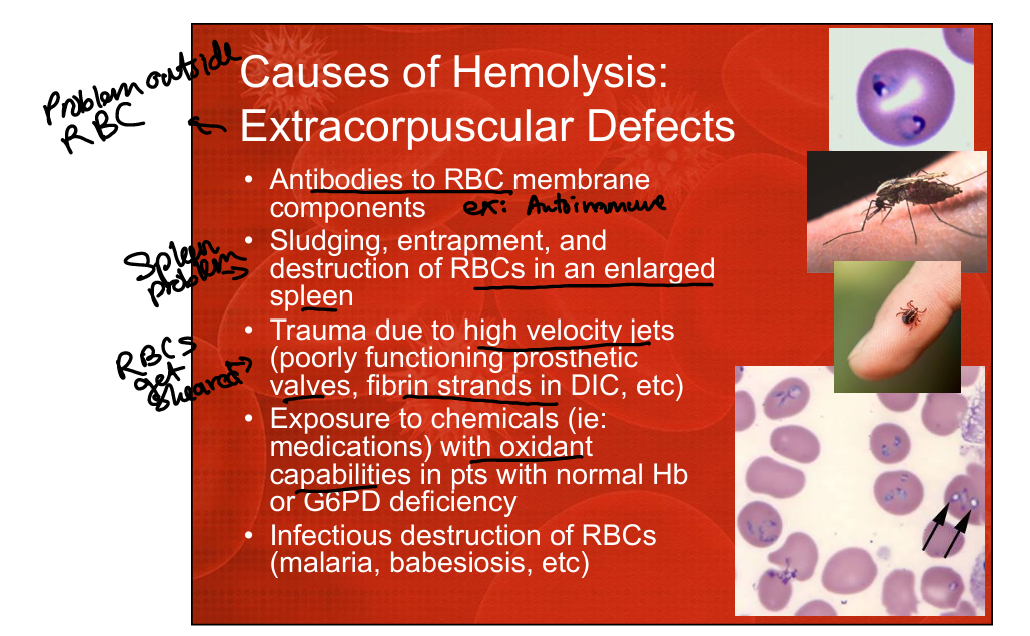
What chemical exposures can cause hemolysis?
Oxidant drugs, especially dangerous in G6PD deficiency.
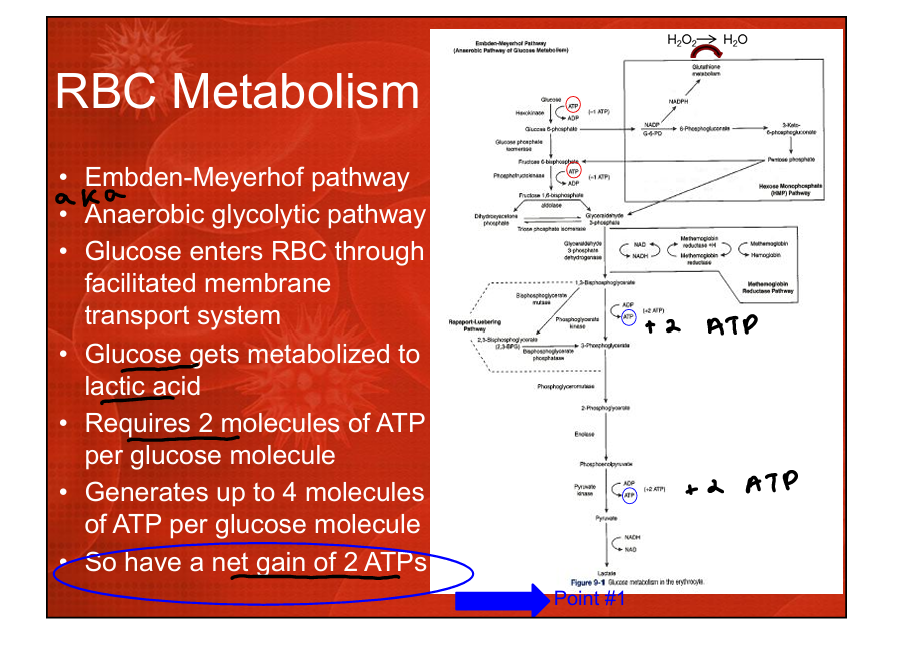
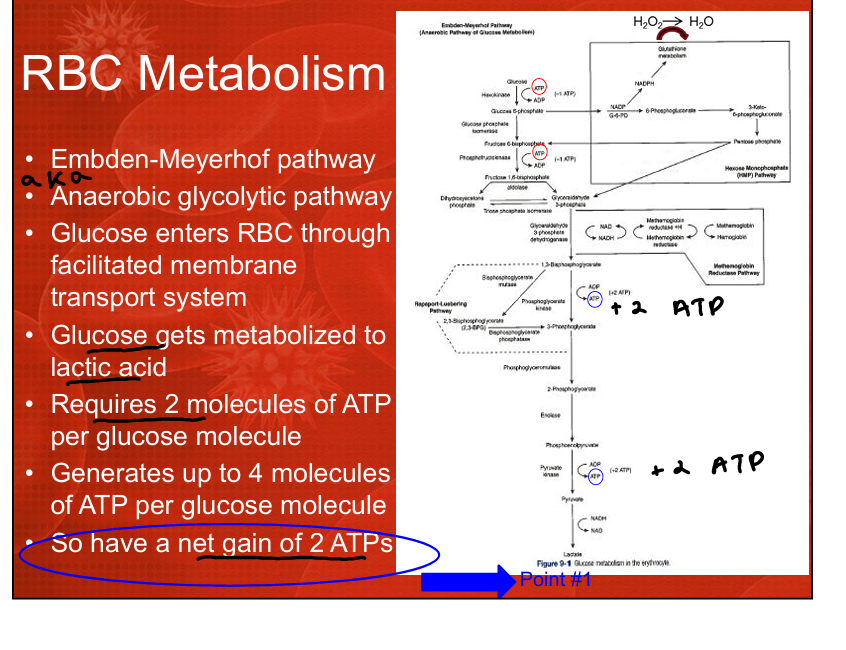
What is the Embden-Meyerhof pathway?
The anaerobic glycolytic pathway in RBCs that generates 2 NET ATP and 2,3‑BPG.
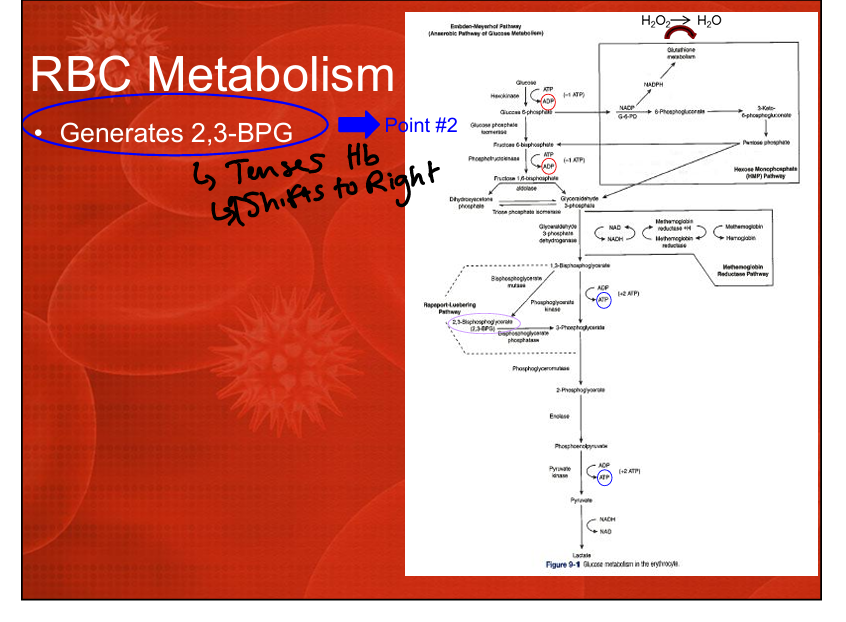
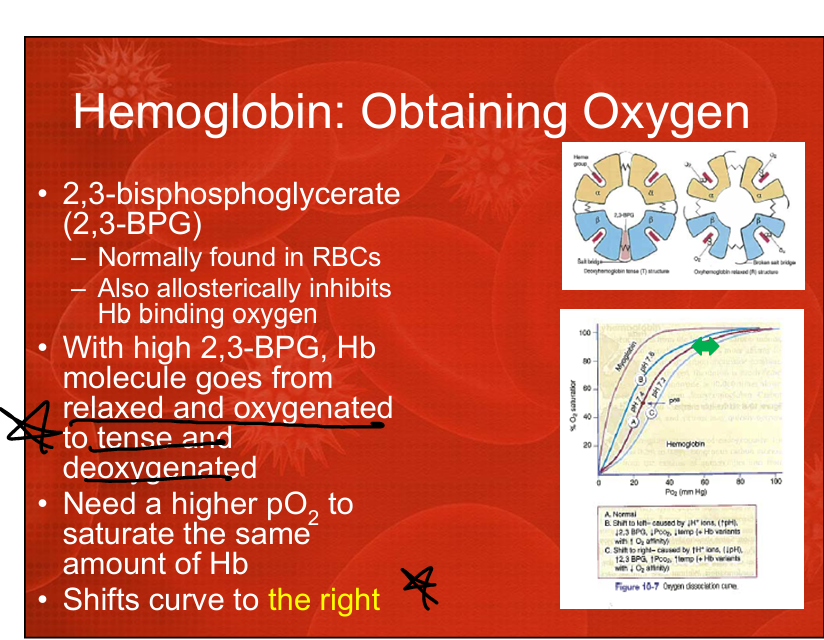
What is the significance of 2,3-BPG production in RBCs?
2,3-BPG decreases Hb oxygen affinity by tensing Hb causing it to release O2, shifting the O2 dissociation curve right and promoting oxygen release.
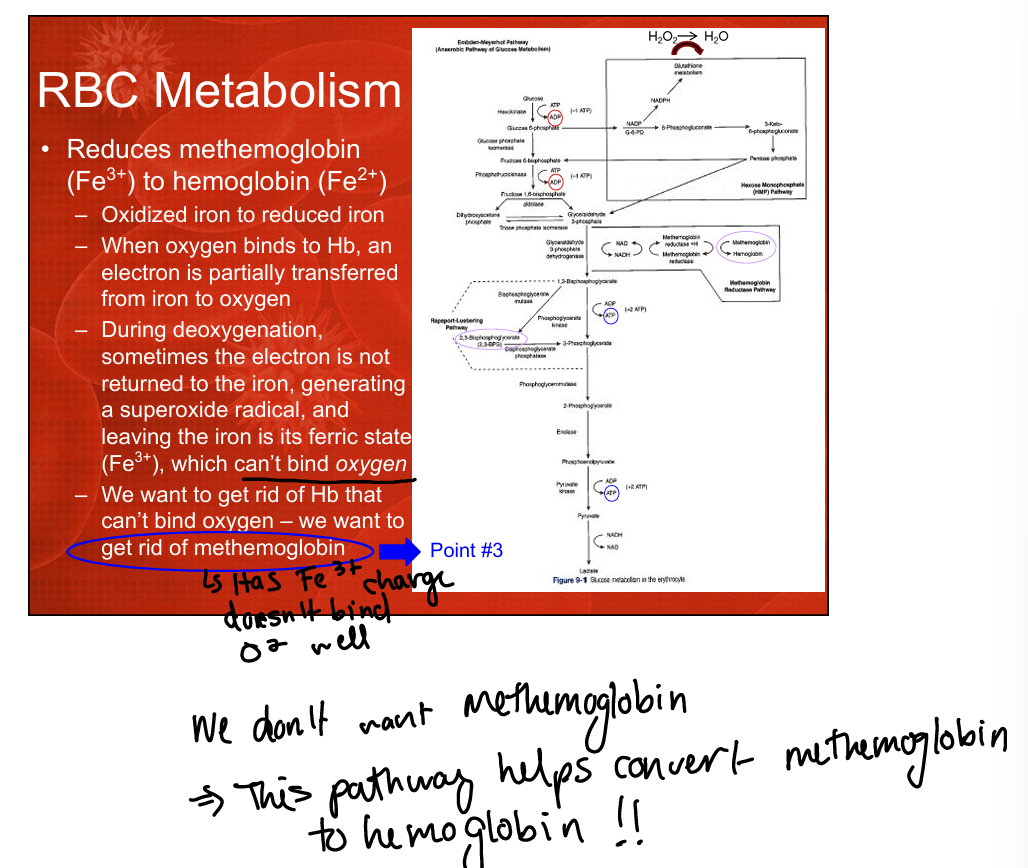
What pathway reduces methemoglobin back to hemoglobin?
The methemoglobin reductase pathway (converts Fe3+ to Fe2+). Occurs during RBC metabolism
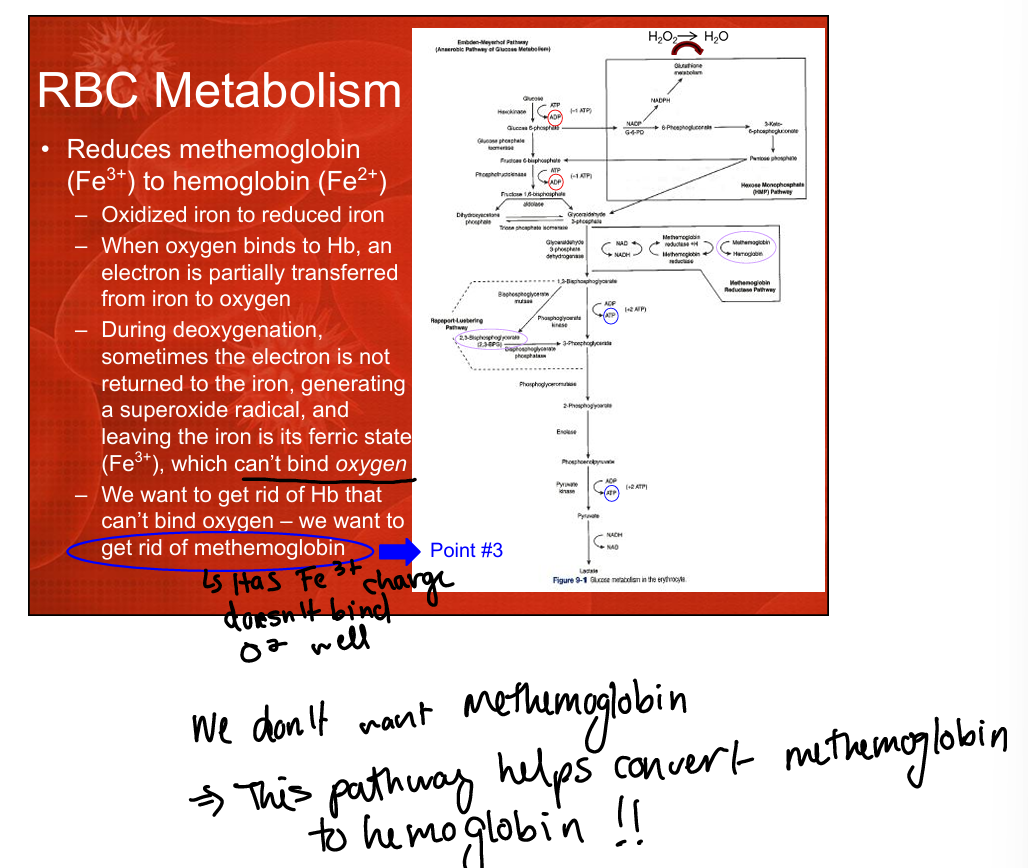
Why is methemoglobin problematic?
Fe3+ cannot bind oxygen, impairing oxygen delivery.
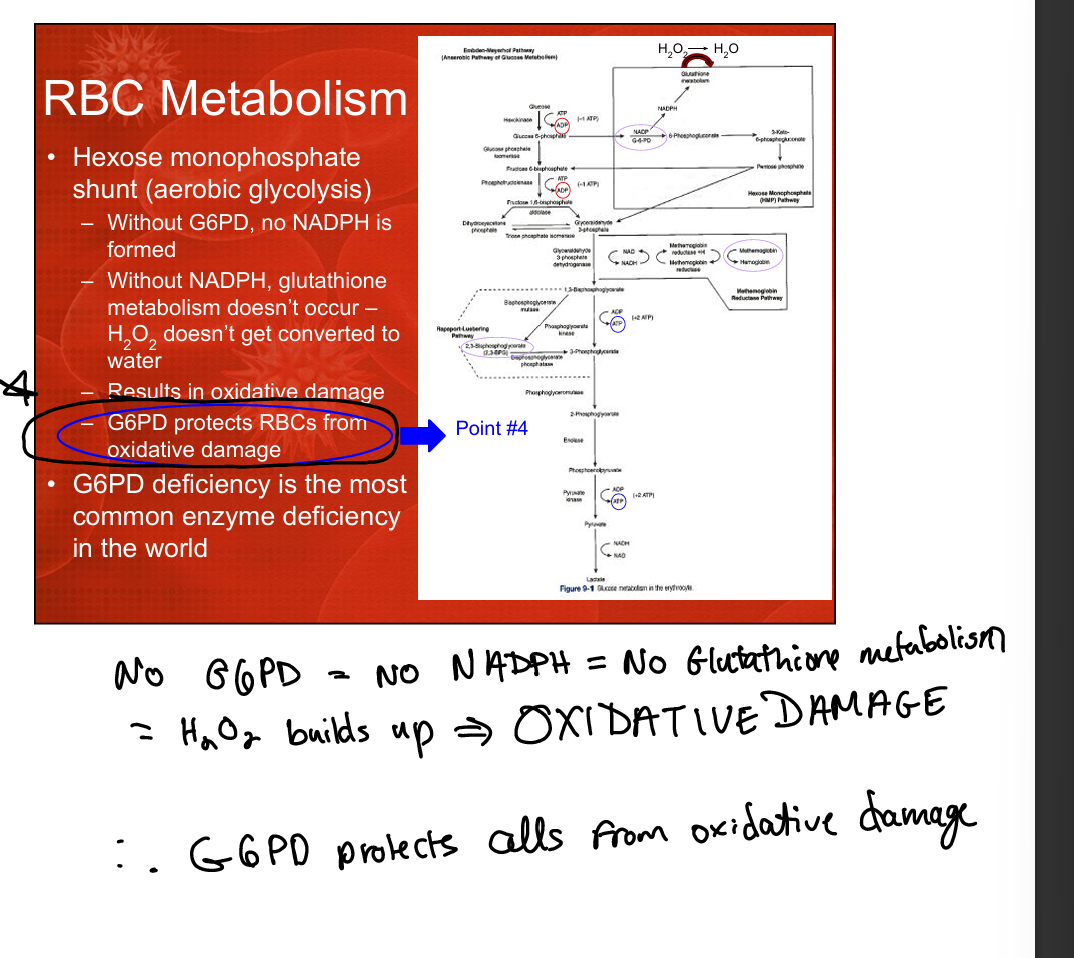
What pathway protects RBCs from oxidative damage?
The hexose monophosphate shunt (HMP shunt), which generates NADPH for glutathione reduction>converts H2O2 to water preventing oxidative damage
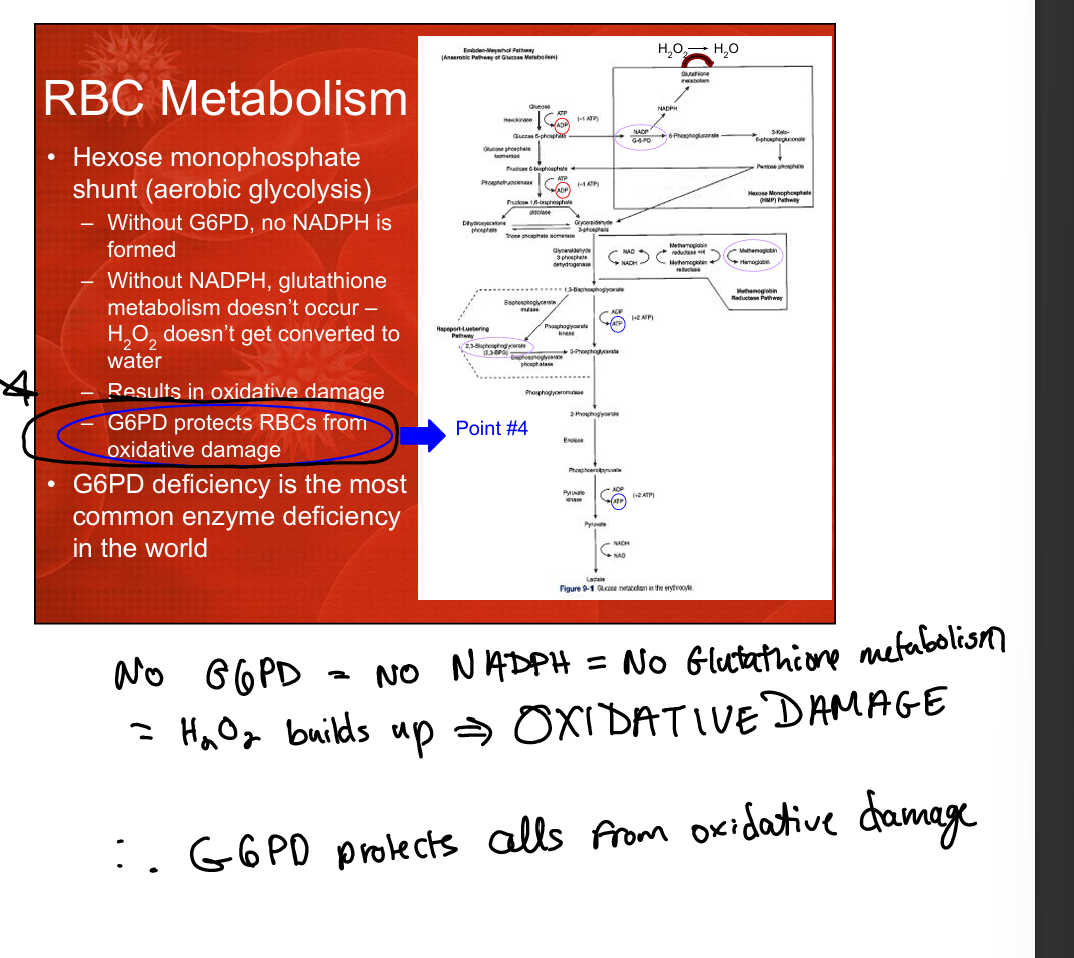
Why is G6PD important?
It produces NADPH, which maintains reduced glutathione to detoxify H2O2 and prevent oxidative hemolysis. (otherwise H2O2 would build up and cause oxidative damage)
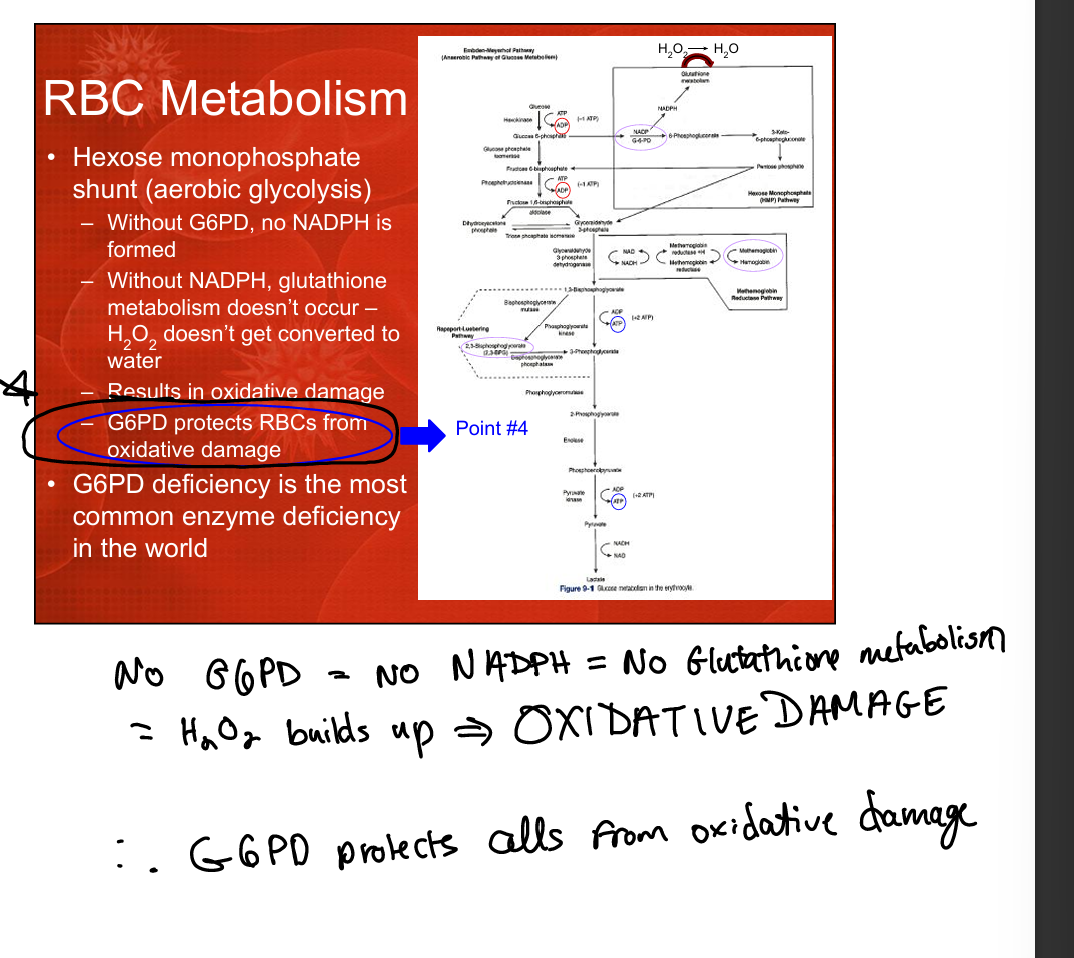
What happens in G6PD deficiency when exposed to oxidant drugs?
No NADPH → no glutathione → oxidative damage → denatured Hb → hemolysis.
What are the major pathways involved in RBC metabolism?
Embden-Meyerhof pathway (ATP), Rapoport-Luebering shunt (2,3-BPG), methemoglobin reductase pathway (Fe3+→Fe2+), hexose monophosphate shunt (NADPH/glutathione).
What happens to hemoglobin during intravascular hemolysis?
Free Hb enters plasma, binds haptoglobin, forms dimers filtered by kidneys, causing hemoglobinuria and hemosiderinuria.
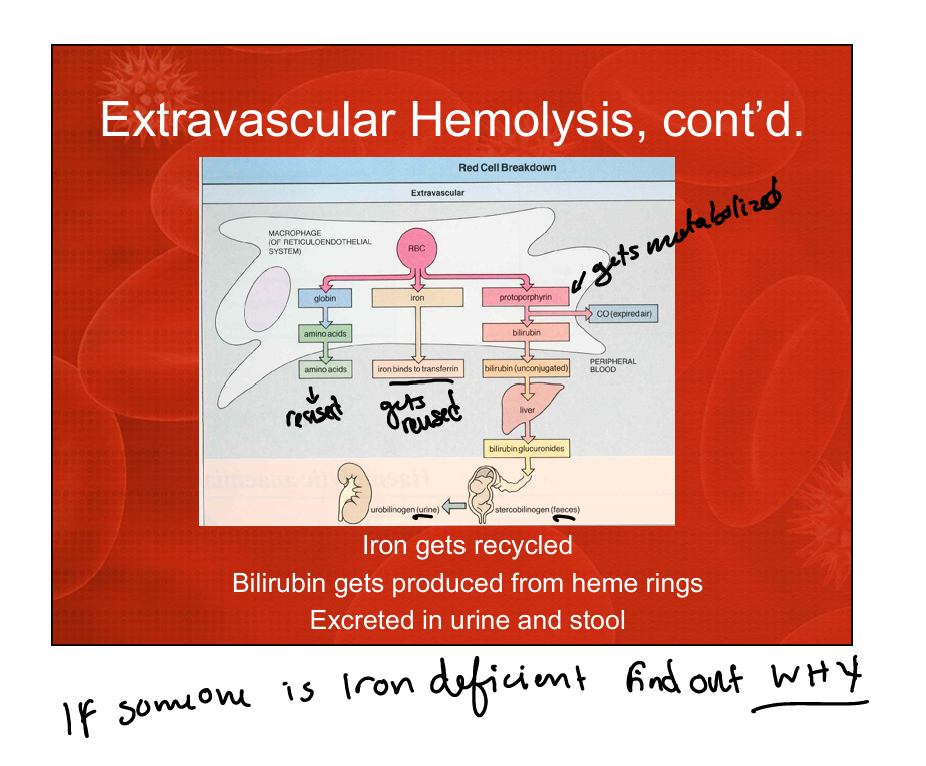
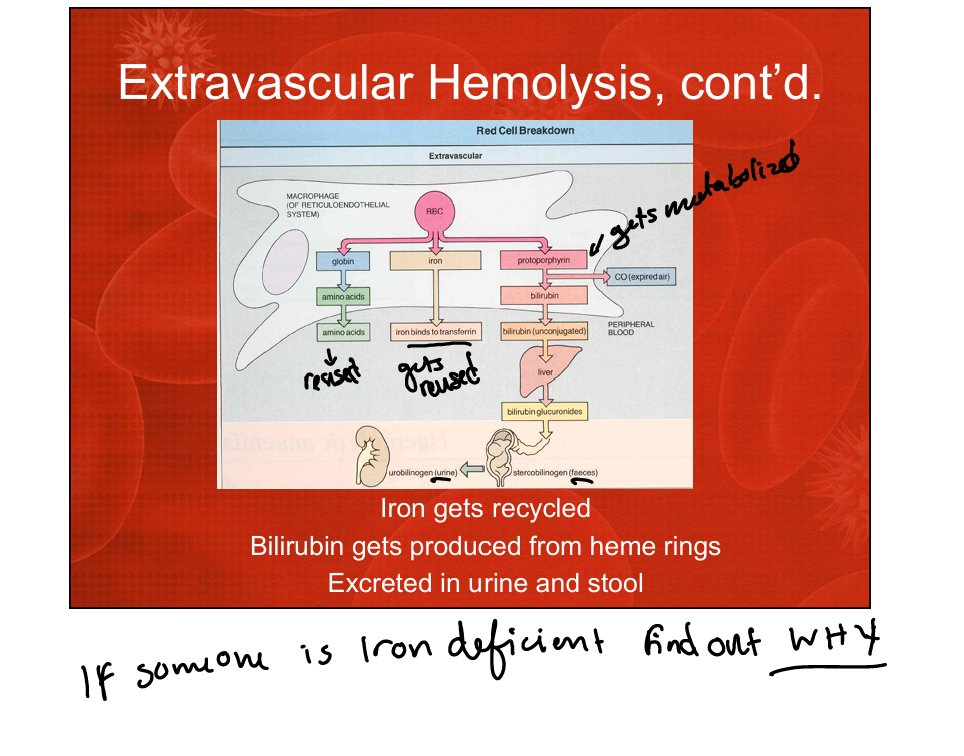
What happens to RBC during extravascular hemolysis? (different parts disassembled)
Macrophages degrade Hb into iron (recycled), globin (amino acids), and bilirubin (excreted).
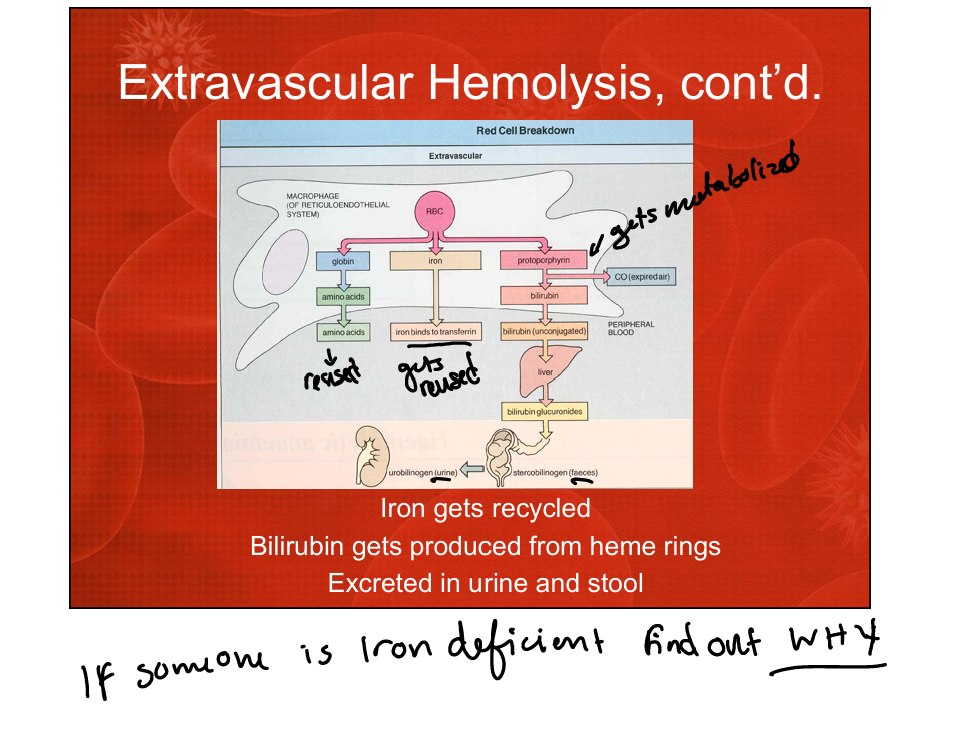
What is the fate of iron during extravascular hemolysis?
Iron is recycled and stored
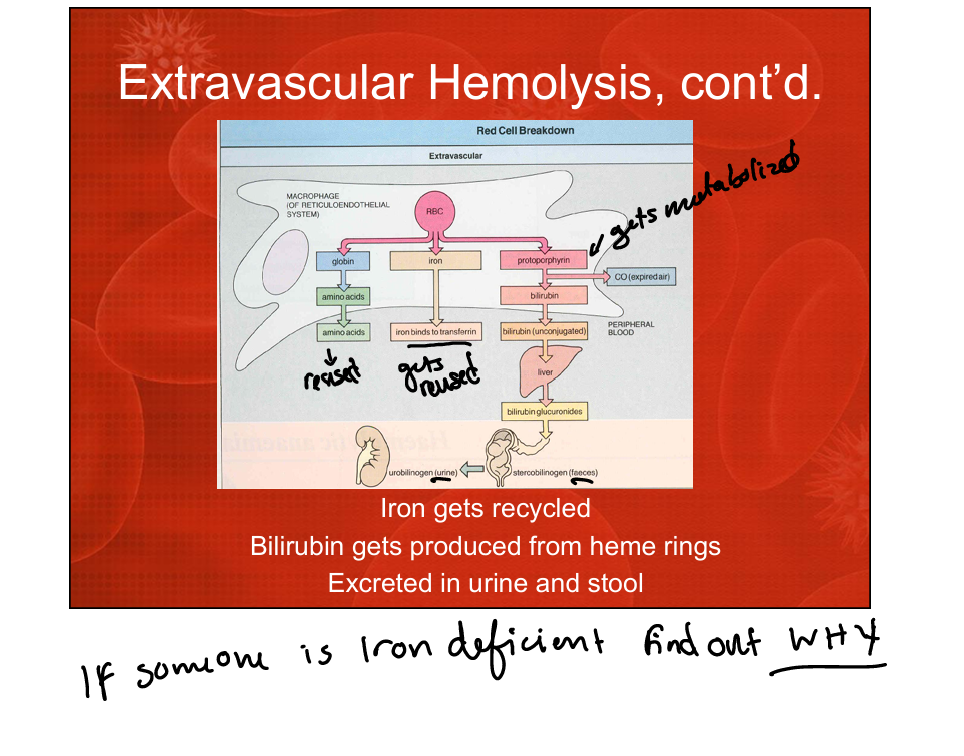
What is the fate of bilirubin during extravascular hemolysis?
Unconjugated bilirubin is transported to the liver, conjugated, and excreted in urine (urobilinogen) and stool (stercobilinogen).
Why do patients with chronic hemolysis need folate supplementation?
Folate stores last only ~10 days and are rapidly consumed due to increased erythropoiesis.
Why do patients with chronic hemolysis usually not need B12 supplementation?
B12 stores last ~10 years.
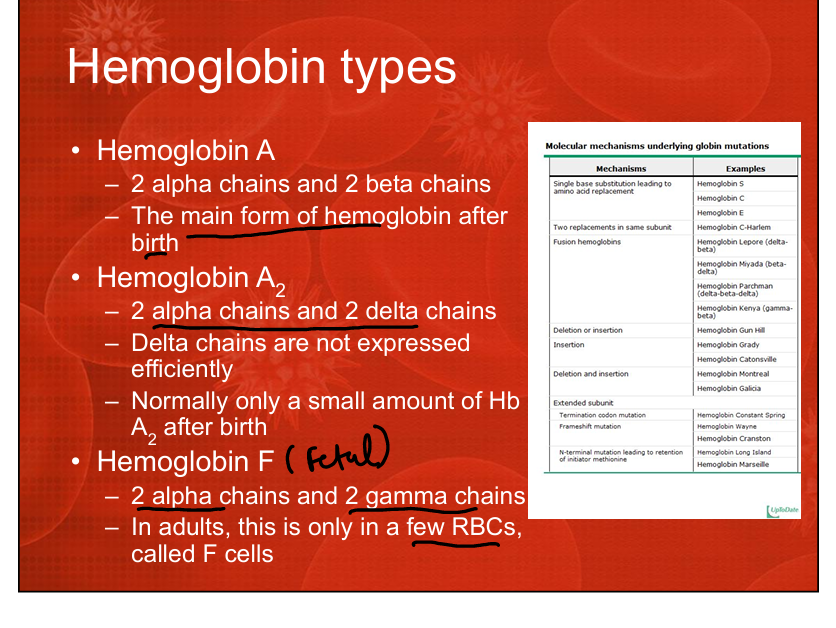
What hemoglobin type predominates after birth? Consists of?
Hemoglobin A (α2β2).
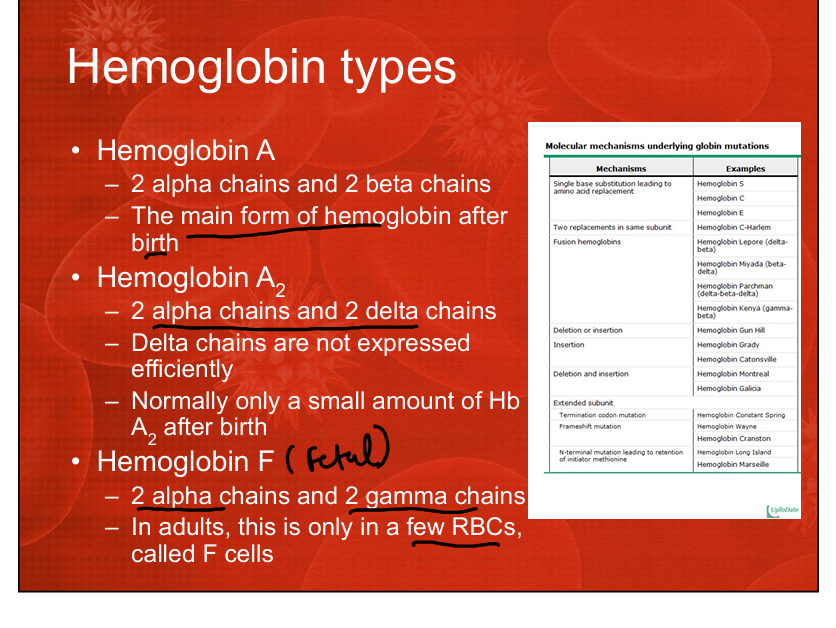
What hemoglobin type predominates in fetal life? Consists of?
Hemoglobin F (α2γ2).
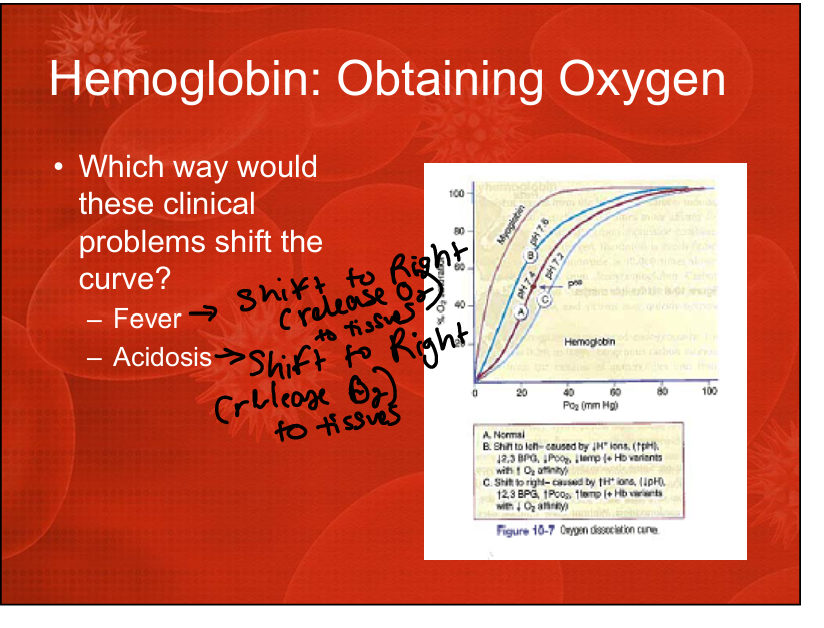
What is the effect of fever on the oxygen dissociation curve?
Shifts the curve to the right (decreases affinity, increases oxygen release).>more blood to tissues. Right Releases, Left Loads
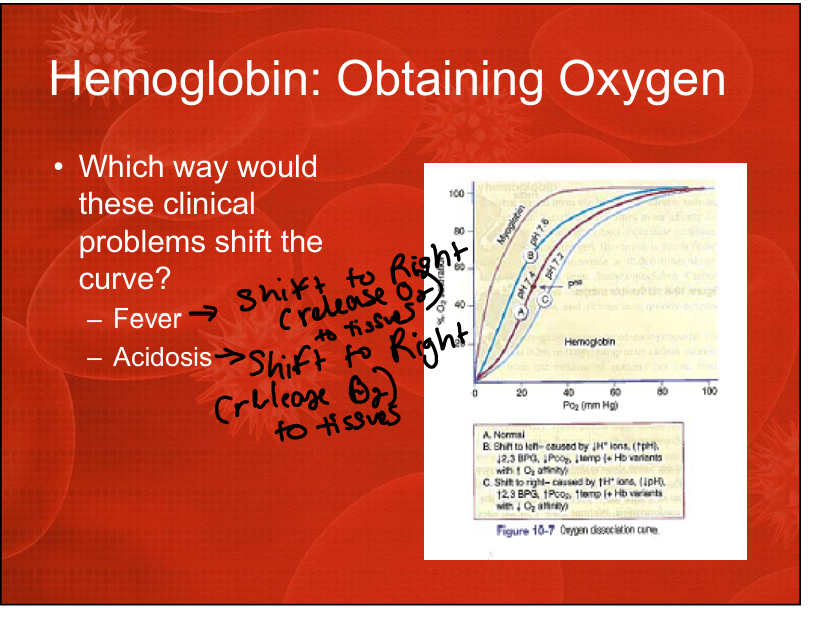
What is the effect of acidosis on the oxygen dissociation curve?
Shifts the curve to the right (Bohr effect). Right Releases, Left Loads
What is the effect of increased 2,3-BPG on the oxygen dissociation curve?
Shifts the curve to the right (promotes oxygen unloading). Right Releases Left Loads
Where are alpha globin genes located?
Chromosome 16.
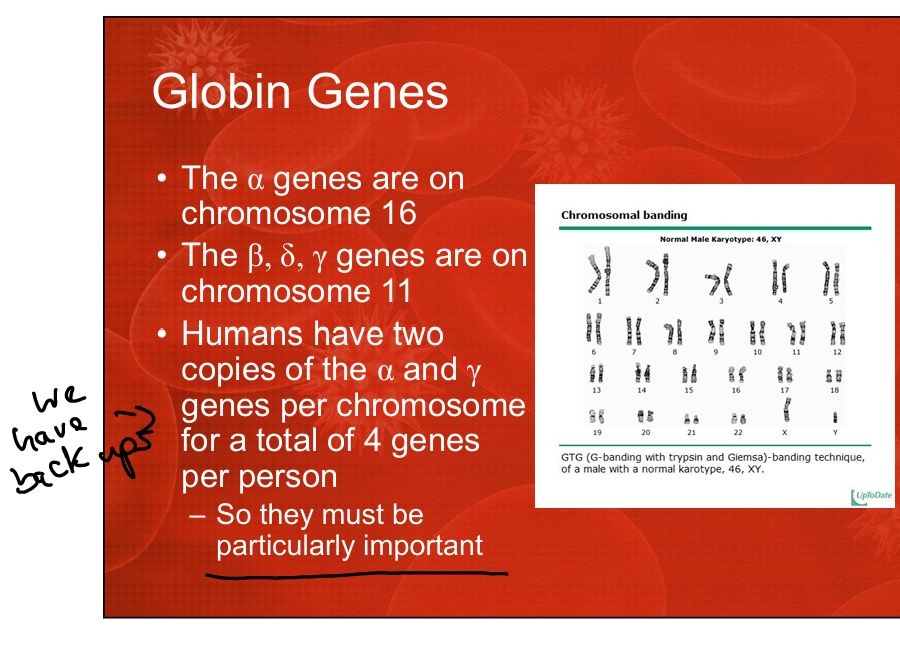
Where are beta, delta, and gamma globin genes located?
Chromosome 11.
What is HbA1c?
Glycated hemoglobin formed by glucose binding to the beta chain